
Abstract
Objectives:
Factors affecting adherence to medications in people with attention-deficit/hyperactivity disorder (ADHD) are not well understood in the context of their influence on the different phases of adherence, that is, initiation, implementation, and discontinuation. This review aimed to identify the factors affecting the three phases of medication adherence in people with ADHD.
Methods:
Six electronic databases, including Medline, PubMed, IPA, CINAHL, Embase, and PsycINFO, were systematically searched from inception through October 2018 with the limitations of English language and human studies. The search strategy was based on three concepts (adherence, ADHD, and factors) and their relevant terminologies.
Results:
Considerable variability was observed with regards to the criteria used to define adherence in identified studies (n = 48). Most studies focused on the implementation phase of adherence (n = 27), while only a handful focused on the initiation (n = 6) and discontinuation (n = 5) phase of adherence. The remaining studies (n = 10) examined multiple phases of adherence. Conflicting information received about medication, medication frequency, and fears of medication's effect on growth were the unique factors impacting initiation, implementation, and discontinuation, respectively. Moreover, factors within each phase of adherence also differed with different populations such as parents, children, adolescents, and adults. Fear of addiction, medication effectiveness, psychiatric comorbidity, and medication side effects were the most common factors identified in all three phases of adherence.
Conclusions:
This review found some unique factors in each phase of adherence while some overlap was also noted. Future interventions to improve adherence should be phase- and group specific rather than consider adherence as a single variable.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common psychiatric disorders among children and adolescents, characterized by hyperactivity, inattention, and impulsivity (Winterstein et al. 2008). ADHD is a chronic condition that often continues to demonstrate notable symptoms throughout life. Polanczyk et al. (2007) estimated the worldwide prevalence of ADHD as 5.29% in children aged 18 years or younger. In another review, Willcutt et al. (2012) estimated the global prevalence of ADHD as 5.9%–7.1% in children and adolescents. In 2014, Polanczyk et al. updated their previous review and reported the global prevalence as about 5% (Polanczyk et al. 2014). The variation in estimated prevalence of ADHD was best explained by the methodological heterogeneity between the studies (Sayal et al. 2018). The worldwide prevalence of ADHD has been reported as 1.2% to 7.3% in adults (Polanczyk et al. 2007).
The use of pharmacological agents is considered an integral component of evidence-based management in people with ADHD. Stimulant medications, such as methylphenidate (immediate release, modified release, and osmotic controlled release) and amphetamines, are the first-line pharmacological agents for the management of ADHD. Nonstimulants, such as atomoxetine, guanfacine, and clonidine, are usually considered as the second-line options (National Institute for Health and Care Excellence 2018).
Despite the availability of effective behavioral treatment, pharmacotherapy plays a primary role in the management of ADHD (Dopheide 2009). The use of pharmacotherapy has been supported by robust efficacy and safety data (Murray et al. 2008). Furthermore, the use of medication is considered the most cost-effective therapy for ADHD (National Institute for Health and Care Excellence 2018). This is particularly important owing to the chronic nature of the disease as it allows the use of long-term pharmacotherapy. It has been reported that the use of long-term medications results in improved academic and social functioning of people with ADHD (Wilens et al. 2008; Chien et al. 2012). The use of pharmacotherapy among children with ADHD has increased substantially in the past 2 decades (Raman et al. 2018). Even in adults, where ADHD is relatively less prevalent and diagnosed, the use of medication has increased by 18% (Dopheide 2009). A study reported that the use of methylphenidate has increased from 39.6% in 1997 to 54% in 2005 in Taiwan (Chien et al. 2012). Another study from Germany reported that 52% of patients were prescribed pharmacological agents as part of ADHD treatment (Garbe et al. 2012). Furthermore, a recent study suggested a 101.8% increase in the use of ADHD medications in Australia from 2007 to 2015 (Brett et al. 2017).
Adherence to ADHD medication is very important to achieve the desired treatment outcomes. However, it has been reported that poor medication adherence is common among people with ADHD and leads to suboptimal therapeutic response. A systematic review of 12 studies measuring adherence in children and adolescents reported a range of 9.8% to 64% (Gajria et al. 2014). The wide variation in the reported rate of adherence could be explained by the use of different terminologies and taxonomies in the adherence-related literature. Medication adherence comes under the broader concept of medication-taking behavior, the history of which is as old as the time of Hippocrates (Osterberg and Blaschke 2005). However, in the late 20th century, the concept was given the term “compliance” (Haynes 1979). Compliance was defined as “the extent to which the patient's behavior (in terms of taking medications, following diets, or executing other lifestyle changes) coincides with medical or health advice” (Haynes 1979). However, as the concept of patient-centered care evolved, the term “compliance” received criticism because it was viewed as implying passive acceptance of clinician's recommendation by the patient. This led to the introduction of the term “adherence” that gives patients a more active role in disease management. Adherence was defined as “The extent to which a person's behaviour- taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider” (World Health Organization 2003). These terms have been used interchangeably in the literature and have generated confusion and inconsistencies in adherence research (Ahmed and Aslani 2014).
Several studies have reported mean adherence of <6 months, and occasionally <1 year, using naturalistic samples (Adler and Nierenberg 2010). Furthermore, a cohort of patients using methylphenidate reported using prescribed medication only half of the time recommended by their clinician (Darredeau et al. 2007). It has also been reported that the rate of adherence in people with ADHD is low regardless of the pharmacological treatment options (i.e., stimulant or nonstimulant) (Treuer et al. 2016). A study reported medication discontinuation rate of 13.2% to 64% among people with ADHD (Adler and Nierenberg 2010). The low level of adherence to ADHD medications results in symptomatic relapse, increased morbidity, increased health expenditure, and difficulties for the clinician to assess the effectiveness of the prescribed regimen (Ahmed and Aslani 2013). Nonadherence has also been associated with suboptimal response and less improvement in clinical severity (Childress and Sallee 2014). The success of transition from initial management to long-term treatment is fraught with pitfalls. Lack of adherence to the prescribed regimen is believed to be the barrier toward successful long-term management of ADHD (Skoglund et al. 2016).
In view of the poor medication adherence in people with ADHD, it is essential to examine the factors contributing to nonadherence. Lack of information about the determinants of medication adherence can pose a critical challenge to clinicians. The reasons for nonadherence to ADHD medications are multifactorial and difficult to examine (Adler and Nierenberg 2010). There has been a recent surge in studies examining the factors associated with medication adherence in people with ADHD (Skoglund et al. 2016). Some studies have reported demographic factors such as socioeconomic status, age, gender, geographic location, race, ethnicity, and clinical characteristics as the major barriers to adherence (Winterstein et al. 2008; Chen et al. 2009; Coker et al. 2016). Other studies have shown the lack of treatment effectiveness, parental will, and social factors as the main contributors toward nonadherence in people with ADHD (Antony 2016). Parental beliefs and attitudes about ADHD medication have also found to be contributory factors toward ADHD medication adherence (Dosreis and Myers 2008). Health care associated costs such as the cost of prescriptions and other indirect costs such as time off from work and providing care for a person with special needs may also affect adherence to medication use in some settings (Fiks et al. 2012).
Few attempts have been made to summarize the factors affecting adherence to medications in people with ADHD. Some reviews have reported the factors associated with discontinuation only (Gajria et al. 2014; Frank et al. 2015), while others have focused on specific medications such as atomoxetine (Treuer et al. 2016). One systematic review distinguished the factors as patient related or medication related (Caisley and Müller 2012), while others narrated the factors without any categorization (Swanson 2003; Charach and Gajaria 2008; Greydanus and Kaplan 2012; Childress and Sallee 2014). No attempt has been made to review the existing body of research to identify and classify the factors affecting medication adherence in the context of its three phases, that is, initiation, implementation, and discontinuation. Research in other disease populations suggests that factors influencing one phase of adherence may not necessarily affect the other two phases (Gillespie et al. 2017; Srimongkon et al. 2018). Therefore, it is important to classify factors based on the three phases so that phase-specific interventions could be developed to improve medication adherence. This concept was initially proposed by Vrijens et al. (2012) who recommended a more rigorous taxonomy (the ABC taxonomy) of adherence to better understand the complex issue of medication adherence in clinical settings.
The ABC taxonomy defines medication adherence as the process by which patients take their medications as prescribed (Vrijens et al. 2012). In this taxonomy, adherence to medication was classified into three phases: initiation, implementation, and discontinuation. The three phases of adherence are underpinned by the assumption that the patient/parent/carer has agreed with the treatment. Initiation was defined as commencement of the prescribed medication. Implementation was defined as the extent to which patients follow their prescribed regimen from initiation until discontinuation. Discontinuation was defined as an earlier than prescribed end of therapy by the patient for any given reason (Vrijens et al. 2012). The aim of this review was to identify the factors affecting adherence at initiation, implementation, and discontinuation phases of adherence (ABC taxonomy) and differentiate the factors affecting adherence to ADHD medications in children, adolescents, adults, and parents/carers based on the three phases.
Methods
Data sources and search strategy
The following six electronic databases were searched: Medline, PubMed, International Pharmaceutical Abstracts (IPA), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, and the Psychological Information Database (PsycINFO). A systematic search was performed for all studies that examined factors affecting medication adherence or its related terms (compliance and persistence) in people with ADHD. All databases were searched from inception through October 2018 with the limitations of English language and human studies. The search strategy combined terms that represented adherence, ADHD, and factors (Supplementary Table S1).
Eligibility criteria
The eligibility criteria were developed to include all studies that examine the factors influencing medication adherence regardless of any minimum or maximum requirement for study duration, number of patients, number of medication, doses, frequency, and type of medication. Moreover, studies were not included/excluded based on the definition of adherence. The broad approach was chosen to accommodate the methodological and taxonomical heterogeneity in the adherence literature. The following inclusion/exclusion criteria were set for the studies.
Inclusion criteria
Studies that: examined factors affecting adherence or its related terms to at least one type of medication used for people with ADHD; included details of what phase(s) of adherence was measured or at what stage of medication-taking the factors were evaluated to allow categorization of the factors based on the three phases of adherence; included children, adolescents, adults, or parents/carer as study participants.
Exclusion criteria
Studies were excluded if they:
examined adherence to nonpharmacological management of ADHD;
measured adherence but did not evaluate the factors affecting medication adherence;
compared the level of adherence between two medications but did not focus on examining factors affecting adherence;
were reviews, commentaries, conference abstracts, and expert opinions.
Study selection
The articles were selected after a thorough two-phase review process. In the first phase, both authors reviewed the title and abstract of the studies retrieved from the literature search for eligibility. In the second phase, the full text of the articles which met the inclusion criteria in phase one was skim-read to ensure consistency with the eligibility criteria. The articles that met the inclusion criteria were then reviewed in detail for data extraction.
Data extraction
M.U.K. extracted the data from the eligible studies. A proportion of extracted data were then reviewed by P.A. for consistency. The data were extracted using a piloted form (Tables 1 and 2). The form extracted the following information: author(s) and publication year, country, study design, study duration, population studied, number of participants, adherence definition used, study measure, type of medication, adherence phase, factors affecting medication adherence, and summary critique. Any ambiguity during this process was addressed through a discussion between the authors.
Study Characteristics
Studies Examining Factors Affecting Medication Adherence in Patients with Attention-Deficit/Hyperactivity Disorder
Adherence definition was taken from the studies, while adherence phase was based on authors' interpretation.
ADHD, attention-deficit/hyperactivity disorder; MPR, medication possession ratio; ODD, oppositional defiant disorder.
Quality assurance
This was a narrative review, which was conducted in a systematic manner to improve the methodological rigor. Therefore, the reporting of this narrative review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, an approach commonly utilized in systematic reviews (Moher et al. 2009) (Supplementary Table S2). For the quality assessment of the selected studies, we followed an alternative approach. The Centre for Reviews and Dissemination (CRD) guideline suggests the use of a structured strategy to assess the quality of articles for inclusion in systematic reviews (Centre for Reviews and Dissemination 2010). However, it also acknowledges the complexities surrounding the definition of quality. Scholars suggest the inclusion of a critique of individual studies in the narrative review to allow the readers to decide on the quality of the studies (Dixon-Woods et al. 2005; Lakhanpaul et al. 2014). The same approach has been used in this review.
Data synthesis
The studies that met the eligibility criteria varied considerably in terms of their design and methods. For example, both quantitative and/or qualitative methods were used to address study questions using a range of study measures. Results were synthesized in the form of a narrative report in view of the heterogeneity among studies, as suggested elsewhere (Dixon-Woods et al. 2005; Popay et al. 2006; Lakhanpaul et al. 2014).
Results
Study selection
A total of 1370 records were identified through database searching (Fig. 1). After removing the duplicates, 424 articles were screened against the selection criteria based on their titles and abstracts. This resulted in the exclusion of 298 articles because of not meeting the inclusion criteria. The full text of the remaining articles (n = 126) was reviewed and assessed for eligibility, of which 81 articles were further excluded for not meeting the inclusion criteria, resulting in the inclusion of 48 articles for qualitative synthesis.
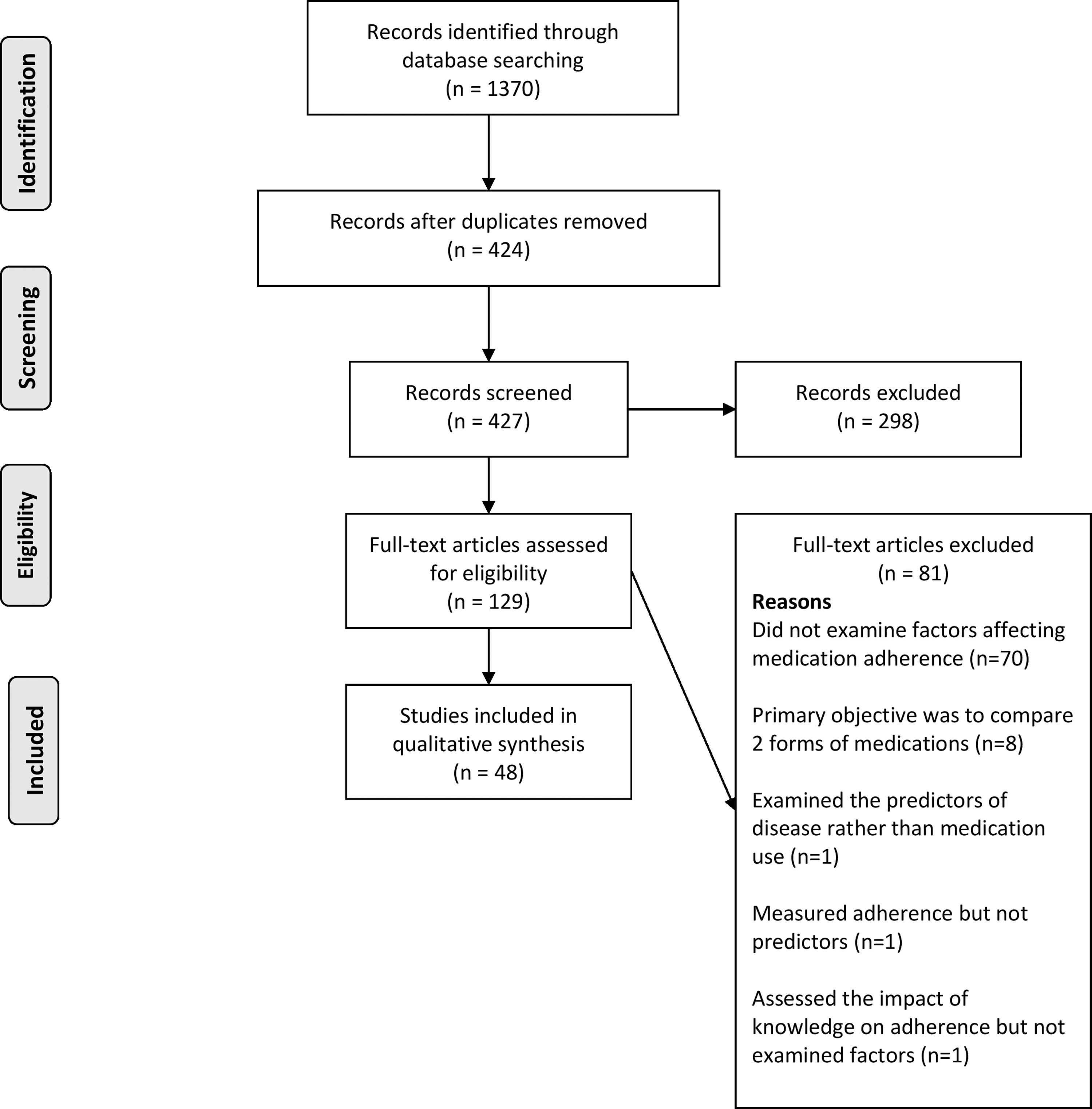
PRISMA flow diagram.
Study characteristics
An overview of the study characteristics is presented in Table 1. Most studies were conducted in the United States (n = 17) (Rieppi et al. 2002; Monastra 2005; Faraone et al. 2007; Safren et al. 2007; Barner et al. 2011; Hodgkins et al. 2011; Brinkman et al. 2012; Coletti et al. 2012; Cormier 2012; Palli et al. 2012; Toomey et al. 2012; Fiks et al. 2013; O'Callaghan 2014; Bali et al. 2015; Li et al. 2017; Schaefer et al. 2017; Sleath et al. 2017) followed by Canada (n = 5) (Thiruchelvam et al. 2001; Miller et al. 2004; Charach et al. 2006; Darredeau et al. 2007; Hebert et al. 2013), Taiwan (n = 4) (Chen et al. 2011; Gau et al. 2006, 2008; Wang et al. 2016), Sweden (n = 4) (Thorell and Dahlström 2009; Bejerot et al. 2010; Bahmanyar et al. 2013; Emilsson et al. 2017), Korea (n = 3) (Hong et al. 2014, 2016; Bhang et al. 2017), United Kingdom (n = 2) (Wong et al. 2009; Raman et al. 2015), Turkey (n = 2) (Ayaz et al. 2014; Semerci et al. 2016), Germany (n = 2) (Sobanski et al. 2014; Wehmeier et al. 2015), the Netherlands (n = 2) (van den Ban et al. 2010; Bijlenga et al. 2017), Italy (n = 1) (Atzori et al. 2009), India (Sitholey et al. 2011), Australia (n = 1) (Ahmed et al. 2017), and Norway (n = 1) (Torgersen et al. 2012). The three remaining studies were multicenter studies conducted in different parts of nonwestern countries (Treuer et al. 2014), Central Europe and East Asia (Hong et al. 2013), and Europe (Kooij et al. 2013). All studies were published between 2001 and 2017. Most studies collected data prospectively (n = 31) (Thiruchelvam et al. 2001; Rieppi et al. 2002; Monastra 2005; Charach et al. 2006; Gau et al. 2006, 2008; Darredeau et al. 2007; Faraone et al. 2007; Safren et al. 2007; Atzori et al. 2009; Thorell and Dahlström 2009; Bejerot et al. 2010; Sitholey et al. 2011; Brinkman et al. 2012; Coletti et al. 2012; Cormier 2012; Toomey et al. 2012; Fiks et al. 2013; Hebert et al. 2013; Hong et al. 2013; Kooij et al. 2013; Ayaz et al. 2014; O'Callaghan 2014; Sobanski et al. 2014; Treuer et al. 2014; Wehmeier et al. 2015; Ahmed et al. 2017; Bijlenga et al. 2017; Emilsson et al. 2017; Schaefer et al. 2017; Sleath et al. 2017) compared to retrospective studies (n = 16) (Miller et al. 2004; van den Ban et al. 2010; Barner et al. 2011; Chen et al. 2011; Hodgkins et al. 2011; Palli et al. 2012; Torgersen et al. 2012; Bahmanyar et al. 2013; Hong et al. 2014, 2016; Bali et al. 2015; Raman et al. 2015; Semerci et al. 2016; Wang et al. 2016; Bhang et al. 2017; Li et al. 2017), while 1 study used both approaches (Wong et al. 2009). The majority of studies included both children and adolescents as study participants (n = 17) (Miller et al. 2004; Gau et al. 2008; Atzori et al. 2009; Barner et al. 2011; Chen et al. 2011; Palli et al. 2012; Bahmanyar et al. 2013; Hong et al. 2013; Ayaz et al. 2014; Hong et al. 2014; Treuer et al. 2014; Bali et al. 2015; Raman et al. 2015; Wehmeier et al. 2015; Hong et al. 2016 Wang et al. 2016; Bhang et al. 2017) followed by parents (n = 11) (Monastra 2005; Charach et al. 2006; Gau et al. 2006; Sitholey et al. 2011; Brinkman et al. 2012; Coletti et al. 2012; Cormier 2012; Toomey et al. 2012; Fiks et al. 2013; Hebert et al. 2013; Ahmed et al. 2017), adults (n = 10) (Darredeau et al. 2007; Safren et al. 2007; Bejerot et al. 2010; Torgersen et al. 2012; Kooij et al. 2013; O'Callaghan 2014; Sobanski et al. 2014; Semerci et al. 2016; Bijlenga et al. 2017; Li et al. 2017), adolescents (n = 4) (Wong et al. 2009; Emilsson et al. 2017; Schaefer et al. 2017; Sleath et al. 2017), children (n = 2) (Rieppi et al. 2002; Faraone et al. 2007), children and parents (n = 2) (Thiruchelvam et al. 2001; Thorell and Dahlström 2009), and children, adolescents, and adults (n = 2) (van den Ban et al. 2010; Hodgkins et al. 2011). The study duration varied from 2 months to 4 years in prospective studies and 2.5 years to 15.6 years in retrospective studies. The number of participants varied from 102 to 112,140 in retrospective studies and 10 to 1068 in prospective studies.
Results of individual studies
Table 2 summarizes the results of individual studies with regards to the definition of adherence, use of adherence measures, adherence phase, and factors affecting medication adherence.
Adherence definition
A considerable variation was observed regarding the criteria used to define adherence. Some studies (Barner et al. 2011; Hodgkins et al. 2011; Hong et al. 2014; Bhang et al. 2017) defined adherence in terms of medication possession ratio by determining the proportion of days patients were in possession of their medicines. Some studies defined adherence based on gaps in therapy (Thiruchelvam et al. 2001; Gau et al. 2006, 2008; van den Ban et al. 2010; Chen et al. 2011; Torgersen et al. 2012). Some defined gaps as no more than 3 months (Thiruchelvam et al. 2001; van den Ban et al. 2010; Chen et al. 2011; Torgersen et al. 2012), while others took it as missing at least 1 dose on a school day for at least 2 days per week for 4 weeks (Gau et al. 2008) or missing 14 days of medication in a month (Gau et al. 2006). A few studies used a cutoff score achieved by patients after using medication adherence instruments to evaluate and define adherence (O'Callaghan 2014; Hong et al. 2013; Wehmeier et al. 2015; Emilsson et al. 2017). For example, medication adherence was defined as the presence of a Pediatric Compliance Self-Rating score of ≥5 on a scale of 1–7 (Wehmeier et al. 2015).
Persistence definition
Persistence was generally defined as continuity of therapy from initiation (Miller et al. 2004; Barner et al. 2011; Hodgkins et al. 2011; Palli et al. 2012; Ayaz et al. 2014; Treuer et al. 2014; Bali et al. 2015; Raman et al. 2015; Hong et al. 2016). However, the length of continuity varied among studies along with the allowed gap (no medication taking) period. It was observed that a gap of 1 month was allowed if persistence was measured over 6 months. A maximum gap of 3 months was allowed if the persistence was measured over a period of 12 months except for one study in which a gap of 4 months was allowed (Miller et al. 2004). One study defined persistence as taking more than 80% of prescribed medication according to the pill count method (Sobanski et al. 2014).
Definitions used for different phases of adherence
A limited number of studies (n = 6) defined the three phases of adherence; initiation, implementation, and discontinuation (Wong et al. 2009; Chen et al. 2011; Coletti et al. 2012; Fiks et al. 2013; Wang et al. 2016; Ahmed et al. 2017). Initiation was defined as commencement of therapy (Wang et al. 2016; Ahmed et al. 2017). Implementation was defined in terms of continuation and persistence with therapy (Ahmed et al. 2017). A couple of studies defined discontinuation as the cessation of therapy for at least 6 months (Wong et al. 2009; Wang et al. 2016). In contrast, a study assumed discontinuation if the patient was not taking therapy at the time of the survey (Toomey et al. 2012). Another study defined discontinuation as the cessation of therapy without specifying the time limit (Ahmed et al. 2017).
Use of measures to examine factors affecting adherence
More than one-third of the studies utilized secondary databases such as hospital prescription records or insurance databases to identify factors affecting medication adherence (n = 18) (Miller et al. 2004; Faraone et al. 2007; van den Ban et al. 2010; Barner et al. 2011; Chen et al. 2011; Hodgkins et al. 2011; Palli et al. 2012; Torgersen et al. 2012; Bahmanyar et al. 2013; Hong et al. 2013, 2014, 2016; Bali et al. 2015; Raman et al. 2015; Semerci et al. 2016; Wang et al. 2016; Bhang et al. 2017; Li et al. 2017) followed by questionnaire (n = 12) (Rieppi et al. 2002; Monastra 2005; Gau et al. 2006; Safren et al. 2007; Thorell and Dahlström 2009; Bejerot et al. 2010; Sitholey et al. 2011; Fiks et al. 2013; Hong et al. 2013; Treuer et al. 2014; Wehmeier et al. 2015; Emilsson et al. 2017), interviews (n = 3) (Thiruchelvam et al. 2001; Cormier 2012; Hebert et al. 2013), and focus group discussions (n = 4) (Charach et al. 2006; Brinkman et al. 2012; Coletti et al. 2012; Ahmed et al. 2017). A few studies (n = 4) used multiple measures (questionnaires and interviews) to examine factors affecting adherence (Gau et al. 2008; O'Callaghan 2014; Bijlenga et al. 2017; Schaefer et al. 2017), while a couple of studies used a combination of prescription records and interviews to collect data (Wong et al. 2009; Ayaz et al. 2014). The detailed description is presented in Table 2.
Studies examining factors affecting different phases of adherence
When the studies were screened against the ABC taxonomy, it was found that more than half of the studies (n = 27) examined the factors affecting implementation of medication taking (Thiruchelvam et al. 2001; Rieppi et al. 2002; Miller et al. 2004; Gau et al. 2006; Darredeau et al. 2007; Faraone et al. 2007; Safren et al. 2007; Thorell and Dahlström 2009; Barner et al. 2011; Sitholey et al. 2011; Kooij et al. 2013; Palli et al. 2012; Torgersen et al. 2012; Bahmanyar et al. 2013; Hebert et al. 2013; Hong et al. 2013; Ayaz et al. 2014; O'Callaghan 2014; Bali et al. 2015; Raman et al. 2015; Wehmeier et al. 2015; Semerci et al. 2016; Bhang et al. 2017; Bijlenga et al. 2017; Emilsson et al. 2017; Schaefer et al. 2017; Sleath et al. 2017). Only a handful of studies identified the factors affecting initiation (n = 6) (Charach et al. 2006; Brinkman et al. 2012; Coletti et al. 2012; Fiks et al. 2013; Hong et al. 2014; Li et al. 2017) and discontinuation (n = 5) (Wong et al. 2009; van den Ban et al. 2010; Toomey et al. 2012; Treuer et al. 2014; Hong et al. 2016) of ADHD medications. A few studies examined multiple phases of adherence such as initiation and implementation (n = 1) (Cormier 2012), initiation and discontinuation (n = 2) (Chen et al. 2011; Wang et al. 2016), and implementation and discontinuation (n = 6) (Monastra 2005; Gau et al. 2008; Atzori et al. 2009; Bejerot et al. 2010; Hodgkins et al. 2011; Sobanski et al. 2014). Only one study evaluated the factors affecting all three phases of adherence (n = 1) (Ahmed et al. 2017).
Factors affecting medication adherence in people with ADHD
This review found that multiple factors affect medication adherence in people with ADHD. A distinction has been made to differentiate the factors based on the phase of adherence (initiation, implementation, or discontinuation) defined by the ABC taxonomy (Fig. 2). This review also differentiated the factors affecting medication adherence in children, adolescents, and adults at each of the three phases (Table 3).
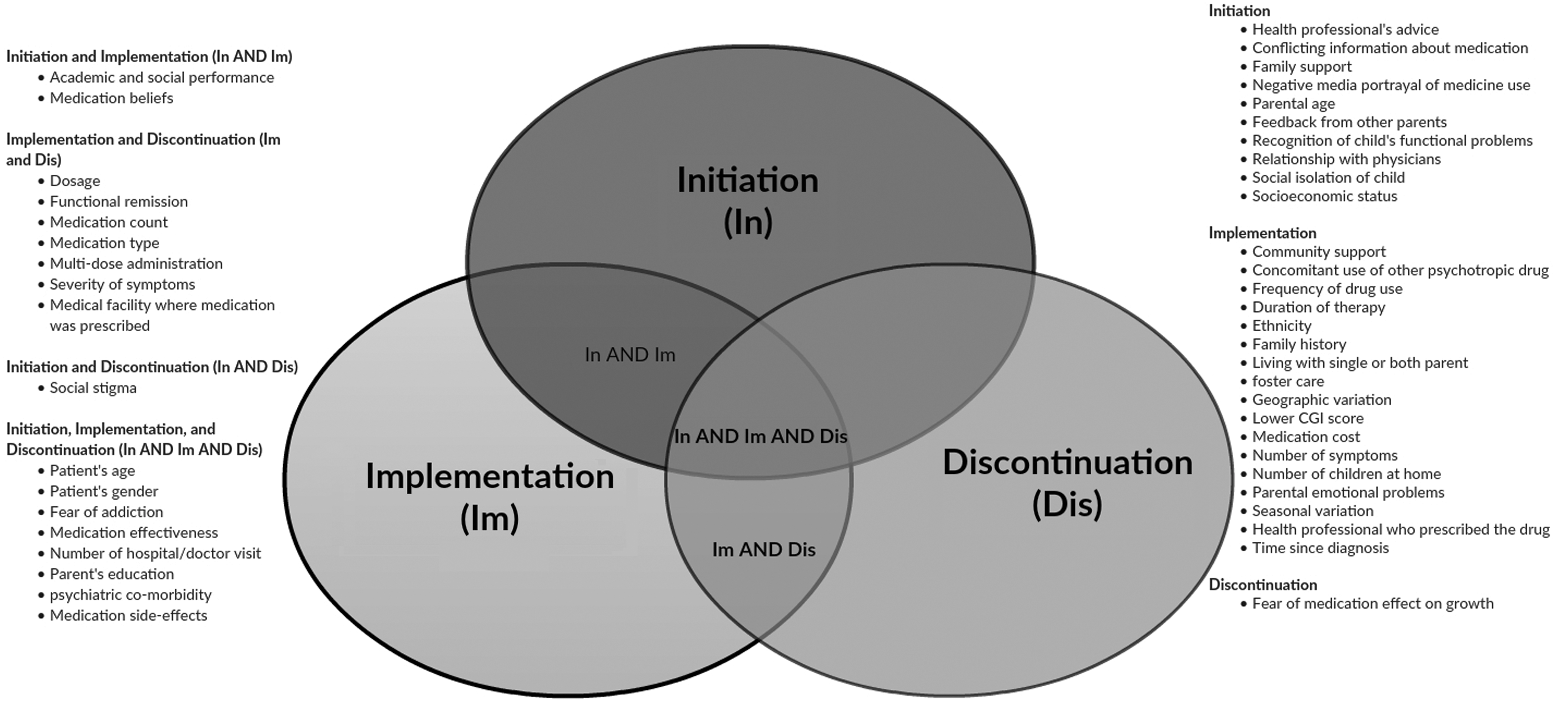
Factors influencing the three phases of medication adherence in patients with ADHD.
Factors Affecting Different Phases of Adherence in Patients with Attention-Deficit/Hyperactivity Disorder
Total number of studies are more than 45 as one study has included more than one group of population.
Charach et al. 2006; Brinkman et al. 2012; Cormier 2012; Coletti et al. 2012; Fiks et al. 2013; Ahmed et al. 2017.
Thiruchelvam et al. 2001; Rieppi et al. 2002; Miller et al. 2004; Faraone et al. 2007; Gau et al. 2008; Atzori et al. 2009; Thorell and Dahlström 2009; Barner et al. 2011; Hodgkins et al. 2011; Palli et al. 2012; Bahmanyar et al. 2013; Hong et al. 2013; Ayaz et al. 2014; Bali et al. 2015; Raman et al. 2015; Wehmeier et al. 2015; Bhang et al. 2017.
Miller et al. 2004; Gau et al. 2008; Atzori et al. 2009; Barner et al. 2011; Hodgkins et al. 2011; Palli et al. 2012; Bahmanyar et al. 2013; Hong et al. 2013; Ayaz et al. 2014; Bali et al. 2015; Wehmeier et al. 2015; Bhang et al. 2017; Emilsson et al. 2017; Schaefer et al. 2017; Sleath et al. 2017; Raman et al. 2018.
Darredeau et al. 2007; Safren et al. 2007; Bejerot et al. 2010; Hodgkins et al. 2011; Torgersen et al. 2012; Kooij et al. 2013; O'Callaghan et al. 2014; Sobanski et al. 2014; Semerci et al. 2016; Bijlenga et al. 2017; Li et al. 2017.
Thiruchelvam et al. 2001; Monastra 2005; Gau et al. 2006; Thorell and Dahlström 2009; Sitholey et al. 2011; Cormier 2012; Hebert et al. 2013; Ahmed et al. 2017.
Gau et al. 2008; Atzori et al. 2009; van den Ban et al. 2010; Hodgkins et al. 2011; Chen et al. 2011; Treuer et al. 2014; Hong et al. 2016; Wang et al. 2016.
Factors affecting the initiation phase of adherence
Medication beliefs and fear of side effects were the prominent parent-related factors reported by most studies. Negative beliefs were associated with lower rates of medication initiation (Brinkman et al. 2012; Coletti et al. 2012; Fiks et al. 2013). Similarly, fear of side effects negatively affected parents' decision to initiate medication (Charach et al. 2006; Brinkman et al. 2012; Coletti et al. 2012; Cormier 2012).
Three studies (Atzori et al. 2009; Chen et al. 2011; Wang et al. 2016) examined the factors affecting treatment initiation in children and adolescents with ADHD. Age, gender, and psychiatric comorbidity were the frequently reported factors that affected medication initiation. Two studies linked the presence of psychiatric comorbidity with a higher rate of medication initiation (Atzori et al. 2009; Wang et al. 2016). Older adolescents were more likely to initiate their medication than younger ones (Chen et al. 2011). One study [58] found that males were more likely to initiate medication, while another study (Atzori et al. 2009) predicted higher initiation rates among females. No study examined the factors associated with the initiation of medication in adults with ADHD.
Factors affecting the implementation phase of adherence
Medication effectiveness, side effects, and frequency of medication use were the frequently parent-related reported factors. Lack of medication effectiveness in terms of academic and social performance was associated with poor medication adherence (Thorell and Dahlström 2009; Sitholey et al. 2011; Hebert et al. 2013; Ahmed et al. 2017). Presence of side effects was also negatively associated with medication adherence (Monastra 2005; Sitholey et al. 2011; Cormier 2012). It was noted that the increased dosing frequency of medications resulted in poor medication adherence (Gau et al. 2006; Sitholey et al. 2011).
A total of 25 factors were identified among children. Age, psychiatric comorbidity, concomitant use of psychiatric medications, and medication type were the common factors identified in the studies. Younger age was associated with higher rates of adherence (Thiruchelvam et al. 2001; Miller et al. 2004; Faraone et al. 2007; Gau et al. 2008; Atzori et al. 2009; Hodgkins et al. 2011; Bahmanyar et al. 2013; Bhang et al. 2017). Two studies (Barner et al. 2011; Bhang et al. 2017) reported that nonstimulants were associated with higher adherence than stimulants, while other studies (Hodgkins et al. 2011; Raman et al. 2015) reported that the use of long-acting medications predicted higher adherence rates. Concomitant use of psychiatric medications also predicted higher adherence (Barner et al. 2011; Ayaz et al. 2014; Bali et al. 2015). Variation in findings was observed regarding the presence of psychiatric comorbidity and adherence. Four studies (Atzori et al. 2009; Palli et al. 2012; Bali et al. 2015; Bhang et al. 2017) predicted higher adherence in patients with psychiatric comorbidity, while two studies (Thiruchelvam et al. 2001; Bahmanyar et al. 2013) reported that the presence of comorbidity was associated with lower adherence.
A total of 23 factors were identified among adolescents. Age and psychiatric comorbidity were the most frequently identified factors. All but one study (Bhang et al. 2017) reported younger age to be highly associated with medication adherence (Miller et al. 2004; Gau et al. 2008; Atzori et al. 2009; Hodgkins et al. 2011; Bahmanyar et al. 2013; Ayaz et al. 2014). Similarly, except for one study (Bahmanyar et al. 2013), most studies reported the presence of psychiatric comorbidity to be associated with higher medication adherence during implementation phase (Atzori et al. 2009; Barner et al. 2011; Palli et al. 2012; Bahmanyar et al. 2013; Bali et al. 2015; Bhang et al. 2017).
Patient education and medication effectiveness were the common factors affecting adherence to medication in adult patients. Some studies demonstrated an association between medication effectiveness and higher adherence (Darredeau et al. 2007; Fiks et al. 2013), while other studies linked higher education with higher medication adherence in adult patients (Kooij et al. 2013; Semerci et al. 2016; Bijlenga et al. 2017).
Factors affecting the discontinuation phase of adherence
Medication discontinuation was associated with medication effectiveness and side effects among parents. Lack of effectiveness was associated with higher discontinuation rates (Monastra 2005; Toomey et al. 2012), while the presence of side effects also resulted in early medication discontinuation (Toomey et al. 2012; Ahmed et al. 2017).
Eight studies examined the factors affecting discontinuation among children with ADHD (Gau et al. 2008; Atzori et al. 2009; van den Ban et al. 2010; Chen et al. 2011; Hodgkins et al. 2011; Treuer et al. 2014; Hong et al. 2016; Wang et al. 2016). A total of 10 unique factors were identified. Psychiatric comorbidity and gender were found to be the most common factors identified in the studies. Female patients were more likely to discontinue their medication (van den Ban et al. 2010; Hodgkins et al. 2011; Wang et al. 2016). Patients with psychiatric comorbidity were also associated with early medication discontinuation (Hodgkins et al. 2011; Wang et al. 2016). Similar factors influenced medication adherence among adolescents and adults; however, the effect of these factors varied between studies. For example, females were more likely to discontinue their medication than males in adolescent and adult patients (Wong et al. 2009; Hodgkins et al. 2011; Wang et al. 2016) in contrast to another study (Fiks et al. 2013) in which males were more likely to discontinue medication than their female counterparts. Presence of psychiatric comorbidity was also associated with early discontinuation of medication among adolescents and adult patients (Bejerot et al. 2010; Hodgkins et al. 2011; Wang et al. 2016).
Discussion
Prior attempts have been made to review the factors affecting medication adherence in people with ADHD (Gajria et al. 2014; Treuer et al. 2016), but no efforts were made to identify the factors affecting the three phases of adherence. This review has summarized as much as possible the available literature and identified the factors affecting adherence at its three phases. This differentiation is essential to better understand the phenomenon of medication-taking behavior and to devise tailored interventions to improve medication adherence in people with ADHD.
This review observed a large variation in the criteria used to define adherence in the selected studies. The findings indicated that most studies focused on examining the factors affecting the implementation phase of adherence, while only a handful of studies focused on the initiation and discontinuation phase of adherence. Some unique factors were identified that affected the specific phases of adherence, while patient's age, gender, fear of addiction, medication effectiveness, parent's education, number of hospital visits, psychiatric comorbidity, and medication side effects influenced all three phases of adherence. This review also identified that factors affecting one phase of adherence differed with regards to different groups; that is, parents/carers, children, adolescents, and adults. Medication beliefs and fear of side effects were the main parental factors that affected the initiation of medication. In contrast, age, gender, and psychiatric comorbidity were frequently reported as the predictors of medication initiation among children and adolescents. For the implementation phase, factors such as medication effectiveness and side effects were related to parents, age and psychiatric comorbidity were associated with children and adolescents, while patient education and medication effectiveness were related to adults. Medication effectiveness and fear of side effects among parents mainly led to discontinuation of medication. Although gender was the common factor among children, adolescents, and adults that affected discontinuation, its effect on adherence varied between studies.
Definition of medication adherence and its phases
Included studies appeared to have used different definitions of the three phases of adherence. For example, Wang et al. (2016) and Ahmed et al. (2017) defined initiation as the commencement of therapy; however, Wang et al. (2016) considered commencement as the first prescription of ADHD medication, while Ahmed et al. (2017) considered commencement as the administration of medication. Different conceptual approaches were used to define implementation. Variations in the definition of implementation were not only evident between studies that used different conceptual approaches but also between studies that used the same conceptual approach. For example, when adherence during the implementation phase was defined as conformity to prescription with respect to dosage, one study (Gau et al. 2006) defined nonadherence as missing at least 1 dose on a school day on at least 2 days a week for 4 weeks, while another study (Hebert et al. 2013) defined nonadherence as missing more than 14 days of any dose on a daily basis for the past 1 month. Similarly, when implementation was defined as continuity of medication, some studies defined implementation as continuation of medication for 12 months (Monastra 2005; Atzori et al. 2009; Ayaz et al. 2014), while other studies defined implementation as continuation at 6 months (Raman et al. 2015) and 36 months (Torgersen et al. 2012). It is important to note that amongst studies that used 12 months as a cutoff period, some studies allowed a gap of 4 months (permissible time off medication) (Monastra 2005; Atzori et al. 2009), while another study allowed a gap of 3 months (Ayaz et al. 2014). Similarly, most studies (Wong et al. 2009; Toomey et al. 2012; Wang et al. 2016; Ahmed et al. 2017) defined discontinuation as the cessation of therapy; however, Wong et al. (2009) and Wang et al. (2016) considered cessation as not taking medication for at least 6 months, while Toomey et al. (2012) and Ahmed et al. (2017) did not use any cutoff period to define discontinuation.
Considerable variability was also observed among studies with regards to the definition of medication adherence, a finding consistent with the literature on adherence in other disease states (Hearnshaw and Lindenmeyer 2006; Banek et al. 2014). The lack of consensus on a definition of adherence in different disease states indicates that it is a universal issue amongst adherence research (Vermeire et al. 2001; Gebbia et al. 2012; Verbrugghe et al. 2013). Lack of consistency and uniformity in the use of operational definitions of medication adherence has hampered health outcome research in the past (Cramer et al. 2008). A considerable number of studies have examined the factors affecting the medication-taking behavior of people with ADHD, yet it is difficult to draw a meaningful conclusion from those findings because of the varied concepts and definitions of adherence used. There is a need to standardize the literature by developing a consensus on the use of the operational definition of medication adherence. The more transparent conceptual model of adherence (ABC taxonomy) proposed by Vrijens et al. (2012) should be considered for use in future research. A consensus was built on this model in the 13th European Consensus Meeting attended by participants from around the world (Vrijens et al. 2012). The use of this conceptual model will standardize the literature, provide a common platform for comparing and combining health research, aid in the development of tailored interventions to improve medication adherence, and promote health policy decisions based on consistent scientific evidence.
Variability in the definition of adherence phases in the literature has increased ambiguity in research findings. Despite a growing number of studies measuring adherence and examining factors influencing medication adherence in patients with ADHD, the ambiguity in research findings has halted the development of adherence research in ADHD population, which is evident by the lack of evidence-based intervention to improve medication adherence at its three phases. Standardization of adherence research using a common taxonomy and conceptual definition of adherence and its phases is important for the development of adherence research in ADHD.
Factors affecting medication adherence
This review found that while there are common factors that affect the three phases of adherence, there are also factors that are unique to each of the three phases of adherence. Studies in other disease populations have also identified different determinants for each adherence phase (Gillespie et al. 2017; Jensen et al. 2017). The primary reason for differences in factors affecting different phases of adherence is a clear distinction in the dynamics of the three phases that change over time. This needs to be given serious consideration while planning interventions to improve adherence and long-term medication outcomes for people with ADHD. More studies are required to investigate the influencing factors based on the phases of adherence.
The review also found variation in the factors within each phase of adherence based on the population being studied. For example, parental factors affecting initiation of medication were considerably different from the factors affecting the initiation in other groups. This finding is supported by other studies that have reported different barriers to adherence between children, adolescents, adults, and parents (McQuaid et al. 2003; Buchanan et al. 2012). Medication adherence among children presents unique challenges, which are different from those in adolescents and adults. The role of parents becomes crucial in this group as parents are mainly responsible for making health decisions. As children grow into adolescents they start to take responsibility for their own medications; however, parents still play an important role in this group. Growing awareness and physical, emotional, and cognitive changes present unique circumstances in adolescents compared to children and adults. To develop effective interventions, it is essential to identify unique adherence barriers impacting different groups in the population.
It is noteworthy to highlight the parental factors that affect medication initiation. Involvement of parents in the treatment process is essential for the successful management of ADHD (Swanson 2003). Therefore, it is essential to provide them information about the disorder, its management, and the likely side effects of medications (Ghanizadeh 2007) so that they can make informed decisions about the use of medications (Swanson 2003). Lack of knowledge leads to negative attitudes and beliefs of parents toward the disease and its management (Schommer 1990). This review found that the negative beliefs about medication and fear of side effects among parents were major obstacles toward achieving optimum medication adherence. These findings have potential implications for both clinicians and researchers. Parents visit clinics with the expectations that their children's condition will improve. However, negative beliefs about the medication may affect their medication-giving behavior and contribute negatively to medication adherence. This indicates the need for interventions to improve patients' understanding of the disease and the medication. One possible intervention could be the provision of education to parents about their children's symptoms and medications (Ferrin and Taylor 2011).
In contrast, age, gender, and psychiatric comorbidity were the common factors that affected medication initiation in children and adolescents. It is worthwhile highlighting the issue of treatment consideration in people with ADHD and psychiatric comorbidities. Some studies have reported that improvements in comorbid psychiatric symptoms could be achieved with effective treatment of ADHD (Spencer et al. 2006; Adler and Nierenberg 2010), which therefore could facilitate adherence. On the contrary, there is also a risk that stimulants (which are the first-line options for ADHD) may lead to mood destabilization in patients with bipolar disorders (Bond et al. 2012), which could lead to reduced adherence or treatment cessation if experienced by the patient or not initiating treatment if the patient or parent believes in the possibility of mood destabilization occurring. This review shows that psychiatric comorbidities may increase the initiation of ADHD medication. This is likely due to more adverse behavioral outcomes in patients with comorbidities compared to people with ADHD alone (Cuffe et al. 2015) and, therefore, more likely for ADHD treatment to be initiated if positive psychiatric symptoms are expected. However, due to a limited number of studies, there is a need for further research in this area. Inconsistencies in findings were observed regarding the effect of gender on medication adherence, making it difficult to provide specific recommendations regarding the effect of gender on medication initiation in people with ADHD. This finding is in line with other studies that explored the effect of gender on medication adherence in other psychiatric and nonpsychiatric disease states (Ahmed and Aslani 2014).
Although more than half of the studies examined factors affecting the implementation phase of medication adherence, the results were not consistent. Inconsistencies in reported factors were not only observed between different groups (parents, children, adolescents, and adults) but also were apparent between the studies within the same population. Similarly, inconsistencies were observed for the discontinuation phase of adherence. However, it is of great importance to discuss the highly variable effects of gender on discontinuation. The possible reasons for the effect of gender were not mentioned in the individual studies; however, the literature suggests that factors contributing to the differences could be related to how adult males and females cope with the burden of managing a chronic disease (Nau et al. 2007). The evidence suggests that adult female patients often use inappropriate coping strategies due to their impulsive nature, which forces them to make an ill-thought decision than their peers (Rucklidge 2010). It is quite possible that their ability to misjudge the situation because of their impulsiveness may affect their medication-taking behavior. With regards to other disease states, studies have reported lower adherence among females with diabetes and cardiovascular complications, but the reasons for these differences have remained a source of speculation (Pittman et al. 2011). Theories have been put forward such as complexity of regimen, out-of-pocket expenses, appearances of side effects, social expectations, and priorities to explain the effect of gender on medication adherence (Manteuffel et al. 2014), but more studies are needed to understand the complicated quagmire of gender-related medication adherence in ADHD. Medication effectiveness was the common factor that affected the discontinuation of medication in all groups. These results are in accordance with previous studies in different disease states in which treatment effectiveness was linked to medication adherence (Osterberg and Blaschke 2005; Brunner et al. 2009; Brown and Bussell 2011). These findings support the importance of following up patients to ensure the effectiveness of medication and hence its adherence (Kav et al. 2008; Jimmy and Jose 2011). However, it is important to understand that the effectiveness of medication in ADHD depends very much on dose optimization. If not tailored according to patients' needs, it either results in a suboptimal response or may lead to side effects (Jensen 1999).
Gaps in the literature and future research
This review did not find any study that evaluated the factors affecting initiation of medications in adult patients with ADHD. This could be due to the lower proportion of new diagnoses of ADHD in adults (de Graaf et al. 2008). However, the prevalence of ADHD in adults has increased by more than threefold in recent times (Montejano et al. 2011), and perhaps more studies will be conducted in the future. Initiation studies are also very limited among children and adolescents. Although a good number of studies have examined the factors affecting the implementation phase of medication adherence, inconsistencies in findings warrant further research, in particular, the greater delineation between the factors influencing parents alone and those that influence children and adolescents directly and indirectly through their parents. In view of the relatively higher prevalence of ADHD in Australia (Graetz et al. 2001), limited data are available regarding adherence to medications. There is a significant need to bridge the knowledge gap in this area. The findings of this review suggest that future studies should examine the factors influencing adherence at each of the three phases of adherence. Within each phase, factors should be differentiated between parents, children, and adults as each population may have unique influencing factors. Moreover, future studies should examine the instruments/measures that can be used to measure adherence at each phase.
Limitations
The findings of this review should be considered in view of some limitations. Although an effort was made to improve the methodological rigor, no statistical techniques were used to synthesize the data due to the narrative nature of this review. Caution should be exercised while generalizing the findings of this review due to heterogeneity in designs, adherence measures, and definitions used in the selected studies. Although a number of factors influencing medication adherence were identified in this review, it is difficult to comment on the aggregate magnitude of these predictors in people with ADHD. Most of the studies focused on implementation phase; therefore, more data are available about predictors of adherence at the implementation phase. More than one-third of studies included children and adolescents as participants. Although a critique of individual studies was provided, no formal approach was undertaken to evaluate the quality of each study. Despite our efforts to differentiate the factors, there remains a possibility for overlap of the factors between the age groups. Gray literature, unpublished studies, and articles not written in the English language were not included for pragmatic reasons. Although a comprehensive 2-phase review process was executed for the selection of eligible studies, there is a possibility that some relevant publications may have been excluded inadvertently. Since there is no consensus on the terms used for adherence and its phases, the search was limited to the concept of adherence, compliance, medication taking, and the three phases of adherence (initiation, implementation, and discontinuation). This may have resulted in the omission of studies that have used other terms like medication acceptability and refusal.
Conclusion
This review found that factors influencing one phase of adherence are relatively different from the ones affecting other phases, while some overlap was also noted. Within each phase, different factors were identified for parents, children, adolescents, and adults, as well as factors that impact one or more groups.
Clinical Significance
The findings of this review should help health care professionals and policymakers plan targeted interventions to promote adherence at each of the three phases of adherence and, for each phase, tailored to the needs of people with ADHD and their parents/carers.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.