
Abstract

We would like to respond to points raised by Strawn and Croarkin (Strawn and Croarkin 2018) regarding a placebo-controlled and fluoxetine-referenced study of desvenlafaxine in pediatric major depressive disorder (MDD) (Weihs et al. 2018). The study was classified as a “failed trial” because neither desvenlafaxine nor fluoxetine separated from placebo on the primary efficacy end point. A significant Clinical Global Impressions–Improvement (CGI-I) response for fluoxetine versus placebo (p = 0.017) was observed secondarily. In a letter to the editor, Strawn and Croarkin outlined aspects of the study design, including enrollment from a large number of low-recruiting sites, inclusion of few academic/hospital sites, and inclusion of principal investigators who had not completed a child and adolescent psychiatry (CAP) fellowship, which may limit the meaningfulness of the results.
We performed a post hoc analysis of the primary (Children's Depression Rating Scale—Revised [CDRS-R]) and secondary (CGI-I, CGI—Severity [CGI-S]) efficacy end points comparing treatment effects in patients from specialist (CAP principal investigator) versus nonspecialist sites, academic/hospital versus nonacademic sites, and high-recruitment (≥12 patients) versus low-recruitment sites to test these assertions. For CDRS-R and CGI-S, separate analysis of covariance models with terms for treatment, site type, and treatment by site type interaction showed no significant effect by treatment or site type, or their interaction, on change from baseline at week 8, consistent with the primary and key secondary results previously reported.
For CGI-I response, interactions between treatment and each site type were not significant in separate logistic regression models with terms for treatment, site type, and interaction. As shown in Figure 1, significantly higher week 8 CGI-I response rates were observed in patients who received fluoxetine versus placebo in high-recruiting (p = 0.029) but not low-recruiting sites and in nonacademic (p = 0.006) but not in academic sites (12% of patients). No significant difference between desvenlafaxine and placebo on CGI-I response was observed in any model; a significant difference in CGI-I response between specialist versus nonspecialist sites was observed in desvenlafaxine-treated patients (p = 0.007). In similar post hoc analyses conducted for a sister study (Atkinson et al. 2018) and for the studies combined, no significant effects of treatment were observed for any site type in the sister study. These results suggest that although larger effects of fluoxetine versus placebo on CGI-I response were noted in high-recruiting and nonacademic study sites, these variables did not appear to influence primary efficacy findings.
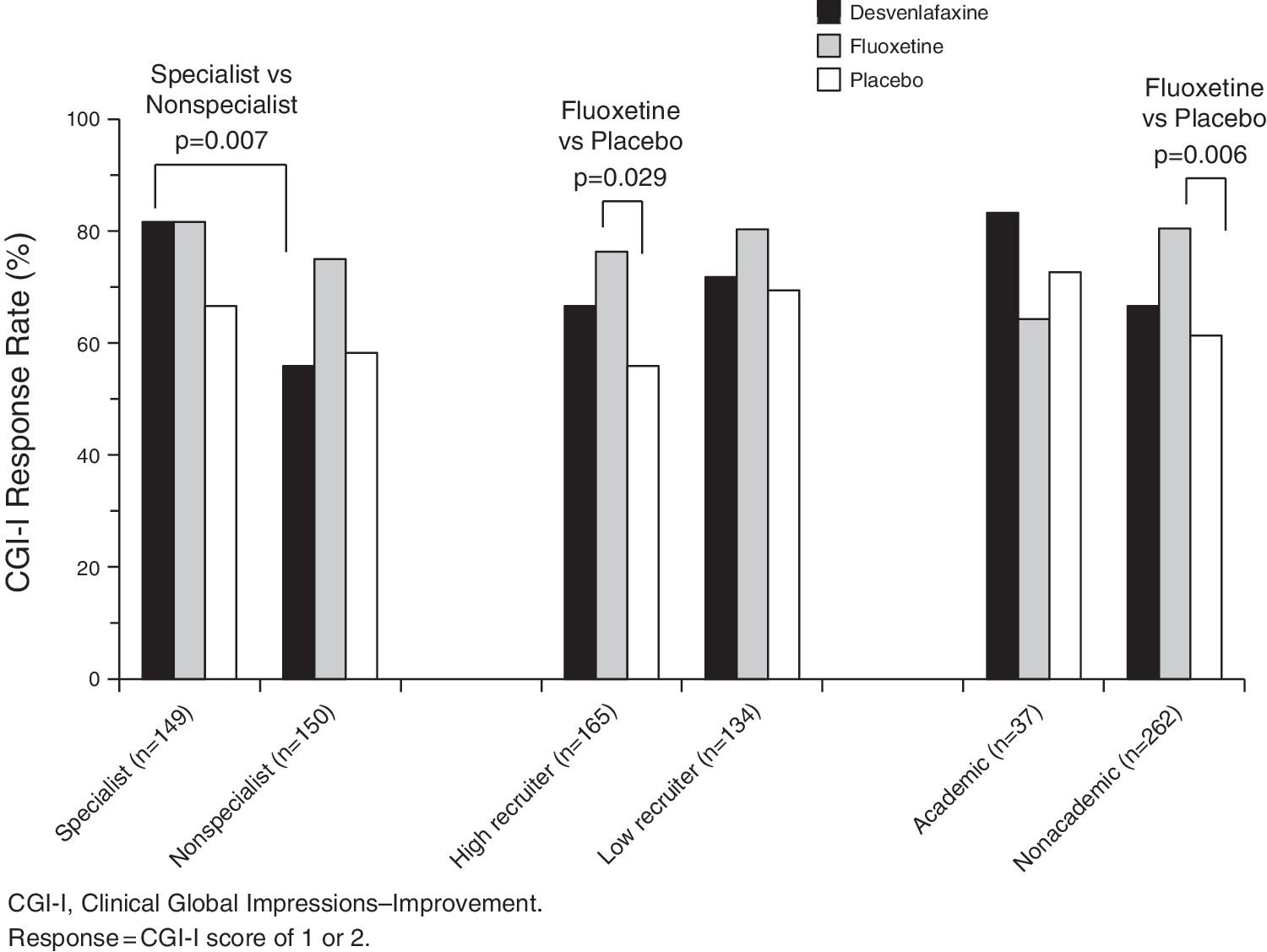
Rates of Clinical Global Impressions–Improvement response by study site variables; post hoc analysis. Study site variables did not appear to influence the primary efficacy findings.
Strawn and Croarkin further proposed that an insufficient fluoxetine dose was used. However, the 20 mg/day fluoxetine dose is consistent with fluoxetine labeling for pediatric MDD and has separated from placebo in two previous pediatric MDD trials (Emslie et al. 2002). Finally, Strawn and Croarkin suggest that expectation bias due to greater odds of assignment to active treatment versus placebo may have distorted study results. Given the challenge of placebo response in pediatric MDD trials, however, an active control arm to provide assay sensitivity remains an important consideration. Nonetheless, we agree there is an urgent need to solve the challenges facing pediatric psychopharmacology clinical trials.
Footnotes
Disclosures
K.L.W. received compensation from Pfizer, Inc. for her role as one of the principal investigators who conducted this study; received compensation in the past from Pfizer, Inc. and other pharmaceutical companies for her role as a principal investigator in numerous clinical trials; and has been a pharmacy and therapeutics consultant for CVS/Caremark. D.B.W., D.C., S.R., and P.C. are employees of Pfizer, Inc. and may hold stocks and stock options.