
Abstract
Objectives:
To estimate the number of patients who started methylphenidate during childhood and continued treatment beyond the age of 18 years and to study the determinants that may be associated with continuing treatment.
Methods:
Patients 17 years of age and younger who have received at least one prescription of methylphenidate were identified in the Integrated Primary Care Information database (1996–2017). Logistic regression analyses were performed to assess the association between potential determinants and continuation with methylphenidate treatment at the age of 18 years.
Results:
Fifty-three percent of all methylphenidate users (n = 1020) continued their treatment after the age of 18 years. Patients were more likely to continue treatment with methylphenidate if they started treatment at the age of 15–17 years compared with patients of 11 years and younger (adjusted odds ratio [OR]: 5.74, 95% confidence interval [CI]: 1.48–22.31), if they had a medication possession ratio (MPR) between 0.80 and 1.00 compared with a low MPR (adjusted OR: 2.18, 95% CI: 1.23–3.85) and if they lived in an area with a medium level of urbanization (adjusted OR: 1.98, 95% CI: 1.06–3.69). Furthermore, a relatively high number of patients had a MPR >1.0 (24.8%), of whom 91.3% started their treatment when they were between 15 and 17 years of age.
Conclusions:
Methylphenidate treatment initiated during childhood was continued in half of the study population when reaching the age of 18, where adolescents were more likely to continue treatment than young children. We also found that ∼25% of our study population had a MPR >1, mainly patients 15–17 years of age, which may suggest misuse or abuse of methylphenidate.
Introduction
One of the most common neurobehavioral disorders is attention-deficit/hyperactivity disorder (ADHD), affecting ∼5% of children worldwide and persisting into adulthood in the majority of the patients (Polanczyk et al. 2007). Stimulant medication such as methylphenidate is mostly prescribed as treatment for ADHD and the use of these drugs has increased over the past years (Ehrhardt et al. 2017). Until the beginning of the year 2018, methylphenidate was only approved in the Netherlands for children between 6 and 18 years of age because of the cardiovascular risk in adults (Jackson 2016). This is also one of the most important reasons that this drug was not approved for use in adults as previous studies have shown that they may increase heart rate and blood pressure and subsequently may lead to a slightly increased risk of myocardial infarction, sudden cardiac death, and stroke (Nissen 2006). Despite the fact that it was not approved for use in adults, there is a considerable degree of off-label use in this group (Nederlandse Vereniging voor Psychiatrie 2015; CBG-MEB 2017). Patients who have started ADHD drugs during childhood often continue treatment during adulthood, especially if they still suffer from symptoms and when the drug remains effective (Gajria et al. 2014). Previous studies have shown that ∼60% of children with ADHD demonstrated persistence of symptoms into their mid twenties (Biederman et al. 2000; Hurtig et al. 2007). In 2015, there were more than 57,000 patients 25 years of age and older who were using methylphenidate in the Netherlands (Hauck et al. 2017). A previous small study by McCarthy et al. (2012) showed that almost half of the study population in U.K. (n = 610) who started treatment in childhood were still on treatment at the age of 18 years or older. They also found that the probability of persistence was lower in females than in males when methylphenidate was initiated at a younger age, but the opposite was observed when treatment was started in adolescence. However, the numbers in this study were low and it is not clear if there are also other determinants that might be associated with persistence. Because of the cardiovascular risks in adulthood, it is important to investigate the determinants of off-label use.
Therefore, the objective of this study was to estimate the number of patients who started methylphenidate during childhood and adolescence and continued treatment beyond the age of 18 in the Netherlands in the period before it was approved for use in adults. In addition, we studied the determinants of continuing treatment with methylphenidate at the age of 18 years.
Methods
Setting
Data were obtained from the Integrated Primary Care Information (IPCI) database, a longitudinal observational dynamic database containing medical records from more than 450 general practitioners (GPs) throughout the Netherlands. The study population is representative of the Dutch population and contains medical records of ∼2,500,000 patients, including longitudinal data on demographics, symptoms, and diagnosis based on ICPC (International Classification of Primary Care) codes and free text, referrals, laboratory findings, discharge letters, and drug prescriptions. All general practices in IPCI are fully automated and prescriptions contain details on product name, daily dosage, ATC (Anatomical Therapeutical Chemical)-code (WHO Collaborating Center for Drug Statistics Methodology, 2016), and duration of use. Details of the database have also been published elsewhere (van der Lei et al. 1993; Vlug et al. 1999).
Study population
The study population consisted of all patients with active follow-up during the study period between January 1, 1996 until January 1, 2017 having at least 1 year of medical records available and a prescription for methylphenidate during the study period. Patients were only included if they started methylphenidate before the age of 18 years and if they reached the age of 19 years (to guarantee at least 1 year of follow-up during adulthood) before the end date of the study. The flowchart for children and adolescents included in the study is shown in Figure 1. All patients were followed from study entry until the end date of the study.
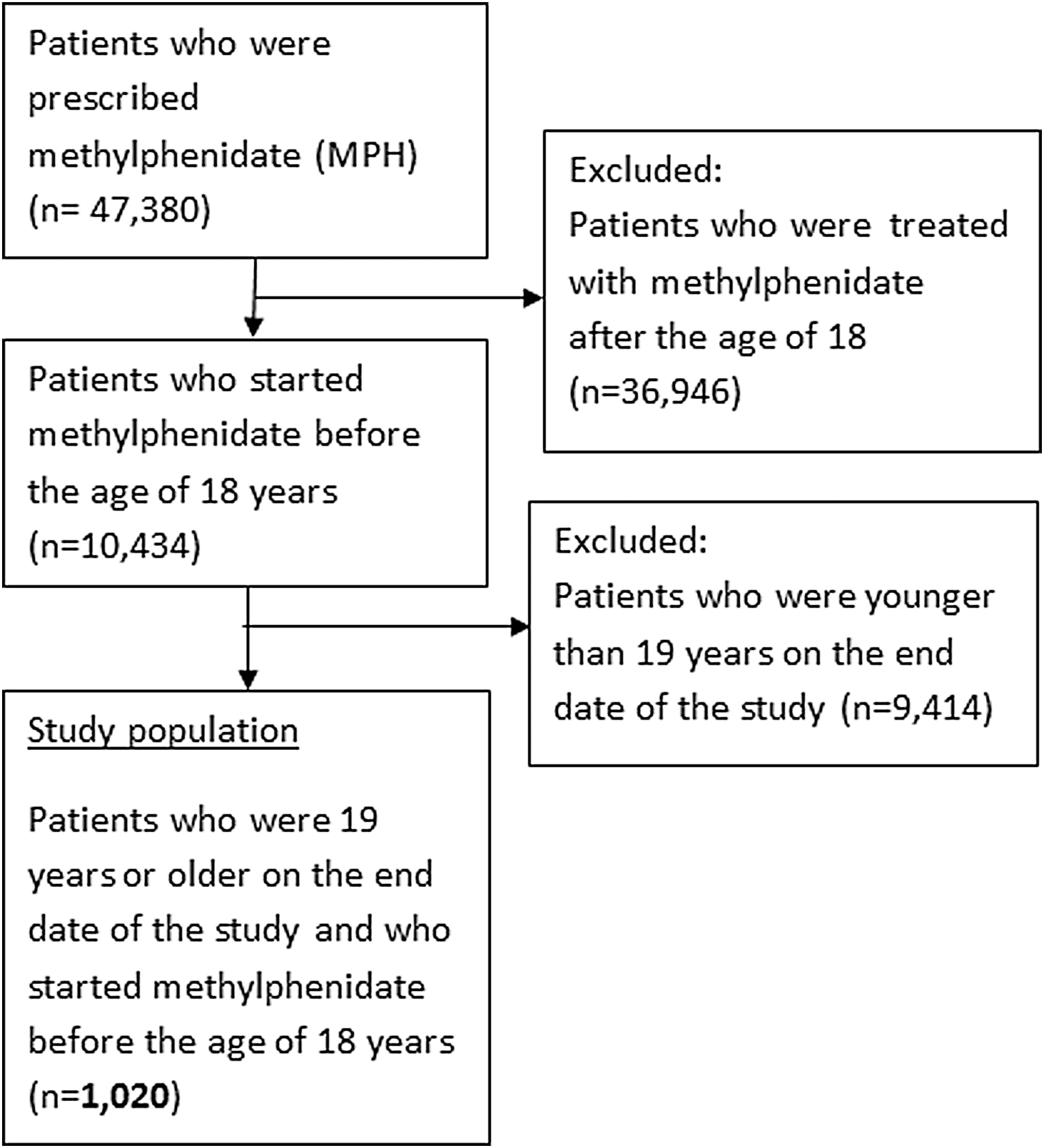
Selection process of the study population.
Case definition
In this nested case–control analysis in a cohort of methylphenidate users, cases were defined as users of methylphenidate who continued use beyond the age of 18 years while controls were users who had used methylphenidate during childhood or adolescence but discontinued treatment before the age of 18 years.
Covariates
For each patient, we retrieved information from the IPCI database on covariates such as sex and age of first prescription of methylphenidate, the duration of use which was calculated from the start date of methylphenidate treatment until the end date of treatment or age of 18 years (whichever came first), the number of different types of ADHD drugs that were prescribed (such as dexamphetamine and modafinil), and the use of other psychotropic drugs before the age of 18. Furthermore, we also included the presence of any potential contraindications for use of methylphenidate namely the presence of cardiovascular and cerebrovascular disease (cerebrovascular accident, heart failure, myocardial infarction) and psychiatric disorders, such as alcohol and drug abuse, somatization disorder, psychotic symptoms, depression, anorexia nervosa, compulsory disorder, anxiety, or suicide attempt. This comorbidity was assessed through disease-specific ICPC code searches. We also considered medication adherence as a potential determinant, which was measured by the medication possession ratio (MPR). The MPR was calculated by dividing the sum of the day's supply of methylphenidate during the study period by the difference between the first and end date of the last. According to international literature, a good adherence is set at a MPR of 0.80 or higher (Adler and Nierenberg 2010; Rolnick et al. 2013). The MPR was only calculated if patients received at least two prescriptions of methylphenidate. Finally, we considered demographic information, such as the living area: socially deprived area, and the urbanization level as potential determinants.
Analysis
Within the study population, we conducted a case–control analysis. As potential determinants, we included sex, age of first prescription (<12, 12–14 and 15–17 years), MPR, number of different types of ADHD drugs before reaching the age of 18 years, use of other psychotropic drugs before the age of 18, and the presence of any potential contraindications in the database before starting treatment with methylphenidate. We also included demographic information where we also considered the living area as potential determinants: socially deprived area (yes/no) and urbanization level (very high: >2500 addresses per km2, high: 1500–2500 addresses per km2, medium: 1000–1500 addresses per km2, low: 500–1000 addresses per km2, and not urban/rural: <500 addresses per km2). For the main analyses, we calculated the odds ratio (OR), with 95% confidence interval (CI) for each determinant associated with continuation of methylphenidate at the age of 18 years. We evaluated the potential determinants of continuation of methylphenidate at the age of 18 years through univariable logistic regression analysis. In addition, a multivariable logistic regression analysis was performed, including all univariably associated determinants. For those patients who continued treatment at the age of 18 years, we also determined the age when they will stop using methylphenidate. Results were considered statistically significant at p < 0.05. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY).
Results
In total, 47,380 patients were prescribed methylphenidate during the study period, where 78% of these patients were older than 18 years (prevalent users or patients starting methylphenidate beyond the age of 18). This group was excluded together with those who were younger than 19 years on the end date of the study (younger than 19 years, n = 9414). Overall, we identified 1020 patients who were prescribed methylphenidate before the age of 18 years of whom there were more males than females (males: 64.8% and females: 35.2%) (Table 1). The majority of the study population received their first methylphenidate prescription when they were between 15 and 17 years (86.9%). The majority of patients have been using methylphenidate for <6 months (55.5%), received one type of ADHD drug (90.9%), did not use any other psychotropic drugs before the age of 18 (87.3%), and did not have a contraindication before the start of treatment with methylphenidate (82.2%). Furthermore, the majority of patients lived in areas with a medium to high level of urbanization (very high: 12.2%, high: 24.6%, medium: 18.4%, low: 7.4%, not urban/rural: 4.3%) and in a nonsocially deprived area (yes: 5.5%, no: 89.3%). We also observed that a relatively high number of patients had a MPR <1.0 (24.8%) compared with the number of patients with a MPR of 1.0 and lower (<0.50: 21.3%, 0.50–0.79: 21.2% and 0.80–1.00: 13.9%). Of the patients with a MPR above 1 (n = 253), the majority had a MPR between 1.01 and 2.00 (n = 209) and a small part had a MPR <2 (n = 44). When stratified for age, we observed that 91.3% of these patients with a MPR above 1 started their treatment when they were between 15 and 17 years of age.
Characteristics of Patients Who Attained the Age of 18 Years and Were Prescribed Methylphenidate (n = 1020)
All numbers are given in n (%), unless stated otherwise.
Age of first prescription of methylphenidate.
MPR was only calculated for patients who received at least two prescriptions (n = 828).
The number of different ADHD drugs is based on the ATC7 codes.
Psychiatric disorders include alcohol and drug abuse, somatization disorder, psychotic symptoms, depression, anorexia nervosa, compulsory disorder, anxiety, or suicide attempt.
ADHD, attention-deficit/hyperactivity disorder; ATC, Anatomical Therapeutical Chemical; MPR, medication possession ratio.
In the multivariable analyses, we found that patients who started treatment at the age of 15–17 years were more likely to continue treatment with methylphenidate at the age of 18 years (adjusted OR: 5.74, 95% CI: 1.48–22.31) (Table 2). People with a MPR between 0.80 and 1.00 were also more likely to continue treatment compared with those with a MPR below 0.50 (adjusted OR: 2.18, 95% CI: 1.23–3.85). We also found that patients living in a medium level of urbanization were also more likely to continue use of methylphenidate beyond the age of 18 years (adjusted OR: 1.98, 95% CI: 1.06–3.69). Patients who continued treatment beyond the age of 18 (n = 542) received their last prescription for methylphenidate before the age of 21 (36.3%) and a small group stopped using methylphenidate when reaching the age of 25 (2.2%). For the majority of patients who continued treatment, it is not known at what age they received their last prescription of methylphenidate as the follow-up ended at the age of 19 years (and we do not know if they received a methylphenidate prescription after that) (61.4%).
Table 2. Determinants That Are Associated with Continued Use of Methylphenidate at the Age of 18 Years (n = 4050)
All numbers are given in n (%), unless stated otherwise.
Sex and variables with p < 0.05 in the univariable analysis were included in the multivariable analysis.
Age of first prescription of an ADHD drug (N06BA).
The MPR was only calculated if patients received at least two prescriptions of methylphenidate (n = 828).
The number of different ADHD drugs is based on the ATC7 codes.
Psychiatric disorders include alcohol and drug abuse, somatization disorder, psychotic symptoms, depression, anorexia nervosa, compulsory disorder, anxiety, or suicide attempt.
ADHD, attention-deficit/hyperactivity disorder; ATC, Anatomical Therapeutical Chemical; CI, confidence interval; MPR, medication possession ratio; OR, odds ratio.
Discussion
In this study, we found that a remarkably high percentage of patients older than 18 years were using methylphenidate. We also found that 53% of all methylphenidate users continued their treatment after the age of 18 years despite the fact that this was a relative contraindication as the drug was not licensed for use in adults during this study period. Previous studies have described concerns about cardiovascular safety in adult patients who are treated with methylphenidate (Schelleman et al. 2012; Jackson 2016). This drug was associated with an increased heart rate and blood pressure and previous studies have shown that even small increases in blood pressure and heart rate were associated with an increased risk of cardiovascular events (Vasan et al. 2001; Perret-Guillaume et al. 2009; Cooney et al. 2010; Liang et al. 2018). Furthermore, we observed that the majority of patients started treatment with methylphenidate at the age of 15–17 years and were more likely to continue their treatment at the age of 18. This observation could be explained by the small number of patients who initiated methylphenidate at a younger age. However, previous studies showed that the number of users in the Netherlands 16 years of age or older was increasing (SFK 2014, 2017). It may appear that more severe, later onset youth were treated in our study. However, it is more likely that the first choice of long-acting stimulants in adults as opposed to the first choice of short-acting treatment in children may explain these findings as the long-acting stimulants are associated with increased adherence (Nederlandse Vereniging voor Psychiatrie 2015). Despite the results where methylphenidate is more likely to be continued at 15–17 years of age, we also observed that the majority of patients who continued treatment at the age of 18 (within the study period), stopped using methylphenidate when reaching the age of 21 and the remaining group stopped before the age of 25. Similar findings were observed in a previous study, where they stopped treatment by age 21 (McCarthy et al. 2009). Patients may stop treatment when they experience less ADHD symptoms when reaching this age or because it was the patient's decision to discontinue medication (dislike of taking medications or the feeling of being able to cope without pharmacological treatment) (Faraone et al. 2006; Zetterqvist et al. 2013; Gajria et al. 2014).
Methylphenidate treatment is mostly initiated during childhood and some patients continue to use it in adulthood as they may still suffer from ADHD symptoms (Kessler et al. 2005). In our study, we observed that methylphenidate was continued in 53% of all methylphenidate users, which is higher than the number found in the study by McCarthy et al. (2012) (∼40%). This may be explained by the differences in drug prescribing between both countries, as the results of the study by McCarthy et al. (2012) also described higher estimates of ADHD drug prescribing in the Netherlands than U.K. In this study, they also found that the probability of persistence in females was lower compared with males when starting treatment at a younger age; however, the opposite was observed in patients who started their treatment in adolescence (McCarthy et al. 2012). In our study, relatively more women were included compared with the previous study, but we did not find a significant association with continued use for the different age groups and gender.
The results of our study also showed that more than half of the patients stopped treatment within 6 months, which is also the moment that patients have to see their physicians as part of the regular monitoring process (cardiovascular status or worsening of psychotic symptoms) for those who started treatment with methylphenidate (NHG 2018). At that moment, patients may stop their treatment due the adverse events or because the drug was ineffective (Pottegard et al. 2015; Brinkman et al. 2018). Another possibility is that they may be misdiagnosed as having ADHD. Even though it is a condition that has been studied extensively, the causes of ADHD remain poorly understood, which makes it difficult to make a correct ADHD diagnosis (Ford-Jones 2015).
It is not clear if the cardiovascular risks of these drugs are considered when deciding to stop or continue treatment with methylphenidate. We only found a small number of patients with cardiovascular disease in their medical history, but no significant associations were found.
In our study, we observed a relatively high number of patients with a MPR <1.0, especially in patients 15–17 years of age. A MPR above 1.0 may indicate that patients are taking more than the prescribed dose, but it may also indicate stock piling due to early refills or vacation supplies (Sperber et al. 2017). However, it is also important to emphasize the possibility that methylphenidate was used for other reasons than for the treatment of ADHD (Clemow 2017). A previous study has shown that the potential for abuse or misuse has increased along with the increase in prescribing frequency of methylphenidate (Cairns et al. 2016). Reasons for misuse of ADHD medication that were frequently reported are to improve attention, concentration, and alertness; to improve academic performances; and they are misused recreationally (Cairns et al. 2016; Clemow 2017). This may also be one of the explanations of the short-term use of methylphenidate in this age group as described earlier, which may be related to the need for treatment in alleviating difficulties in education instead of taking methylphenidate to treat ADHD-related symptoms (Weibel et al. 2019). These findings were also observed in a previous study conducted in Sweden (Bjerkeliet al. 2018). Furthermore, a previous study showed that misuse of short-acting methylphenidate is also more common than with the long-acting methylphenidate (Weyandt et al. 2014). The fact that only the short-acting methylphenidate is fully reimbursed in the Netherlands may have also influenced this. These data suggest close monitoring of methylphenidate use and dispensation of these drugs, in particular to patients 15 years of age and higher.
The main strength of our study is that we had access to a large real-life population-based cohort with detailed information on drug prescriptions and comorbidities over a long period of time. Furthermore, selection bias in our study is not likely as almost all inhabitants in the Netherlands are registered with one GP, where data are collected as part of routine patient care, irrespective of a research question. However, our study also has several limitations. First, there was no information available on dispensing by the pharmacy nor on actual drug intake. Second, we do not have (complete) information about the severity of the disease and therefore we may have included the less severe cases of depression or other disorders where the use of methylphenidate is contraindicated. Furthermore, the database may miss the prescriptions that are directly written by medical specialists. This database mainly contains GP prescriptions and also prescriptions that are initiated by the specialist and continued by the GP, but it is possible that not all prescriptions by medical specialists are captured in the database. However, in the Netherlands it is common practice for GPs to continue prescriptions when initiated by medical specialists, especially if it concerns drugs for chronic use. There is also the potential of selection where especially older children are selected, as the median active follow-up time in IPCI is relatively short (mean: 6.8 years, SD: 2.0 years), as our study only selected children who were followed until at least the age of 19 years. Previously published articles showed that the number of methylphenidate dispensations among people of 15 years and older have increased in the Netherlands and in other European countries (U.K., Denmark, and Germany) (SFK 2014, 2018; Bachmann et al. 2017). Furthermore, the lack of objective measures of ADHD and the changes over time may have influenced the findings as we did observe a higher percentage of patients continuing treatment beyond the age of 18 years in the period 2012–2016 compared with the previous 5 years. This can be explained by the increased ADHD recognition and treatment and the change in different prescribing patterns among different age groups and gender (van den Ban et al. 2010; Bachmann et al. 2017). Because these changes also occurred in other Western countries, we think that our results can be generalized to many of these countries. ADHD diagnosis and treatment with medication may be more accepted in the future by the general population as the attitude of parents and children toward ADHD has also changed. Treatment with medication can be considered by parents as a way to improve their child's achievements and performance at school. Also the children themselves may feel the need to use psychostimulants to improve their performance at school (Davidovitch et al. 2017). Furthermore, it is possible that treatment in girls may also increase in the future as ADHD diagnosis in this gender group may improve over time (Mowlem et al. 2019).
Conclusions
About half of the patients who were prescribed methylphenidate during childhood and adolescence continued their treatment in adulthood, which was considered as off-label use until recently. The majority of this population started their treatment in adolescence, which may explain the reason for continuing treatment at the age of 18 years. We also found that ∼25% of our study population had a MPR <1 (mainly patients 15–17 years of age), which may suggest misuse or abuse of methylphenidate.
Clinical Significance
The results of this study showed that more than half of the study population continued treatment with methylphenidate off-label when reaching the age of 18 years, despite the fact that use in adults was contraindicated because of cardiovascular risks.
Disclosures
K.M.C.V. works for a research group who in the past received unconditional grants from Yamanouchi, Pfizer, Boehringer-Ingelheim, Novartis, and GSK. None of these is related to the content of this article. R.H. is an employee of the PHARMO Institute for Drug Outcomes Research. This independent research institute performs financially supported studies for government and related health care authorities and several pharmaceutical companies. The other authors K.C., L.E.V., and B.H.S. declare that there is no conflict of interest regarding the publication of this article.