
Abstract
Objective:
Meta-analytic evidence shows alterations of peripheral inflammatory cytokines in adults with depressive disorders. By contrast, no evidence synthesis on alterations of peripheral inflammatory cytokines in children/adolescents with depressive disorders is available to date. To fill this gap, we conducted a systematic review and meta-analysis of case–control studies comparing serum cytokine levels in children/adolescents with depressive disorders and healthy controls.
Methods:
Based on a preregistered protocol (PROSPERO-CRD42018095418), we searched PubMed, Ovid, and Web of Knowledge from inception through July 21, 2018, with no language restrictions, and contacted study authors for unpublished data/information. Random-effects model was used to compute effect size for each cytokine. The Newcastle–Ottawa Scale was used to asses study bias.
Results:
From a pool of 4231 nonduplicate, potentially relevant references, 8 studies were retained for the qualitative synthesis and 5 for the meta-analysis. TNF-α was higher in participants with depressive disorders versus controls, falling short of statistical significance.
Conclusions:
Overall, due to the small number of studies, in contrast to the literature in adults, further evidence is needed to confirm possible inflammatory alterations associated with depression in youth.
Introduction
With a prevalence of 1%–2% in children and 2%–5% in adolescents, depressive disorders represent a major public health concern (Kessler et al. 2005; Thapar et al. 2012). Depressive disorders lead to substantial impairment in the personal and social functioning, and significantly increase the risk of suicidal ideation and behavior (Thapar et al. 2012). Intervention strategies for depressive disorders in youth include nonpharmacological treatments, in particular cognitive behavioral therapy and interpersonal therapy. Among medications, fluoxetine is so far the only compound supported by evidence, although its mean effect size was found to be moderate rather than large (Cipriani et al. 2016). Novel treatment approaches, such as glutamatergic modulation and noninvasive brain stimulation techniques including transcranial magnetic stimulation, transcranial direct current stimulation, cranial electrotherapy stimulation, and magnetic seizure therapy (Huan et al. 2017), have been poorly investigated in youth.
In terms of the etiology and pathogenesis underlying depressive disorders, while the monoamine hypothesis has been the mainstay over the past decades, alternative or complementary hypotheses have been put forward more recently. Neurobiological hypotheses for the pathophysiology of depression include the excitatory synapse hypothesis, involving changes in the glutamatergic system (Thompson et al. 2015) and the neurotrophic hypothesis, postulating a decreased neurotrophic support, leading to neuronal atrophy (Duman and Li 2012). Another relatively novel hypothesis relates to a possible role of inflammatory mechanisms as a contributor to the depressive symptomatology, at least in a subset of patients. Indeed, there is emerging evidence that (1) around one-third of individuals with depressive disorders present with elevated inflammatory cytokines; (2) patients with inflammatory conditions are at higher risk of depression; (3) cytokine-based treatments may induce depression; and (4) high markers of inflammation decrease the response to antidepressant medications (Leighton et al. 2018).
The increasing body of evidence on alterations of peripheral inflammatory cytokines in adults with depressive disorders has been quantitatively synthesized in a series of meta-analyses (Howren et al. 2009; Dowlati et al. 2010; Hiles et al. 2012a, 2012b; Liu et al. 2012; Haapakoski et al. 2015; Goldsmith et al. 2016; Kohler et al. 2017; Leighton et al. 2018). In the most recent and largest meta-analysis of cross-sectional and case–control studies (Kohler et al. 2017), peripheral levels of IL-6, TNF-α, IL-10, soluble IL-2 receptor, C-C chemokine ligand 2, IL-13, IL-18, IL-12, IL-1 receptor antagonist, and soluble TNF receptor 2 were found to be significantly more elevated in adults with depressive disorders compared with healthy controls. By contrast, peripheral levels of IL-1β, IL-2, IL-4, IL-8, the soluble IL-6 receptor, IL-5, CCL-3, IL-17, and TGF-β1 did not significantly differ between participants with depressive disorders and healthy controls. Alterations in peripheral inflammatory markers, in particular IL-6, have also been meta-analytically confirmed in the elderly with depressive disorder (Ng et al. 2018; Smith et al. 2018). Interestingly, there is also meta-analytic evidence that increased inflammatory markers increase the risk of subsequent development of depression (Valkanova et al. 2013).
While meta-analyses have been conducted for studies in adults, to our knowledge, no existing quantitative evidence synthesis of studies assessing inflammatory markers in children/adolescents with depressive disorders is available. To fill this knowledge gap, we conducted a systematic review and meta-analysis, including published and unpublished data, of case–control studies comparing peripheral cytokine levels in children or adolescents with depressive disorders versus controls without psychopathology. Given the exploratory nature of the study, no a priori hypotheses were formulated, but we expected findings to replicate, at least in part, those in the adult literature.
Methods
We followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Liberati et al. 2009). The protocol of this systematic review was registered in PROSPERO (CRD42018095418). Data were extracted from the published report (journal article) of the study or obtained from study authors.
Types of studies
We included case–control studies comparing serum levels of inflammatory cytokines in cases (children/adolescents with any depressive disorder) and healthy controls with no diagnosed psychopathology.
Types of participants
Inclusion criteria
These include children/adolescents (up to 18 years) with a categorical diagnosis of depressive disorder (any type of depressive disorder according to any version of the Diagnostic and Statistical Manual of Mental Disorders or International Classification of Diseases).
Exclusion criteria
These include children/adolescents with depressive symptoms not meeting formal diagnostic criteria for depressive disorders.
Outcomes
Difference observed in serum levels of the most commonly investigated cytokines (IL-1, 4, 6, 8, 10, TNF-α, and IFN-γ) between cases and controls.
Search strategy/syntax
The following electronic databases were searched until July 21, 2018, with no language/date/type of document restrictions: PubMed (MEDLINE), Ovid databases (PsycINFO, EMBASE+EMBASE classic, Ovid MEDLINE), and Web of Knowledge databases (Web of Science [science citation index expanded], Biological abstracts, Biosis, Food science and technology abstracts). Additional details on the search strategy/syntax, including search terms for each database, are reported in Supplemental Material S1. In addition, references of included studies were searched to identify potentially pertinent studies to supplement the electronic search.
Study selection
Retrieved references were independently screened and blindly double coded for eligibility by two authors. If consensus was not reached, any disagreement was arbitrated by a senior author. If needed, authors of included studies were contacted to provide missing/additional information.
Study quality/bias assessment
Study quality was assessed using the Newcastle–Ottawa Scale for case–control studies* focusing on the following: case definition, representativeness of the cases, selection of controls, definition of controls, comparability of cases and controls on the basis of the design or analysis, ascertainment of exposure and nonresponse rate.
Data extraction and statistical analysis
Data extraction was performed blindly by two of the authors, and discrepancies in data extraction were resolved through discussion with a third author until consensus was reached. Study authors were contacted when necessary to retrieve additional data. Data extracted from each study included first author, publication year, country where the study was conducted, participants' details, and study key findings.
Random-effects model was used to compute effect size for each cytokine. We calculated the standardized mean difference (SMD), with 95% confidence intervals (CIs), with the correction of Hedges (1981) to avoid bias due to sample size. The pooled SMD and the related 95% CI were calculated through the inverse variance method, and its statistical significance was assessed by the Z statistic. I 2 (Higgins and Thompson 2002) was calculated to quantify heterogeneity among studies. Finally, Egger's test (Egger et al. 1997) was used to evaluate publication bias. Analyses were performed using Comprehensive Meta-Analysis software.
Results
Studies included in the qualitative synthesis
From a pool of 4231 nonduplicate, potentially relevant references, 8 studies (Brambilla et al. 2004; Gabbay et al. 2009a, 2009b; Henje Blom et al. 2012; Byrne et al. 2013; Gariup et al. 2015; Pallavi et al. 2015; Miklowitz et al. 2016) were retained for the qualitative synthesis and 5 (Brambilla et al. 2004; Gabbay et al. 2009a, 2009b; Byrne et al. 2013; Miklowitz et al. 2016) for the meta-analysis. For three studies (Henje Blom et al. 2012; Gariup et al. 2015; Pallavi et al. 2015), data necessary for the meta-analysis were missing (even after contacting the authors to request them). A detailed description of the selection process is illustrated in Figure 1, showing the PRISMA flow diagram. Studies excluded, with reasons for exclusion, after full-text review are listed in Supplementary Table S1. Table 1 reports the main characteristics of studies included in the qualitative synthesis. Sample size ranged from 11 to 77. In all studies, depressive disorders were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria. Included studies were conducted in Europe, America, or Asia. Table 2 reports the key findings for each study included in the qualitative synthesis. Results of study quality/bias assessment are shown in Supplemental Material S2. Studies were scored out of 9; studies scoring 8 or 9 were regarded as being high quality, studies that scored 6 or 7 regarded as medium quality, and those scoring <6 regarded as low quality. Seventy-five percent of studies were of high quality, whereas 25% of studies were regarded as being of medium quality.
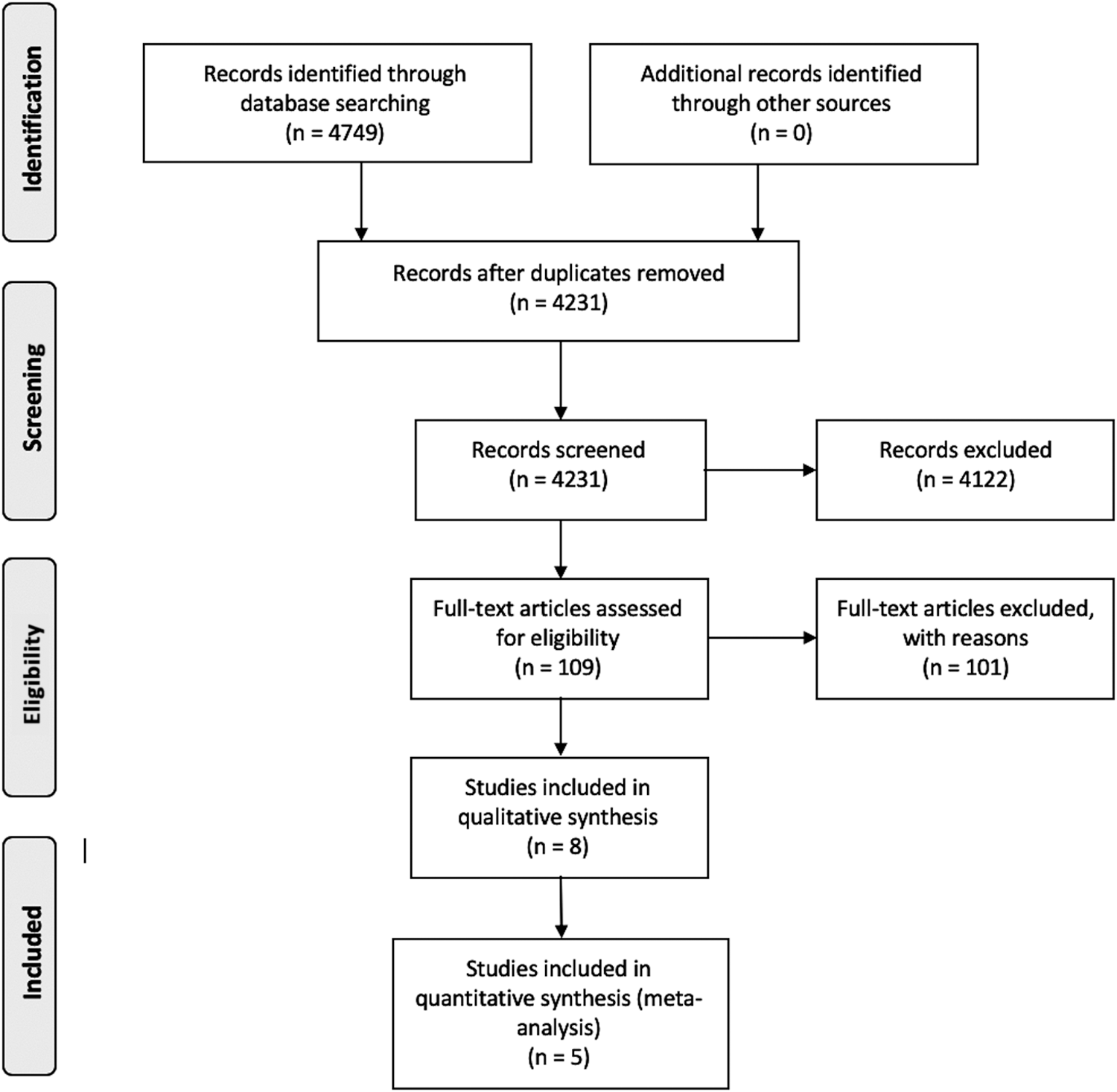
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
Characteristics of the Studies Included in the Qualitative Synthesis
DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; MDD, major depressive disorder.
Key Results for Each Study Included in the Qualitative Synthesis
SSRI, selective serotonin reuptake inhibitor.
With regard to specific study findings, three studies (Brambilla et al. 2004; Byrne et al. 2013; Miklowitz et al. 2016) did not find any significant differences between children/adolescents with major depressive disorder (MDD) and controls in any of the included cytokines (TNF-α and IL-1β; IL-1a, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12p70, IL-13, IL-17, IFN-c, TNF-α, and IFN-α2; IL-1β, IL-6, IL-8, TNF-α, and IL-10, respectively), although one of these studies (Brambilla et al. 2004) found that TNF-α and IL-1β were, respectively, significantly lower and higher in patients with dysthymia compared with controls. Two studies (Gabbay et al. 2009a; Gariup et al. 2015) found significantly higher cytokine levels in youth with MDD compared with controls (IFN-γ and IFN-γ/IL-4 ratio 9 plus a trend for IL-6; IL-6, IL-8, and IL-1β, respectively). One study (Pallavi et al. 2015) explored sex differences, reporting significantly higher levels of IL-2 in males with MDD compared with controls, and significantly increased values of IL-2 as well as IL-6 in females with MDD compared with controls. Another study (Gabbay et al. 2009b) explored the moderating role of suicidality, and found increased IFN-γ in both suicidal and nonsuicidal patients with MDD, and significantly decreased levels of TNF-α in suicidal compared with nonsuicidal patients with MDD. Finally, Henje Bloom et al. (2012) assessed the possible impact of treatment with selective serotonin reuptake inhibitor, and found significantly higher levels of IL-2, IL-6, and IL-1β in the untreated versus treated group, higher values of IL-2 only in treated versus controls, and significantly higher levels of IL-6 in nontreated compared with treated patients.
Meta-analysis
Five studies (Brambilla et al. 2004; Gabbay et al. 2009a, 2009b; Byrne et al. 2013; Miklowitz et al. 2016) were included in the meta-analysis. For three studies (Henje Blom et al. 2012; Gariup et al. 2015; Pallavi et al. 2015), data necessary for the meta-analysis were missing despite authors being contacted.
Data were pooled through meta-analysis when two or more studies were available for any cytokine. The results of the meta-analysis for each cytokine are summarized in Table 3. Forest plots and details regarding heterogeneity are reported in Supplemental Material S3. TNF-α values were higher in depressed versus nondepressed participants, falling short of statistical significance (SMD: 0.347, 95% CI = −0.005 to 0.699), with no heterogeneity (I 2 = 0%) and no evidence of publication bias (Egger's test, p = 0.013; Fig. 2). We did not find any significant difference between participants with depressive disorders and controls in any other cytokine included in the analysis (IFN-γ, IL-1 β, IL-4, IL-6, IL-8, and IL-10).
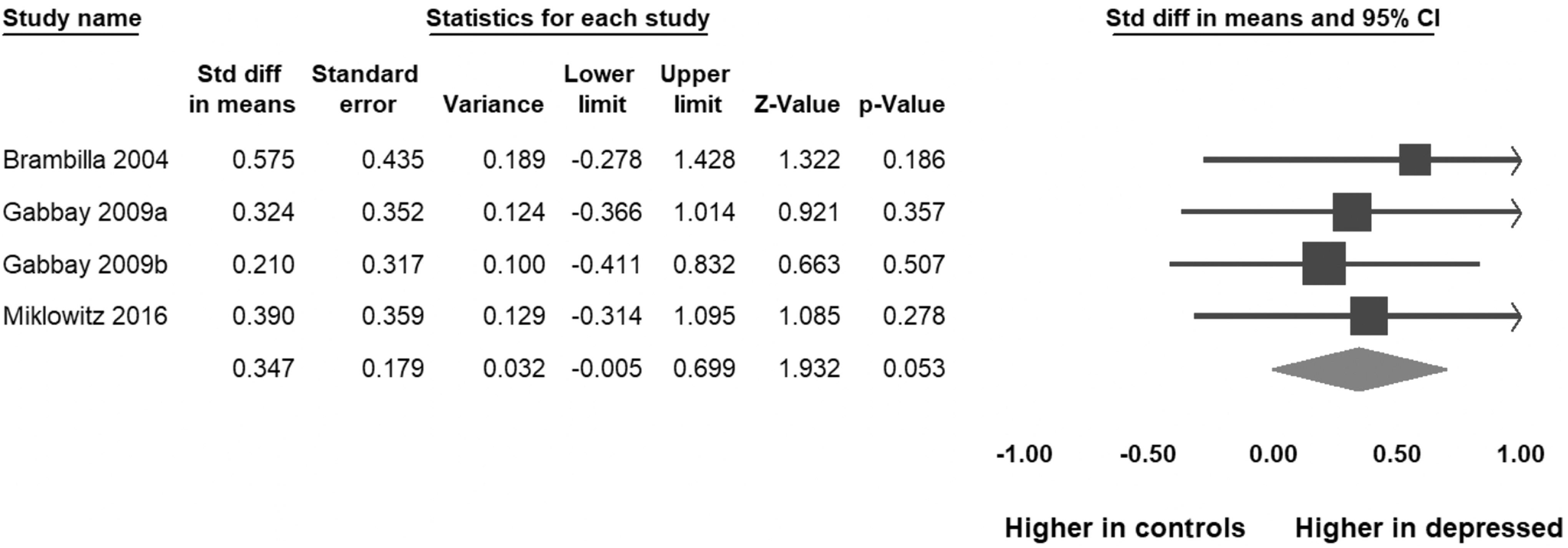
Forest plot for the meta-analysis of TNF-α. CI, confidence intervals.
Results of the Meta-Analysis
CI, confidence intervals; LL, lower limit; NA, Egger's test not applicable to two studies; SMD, standardized mean difference; UL, upper limit.
Discussion
To our knowledge, this is the first systematic review and meta-analysis focusing on peripheral inflammatory markers in children and adolescents with depressive disorders. We found that compared with healthy controls, participants with depressive disorders showed a trend for significantly higher levels of peripheral TNF-α. This cytokine is secreted by macrophages, mast cells, and natural killer cells to stimulate the release of inflammatory cytokines and prostaglandin from macrophages, which in turn contributes further to the inflammatory process (Lindemann 1991). In turn, increased levels of peripheral cytokines may reflect proinflammatory changes in the brain, as inflammatory cytokines may cross the blood–brain barrier (Banks et al. 2002). Of note, levels of other cytokines included in the meta-analysis (i.e., IFN-γ, IL-1β, IL-4, IL-6, IL-8, and IL-10) were not significantly different between subjects with and without depressive disorders. However, it should be noted that the number of studies (and total participants) included in the meta-analysis was low, therefore making it difficult to draw valid inferences. In particular, only two studies were available for IFN-γ, IL-4, IL-6, IL-8, and IL-10. While we deemed it useful to pool data even from two studies as there are no established minimum number of studies recommended to be included in a meta-analysis (Borenstein 2009) and data from two samples are more informative than one, our analyses might have been clearly underpowered to detect significant differences. Interestingly, the first meta-analysis, which included 24 studies, focusing on cytokines in adults with depressive disorders (Dowlati et al. 2010) detected significantly different levels of two cytokines only (i.e., TNF-α and IL-6), while the most recent and comprehensive meta-analysis, based on 82 studies, highlighted a large number of cytokines with significantly higher (IL-6, TNF-α, IL-10, soluble IL-2 receptor, C-C chemokine ligand 2, IL-13, IL-18, IL-12, IL-1 receptor antagonist, and soluble TNF receptor) in participants with depressive disorders compared with controls (Kohler et al. 2017). It is possible that this trend will be reflected in the literature related to pediatric depression. We would refrain from stating that our results support an imbalance between pro- and anti-inflammatory cytokines as this early distinction is likely to be oversimplistic, as it has been shown that IL-6 may contribute to both pro- and anti-inflammatory processes (Kohler et al. 2017).
In the adult literature (Dowlati et al. 2010), a number of factors have been identified as possible confounders or modifiers vis-a-vis the increased levels of inflammatory cytokines, including acute or chronic infectious diseases, psychiatric comorbidities, elevated body mass index, smoking, and pharmacological treatment (Miller and Raison 2016). While included studies ruled out acute or chronic diseases, due to the fact that they did not report subgroup analyses stratifying for the other possible confounders, we could not assess their impact in our meta-analysis. Furthermore, as shown in Table 1, the percentage of participants pharmacologically treated varied across studies, which may contribute to the heterogeneity reflected in the values of I 2. Other factors that may have increased interstudy heterogeneity include but are not limited to differences in the type of assay to measure cytokines (ranging from ELISA, to Radioimmunoassay and Multiplex Bead Array), laboratory practices, temperature in which blood was stored across studies. In addition, cytokines level varies diurnally, and so the time in which cytokines are measured could affect their expression (Byrne et al. 2013). Some studies did not specify the time in which blood was collected, which could explain the differences in findings between studies. Furthermore, the difference in the severity of depressive symptoms across studies may have further contributed to introduce heterogeneity. These aspects should be taken into account when interpreting our results.
Our results should be considered in the light of study strengths and limitations. As for the strengths, we conducted a comprehensive search across several databases with no restrictions to language or date of publication. We endeavored to contact study authors for additional data or information. We also used a state-of-the-art tool (Newcastle–Ottawa Scale) to rate possible study bias, which showed that in the majority of the studies there were no bias in terms of comparability between study groups. In addition, when feasible, Egger's test revealed that publication bias was unlikely in our analyses.
As for the limitations, due to the small number of studies we were underpowered to detect possible significant differences for a number of cytokines, and we could not conduct subgroup, sensitivity, and meta-regression analyses to test the possible role of confounders or mediators.
Overall, our systematic review and meta-analysis show that, in contrast to the literature in adults, the body of evidence on inflammatory alterations in children/adolescents is still limited, and no firm conclusions can be drawn based on available data. Therefore, further research aimed at understanding the possible involvement of inflammatory markers in pediatric depression and the possible related pathophysiological mechanisms is needed. In adults, it has been suggested that altered levels of cytokines may lead to hippocampal neurogenesis (Campbell et al. 2004), which could contribute to the reduction of the hippocampal volume found in major depression, although, due to developmental differences, the pathophysiological mechanisms may be different in children. Furthermore, brain areas affected by peripheral inflammation show a striking overlap with the network of areas implicated in the key deficits characteristic of MDD, including dysfunctional connections between the insula, the anterior and mid-cingulate cortex (Harrison 2017).
From a neuropsychological standpoint, there is evidence that inflammation is associated with exaggerated reactivity to negative information, altered reward reactivity, and somatic symptoms, key dysfunctions underpinning depression (Dooley et al. 2018).
In turn, this line of research could pave the way to pathophysiology-driven treatments based on adjunctive anti-inflammatory compounds for the treatment of depression in children and adolescents, which have been shown to be promising in adults (Kohler et al. 2016).
Conclusion
Overall, due to the small number of studies, in contrast to the literature in adults, further evidence is needed to confirm possible inflammatory alterations associated with depression in youth.
Clinical Significance
Research on inflammatory alterations in children and adolescents with depressive mood disorders may lead to novel therapeutic strategies.
Footnotes
Disclosures
G.M. was in advisory board with Angelini; has received research grants from Lundbeck, FB Health, and Humana Italia; and has been speaker for FB Health. S.C. declares reimbursement for travel and accommodation expenses from the Association for Child and Adolescent Central Health (ACAMH), a nonprofit organization, in relation to lectures delivered for ACAMH, and from Health care Convention for educational activity on attention-deficit/hyperactivity disorder. The other authors do not have conflicts of interest to declare.
Supplementary Material
Supplementary Material S1
Supplementary Material S2
Supplementary Material S3
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.