
Abstract
Objective:
To determine whether genetic variants in a pharmacokinetic gene (the number of CYP2C19 reduced function alleles [RFAs]), and in pharmacodynamic genes (HTR2A, SLC6A4, and GRIK4) influence sertraline tolerability and response in a cohort of pediatric patients with anxiety and depressive disorders.
Methods:
A retrospective analysis was performed using the electronic medical record data of 352 patients <19 years of age being treated for anxiety and/or depressive disorders with sertraline and who underwent routine clinical CYP2C19 genotyping. Additional genotyping and analysis of variants in HTR2A, SLC6A4, and GRIK4 were conducted for 249 patients. Multivariate regression models testing for associations with CYP2C19 were adjusted for concomitant use of interacting medications. Combinatorial classification and regression tree (CART) analyses containing all pharmacokinetic and pharmacodynamic genes and clinical factors were performed.
Results:
The maximum sertraline dose during the initial titration period of sertraline was inversely associated with the number of CYP2C19 RFAs and sertraline dose at 60 (p = 0.025) and 90 days (p = 0.025). HTR2A rs6313 was associated with sertraline dose (p = 0.011) and time to the average maximum sertraline dose (p = 0.039). Regarding efficacy, the number of CYP2C19 RFAs was not associated with the sertraline dose at the time of response (p = 0.22), whereas for the pharmacodynamic genes, only HTR2A rs6313 was associated with response dose (p = 0.022). An association was observed between predicted expression levels of SLC6A4 and the duration on sertraline (p = 0.025). Combinatorial CART and multivariate regression analyses implicated that pharmacodynamic genes and clinical factors influence the maximum sertraline dose and response dose. The total number of side effects was not associated with any of the variants tested.
Conclusion:
Both pharmacokinetic and pharmacodynamic factors, in addition to clinical and demographic components, influence sertraline dose, response, and tolerability, thereby necessitating further research to assess for the validity of these pharmacogenetic associations in children and adolescents.
Introduction
The efficacy and tolerability of selective serotonin reuptake inhibitors (SSRIs) in pediatric patients are variable and difficult to predict. Typically, only three in five patients with anxiety disorders (Walkup et al. 2008) or major depressive disorder (MDD) (March et al. 2004) respond to an initial SSRI trial. In addition, side effects are common in pediatric patients treated with SSRIs (Rynn et al. 2015; Luft et al. 2018). This variability in treatment response and tolerability in SSRI-treated children and adolescents is potentially related to multiple factors, including genetic variation affecting the medication target, the metabolism of the individual medication (pharmacokinetics), and/or the site of action (pharmacodynamics) (Ramsey 2018; Wehry et al. 2018). In this regard, accumulating pharmacogenetic and pharmacogenomic data implicate pharmacokinetically and pharmacodynamically relevant polymorphisms in these processes. Therefore, there has been considerable, but cautious, enthusiasm regarding the potential role of pharmacogenetics in optimizing treatment outcomes from psychotropic medications and SSRIs (Bousman and Muller 2018; Wehry et al. 2018; Zeier et al. 2018; Zubenko et al. 2018).
Among the SSRIs frequently used in pediatric patients, sertraline is commonly prescribed (Rynn et al. 2001; Bogetto et al. 2002; Walkup et al. 2008; Robb et al. 2010; Akpinar et al. 2016; Cipriani et al. 2016; Yuce-Artun et al. 2016) and effectively reduces anxiety (Rynn et al. 2001; Walkup et al. 2008) and depressive symptoms (Rynn et al. 2007) in children and adolescents. Despite being generally efficacious, not all pediatric patients respond adequately to sertraline, and a significant number of youth may experience sertraline-related adverse side effects (Rynn et al. 2015). Therefore, discontinuation due to intolerable side effects or a lack of efficacy is common (Rynn et al. 2001; Bogetto et al. 2002; Walkup et al. 2008; Robb et al. 2010; Akpinar et al. 2016). Notably, more than 25% of pediatric patients may discontinue sertraline, and in the largest prospective trial of sertraline in pediatric patients, nearly one-third of sertraline-treated patients experienced adverse events (Rynn et al. 2015).
Multiple hepatic, polymorphic cytochrome P450 enzymes metabolize sertraline, although the predominant enzyme is CYP2C19 (Obach et al. 2005; Probst-Schendzielorz et al. 2015). Polymorphisms in the CYP2C19 gene (e.g., reduced function, normal function, and increased function alleles) influence the efficiency of sertraline metabolism (Wang et al. 2001; Yuce-Artun et al. 2016) and plasma sertraline levels (Wang et al. 2001; Rudberg et al. 2008). This metabolic process involves N-demethylation followed by oxidative deamination, reduction, hydroxylation, and glucuronide conjugation (ZOLOFT 2019). Because of the direct relationship between genotype (e.g., alleles) and CYP2C19 activity, a patient's genotype corresponds to a metabolizer phenotype, with individuals being classified as a poor (PM), intermediate (IM), normal (NM), rapid (RM), or ultra-rapid metabolizer (UM) (Caudle et al. 2017).
There is evidence suggesting that pharmacogenetically-guided treatment may improve patient response and reduce side effects (Stingl et al. 2013; Winner et al. 2013; Perez et al. 2017; Greden et al. 2019). Currently, the Clinical Pharmacogenetics Implementation Consortium (CPIC) provides CYP2C19-dosing guidelines for sertraline in adults. These guidelines recommend clinicians start PMs at a lower dose and titrate to response or select an alternative medication not metabolized by CYP2C19. CPIC recommends sertraline be initiated at the “normal” starting dose for IMs and NMs, while for UMs, clinicians should initiate treatment at the recommended initial dose, but should switch to an alternative medication if patients fail to achieve response.
CPIC cautions applying these guidelines to pediatric patients, however, because the pharmacokinetic activity of CYP2C19 may be increased in children relative to adults (Hicks et al. 2015). In addition, all CPIC guidelines include a classification of recommendation based on the level of evidence, and the dosing recommendations for sertraline based on CYP2C19 phenotype are regarded as “optional,” adding that there is “room for differences in opinion as to the need for the recommended course of action” (Hicks et al. 2015).
Despite evidence of pharmacogenetic predictors of antidepressant tolerability and response in adults (McMahon et al. 2006; Paddock et al. 2007; Peters et al. 2009; Horstmann et al. 2010; Kato and Serretti 2010; Porcelli et al. 2012; Altar et al. 2013; Lohoff et al. 2013; Kato et al. 2013; Niitsu et al. 2013; Kawaguchi and Glatt 2014; Lin et al. 2014; Staeker et al. 2014; Hicks et al. 2015; Lett et al. 2016), limited data concerning pharmacogenetics and antidepressant response or tolerability in pediatric patients are available (Sakolsky et al. 2010; Gasso et al. 2018). In adults who were slower metabolizers or had more CYP2C19 reduced function alleles (RFAs), plasma sertraline concentrations were increased compared to NMs; however, plasma sertraline concentrations did not differ between faster CYP2C19 metabolizers and NMs (Wang et al. 2001; Rudberg et al. 2008). Similarly, pharmacokinetic models in adolescents showed that slower metabolizers had higher plasma sertraline concentrations compared to NMs based on standard dosing procedures (Strawn et al. 2019b). Taken together, these data indicate that both adults and adolescents who are slower metabolizers are at greater risk of experiencing side effects, but are more likely to respond to sertraline (Hicks et al. 2015). In addition, sertraline exposure appears to be related to age because older adults (e.g., patients >60 years) have higher plasma sertraline concentrations compared to younger adults (Reis et al. 2009; Unterecker et al. 2013). No difference in plasma sertraline concentrations were observed between children (e.g., patients 6–12 years), adolescents (e.g., patients 12–18 years), and adults (e.g., patients >18 years) (Alderman et al. 2006).
Several pharmacodynamic genes are also associated with SSRI response. These genes include the following: HTR2A, which encodes the 5-HT2A receptor; SLC6A4, the gene that encodes the serotonin transporter; and the glutamate ionotropic receptor kainite type subunit 4, GRIK4. A single-nucleotide polymorphism (SNP), rs7997012, in HTR2A has been implicated with antidepressant-related improvement in multiple studies (McMahon et al. 2006; Paddock et al. 2007; Peters et al. 2009; Lohoff et al. 2013; Niitsu et al. 2013; Lin et al. 2014; Gasso et al. 2018) and may be associated with increased risk of side effects in adults with MDD (Staeker et al. 2014), with the A allele encoding for improved likelihood of response. In addition, as reviewed by Lett et al. (2016), rs6313 in the HTR2A gene is associated with variable antidepressant response in adults with MDD (Lin et al. 2014), with the G allele encoding for improved probability of response. Not all studies, however, have observed associations between these alleles and both response and side effects in patients receiving antidepressants (Niitsu et al. 2013; Amitai et al. 2016).
SLC6A4 has been linked to variable antidepressant treatment response and side effects in some (Kato and Serretti 2010; Porcelli et al. 2012; Kato et al. 2013; Lohoff et al. 2013; Staeker et al. 2014), but not all (Ng et al. 2006) studies, with the long (L) and short (S) forms displaying high and low expression levels, respectively. Moreover, a SNP in the 5-HTTLPR region, rs25531, influences expression levels of the transporter, with the A allele being associated with increased expression levels and the G allele with lower expression levels (Hu et al. 2006).
In addition to serotonergically related genes, GRIK4 is associated with antidepressant response (Paddock et al. 2007; Horstmann et al. 2010; Sakolsky et al. 2010; Kawaguchi and Glatt 2014) as well as nonresponse (Perlis et al. 2010; Serretti et al. 2012), with the C allele of rs1954787 being associated with improved probability of response. Despite the inconsistencies in these findings, which could be due, in part, to the complex interactions between each gene's polymorphisms, these are still novel genes to investigate for pharmacogenetic associations. Further research is, therefore, necessary to determine the reliability of these associations, especially since they are included in many commercially available pharmacogenetic tests in combination (Altar et al. 2015).
We retrospectively analyzed the electronic medical record (EMR) data of youth diagnosed with anxiety and/or depressive disorders to determine if the number of CYP2C19 RFAs and variants in HTR2A, GRIK4, and SLC6A4 influence patient response and overall tolerability of sertraline. Based on pharmacogenetic studies in adults, we hypothesize that pediatric patients who had more CYP2C19 RFAs would be prescribed lower sertraline doses, experience greater dose-normalized effectiveness, and have more sertraline-related side effects compared to those with fewer CYP2C19 RFAs. In addition, we hypothesize that polymorphisms in HTR2A, SLC6A4, and GRIK4 influence treatment response and would be associated with variable tolerability in children and adolescents.
Methods
Subjects
Following Institutional Review Board approval, a query was utilized to determine and extract all data from eligible patients' EMRs at Cincinnati Children's Hospital Medical Center, who were tested for CYP2C19 alleles during admission into the inpatient psychiatry service and returned for follow-up in the outpatient clinic between January 2010 and May 2017. The procedure utilized in this study, including conditions for both the tolerability and response cohorts, emulates a study conducted by Aldrich et al. (2019), analyzing pediatric patients treated with citalopram or escitalopram. Inclusion criteria included the following: sertraline pharmacotherapy that was initiated at <19 years of age, presence of an anxiety and/or depressive disorder diagnosis, and CYP2C19 genotyping that was performed after September 1, 2013. Exclusion criteria included the following: a thyroid-stimulating hormone level of >5.5 mU/L or a diagnosis of a traumatic brain injury, substance use disorder, intellectual disability, congenital brain abnormality, or bipolar disorder.
Of the 369 prospective patients identified through the EMR query, 352 patients were included in the tolerability cohort and 199 patients were included in the response cohort, with 182 patients overlapping between these two groups. The sertraline treatment period was defined as the total number of consecutive days from the prescription start date to the end date. The concomitant use of 26 other psychotropic medications (e.g., bupropion, desvenlafaxine, duloxetine, fluoxetine, fluvoxamine, mirtazapine, escitalopram, citalopram, venlafaxine, aripiprazole, asenapine, lurasidone, olanzapine, paliperidone, prochlorperazine, quetiapine, risperidone, ziprasidone, alprazolam, buspirone, clobazam, clonazepam, clonidine, guanfacine, hydroxyzine, and lorazepam) and CYP2C19 inhibitors (e.g., oral contraceptives and omeprazole) was assessed for any overlap with the sertraline treatment period. The maximum sertraline dose was defined as the highest dose (mg/day) prescribed during the sertraline treatment period. Time to a dose >100 mg was calculated as the number of days between the date when sertraline was initiated and the first date when the maximum prescribed sertraline dose was greater than 100 mg. The reviewer was blind to CYP2C19 phenotype and the number of RFAs during data abstraction to avoid any potential bias.
Tolerability
The tolerability cohort encompassed patients who were prescribed sertraline for ≥1 day and had ≥1 recorded psychiatric encounter note within the sertraline treatment period. This study analyzed 10 side effects (e.g., activation, drowsiness, gastrointestinal symptoms, headache, hyperactivity, impulsivity, insomnia, irritability, nausea, and weight gain) and their related terms that had previously been reported in pediatric patients receiving sertraline (ZOLOFT 2019; Luft et al. 2018). These side effects and all related terms are located in Supplementary Data. Following a manual review of the EMR to identify common terms and phrases used to record the presence of side effects, an algorithm was developed to detect these side effects within each psychiatric encounter note, while excluding words that would come up as false positives. For example, hyperactivity returned a positive value with the presence of “restless,” “hyperactive,” “hyperactivity,” “mania,” and/or “hyperarousal,” whereas presence of phrases including “no hyperarousal,” “no restlessness,” “no mania,” or “Hyperactive: none” returned negative values. This algorithm was refined through secondary manual chart reviews to achieve a false positive rate of <10% for each side effect.
Furthermore, adherence to sertraline was assessed in the EMR using the same algorithm, where the treating clinician used a 0–4 numerical scale (0 = no concerns, 1 = mild concerns, 2 = moderate concerns, 3 = severe concerns, and 4 = very severe concerns). The presence of 1, 2, 3, or 4 in the EMR was categorized as nonadherence. Time to the first documented side effect associated with sertraline was defined as the number of days between the sertraline start date and first date the side effect was noted in the EMR during the sertraline treatment period. The total number of side effects was the collective number of side effects coded as being present during treatment with sertraline.
Response
The response cohort encompassed patients who were prescribed sertraline for at least 28 consecutive days and had one Clinical Global Impression-Improvement (CGI-I) score recorded by a clinician during the sertraline treatment period. The majority of patients returned for outpatient follow-up and CGI scores were obtained approximately every 60 days (median, 25th–75th percentile 24–101 days) by clinicians. In addition, the median number of CGI measures reported for each patient during the treatment period was 5 (range: 1–78). The CGI-I score assesses treatment response in patients using a 7-point scale, with “1” indicating the highest level of improvement and “7” indicating the highest level of deterioration (Guy 1976). This measurement tool has shown to be useful to clinicians in tracking patient progress and treatment response over time in the clinical setting (Busner and Targum 2007); also, this scale is frequently used at our institution in assessing treatment response in patients and has been utilized in other clinical trials of sertraline (Walkup et al. 2008; Robb et al. 2010; Akpinar et al. 2016; Perez et al. 2017). “Responders” achieved a CGI-I score of 1 ( = “very much improved”) or 2 ( = “much improved”); all other patients were classified as “nonresponders.” Time to response was the number of consecutive days between the date when sertraline was initiated and the first CGI-I score of 1 or 2. The response dose was the dose of sertraline (mg/day) being prescribed at the first CGI-I score of 1 or 2. The time to response dose was the number of days between the sertraline initiation date and the first date the response dose was prescribed.
CYP2C19 genotyping
During inpatient psychiatric admission, genomic DNA was routinely collected (through either phlebotomy or buccal swab sampling) using the MagNA Pure Compact System (Roche Applied Science, Indianapolis, IN). Patient CYP2C19 genotyping was performed in the College of American Pathologists (CAP) and Clinical Laboratory Improvement Amendments-certified Molecular Genetics Laboratory at Cincinnati Children's Hospital Medical Center (Cincinnati, OH). A report containing patient genotypes and metabolizer status (but not sertraline dosing recommendations) was uploaded into the EMR (Ramsey et al. 2019). Genotyping assessed for eight allelic variations in CYP2C19, which were determined using the TaqMan allelic discrimination system (Life Technology, Forest City, CA) on a low-density microarray. Of these eight allelic variations, there are seven categorized by CPIC as RFAs (*2, *3, *4, *5, *6, *7, and *8) and one increased function allele (*17) (Caudle et al. 2017). A normal function allele (*1) was inferred from the absence of the previous alleles (Ramsey et al. 2019). CPIC guidelines were used to assign a CYP2C19 metabolizer phenotype from the alleles present for each patient. Since there is no observed difference in plasma sertraline concentrations between NMs, RMs, and UMs (Wang et al. 2001; Rudberg et al. 2008), all associations with CYP2C19 were analyzed based on the number of RFAs rather than metabolizer phenotype. Therefore, PMs have two RFAs; IMs have one RFA; and NMs, RMs, and UMs have zero RFAs.
Pharmacodynamic gene genotyping
Patients' genomic DNAs, collected with consent for research and Institutional Review Board approval, were provided by the Discover Together Biobank, a CAP-accredited biorepository operating within our institution. HTR2A, GRIK4, and SLC6A4 were genotyped in patients with available blood samples (n = 249). Of these, 239 patients were included in the tolerability cohort and 147 were included in the response cohort, with 138 patients overlapping between groups. Genotyping for SNPs in HTR2A (rs7997012 and rs6313) and GRIK4 (rs1954787) was performed by quantitative PCR analysis using the StepOnePlus Real-Time PCR System (ThermoScientific, Wilmington, DE) and commercially available TaqMan assays (Applied Biosystems, CA). The rs25531 SNP variant and promoter length in SLC6A4 were assessed by restriction fragment length polymorphism analysis using PCR amplification, using the oligonucleotide primers described by Kraft et al. (2005) (forward primer: 5′-GGC GTT GCC GCT CTG AAT GC-3′; reverse primer: 5′-GAG GGA CTG AGC TGG ACA ACC AC-3′), followed by restriction digest with Mspl enzyme. The undigested and digested PCR products were electrophoresed on agarose gel and imaged using ethidium bromide staining and UV transillumination. Promoter length (L/S) and rs25531 SNP genotype (A/G) were then determined by comparing undigested and digested PCR product migration to that of an external standard (100 bp DNA ladder; ThermoScientific). The determined SLC6A4 genotypes were grouped into high (e.g., La and xLa) and low (e.g., Lg, Sg, Sa, and xLg) expression levels for analysis (Odgerel et al. 2013). For polymorphisms in HTR2A and GRIK4, no deviance from Hardy-Weinberg Equilibrium (χ 2) was observed. In addition, for the purpose of quality control, five samples from each pharmacodynamic gene were genotyped in duplicate with 100% concordance.
Statistics
Regression analyses were performed, where the number of CYP2C19 RFAs and genetic variants for HTR2A, SLC6A4, and GRIK4 were treated as ordinal predictors. One-way analysis of variance test for linear trend was used when assessing association with pharmacogenetic variants. Binary variables were analyzed using generalized linear regression models and continuous variables were analyzed using linear regression models in R version 3.2.2. Classification and regression tree (CART) analyses containing both genetic and clinical factors (e.g., age, sex, race, diagnosis, and number of concomitant medications) were utilized in R using the “rpart” package to reveal complex interactions between predictors. CART analyses operate by determining what variable best separates the independent variable into two groups, and then, this same process is applied independently to each subgroup until the data cannot be separated or improved further (Breiman et al. 1984).
Due to the inhibition of CYP2C19 activity caused by oral contraceptives (Carlsson et al. 2001; Reis et al. 2007) and the proton pump inhibitor omeprazole (Rocha et al. 2010; Gjestad et al. 2015), concomitant use of both medications were included in regression models assessing for associations between the number of CYP2C19 RFAs and treatment outcomes. In addition, concomitant psychotropic medications were included in all side effect-related regression models as an auxiliary factor without interaction to control for the algorithm's inability to differentiate sertraline treatment-related side effects from side effects associated with other psychotropic medications. Time to response dose and time to the average maximum sertraline dose were analyzed with either the log-rank test (for two treatment groups) or, when natural ordering was examined, with the log-rank test for trend (for three or more treatment groups) using Prism 7 for Windows (GraphPad, La Jolla, CA). The proportion of responders for all genetic variants was analyzed with the Chi-square test (χ 2) using Prism. Specifically for t-tests, a two-tailed p-value was utilized. All values are reported as the mean ± standard deviation, and p-values <0.05 were considered statistically significant.
Results
Patient characteristics
Demographic and clinical data for patients included in the tolerability and response analyses can be found in Table 1. The overall study cohort consisted largely of adolescents being treated for anxiety and depressive disorders, and we observed the expected racial distribution (based on our catchment area) and the expected predominance of females (Beesdo-Baum and Knappe 2012). For analyses including CYP2C19, the patient overlap between the tolerability and response cohorts was 182 patients, whereas the overlap between the tolerability and response cohorts for the pharmacodynamic genes was 138 patients. While the cohorts were similar in regard to demographics and treatment indication, the duration of sertraline treatment considered for pharmacogenetic analyses of tolerability was shorter than that used for pharmacogenetic analyses of patient response.
Clinical and Demographic Data of Tolerability and Response Cohorts
NA, not applicable.
Initial titration period of sertraline
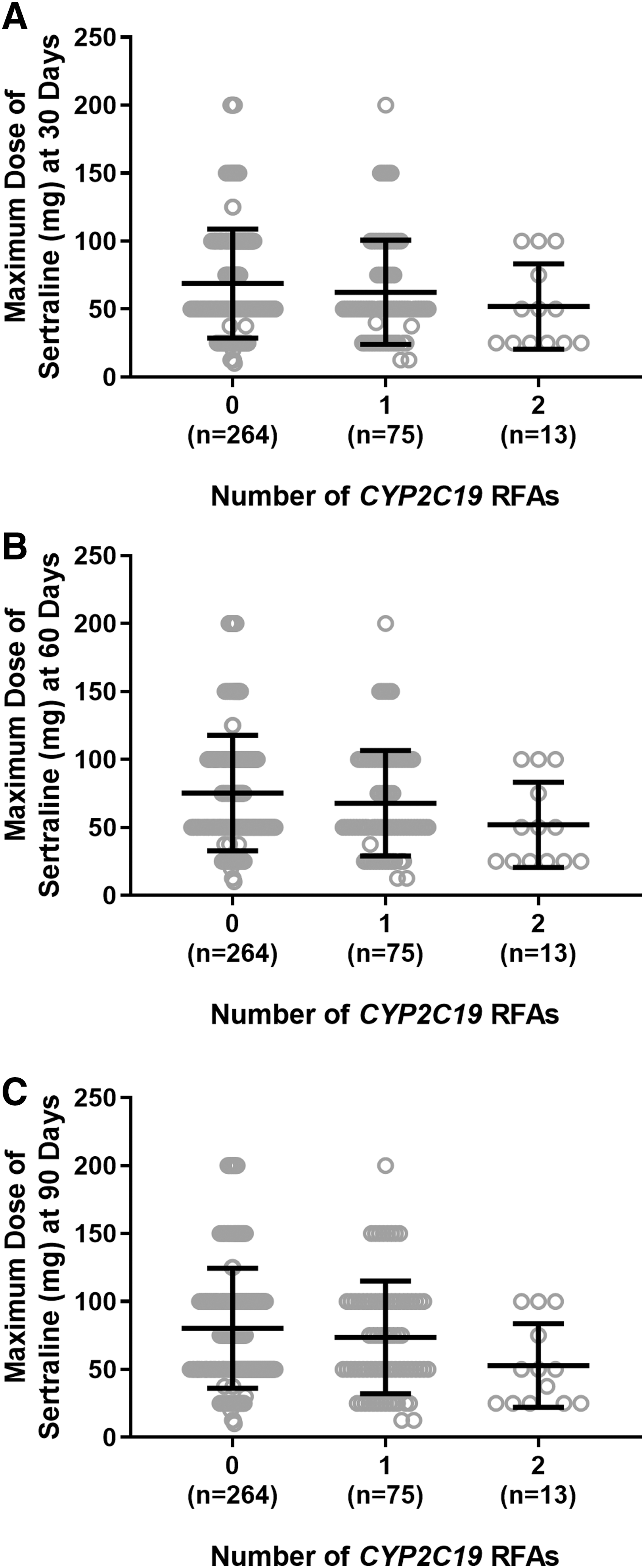
Regarding the maximum sertraline dose arrived at during the initial titration period (i.e., the first 30, 60, and 90 days of sertraline treatment), the number of CYP2C19 RFAs was not associated with dose during the first 30 days of sertraline treatment (p = 0.066, Fig. 1A). In contrast, the maximum sertraline dose was significantly associated with the number of CYP2C19 RFAs at 60 days (p = 0.025, Fig. 1B) and 90 days (p = 0.025, Fig. 1C) of treatment. As anticipated, the maximum dose of sertraline used was inversely related to the number of RFAs.
HTR2A and sertraline dosing
The rs6313 variant in HTR2A was associated with the maximum sertraline dose (p = 0.011, Fig. 2A), where patients with AA (n = 44) and AG (n = 108) genotypes were prescribed a higher maximum dose compared to those with GG (n = 87) genotypes. Post-hoc analysis revealed a significant difference in maximum sertraline dose between patients with AA and GG genotypes (p = 0.046, Tukey's multiple comparisons test). Time to the average maximum sertraline dose was also significantly associated with HTR2A rs6313 (p = 0.039, log-rank test for trend, Fig. 2B).
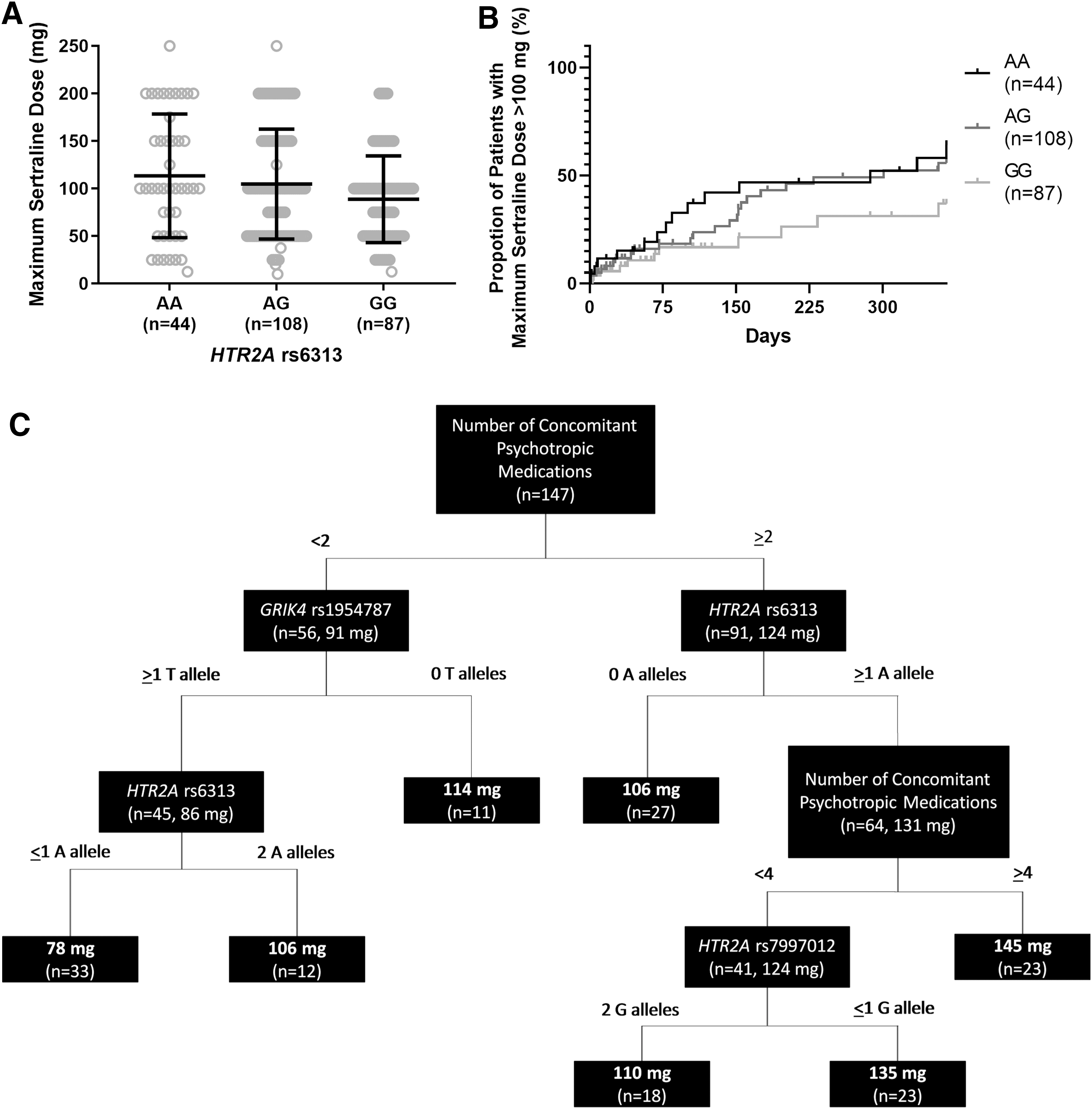
A multivariate regression model, including all pharmacokinetic and pharmacodynamic genes and clinical factors (e.g., age, sex, race, diagnosis, and number of concomitant medications), revealed that the rs6313 variant in HTR2A (p = 0.028) and the number of concomitant psychotropic medications (p = 0.002) were independently associated with the maximum sertraline dose. CART analysis of these genetic and clinical factors illustrates that in combination, GRIK4 rs1954787, HTR2A rs6313, and HTR2A rs7997012, and the number of concomitant psychotropic medications influence the maximum dose of sertraline (Fig. 2C).
CYP2C19 and response
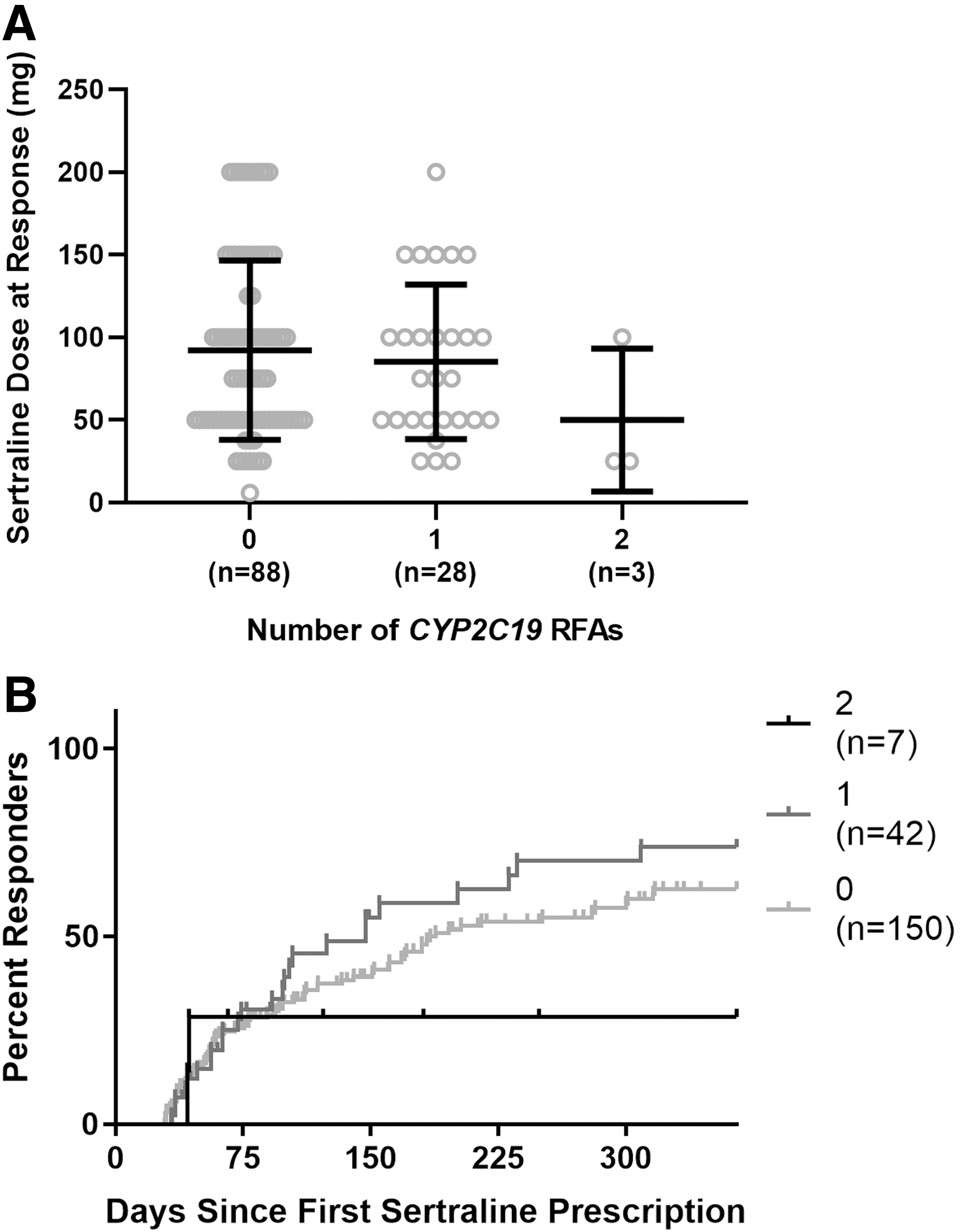
Analysis of the 199 patients included in the response cohort revealed that 61.3% (n = 122/199) responded (i.e., CGI-I score of 1 or 2, while prescribed sertraline). No association was observed between the sertraline dose at the time of response and the number of CYP2C19 RFAs (p = 0.22, Fig. 3A), and this remained insignificant when standardized for body weight (p = 0.29). In addition, the proportion of responders (p = 0.1, χ 2) and time to response (p = 0.73, log-rank test for trend, Fig. 3B) were not different among RFA groups.
Pharmacodynamic factors and response
Of the 147 individuals included, 60.5% (n = 89/147) responded. The rs6313 variant in HTR2A was associated with the sertraline dose at the time of response (p = 0.022, Fig. 4A) with the dose highest in patients with an AA genotype. When standardized with body weight at the time of response, the association remained significant (p = 0.034). This variant, however, was not related to time to response (p = 0.85, log-rank test for trend, Fig. 4B).
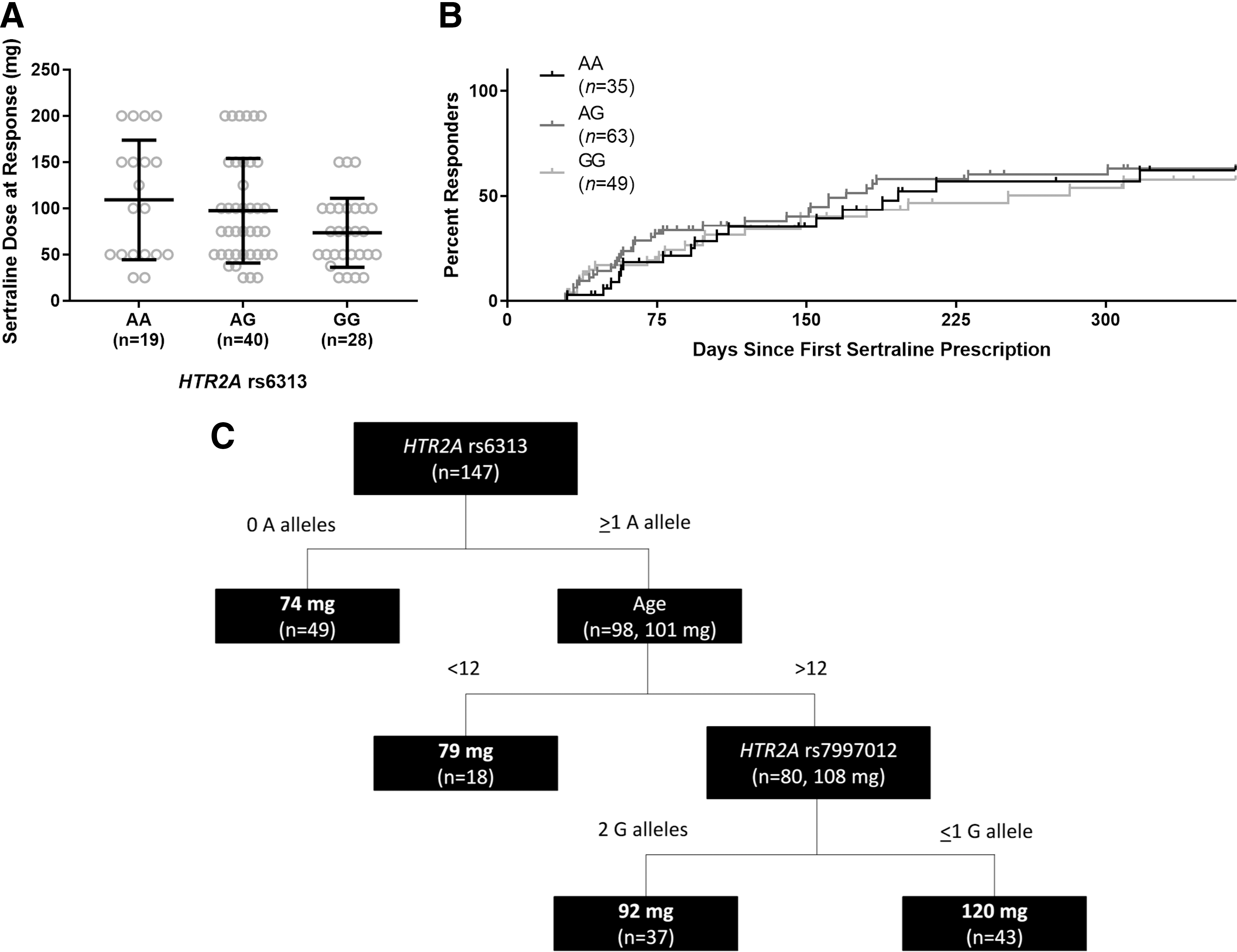
In a multivariate regression model, including all pharmacokinetic and pharmacodynamic genes and clinical factors (e.g., age, sex, race, diagnosis, and number of concomitant medications), HTR2A rs6313 (p = 0.008) and the number of concomitant psychotropic medications (p = 0.005) were implicated independently with variable response dose. Furthermore, combining these factors in a CART analysis elucidates the effect of age and HTR2A rs6313 and rs7997012 on the sertraline dose at response (Fig. 4C).
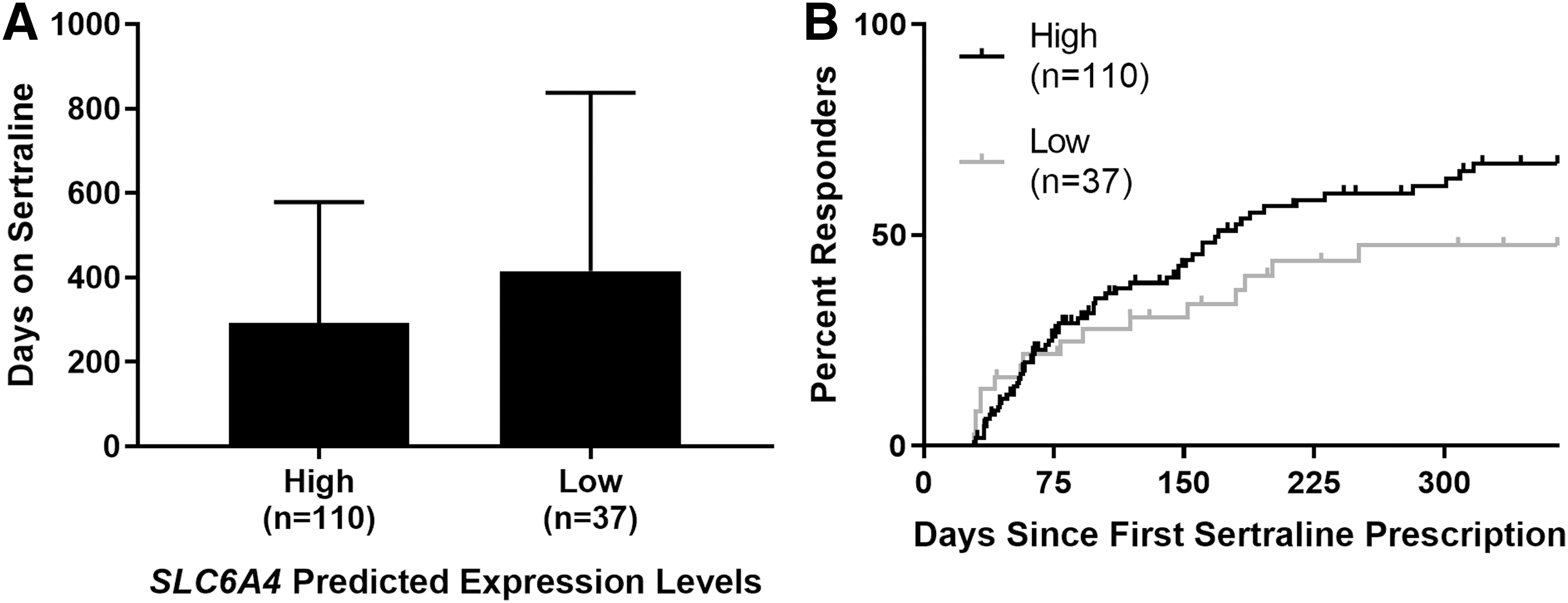
Predicted expression levels for SLC6A4 were associated with the duration of sertraline treatment, as patients with lower predicted levels of expression were treated with sertraline longer than those with higher predicted levels of expression (p = 0.025, t-test, Fig. 5A). Predicted expression levels for SLC6A4 were not associated with time to response (p = 0.15, log-rank test, Fig. 5B); also, the proportion of responders was unrelated to the level of SLC6A4 expression (p = 0.82, χ 2).
Sertraline tolerability
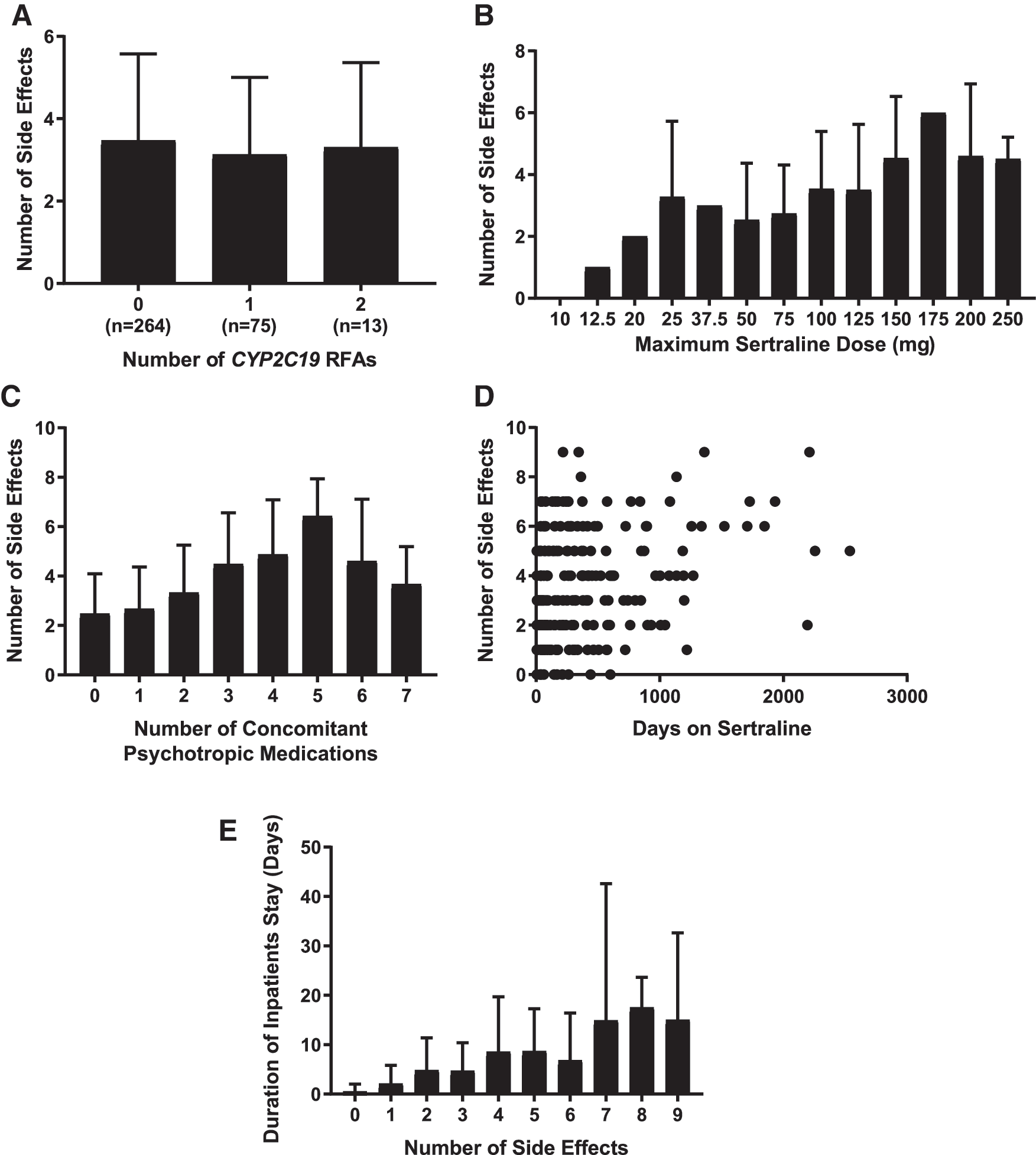
Of sertraline-treated children and adolescents, 94.3% (n = 332/352) experienced at least one side effect potentially associated with sertraline treatment (Table 2). While not related to the number of CYP2C19 RFAs (p = 0.24, Fig. 6A), the total number of side effects experienced was associated with the maximum sertraline dose (p = 0.001, Fig. 6B), the number of concomitant psychotropic medications (p = 2.54 × 10−9, Fig. 6C), the duration of sertraline treatment (p = 0.005, Fig. 6D), and the total duration of inpatient psychiatric hospitalization during the treatment period (p = 2.23 × 10−7, Fig. 6E) in a multivariate regression model.
In a multivariate regression model, the total number of side effects was not associated with
Prevalence of Side Effects in Tolerability Cohort by the Number of CYP2C19 Reduced Functioning Alleles (n = 352)
RFA, reduced functioning allele; GI, gastrointestinal.
Pharmacodynamic factors and tolerability
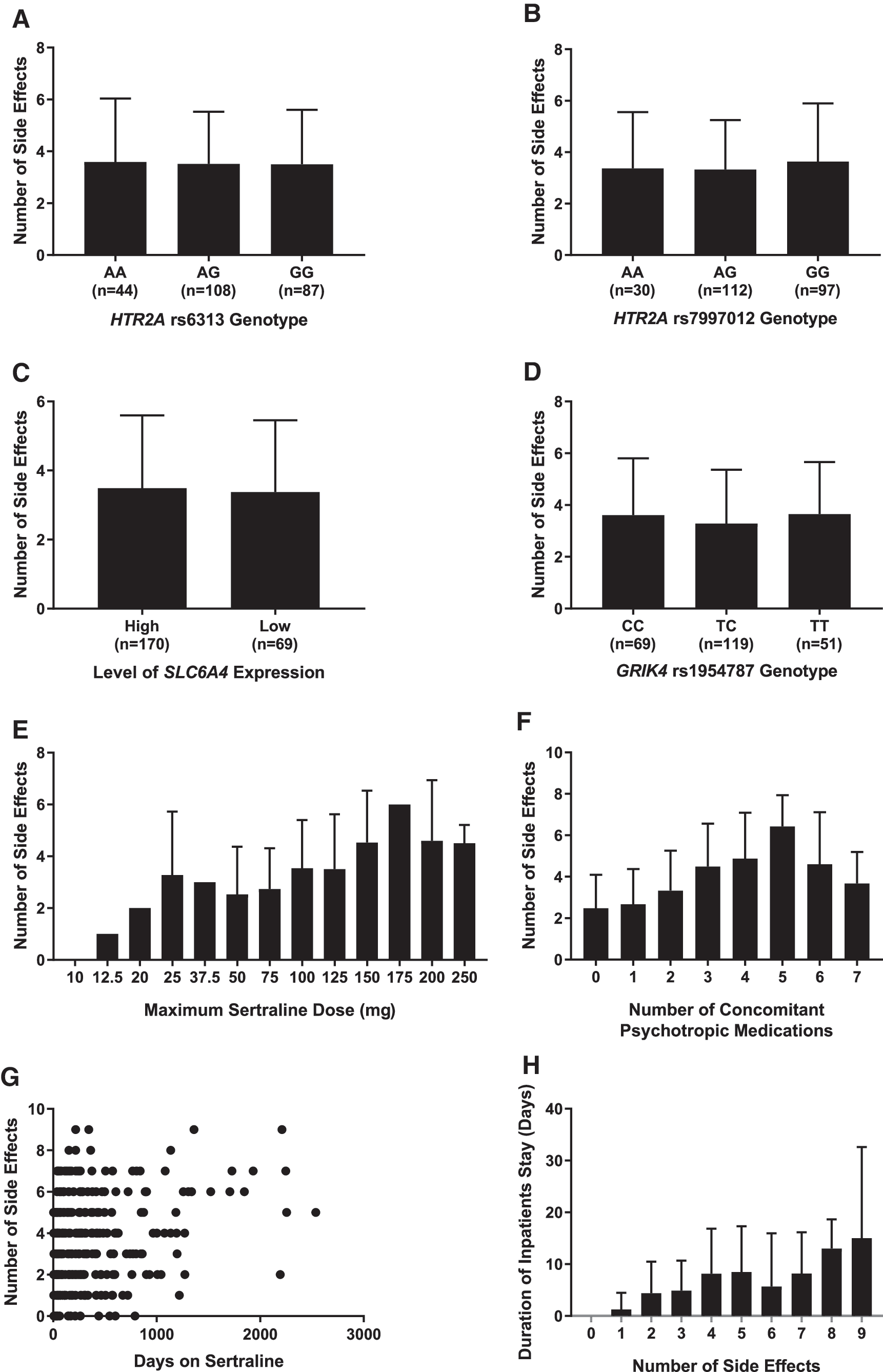
Among the 352 patients in the tolerability cohort, 239 had DNA evaluable for pharmacodynamic variant testing. There was a high proportion that experienced at least one side effect while treated with sertraline (94.9%, n = 227/239) (Table 3). In a multivariate model, the total number of side effects was not associated with any of the pharmacodynamic variants (i.e., HTR2A rs6313: p = 0.59, Fig. 7A; HTR2A rs7997012: p = 0.35, Fig. 7B; SLC6A4 predicted expression levels: p = 0.56, Fig. 7C; and GRIK4 rs1954787: p = 0.84, Fig. 7D) tested, but was positively associated with the maximum sertraline dose (p = 0.006, Fig. 7E), the number of concomitant psychotropic medications (p = 1.17 × 10−7, Fig. 7F), duration on sertraline (p = 0.01, Fig. 7G), and the total duration of inpatient psychiatric hospitalization during the treatment period (p = 2.45 × 10−6, Fig. 7H). Diagnosis was not related to the number of side effects.
In a multivariate regression model, the total number of side effects was not associated with
Prevalence of Side Effects in Tolerability Cohort for Each Pharmacodynamic Gene Variant (n = 239)
GI, gastrointestinal.
Discussion
This is a novel retrospective study utilizing EMR data to investigate pharmacogenetic polymorphisms related to sertraline pharmacokinetics and pharmacodynamics with treatment tolerability and efficacy in a pediatric population. The findings of this study suggest that the number of CYP2C19 RFAs, as well as polymorphisms in genes related to serotonergic (and possibly glutamatergic) transmission, correspond to differences in medication tolerability and response. In particular, CYP2C19 genotype appears to have influenced the titration of sertraline, while pharmacodynamic gene variants appear to have influenced the maximum utilized dose of sertraline, the titration of sertraline, the sertraline dose at the time of response, and sertraline tolerability.
During the initial titration period of sertraline, patients with two CYP2C19 RFAs were prescribed lower maximum doses compared to those with one RFA or zero RFAs within the first 60 and 90 days. This finding suggests that sertraline was more slowly titrated in slower metabolizers compared to faster metabolizers. While slower sertraline titration may delay therapeutic response in adults (Bogetto et al. 2002), in our cohort, patients with two RFAs experienced the opposite of this. This could likely be attributed to increased plasma sertraline concentrations in slower metabolizers, as has been observed in adults (Wang et al. 2001; Rudberg et al. 2008) and modeled in adolescents (Strawn et al. 2019b). This is also similar to a study of adult patients treated with risperidone whose dose was titrated differently by CYP2D6 metabolizer groups (Mas et al. 2012). It is also pertinent to mention that sertraline dosing guidelines were not included in the report uploaded into the EMR and would not have influenced the dose prescribed by the clinician.
The results reported for the rs6313 variant in HTR2A herein support prior studies showing that the G allele is associated with improved response to sertraline treatment (Lin et al. 2014). Regarding sertraline dosing, the maximum dose of sertraline was inversely related to the number of G alleles; patients with GG genotypes were titrated onto sertraline more slowly than patients with AA and AG genotypes; and the multivariate regression model and CART analysis showed that, even when including genetic and clinical factors, patients with more G alleles were prescribed a lower sertraline dose compared to patients with more A alleles. Moreover, the significant association between the rs6313 variant in HTR2A and the sertraline response dose shows that this polymorphism may underlie clinical improvement, where patients with the alleles encoding for better treatment response require a lower dose to achieve response. Still, while not completely unexpected since adult studies yield conflicting reports with antidepressants and SSRIs (Altar et al. 2013; Amitai et al. 2016), the time to response was not different for each genotype. It is important to note that genotyping results for the pharmacodynamic genes were not included in the report uploaded to the EMR and, therefore, would not have influenced the clinician in prescribing sertraline. The multivariate regression model and CART analysis looking at the sertraline dose at response further reinforces this association, indicating that the rs6313 polymorphism in HTR2A could explain some of the variability in treatment response. This CART analysis also showed that both pharmacodynamic and clinical factors, more than CYP2C19 genotype, explained why the response dose varied among patients. Altogether, these results support the evidence implicating the G allele of HTR2A rs6313 with improved response (Lin et al. 2014), in addition to the importance of studying pharmacokinetic and pharmacodynamic genes in combination. This supports the pharmacogenetic relevance of HTR2A and adds to the evidence associating treatment response with other pharmacodynamic genes, such as GRIK4, in children and adolescents (Sakolsky et al. 2010; Gasso et al. 2018). Further research is, therefore, necessary to confirm these findings.
The correlation between predicted expression levels in SLC6A4 and duration of sertraline treatment raises the possibility that patients with low levels of expression may have improved tolerability to sertraline compared to those with high levels of expression, contrary to prior antidepressant reports (Kato and Serretti 2010). Furthermore, in concordance with prior studies, patients with high or low levels of expression did not differ regarding how fast they responded (Ng et al. 2006), thereby recapitulating that the difference in duration on sertraline is most likely influenced by differences in tolerability. Notably, however, there was a divergence in the time to response after the initial titration period. Nevertheless, this finding adds to the work suggesting SLC6A4 influences tolerability (Staeker et al. 2014), thereby illustrating the novelty of this gene and that it should be evaluated further for pharmacogenetic significance.
The total number of side effects was not directly related to the number of CYP2C19 RFAs, although, after adjusting for RFA groups, it was correlated with sertraline dose. These findings contrast with studies of sertraline-treated adults in whom side effects are more common in slower CYP2C19 metabolizers (Wang et al. 2001; Rudberg et al. 2008; Hicks et al. 2015), which could be due, in part, to our study's naturalistic characteristics and low power. In addition, it is noteworthy that the frequency of sertraline-related side effects in this cohort was higher than in prospective, short-term, randomized controlled trials of sertraline in pediatric patients (Rynn et al. 2001; Walkup et al. 2008; Strawn et al. 2015), which could be related to the greater number of reporting opportunities in our study compared to short-term clinical trials, the multitude of neuropsychiatric medications our patients were receiving (median of two in addition to sertraline), or the algorithm utilized to determine side effects.
While this study assessed both pharmacokinetic and pharmacodynamic genes for associations with response and tolerability to sertraline in children and adolescents, several limitations warrant additional discussion. First, while our sample size was large, the number of patients with two RFAs for CYP2C19 was small (n = 13), increasing the potential for false discovery. Second, this was a retrospective study of patients receiving routine clinical care; thus, the assessment of side effects and efficacy varied considerably. Third, plasma sertraline concentrations at the time of response were not determined and, therefore, we cannot causally link increased or decreased sertraline concentrations at any dose with side effects or efficacy. Finally, the natural language processing algorithm that was leveraged to detect side effects, while efficient, may have limited our ability to differentiate side effects associated with concomitant medications and symptoms associated with the patient's primary psychiatric disorder despite manual review and controlling for concomitant psychotropic medication usage in our analysis.
Conclusion
CYP2C19 influenced the titration of sertraline, indicating prescribers were titrating patients who were slower metabolizers onto sertraline more slowly. Pharmacodynamic gene variants, particularly HTR2A rs6313, were also associated with sertraline dosing, including the titration of sertraline. In addition, while GRIK4 was not associated with sertraline tolerability and response, both HTR2A and SLC6A4 could influence tolerability and accelerate treatment response in pediatric patients. Pharmacogenetics-based dosing, in addition to clinical and demographic factors, should be considered by clinicians when prescribing sertraline to help optimize treatment outcomes. Continued research is needed to validate that these results influence treatment outcomes in pediatric patients, to develop personalized dosing or titration recommendations for children and adolescents based on CYP2C19, and to determine if sertraline dosing recommendations for HTR2A and SLC6A4 are warranted.
Clinical Significance
Sertraline response and tolerability vary significantly in pediatric patients with depressive and anxiety disorders, and genetic variants in pharmacokinetic and pharmacodynamic genes may partially explain this variability. While sertraline dose ranges are substantially larger compared to other antidepressants in the pediatric population (e.g., fluoxetine and escitalopram), slower CYP2C19 metabolizers (as reflected by the presence of RFAs) receive lower doses during the initial 60 and 90 days of medication titration. In addition, sertraline dose and rate of titration are associated with polymorphisms in HTR2A (i.e., rs6313). However, the relationship between antidepressant dose (and variability in dosing) and polymorphisms in pharmacokinetic/pharmacodynamic genes is complex (Wehry et al. 2018) and potentially subtended by tolerability. Moreover, antidepressant response and tolerability in pediatric patients covary (Strawn et al. 2019a) and likely influence one another. Thus, clinicians should continue to consider clinical and demographic predictors of response and tolerability in parallel with pharmacogenetic factors.
Footnotes
Acknowledgments
Samples, data, and/or services from the Discover Together Biobank at Cincinnati Children's Research Foundation were used in this study. We thank the Discover Together Biobank for support of this study, as well as patients and their families, whose help and participation made this work possible. In addition, we thank Jay Gholap, Diana Epperson, Bradley Owens, and Cynthia Prows for their contributions.
Disclosures
Dr. J.R.S. has received research support from the National Institutes of Health, Allergan, Edgemont Pharmaceuticals, Lundbeck, Neuronetics, and Shire. He has received material support from Genesight/Assurex and has provided consultation to Genesight/Assurex. He has received honoraria from CMEology and is an Associate Editor for Current Psychiatry and the Journal of Child and Adolescent Psychopharmacology, and receives royalties from UptoDate and Springer. Dr. L.B.R. has received travel support from the American Academy of Child and Adolescent Psychiatry. E.A.P., S.L.A., L.J.M., and D.H. have no financial conflicts of interest.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.