
Abstract
Objective:
The goal of this study was to characterize the frequency and trends of psychotropic drug prescribing in Canadian children from 2010 to 2016 and to compare these results with a previous study conducted between 2005 and 2009.
Methods:
Using a national physician panel survey database from IQVIA Canada, aggregated frequencies of written prescriptions and therapeutic indications for antipsychotics, attention-deficit/hyperactivity disorder (ADHD) medications (psychostimulants and nonstimulants), and antidepressants were analyzed in children. Changes in frequency of written prescriptions and therapeutic indications are presented using descriptive statistics.
Results:
Written prescriptions for antipsychotics decreased by 10% from 2010 to 2016, in contrast to a 114% increase in written prescriptions for antipsychotics observed between 2005 and 2009. Written prescriptions for psychostimulants and antidepressants rose by 35% and 27%, respectively, between 2012 and 2016, comparable with previous results. The most common reasons for recommending an antipsychotic were ADHD and conduct disorder, although there appears to be a downward trend for ADHD compared with other conditions. In contrast, the share of written prescriptions for antipsychotics for autism increased 34% over the study period. Within the second-generation antipsychotics, written prescriptions for aripiprazole increased. An increase in the use of guanfacine extended release for ADHD was also observed.
Conclusion:
Several factors may be involved in stabilization and small decrease in antipsychotic use in recent years, including physician and patient awareness of adverse effects related to antipsychotic use, knowledge implementation strategies advocating short-term and judicious use of antipsychotics in children, and the approval of guanfacine extended release for use in Canada for ADHD in 2013.
Introduction
The use of antipsychotic medications in children increased substantially between the 1990s and early 2000s, with multiple pharmacoepidemiological studies in Canada, the United States, and the United Kingdom demonstrating dramatic increases in the use of second-generation antipsychotics (SGAs) during this time period (Patel et al. 2002; Rani et al. 2008; Pringsheim et al. 2011b; Alessi-Severini et al. 2012). While the increase in use may be partly attributed to increased awareness and treatment of mental illness in youth, growth in antipsychotic use has greatly outpaced use of other medications for mental illness, including psychostimulants and antidepressants (Pringsheim et al. 2011b).
The use of antipsychotic medications was most prominently associated with the diagnosis of attention-deficit/hyperactivity disorder (ADHD), followed by conduct disorder in school-age children (Pringsheim et al. 2011b; Olfson et al. 2012). Guidelines and educational programs addressing the assessment and management of disruptive and aggressive behavior in children (Knapp et al. 2012; Scotto Rosato et al. 2012; Gorman et al. 2015; Pringsheim et al. 2017) and promotion of antipsychotic drug safety monitoring followed (Pringsheim et al. 2011c; Barclay et al. 2017) in an effort to address knowledge gaps, increase awareness and detection of adverse effects associated with antipsychotic use, and decrease antipsychotic prescribing.
A previously published pharmacoepidemiological study of antipsychotic use in Canada evaluated and compared trends in use of psychostimulants and antidepressants from 2005 to 2009 (Pringsheim et al. 2011b). The pronounced secular trends observed in the use of these medications require ongoing monitoring, particularly the increased use of antipsychotic medications over the time period examined. Hence, the aim of the current study is to evaluate prescribing trends of psychotropic medications since the initial study using the same data source to enhance compatibility. We hypothesized that the use of antipsychotic medications in children would stabilize or decrease from 2010 onward, while the use of psychostimulants and antidepressants would continue to increase at a similar rate as previously observed.
Methods
Study population
IQVIA's Canadian Disease and Therapeutic Index (CDTI) was used to obtain a comprehensive overview of psychotropic medication prescribing to Canadian children, defined as those 18 years old or younger. CDTI is a survey-based dataset that collects treatment data from a sample of office-based physicians in Canada and allows for analyses to identify pharmacoepidemiologic patterns by drug, indication, patient demographics, and physician specialty. A random sample of physicians, stratified by region in Canada and by office-based specialty, are requested to complete a survey of patients they have seen during the reporting period, capturing information on patient demographics, diagnosis, and prescribing decisions, among other information. All major office-based specialties are represented, with representation based on proportionality. Some specialties with very few physicians are oversampled to allow for greater reliability in these areas. In total, up to 750 physicians are sampled each quarter. A minimum of 85% of reporting physicians in a current period are maintained from the previous reporting period. Statistical weighting, stratified by region and specialty, of the reported prescribing from the sample physicians to the universe of physicians is conducted to derive national projections. Projection factors are adjusted to compensate for oversampling. While there are several provincial administrative databases that capture pharmacoepidemiological data, CDTI provides nationwide data on prescribing of medications in the outpatient setting to the general population.
Participating physicians complete an anonymous record of all patient visits during a 48-hour period in each quarter of the year, including patient age, gender, drug recommendation (prescribed drug), and reason for recommendation (therapeutic indication). Rates of prescription purchases are not recorded in this database. Informed consent was not required as no personal identifying information is collected.
Our current investigation involves children 18 years of age and younger who were recommended by a physician in Canada to take an antipsychotic between January 2010 and December 2016 or a psychostimulant, nonstimulant, or antidepressant between January 2012 and December 2016. Class data for psychostimulants, nonstimulants, and antidepressants were not available for 2010 or 2011.
We characterized treatment patterns of antipsychotics, antidepressants, and ADHD medications (including psychostimulants, alpha agonists, and atomoxetine). We also investigated the therapeutic indication for written prescriptions. Results in the analysis period were compared with those from the previous analysis of this data source for these product classes from 2005 to 2009 (Pringsheim et al. 2011b) to provide additional context that underlies changes in prescribing behavior over time.
Analyses
We used counts, percentages, and rates (per 1000 person-years) along with percent change to summarize the raw frequencies of written prescriptions and reasons for these, with data presented in figures and tables. Trends observed with calculated recommendation rates followed similar trends to that of the recommendation counts as the Canadian population aged 18 and younger did not change between 2010 and 2016 (Statistics Canada 2018). The population size of children and youth in 2010 was 7,401,861, increasing only 0.34% to 7,426,926 by 2016.
Calculation of descriptive statistics and visualization of data were conducted in Microsoft Excel 2016 (Redmond, Washington). All counts were weighted to the national population by IQVIA. For calculation of rates, we estimated person-time using mid-year population estimates (Statistics Canada 2018).
Results
Between 2010 and 2016, the number of written prescriptions for antipsychotics decreased by 10%, from 784,040 to 704,854 written prescriptions for the study population (Table 1), in contrast to an increase of 114% between 2005 and 2009 (Pringsheim et al. 2011b). The rate of antipsychotic prescriptions was 112/1000 person-years in 2010, 101/1000 person-years in 2012, and 100/1000 person-years in 2016 (Fig. 1), representing a change in the rate of prescribing of 12% between 2010 and 2016 and a decline of 1% between 2012 and 2016 (Table 1). For antidepressants, there were an estimated 882,670 written prescriptions in 2012 (a rate of 120/1000 person-years), increasing to 1,193,517 in 2016 (a rate of 161/1000 person-years), resulting in a 35% increase in the rate of written prescriptions during this time period. For psychostimulants, the proportional increase over the same time period was not as great as it was for antidepressants; however, the number and rate of written prescriptions were higher. There were an estimated 2,164,650 prescriptions in 2012 (a rate of 293/1000 person-years), increasing to 2,741,971 in 2016 (a rate of 369/1000 person-years). This is a 26% increase in the rate of written prescriptions. Between 2005 and 2009, antidepressant and psychostimulant written prescriptions increased 44% and 36% (Pringsheim et al. 2011b).
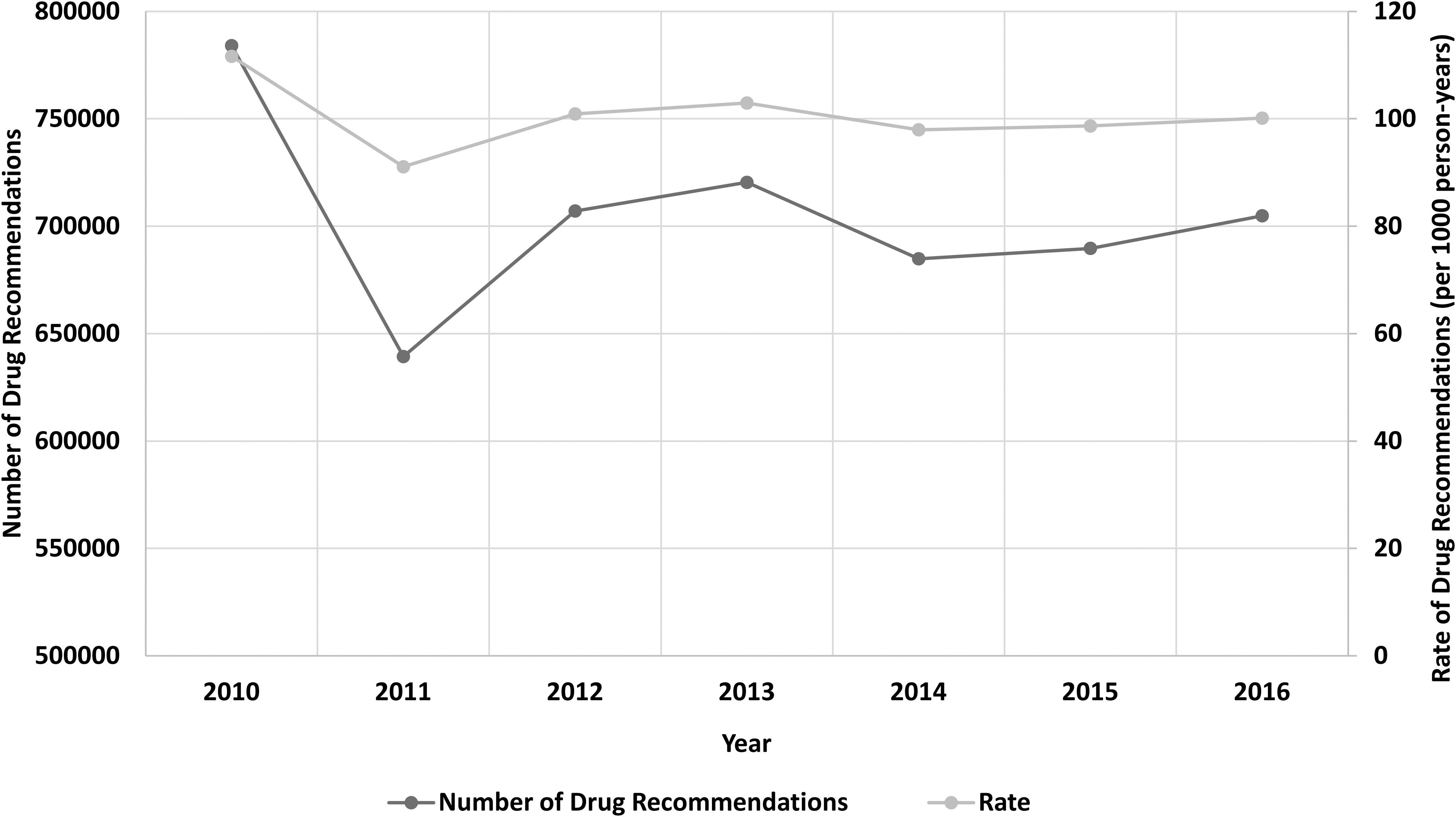
Number and rate of antipsychotic recommendations by year, 2010–2016.
Number and Percentage of Recommendations by Drug Class for Children in Canada
Classes are further broken down into individual drugs with the highest level of prescribing. Class percentages are presented relative to total number of psychotropic recommendations, while those of drugs are presented relative to their class.
FGA, first-generation antipsychotics; SGAs, second-generation antipsychotics; SSRI, selective serotonin reuptake inhibitor; SNRI, serotonin–norepinephrine reuptake inhibitor.
As with the earlier study, the majority of written prescriptions for antipsychotics (>95%) were for SGAs (Fig. 2). Written prescriptions for aripiprazole increased from 32,250 in 2010 to 164,231 in 2016 (a 409% increase), while utilization of quetiapine decreased from 228,420 written prescriptions in 2010 to 118,207 in 2016, a 48% decline. Risperidone use also declined, by 16%, from 436,840 written prescriptions in 2010 to 366,707 in 2016. With aripiprazole only entering the Canadian market in late 2009, the growth in SGA written prescriptions observed during 2005–2009 was driven by risperidone and quetiapine (Pringsheim et al. 2011b).
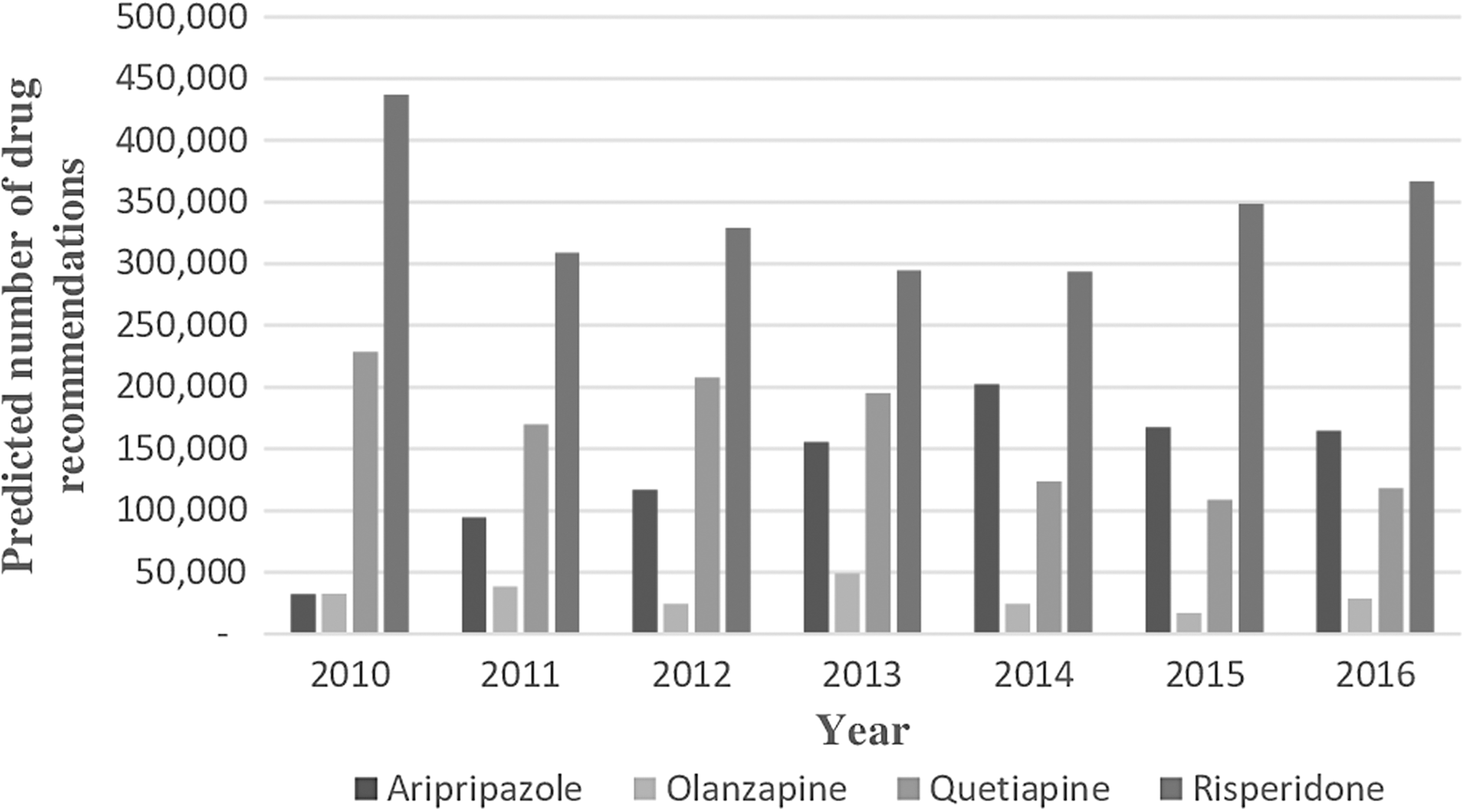
Second-generation antipsychotic recommendations by medication for children in Canada, 2010–2016.
For antidepressants, most written prescriptions were in the class of selective serotonin reuptake inhibitors. Notably, written prescription frequencies for escitalopram, fluoxetine, and sertraline increased by 40%, 48%, and 77%, respectively, between 2012 and 2016. Last, in the psychostimulant class, lisdexamfetamine and methylphenidate were the most commonly prescribed drugs. Their use continued to grow, increasing by 44% and 38%, respectively. For nonstimulant ADHD medications, an increase in guanfacine extended-release written prescriptions for ADHD was observed, although the overall number of written prescriptions was modest at <150,000 per year in 2016 compared with almost two million written prescriptions for methylphenidate.
Overall trends in reasons for an SGA prescription remained similar between the two analysis periods (Table 2). In 2010–2016, the most common reason for a written prescription for an SGA was ADHD, followed by conduct disorder, psychotic disorder, and tic disorder. The number of SGA written prescriptions for ADHD decreased from 176,610 in 2010 to 107,625 in 2016. There was a slight decrease in written prescriptions for conduct disorder and tic disorder over this time period, while written prescriptions for psychotic disorder remained stable. Written prescriptions for autism increased from 35,010 in 2010 to 90,288 in 2016. As expected, antidepressants were most frequently recommended for anxiety disorder (36%), depression (33%), and obsessive-compulsive disorder (6%), and psychostimulants were primarily recommended for ADHD (94%).
Second-Generation Antipsychotic Drug Recommendations by Indication (Top Ten Indications), 2010–2016
ADHD, attention-deficit/hyperactivity disorder.
Indications for antipsychotic medication written prescriptions varied by age over the study period. For children aged 1–6 years, the top three indications for which SGAs were recommended were ADHD, conduct disorder, and autism. In children aged 7–12 years, the top three indications were ADHD, conduct disorder, and tic disorder. In adolescents, 13–18 years, the top three indications were psychotic disorder, bipolar disorder, and anxiety disorder.
Psychiatrists recorded the most written prescriptions for antipsychotics compared with other physicians, averaging 64% of the recommendations yearly from 2012 to 2016 (Fig. 3), followed by general practitioners (17%), pediatricians (17%), neurologists (2%), and other specialties (0.1%). These physician prescribing patterns remained similar to those observed during the 2005–2009 period. The overall decrease in written prescriptions during 2012–2016 for these medications was mainly driven by the change in prescribing frequencies by general practitioners and psychiatrists, which decreased by 26% and 13%, respectively. However, written prescriptions for antipsychotics by pediatricians saw a 102% increase during the same period. For antidepressants, similar trends across physician specialties were observed with psychiatrists (48% of written prescriptions), followed by general practitioners (39%), pediatricians (12%), neurologists (1%), and other specialties (0.2%). For psychostimulants, general practitioners prescribed most often (40% of written prescriptions), followed by pediatricians (37%), psychiatrists (22%), neurologists (1%), and other specialties (0.1%).
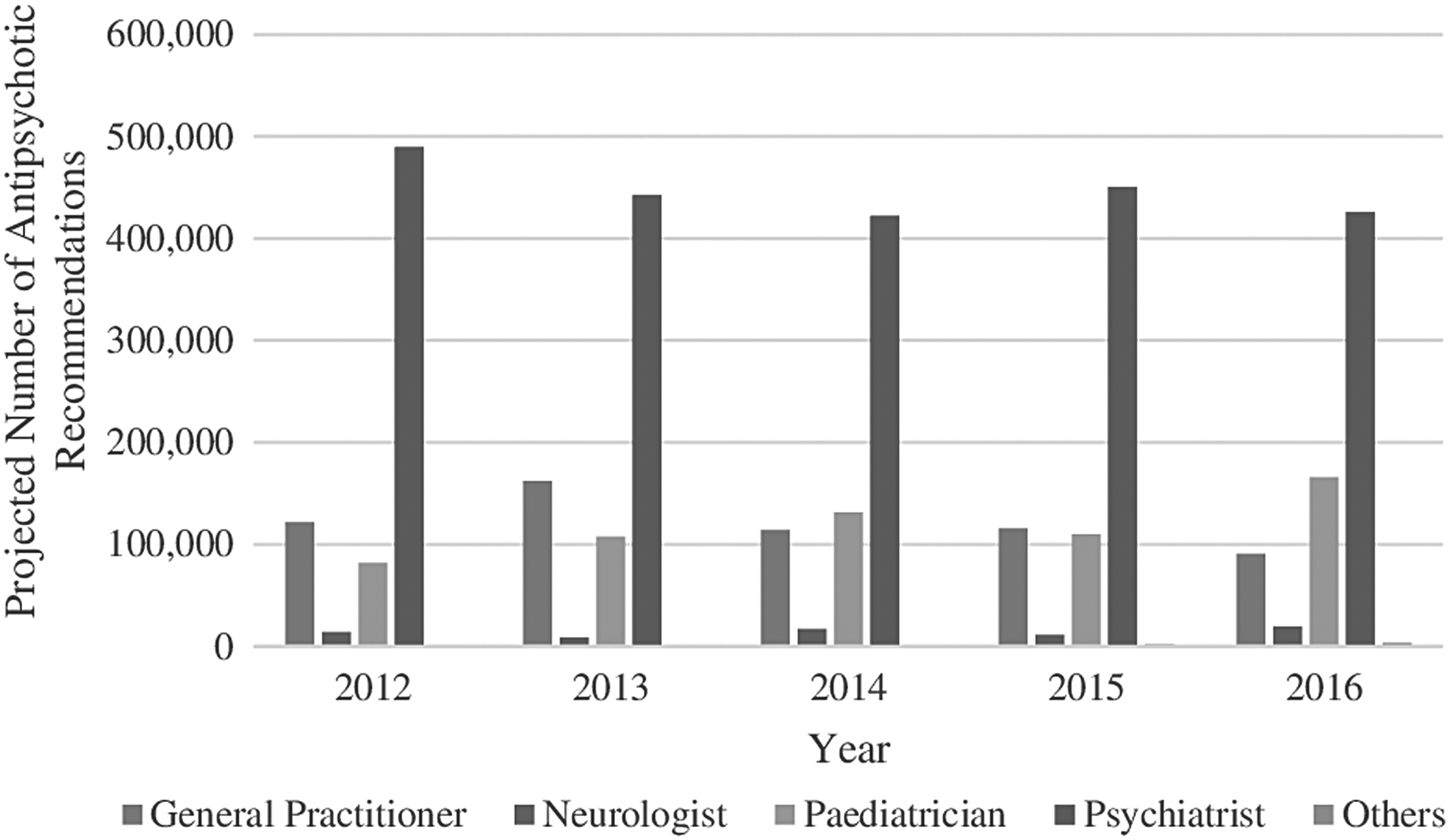
Number of antipsychotic recommendations by physician specialty.
Discussion
This study demonstrated a modest decrease in written prescriptions for antipsychotics for children and youth from 2010 to 2016 using a Canadian national data source. This decrease is a welcome discovery given concerns regarding metabolic, hormonal, and extrapyramidal adverse effects with antipsychotic use in children (Pringsheim et al. 2011a). However, the change was largely driven by a reduction in 2011 relative to 2010, with only a negligible change since then. The decrease in written prescriptions for antipsychotics was most prominent in children with ADHD. Possible reasons for this change include the publication of clinical practice guidelines and educational programs related to assessment and management of disruptive and aggressive behavior and the availability of a new medication in Canada, which targets these symptoms. In 2012, the Treatment of Maladaptive Aggression in Youth (TMAY): Center for Education and Research on Mental Health Therapeutics, Guidelines 1 and 2, were published in the journal Pediatrics (Knapp et al. 2012; Scotto Rosato et al. 2012). These guidelines made strong recommendations for providing evidence-based psychosocial interventions as the first-line treatment of maladaptive aggression in children and youth and that such interventions should continue through all phases of care. In 2015, Canadian guidelines on pharmacotherapy for disruptive and aggressive behavior in children and adolescents with ADHD, oppositional defiant disorder, and conduct disorder were published in the Canadian Journal of Psychiatry (Gorman et al. 2015). Based on a systematic review of randomized controlled trials, these guidelines recommended that when severe disruptive or aggressive behavior occurs with ADHD, medication for ADHD should be used first, including psychostimulants, alpha agonists, and atomoxetine. Risperidone was given a conditional recommendation when psychosocial interventions and ADHD medications were unsuccessful in treating disabling symptoms. It was recommended that the duration of treatment be limited to 3 months, after which time tapering and discontinuation should be attempted. The TMAY and Canadian guidelines provided the foundation for two major cross-Canadian educational initiatives—a resident education curriculum in pediatrics and psychiatry on the assessment and treatment of disruptive and aggressive behavior in children and youth (Pringsheim et al. 2017) and an electronic continuing medical education program for physicians in practice. As these programs were launched in 2016, the impact on prescribing behavior was likely limited.
The approval by Health Canada in 2013 of Intuniv XR, an extended-release formulation of the alpha agonist guanfacine for treatment of ADHD in patients aged 6–17 years, may also have led to a change in prescribing behavior for aggressive and disruptive behavior in children with ADHD. Guanfacine was not available in Canada before the approval of Intuniv XR. Intuniv XR, once available, may have replaced written prescriptions for risperidone due to available evidence showing safety and benefit in combination with psychostimulants in reducing residual ADHD symptoms and a positive effect specifically on oppositional behavior (Connor et al. 2010).
Growth in written prescriptions for aripiprazole over the study period is not unexpected as it was only approved and available for use in Canada from 2009. In youth, aripiprazole is Health Canada approved for the treatment of schizophrenia (age 15–17) and bipolar disorder (age 13–17). The Food and Drug Administration (FDA) also approved aripiprazole in the United States for treatment of irritability in autism in 2009 and for treatment of tics in Tourette's disorder in 2014. The evidence to support efficacy across multiple child and youth mental health disorders may have encouraged written prescriptions for aripiprazole by physicians. Positive clinical trials and FDA approvals for risperidone (Jesner et al. 2010) in 2007 and aripiprazole (Hirsch and Pringsheim 2016) in 2009 for irritability in autism may have led to the increase in written prescriptions for SGAs in children with autism observed over the 2010–2016 time period.
In contrast to the multiple studies evaluating prescribing trends of antipsychotics in children and youth from 1990 to 2010, studies evaluating prescribing trends in the past 5 years are scarce. Using the IMS LifeLink LRx Longitudinal Prescription database, Olfson et al. (2015) found that antipsychotic usage increased from 2006 to 2010 for adolescents and young adults, but remained stable in children 12 years and younger. We were unable to find any other Canadian or U.S. pharmacoepidemiological studies evaluating the use of antipsychotic medications over time within the past 5 years to compare our data with. A systematic review of recent prescription trends of antipsychotic medications in children published in 2015 did not include any data later than 2011 (Carton et al. 2015).
In the United States, a number of statewide programs to monitor and improve prescribing practices for psychotropic medications for children have been instituted, leading to changes in the frequency of off-label use of antipsychotic medications within the Medicaid population. In 2008, Washington State created a consultation service to improve primary care access to child and adolescent psychiatric expertise, with elective consults for primary care, and mandatory medication reviews for antipsychotic prescriptions based on young age, high doses, and antipsychotic polypharmacy. Analysis of atypical antipsychotic use among child Medicaid enrollees demonstrated a decrease from 0.51% in 2006 to 0.25% in 2013 (Barclay et al. 2017). The impact of a peer review program on antipsychotic use among Medicaid insured youth in a mid-Atlantic state also has demonstrated significant decreases in antipsychotic use postimplementation. The Department of Health and Mental Hygiene implemented a program in 2011, which involved review of antipsychotic prescriptions by clinical pharmacists based on prespecified clinical criteria, including age, diagnosis, target symptom severity, psychosocial service use, and medication dosage based on weight and age, and monitoring criteria. Secondary review with a child and adolescent psychiatrist was available if the prescription request was denied. An overall reduction in the proportion of antipsychotic-medicated children and youth was found, from 5.6% in the preimplementation period (2011) to 3.9% in the postimplementation (2014) period (Pennap et al. 2018).
Our study used data from IQVIA. Although this is a valuable source of pharmacoepidemiologic information, there are some limitations. Data from the CDTI are based on a national sampling strategy that comprises a representative sample both geographically and by specialty; it is possible for sampling errors to over- or underestimate national drug recommendations. In addition, the database records the number of written prescriptions, but does not track the quantity or duration of the prescription. As such, the estimates presented here may not fully reflect the total quantity of medications prescribed. Additionally, the database records medication prescriptions written, but not whether the prescription was filled. Consequently, some proportion of prescriptions may not be filled. Polypharmacy is not recorded in the database. Due to the nature of the database, we are not able to establish causation for the changes in written prescription frequency over time.
Conclusion
In conclusion, written prescriptions for antipsychotics to Canadian youth appear to be stabilizing and may be related to switching from antipsychotics to other medications (i.e., guanfacine extended release), improved awareness of adverse effects related to their use, and greater implementation of evidence-based care for management of disruptive and aggressive behavior in youth.
Clinical Significance
We analyzed prescribing trends for psychotropic medications in Canadian children from 2010 to 2016 and compared our findings with a previous analysis from 2005 to 2009 using the same national data source. In this first pharmacoepidemiological study describing prescribing trends after 2011, we demonstrate a leveling off of antipsychotic use in children, after more than a decade of exponential growth in use of these medications. Written prescriptions for antipsychotics fell by 10% from 2010 to 2016, in contrast to a 114% increase between 2005 and 2009. Written prescriptions for antidepressant and ADHD medications demonstrated a similar increase over the two time periods. This study suggests that educational initiatives recommending limited and cautious use of antipsychotics for nonpsychotic disorders in children have been effective.
Footnotes
Disclosures
D.G.S., P.C., and A.T. are employees of IQVIA Canada.