
Abstract
Objective:
The high placebo response rate may hamper the discovery of antidepressants in children and adolescents with major depressive disorder (MDD). The aim of the study was to clarify the relationship between the placebo response rate and clinical trial outcomes of the use of antidepressants in children and adolescents, and distinguish main factors responsible to placebo response rate.
Methods:
The PubMed and Cochrane Library databases were searched for double-blind randomized placebo-controlled trials of the new-generation antidepressants for the acute treatment of MDD in children and adolescents. The response rate differences (RDs) between placebo group and treatment group under different level of placebo response rate were pooled by random-effects meta-analysis. The classification thresholds for low, medium, and high placebo response rate were set at <40%, 40%–50%, and ≥50%, respectively. Predictors of placebo response rate were explored using meta-regression.
Results:
The analysis included 18 trials with 4365 participants. This study found that the lower the placebo response rate, the greater the efficacy differences between antidepressants and placebo. In the high, moderate, and low placebo response rate subgroups, the response RDs (95% CI) between antidepressants and placebo were 8 (1–14)%, 10 (2–17)%, and 21 (9–32)%, respectively. The meta-regression showed that the number of study sites was the factor most associated with placebo response rate, and that response rate increased 3% with every additional 10 study sites.
Conclusions:
The clinical outcome was related to the placebo response rates in the clinical trials of antidepressants in children and adolescents with MDD. The efficacy differences between antidepressants and placebo will be maximized when placebo response rates are reduced. The number of study sites was the factor most associated with the placebo response rates.
Introduction
Major depressive disorder (MDD) is one of the most common mental disorders in children and adolescents. A recent study in the United States reported an increase in the 12-month prevalence of major depressive episodes in adolescents, from 8.7% in 2005 to 11.3% in 2014 (Mojtabai et al. 2016). Unlike adults, children and adolescents with MDD are underdiagnosed, and only 36%–44% of them are treated or receive health care (Olfson et al. 2014). Persistent depression in children and adolescents is associated with serious complications, including poor school performance and social functioning, recurring depression in adulthood, and suicide (Hopkins et al. 2016). Therefore, the US food and drug administration (FDA) has stressed the need to treat MDD in children as early as possible (US FDA 2017).
Currently the use of antidepressants in adolescents is gradually increasing (Bachmann et al. 2016). However, previous meta-analyses and many clinical trials indicate that antidepressants are minimally effective or equivalent to placebo (Bridge et al. 2007; Kirsch 2014; Cipriani et al. 2016; Jureidini 2016; Le Noury et al. 2016; Locher et al. 2017). Unfortunately, most of these studies ignored the heterogeneity of the studies with different placebo response rates.
In this study, we present a comprehensive systematic analysis to understand the efficacy of the new-generation antidepressants in children and adolescents under the different levels of placebo response rate. Moreover, the factors related to the placebo response rate in children and adolescents will be identified to provide a valuable reference for future clinical trials.
Methods
Search strategy
The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard (Liberati et al. 2009) (Supplementary Appendix p1–4). The PubMed and Cochrane Library databases were searched for double-blind randomized placebo-controlled trials. The retrieval deadline was December 31, 2017. We also screened the pharmaceutical company websites, the FDA website, and key journals for published and unpublished studies. The detailed search strategies are described in Supplementary Appendix p5.
Outcome
Our primary outcome was response rate. Response rate refers to the ratio of participants who respond to treatment. Being a responder was defined as having a clinical global impression-improvement (CGI-I) score ≤2 (Guy 1976), at least a 50% reduction in Children's Depressive Rating Scale-Revised (CDRS-R) score relative to baseline (Emslie et al. 2002), or kiddie schedule for affective disorders and schizophrenia present episode version (K-SADS-P) depression and anhedonia scores ≤2 at the end of the study (Chambers et al. 1985).
Inclusion and exclusion criteria
The inclusion criteria for trials were as follows: (1) double-blind randomized placebo-controlled trials in which antidepressant monotherapy was used as the acute-phase treatment; (2) participants were children or adolescents (age <18 years of age) who meet the DSM diagnostic criteria for MDD; and (3) studies reporting the response rate at the end of the trial.
To reduce the heterogeneity and variability in the characteristics of the participants and the study design, the exclusion criteria were as follows: participants with comorbid nonaffective psychiatric disorders or treatment-resistant depression; studies with a sample size of <10.
Data extraction and risk of bias assessment
A Microsoft Excel 2010 database was established to categorize the relevant information of the included studies, and included the following categories: study design (grouping, sample size, number of study sites, and treatment duration), characteristics of participants (mean age, gender ratio, region, and disease severity), and the clinical outcome (response rate of each treatment group at endpoint). Data from intention-to-treat were entered when available.
Two investigators (Y.F.L. and J.H.H.) independently extracted the relevant information and assessed the risk of bias by the Cochrane risk of bias tool (The Cochrane Collaboration 2017). Any disagreement was resolved through discussion with a third investigator (L.J.L.). In total, seven items, including randomization sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias, were used to evaluate bias in each trial. We defined other bias as trials in which baseline characteristics were not similar in different intervention groups. Each quality item was graded as low risk, high risk, or unclear risk.
The included studies were graded as high quality, moderate quality, or low quality based on the following criteria: (1) studies were considered high quality when both randomization and allocation concealment were assessed as a low risk of bias, and all other items were assessed as low or unclear risk of bias in a trial; (2) studies were considered low quality if either randomization or allocation concealment was assessed as a high risk of bias, regardless of the risk of other items; and (3) studies were considered moderate quality if they did not meet criteria for high or low risk.
Data synthesis and analysis
The meta-analyses were performed using Stata software version 13.1 (2013, StataCorp LP, College Station, TX). Response rate differences (RDs) between the drug group and placebo group were obtained by the “metan” command in Stata. Random effects models were used to estimate the effect size by the “random” command in Stata (Cornell et al. 2014). The statistical heterogeneity across studies was assessed using the I 2 statistic, where an I 2 ≥50% suggests that there was significant heterogeneity among the studies (Annane et al. 2004). We evaluated the potential publication bias using funnel plots and Egger's tests (Stuck et al. 1998; Biljana et al. 1999).
The focus of our analysis was to verify whether the clinical outcome of treating children and adolescents with antidepressants was significantly affected by the placebo response rate. Therefore, subgroup analysis was undertaken according to the placebo response rate classification. However, there are no uniform classification thresholds for placebo response rate. According to a previous study (Walkup 2017) and the distribution of placebo response rates in the included studies, the classification thresholds for the low, medium, and high placebo response rate were set at <40%, 40%–50%, and ≥50%, respectively.
Meta-regression was performed to test the factors associated with placebo response rate using the random-effects model (Thompson and Higgins 2002). The weight for each trial was equal to the inverse of the sum of the within trial variance and the residual between trial variance. Univariate meta-regression analysis was first performed, and multivariate meta-regression was conducted if more than one factor was significant in the univariate model. The Stata command metareg, knapphartung, and reml were to be used.
We tested the following variables: (1) trial characteristics: sample size per study, sample size of the placebo group, mean sample size per study site, number of arms, dosing regimen (fixed dose or flexible dose), study design (placebo lead in or not), treatment duration, number of study visits, number of study sites, country (single country or mixed countries), publication year, and funding source (industry-sponsored or not); (2) participant characteristics: average age, gender, inpatient or outpatient, and severity at baseline as measured by CDRS-R scores; and (3) drug type: selective serotonin reuptake inhibitors (SSRIs) drugs or non-SSRIs drugs. When the disease severity at baseline was only reported by the MADRS or HDRS, these scores were converted to equivalent CDRS-R scores according to the reported methods (Jain et al. 2007; Lovieno et al. 2016).
Sensitivity analysis
Five sensitivity analyses were conducted to evaluate the robustness of the primary findings. (1) The leave-one-out approach was used to test the influence of each individual study on the response rate. (2) We excluded the studies of fluoxetine and escitalopram in the pooled analysis of response rate as these have been approved to be used by children or adolescents with MDD by the FDA. (3) We excluded the studies with other scales besides the CGI-I in the pooled analysis of response rate. (4) We excluded the studies of non-SSRIs drugs to explore the influence of drug type on the results. (5) For the significant factors obtained by the univariate meta-regression, the leave-one-out approach was applied to test the stability of the predictors.
Results
Characteristics of the included studies
Overall, 757 citations were identified by the search, a total of 606 abstracts were examined and 101 potentially eligible full-text articles were retrieved. Three additional studies were selected from the FDA reports and pharmaceutical company websites (Fig. 1). Finally, 18 studies (Supplementary Appendix p6–7) consisting of 40 groups were included for analysis, of which 22 groups were given antidepressants (N = 2500) and 18 groups received a placebo (N = 1865) (Emslie et al. 1997, 2002, 2006, 2007, 2009, 2014; Keller et al. 2001; Organon Pharmaceuricals USA, Inc. 2001; Wagner et al. 2003, 2004, 2006; March et al. 2004; Berard et al. 2006; von Knorring et al. 2006;
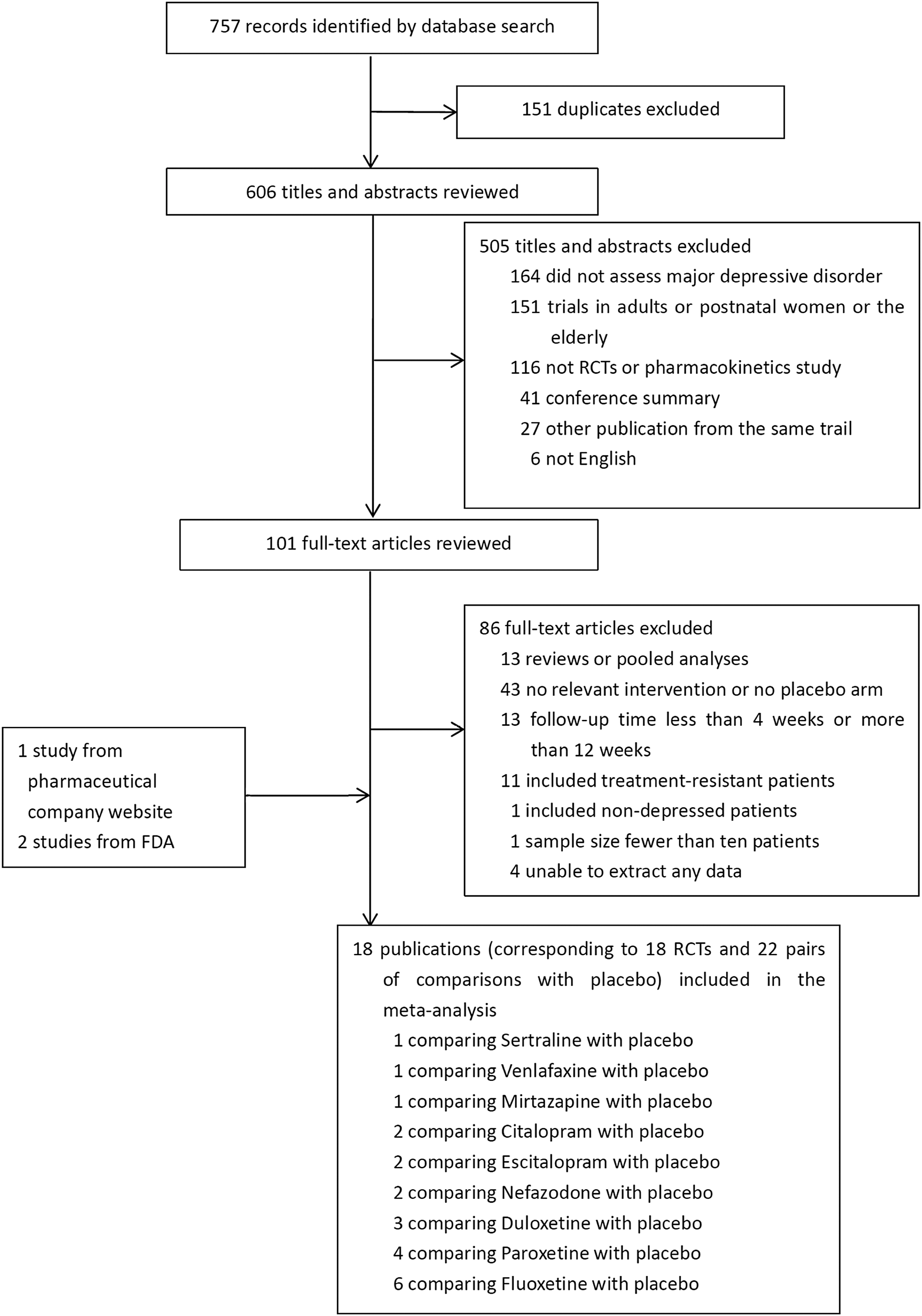
PRISMA diagram of the literature search.
Characteristics of Included Studies
One-way ANOVA.
Kruskal–Wallis test.
CDRS-R, Children's Depressive Rating Scale-Revised.
In the 18 included studies, 7 studies found a high placebo response rate (≥50%), 7 studies found a moderate placebo response rate (40%–50%), and 4 studies found a low placebo response rate (<40%). Moreover, the four studies that found a low placebo response rate were all studies where the active drug was fluoxetine.
According to the criteria of literature quality, 15 studies were rated as high quality, and the remaining 3 studies were graded as moderate quality. Overall, the quality of the involved studies was relatively high (Supplementary Appendix p8–9).
Response rate
As shown in Figure 2, the overall response RD between antidepressants and placebo was 10% (95% CI 6–15). Subgroup meta-analysis showed that the response RDs between antidepressants and placebo were 8% (95% CI 1–14), 10% (95% CI 2–17), and 21% (95% CI 9–32) in the high, moderate, and low placebo response rate subgroups, respectively.
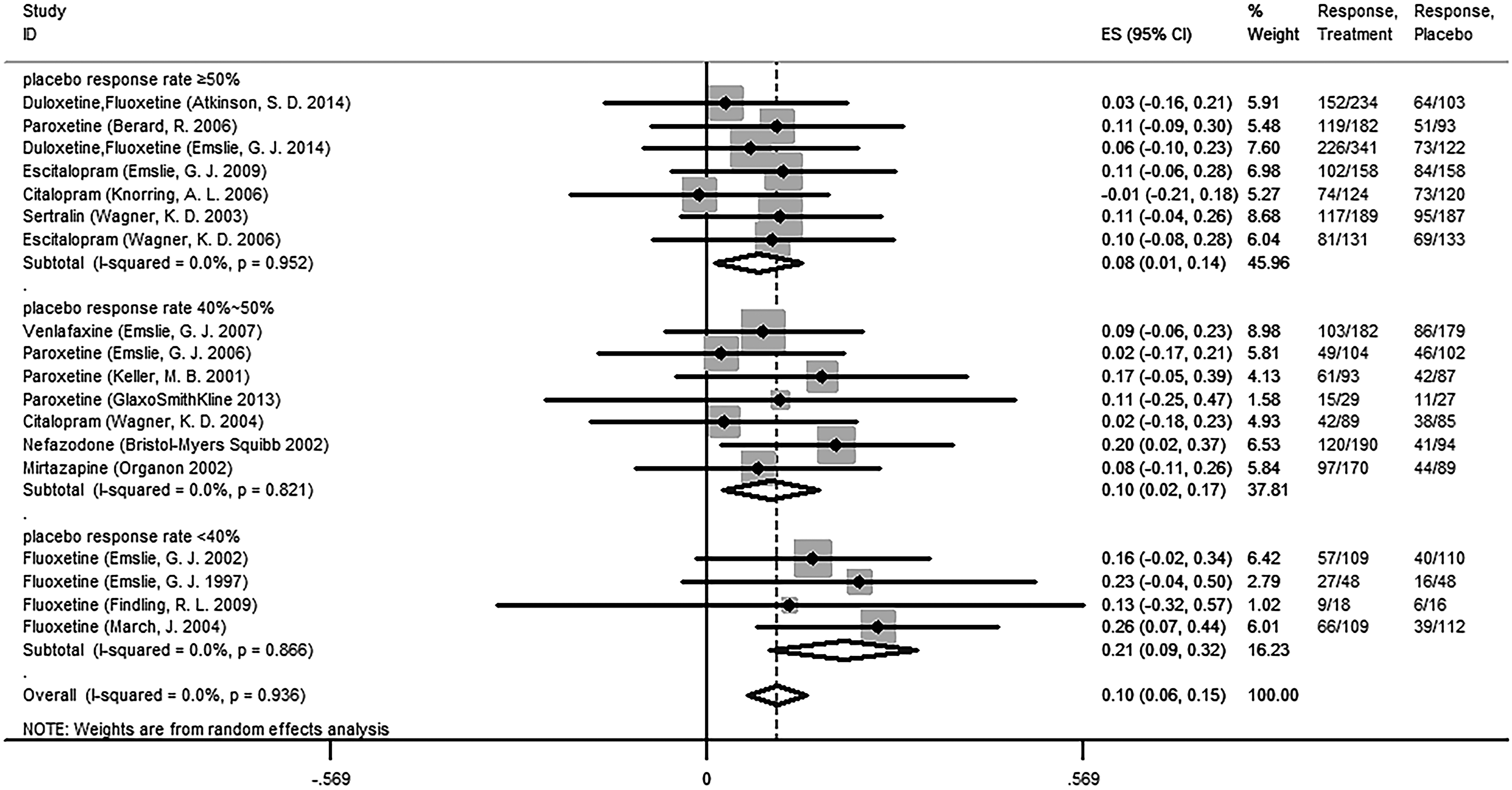
Forest plot of the RDs of response rates for antidepressants versus placebo. RDs, rate differences.
Sensitivity analysis showed that, after excluding the studies with non-CGI-I scales (Supplementary Appendix p11), the response RDs between antidepressants and placebo were 11% (95% CI 2–19), 10% (95% CI 2–17), and 21% (95% CI 9–32) in the high, moderate, and low placebo response rate subgroups, respectively. After excluding the studies of non-SSRIs drugs (Supplementary Appendix p12), the response RDs between antidepressants and placebo were 7% (95% CI 2–11), 8% (95% CI 0–15), and 21% (95% CI 13–29) in the high, moderate, and low placebo response rate subgroups, respectively. These results were essentially consistent with the original results. When conducting leave-one-out meta-analysis (Supplementary Appendix p12), the response RDs between antidepressants and placebo were ranged from 7% to 9%, from 8% to 11%, and from 18% to 24% in the high, moderate, and low placebo response rate subgroups, respectively. These results suggested that the original results were robust and less influenced by the individual studies.
As the four low placebo response rates studies were all studies of fluoxetine, after exclusion of the groups who were given fluoxetine and escitalopram, the subgroup of low placebo response rates was missing. The subgroup results of the high and medium placebo response rates were 8% (95% CI −1 to 16) and 10% (95% CI 2–17), which were still consisted with the original results (Supplementary Appendix p10).
A separate meta-analysis was performed for fluoxetine (Supplementary Appendix p17). The results showed that the response RDs between fluoxetine and placebo in the low and high placebo response rate subgroups were 21% (95% CI 9–32) and 1% (95% CI −13 to 15), respectively.
Potential publication bias
The funnel plot showed symmetry, and the publication bias was not significant for the response RD, according to Egger's test (p > 0.05; Supplementary Appendix p14).
Predictors of placebo response rate
The results of meta-analysis showed that the overall placebo response rate was 48% (95% CI 44–52) and heterogeneity test I 2 = 66.4% (Supplementary Appendix p14), suggesting that the heterogeneity of placebo response rate among studies was large and the source of heterogeneity needs to be analyzed. The results of univariate meta-regression showed that the number of study sites, sample size per study, mean sample size per site, publication year, country (in single country or mixed countries), and funding source (industry-sponsored or not) were significantly correlated with the placebo response rate (Table 2). Sensitivity analyses confirmed that the number of study sites, sample size, publication year, and country were robust predictors that were insensitive to the exclusion of any individual study (Supplementary Appendix p15).
Meta-Regression of Potential Predictors on the Placebo Response Rate in the Trials of Antidepressants in Children and Adolescents
CDRS-R, Children's Depressive Rating Scale-Revised; CI, confidence interval; SSRI, selective serotonin reuptake inhibitor.
As the number of study sites was correlated with the sample size per study and the publication year (Supplementary Appendix p16), we only placed the number of study sites into the multivariate meta-regression, together with country, to avoid collinearity. As shown in Table 2, only the number of study sites was significantly related with the placebo response rate (p < 0.05).
Discussion
Previous meta-analyses have shown that most antidepressants, except for fluoxetine, were not superior to placebo for the alleviation of symptoms in children and adolescents with MDD (Bridge et al. 2007; Kirsch 2014; Cipriani et al. 2016; Jureidini 2016; Le Noury et al. 2016; Locher et al. 2017). Walkup (2017) put forward an important point that the conclusions of meta-analysis should be questioned, as those meta-analyses included improper industry-sponsored studies. To complete the studies in a very tight time frame, some inexperienced investigators did not receive adequate training, which resulted in the recruitment of some participants who did not meet the inclusion criteria (Walkup 2017). Therefore, guidelines that were based on those meta-analyses need to be questioned. However, there is a lack of systematic review to support this view. This study we systematically compared the characteristics of the clinical outcomes of the new-generation antidepressants in children and adolescents under different levels of placebo response rate.
This study showed that the antidepressants have a weak effect in children and adolescents, as this response rate was just 10% higher than the placebo. In addition, the efficacy differences between the antidepressants and the placebo increased as the placebo response rate decreased. The efficacy difference in the low placebo response rate subgroup (21%) was about three times that of the high placebo response rate subgroup (8%). The most recent network meta-analysis shows that fluoxetine was the only effective drug for children and adolescents with MDD (Cheung et al. 2006), and it is also the only antidepressant approved by the FDA for use in children (US FDA 2007). This study included six fluoxetine trials, four had a low placebo response rate, and two had a high placebo response rate. We performed a separate meta-analysis for fluoxetine, which showed that even fluoxetine was ineffective in the high placebo response rate study. It is noteworthy that, except for fluoxetine, the placebo response rates in the other antidepressants studies were all >40%, which is perhaps the reason why most studies came to the conclusion that antidepressants were minimally effective or ineffective for children and adolescents.
Furthermore, we explored the factors impacting the difference in efficacy between the antidepressants and the placebo. The results showed that the placebo response rate was indeed the most significant factor affecting the difference in efficacy between the antidepressants and the placebo (Supplementary Appendix p19–21). Therefore, when conducting a meta-analysis to compare the efficacy among the antidepressants in children and adolescents, the heterogeneity of the placebo response rate among the studies needs to be examined; otherwise, it would lead to incorrect conclusions.
A study published in the World Psychiatry accessed the FDA reviews for 16 antidepressants approved between 1987 and 2013 (Khan et al. 2017). The results of this study suggested that the relationship between the magnitude of placebo response and the outcome of antidepressant clinical trials is weak, although the magnitude of placebo response has steadily grown in the past 30 years, the magnitude of antidepressant-placebo differences have remained equivalent. However, this conclusion is based on adult patients with MDD. Previous studies showed that children and adolescents with MDD exhibit higher placebo response rates compared with adult patients (46% vs. 31%) (Walsh et al. 2002), and the psychological and physiological characteristics of children and adolescents are quite different from those of adults (Bylund and Reed 2007). Therefore, the findings from adult patients may not be applicable to children and adolescents.
Identification of the impact factors of placebo response could be useful for clinical research. Low placebo response might decrease the necessary sample size and increase the power to detect differences between antidepressants and placebo.
Previous studies suggested that many factors, such as treatment condition, stage of change, number of comorbid disorders, cognitive distortions, psychological theories, and early-life adversity, were strongly related to the trajectory of the change in the symptoms of depression in adolescents (Cohen et al. 2008, 2010; Scott et al. 2019). Therefore, these factors may be potential predictors of the placebo response in MDD. In addition, many studies have reported that the placebo response stems from highly active processes in the brain that are mediated by the dopaminergic reward mechanisms (de la Fuente-Fernández et al. 2002; Enck et al. 2008; Colloca et al. 2014). Therefore, it is also possible to explore the predictors of placebo response from the perspective of electrophysiology or neuroimaging. A recent study has confirmed that electrophysiology can be used to identify potential placebo responders among patients with MDD (Trivedi et al. 2018). However, given the limited information reported in the literature, we were unable to investigate the correlation between these factors and placebo response.
In this study, we only found that some trial characteristics, such as the number of study sites, sample size per study, country, and publication year, were significantly correlated with the placebo response rate. Many studies reported that the placebo response rates of antidepressants increased year by year (Walsh et al. 2002; Khan et al. 2017), which was consistent with our findings. In recent years, it has become more common to conduct clinical trials using multicenters with large sample sizes, which increases the difficulty in strictly controlling the quality of studies and easily leads to high placebo response rates. Therefore, the influence of publication year on placebo response rates is mainly derived from the number of study sites, the sample size, and so on.
To prevent collinearity, we only introduced the number of study sites and country in the multivariate meta-regression. When country and the number of study sites were both placed in the model, the significant influence of country disappeared, indicating that country was not an essential predictor for the placebo response rates. The trials conducted in the mixed countries usually include multicenter sites. Finally, the number of study sites was the factor most associated with the placebo response rates. This conclusion is consistent with the finding by the previous studies (Bridge et al. 2009; Parellada et al. 2012; Meister et al. 2018). However, our study was based on more extensive data, and further quantified the impact of the number of study sites on the placebo response rate. We found that the placebo response rate will increase by 3% (95% CI 1–5) with every additional 10 study sites (Fig. 3).
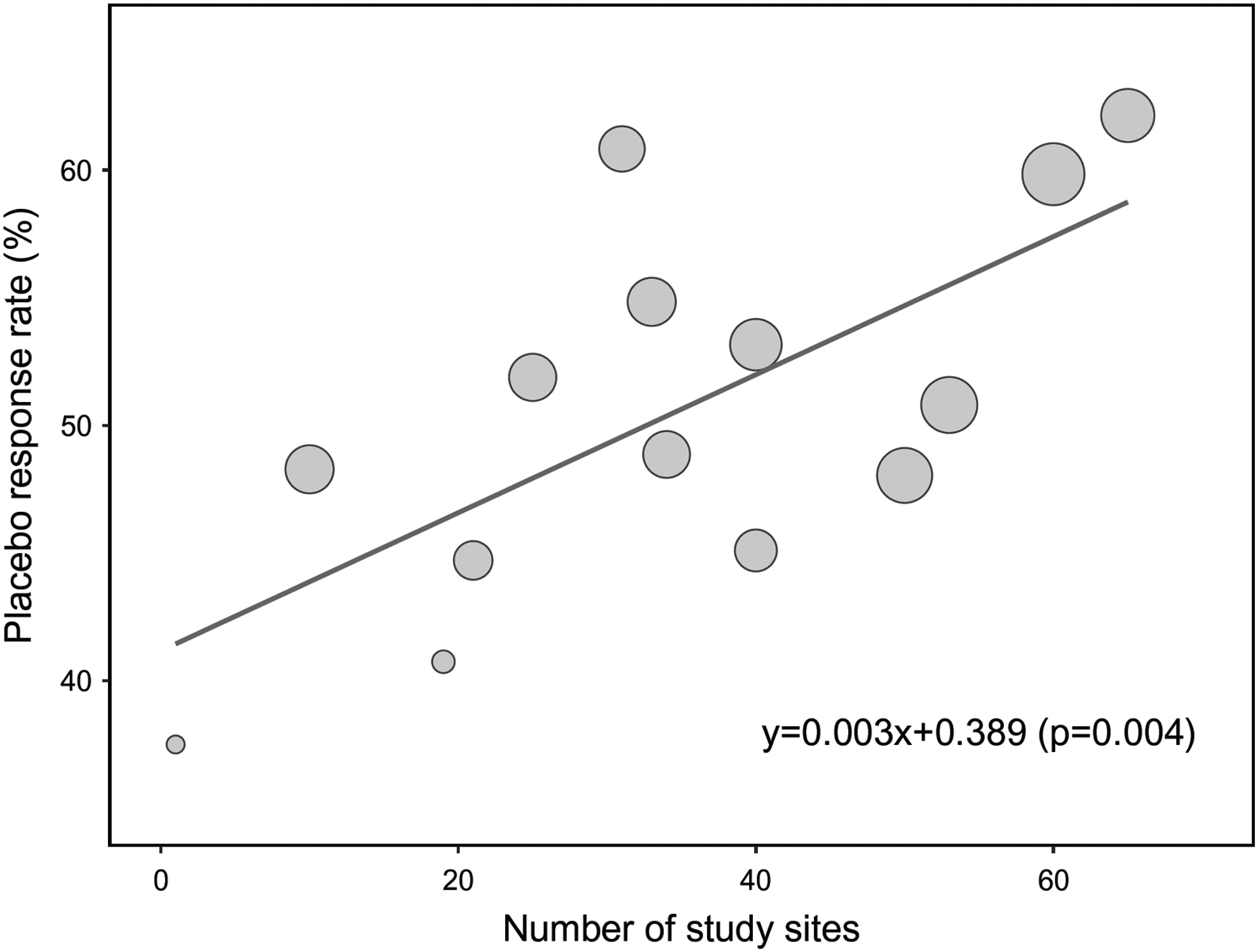
Association between number of study sites and placebo response rates. The circle size is proportionate to the number of participants.
It is worth noting that a vicious circle is prevalent in the clinical trials of antidepressants in children and adolescents. As the efficacy differences between antidepressants and placebo were small, a large sample size is needed to get positive conclusions (Cohen 2007). A large sample size usually needs a large number of study sites to be realized. However, with an increasing number of study sites, the screening for participants may be less stringent and the outcome assessment may be less consistent owing to the lack of experienced investigators (Bridge et al. 2009), resulting in the higher placebo response rates and much smaller efficacy differences. When there is a need for many study sites, it is necessary to reduce the potential sources of variability within and between study sites, such as amount of investigator experience and procedures used to recruit subjects (Amsterdam and Brunswick 2002).
Several limitations should be considered when interpreting our results: (1) all included studies were published in English, which may contribute to publication bias; (2) we did not perform the subgroup analyses classified by the different antidepressants type due to the small number of included trials, which may lead to the results mixed of the variation among the different drugs; (3) as the four low placebo response rates studies were all from trials of fluoxetine, we could not obtain information on the efficacy of other antidepressants under the low placebo response rates; and (4) as most of the participants in the included studies are adolescents, this study did not distinguish the difference in efficacy for children and adolescents. It is suggested that more attention should be paid to the efficacy and safety of antidepressants in the younger children.
Conclusions
(1) In the clinical trials of antidepressants in children and adolescents with MDD, the clinical outcome was related to the placebo response rates. With the decrease of placebo response rates, the efficacy differences between antidepressants and placebo were obviously increased, which helps to come to positive conclusions. (2) The number of study sites was the factor most associated with the placebo response rates, and the placebo response rate increased by about 3% with every additional 10 study sites.
Clinical Significance
The high placebo response rate may hamper the discovery of antidepressants in children and adolescents with MDD. However, there is a lack of systematic evaluation to support this view. This study systematically compared the characteristics of the clinical outcomes of antidepressants in children and adolescents under different levels of placebo response rate. The results showed that the lower the placebo response rate, the greater the efficacy difference between antidepressants and placebo, and placebo response rate can be decreased by reducing the number of study sites. These findings will help to provide important information for clinical trials in children and adolescents with MDD.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.