
Abstract
Objectives:
In Japan, there are currently no approved antidepressant treatments for pediatric patients with depression. This study aimed to estimate the prevalence of depression among adolescents under medical care in Japan, the pharmacological treatments used, and the perceived unmet needs among the medical specialties treating depression in the pediatric population.
Methods:
The study was conducted in November 2014 as an internet survey among physicians in clinical practice. It included a sample of 731 physicians with the potential to treat adolescent patients with depression and 161 physicians who had treated at least one adolescent with depression with pharmacotherapy in the previous 12 months. Of the sample of 161 treating physicians, 60 were internal medicine specialists, 73 were psychiatrists, and 28 were certified specialists from the Japanese Society of Child and Adolescent Psychiatry, Japanese Society of Psychosomatic Medicine Pediatrics, or Japanese Society of Pediatric Psychiatry and Neurology. The participants completed questionnaires concerning their patient population with depression, drug-treated population, and drugs prescribed.
Results:
Estimates of prevalence data indicated that there were ∼550,000 adolescent patients with depression in Japan (10% of the patient population with depression) under medical care of different medical specialties; ∼64% of these patients were receiving pharmacotherapy. Pharmacotherapy for adolescents with depression was prescribed mainly by psychiatrists (62% of prescriptions for these patients). The most common first-choice agent was sertraline (23% of respondents) followed by anxiolytics (17%) and fluvoxamine (13%), while antipsychotics were the preferred choice for 7%.
Conclusion:
The study indicates a high prevalence of depression among adolescents in Japan. These patients are seen by different medical specialties; the use of pharmacotherapy is relatively common and comprises various drug classes, including antidepressants, anxiolytics, and antipsychotics. This study shows that there is a medical need for approved treatments for adolescents with depression in Japan.
Introduction
Mood disorders in children and adolescents are among the most debilitating illnesses, exerting a major impact on school performance, and family and social functioning, accompanied by a high risk of recurrence, substance abuse, psychiatric comorbidity, and suicidality (Fergusson and Woodward 2002; Birmaher et al. 2007; Perou et al. 2013; Avenevoli et al. 2015). Estimates of 12-month prevalence for major depressive disorder (MDD) are ∼1%–2% in childhood and ∼3%–8% in adolescence (Costello et al. 2006; Merikangas et al. 2010; Gledhill and Hodes 2015). In Japan, the prevalence for depression among children 12–14 years of age is 4.9% and the lifetime prevalence is 8.8% (Mizuta et al. 2017).
There has been an increased focus on the importance of mental health problems in children and adolescents in recent years, and trends suggest that, particularly in adolescents, the prevalence of depression has increased (Skurtveit et al. 2018). However, only a small proportion of adolescents with depression are treated by mental health professionals (Persico et al. 2015; Mojtabai et al. 2016; Merry et al. 2017; Cheung et al. 2018; Skurtveit et al. 2018).
Young people who seek help for depressive disorders usually attend primary care services, but only a minority are referred for specialist care. Significant differences exist in clinical practice between primary and specialist care settings for the treatment of MDD. There are also differences in clinical practice between countries (Persico et al. 2015; Cheung et al. 2018). A recognized gap in clinical guidance recently led a group of researchers and clinical experts from the United States and Canada to develop guidelines for medical care of adolescent depression in primary care, to assist clinicians in the management of these patients at a time of growing clinical need (Persico et al. 2015; Cheung et al. 2018).
The first-line recommended pharmacological treatment for depressive disorders comprises the selective serotonin reuptake inhibitors (SSRIs) (Locher et al. 2017). In the clinical care of young people with MDD, clinical guidelines recommend psychotherapy (especially cognitive behavioral or interpersonal therapy) as the first-line intervention, with the SSRI fluoxetine being considered only for patients with moderate-to-severe depression (especially adolescents). It is also recommended that, if depression continues, the decision to use pharmacotherapy should be taken by child and adolescent psychiatrists (Clark et al. 2012; Cipriani et al. 2016; Locher et al. 2017; Cheung et al. 2018).
The most important current unmet needs in pediatric psychopharmacology include the lack of effective medications for many pediatric psychiatric disorders and a paucity of positive data from randomized placebo-controlled trials conducted in the pediatric population (Emslie 2015; Gledhill and Hodes 2015; Persico et al. 2015). Placebo-controlled clinical trials in pediatric patients are needed to gain a better understanding of how to treat this population and to increase the availability of licensed therapeutic options. As also highlighted in a recent review of pediatric drug development in the United States, obtaining approval for drugs to treat psychiatric disorders in pediatric patients remains challenging, and strategies are required to encourage more clinical studies in this patient population (Grabb and Gobburu, 2017).
In Japan, there is limited research being conducted in this patient group. From clinical trial registries in Japan, it appears that some clinical trials with medications approved for the adult population have been initiated in the pediatric population in recent years; however, several years later, results do not appear to have been reported. The reasons behind this are not obvious, but it is known that poor patient recruitment may be at least partly responsible for the failure of pediatric studies to complete (Benkouiten et al. 2014; Bhatnagar et al. 2014).
Currently, only two antidepressants are approved for treating MDD in the pediatric population in the European Union and/or the United States: fluoxetine (Emslie et al. 1997, 2002), which is approved for patients ≥8 years of age, and escitalopram, which is approved for adolescents 12–17 years of age (Wagner et al. 2006; Emslie et al. 2009). There is currently no approved pharmacotherapy for pediatric patients with depression in Japan. Antidepressants approved for the treatment of depression in adults in Japan at the time the survey was conducted included escitalopram, paroxetine, sertraline, duloxetine, and milnacipran.
The study reported here aimed first to estimate the size of the current population of adolescent patients with diagnosed depression in Japan and the proportion of adolescent patients who receive pharmacological therapy; second, to gain a clearer understanding of the medical specialties that are treating adolescents with depression in Japan and current pharmacological treatment trends; and, finally, to identify unmet needs among the medical specialties treating these patients.
Methods
Two internet-based surveys were conducted of physicians involved in treating patients with depression in Japan. One survey aimed to estimate the prevalence of adolescent patients with depression, the physician specialties involved in treating these patients, and the current number of patients receiving pharmacotherapy for depression (prevalence survey). The second survey examined treatment trends and unmet needs among physicians treating adolescents with depression (treatment of adolescent depression survey). The surveys were conducted by Anterio, Inc. (Tokyo, Japan) in November 2014.
Selection of target respondents
Medical specialties and institutions throughout Japan that were considered likely to be treating adolescent patients with depression were identified and the survey questionnaire was made available (through an internet link) to hospital-based (HP) and office-based (GP) internists, psychiatrists, pediatricians, psychosomatists, and pediatric psychiatry specialists working in these facilities. Certified specialists belonging to the Japanese Society for Child and Adolescent Psychiatry, Japanese Society of Psychosomatic Pediatrics, or Japanese Society of Pediatric Psychiatry and Neurology were also invited to participate.
To estimate the distribution of physicians treating adolescents with depression and the current volume of adolescent patients receiving pharmacotherapy, a random sample was taken from each medical specialty (internal medicine, pediatrician, psychosomatist, and psychiatrist) and facility type (university hospital, psychiatric hospital, other public hospital, other private hospital, office, or clinic). The distribution of medical specialties in this sample (and their affiliation to the medical societies) was then weighted to match the structure of physician settings throughout Japan using the 2012 Ministry of Health, Labor and Welfare Physician Survey statistics to allow estimation of total adolescent patients with depression in Japan.
The pediatricians were defined based on academic society certification. However, owing to the lack of available data to determine the “pediatric psychiatrist” physician setting, estimates of the patients seen by these specialists were not created.
Prevalence survey
A sample of physicians from the selected medical specialties were asked questions about their patient population (total number seen in previous 12 months, total number of patients with depression/depressive state, and total number of adolescent patients [12–17 years of age] with depression/depressive state). For the adolescent patients with suspected or confirmed depression, physicians were then asked how many they had referred without initiating any treatment, how many they had prescribed pharmacotherapy, and how many they had treated with counseling/watchful waiting only. Physicians who said they had not prescribed pharmacotherapy for some of their adolescent patients with depression were asked to give their reasons (selected from a list of possible reasons and with the option to state other reasons) for taking this course of action, and to identify the single main reason for their decision.
Physicians were then asked to respond to the following four statements: “Diagnosing adolescent depression is difficult”; “Drug therapy is an effective option for treating adolescent depression”; “Choosing an appropriate drug therapy for adolescent depression is difficult”; and “Counseling is the best way to treat adolescent depression” using a 7-point scale where 1 = “Strongly disagree,” 2 = “Disagree,” 3 = “Somewhat disagree,” 4 = “Can't say either way,” 5 = “Somewhat agree,” 6 = “Agree,” and 7 = “Strongly agree.”
Treatment of adolescent depression survey
The second sample consisted of physicians who had prescribed pharmacotherapy to at least one adolescent patient with depression in the previous 12 months. These physicians were asked to participate in a more detailed survey about their adolescent patients. Questions included the number of adolescent patients with depression whom they had seen in the previous 12 months and how many had been referred to them by other physicians or health care practitioners (HCPs), the types of HCPs who most commonly referred patients with adolescent depression/depressed state to them, the severity of depression in the adolescent patients seen in the previous 12 months, and the treatment approaches selected (referred without initiating any treatment; prescribed pharmacotherapy; treated with counseling only; and watchful waiting only). They were then asked to give reasons for referring out adolescent patients with mild, moderate, and/or severe depression.
Regarding adolescent patients for whom they had prescribed pharmacotherapy in the previous 12 months, physicians were asked to identify which agents they had ever used, their first-choice agent (with reasons), whether they had a preferred class of antidepressant medication that they prescribe for these patients, and which antidepressants they prescribed for each level of depression severity.
Physicians were asked to rate their satisfaction with the current situation in Japan for treating adolescent patients with depression on a 7-point scale from 1 = “Not satisfied at all” to 7 = “Very satisfied,” and to identify the main unmet needs when treating these patients. They were also asked if they were aware of any agents with an indication for treating adolescent depression overseas or any studies conducted in adolescent patient populations overseas, and to rate (7-point scale, as above) how strongly they agreed or disagreed with the following statements: “There is a strong need for clinical evidence based on Japanese patients to guide treatment decision-making for adolescent patients with depression/depressive state” and “There is a strong need for an antidepressant that is indicated for the treatment of adolescent depression/depressive state.”
Physicians were also asked to consider if a well-known antidepressant from each of the SSRI, serotonin–norepinephrine reuptake inhibitor, or tricyclic/tetracyclic antidepressant classes obtained an indication for treating adolescent depression/depressive state in Japan, (1) how likely each would become their first-choice therapy (7-point scale) and (2) how they thought their use of pharmacotherapy in this patient population would change (increase, stay the same, or decrease). Finally, they were asked if they would be interested in participating in a clinical trial for an antidepressant with positive overseas data in adolescent patients with depression to provide scientific data for guiding treatment decisions in Japan (yes/no).
Results
Survey respondents
In the prevalence survey, from 3165 invitations to participate that were sent out, responses were obtained from 731 physicians in clinical practice. Among the responders, their primary specialty was as follows: 229 general internal medicine doctors (IMs) (23%), 233 pediatricians (31%), 41 psychosomatic medicine specialists (6%), and 228 psychiatrists (31%). Of these, 26 physicians (4%) were certified specialists.
In the second survey, from 1211 invitations that were sent out to physicians who had pharmacologically treated at least one adolescent patient with depression in the previous 12 months, 169 responses were received. Eight were rejected due to errors in completing the questionnaire, so a total of 161 physicians (14%) were included in the survey. Of these, 60 were IMs (28 GP IMs and 32 HP IMs) (37%), 73 were psychiatrists (40 GPs and 33 HPs) (45%), and 28 were certified specialists (17%).
Adolescents with depression in Japan
Based on the responses from the 731 physicians who completed the prevalence survey, estimates of the adolescent population with depression were calculated.
The results from this survey indicated that there were ∼550,000 adolescent patients with depression across Japan (∼10% of the total population of patients with depression) receiving medical care from the four specialties surveyed. Overall, across all medical specialties, the survey found that 64% of adolescent patients were prescribed pharmacotherapy (equating to 353,650 nationally), 20% were referred without initiating treatment, and 16% were treated with counseling or watchful waiting only.
The total number of physicians in Japan working in the four medical specialties surveyed was 93,097. Of these, an estimated 50,205 would have treated adolescent patients with depression or depressive state; an estimated 20,968 were IM GPs, 9836 were IM HPs, 2758 were pediatrician GPs, 4278 were pediatrician HPs, 640 were psychosomatists, 3065 were psychiatrist GPs, and 8660 were psychiatrist HPs. Nationally, an estimated 31,640 physicians would have prescribed pharmacological agents to their adolescent patients with depression.
The survey indicated that of the physicians who prescribed pharmacological agents to their adolescent patients with depression, 62% were psychiatrists (24% HPs, 38% GPs) and 31% were IMs (11% HPs, 20% GPs). Psychiatrist GPs were more likely to prescribe pharmacotherapy for their adolescent patients with depression (83% of patients) rather than referring the patient without initiating treatment (1%) or adopting a counseling/watchful waiting approach (15% of patients). In contrast, GP and HP pediatricians only prescribed pharmacotherapy to 35%–39% of their adolescent patients, preferring instead to rely on counseling or watchful waiting (26%–27% of patients), while 33%–39% were referred without initiating treatment. IMs also referred out approximately one-third (35%–38%) of their adolescent patients with depression without initiating treatment.
The most commonly cited reasons given by physicians for not prescribing drugs to their adolescent patients with depression were “Lack experience prescribing to adolescent patients” (42%); “Difficulties in confirming a depression diagnosis” (42%); “Prefer to refer patients requiring drug therapy to a specialist without initiating treatment” (41%); and “Not confident in selecting drug therapy for adolescent patients” (37%) (Fig. 1). “Lack of an approved antidepressant for adolescents in Japan” was given as a reason by 9% of physicians, while “No Japanese data available in adolescent patients with depression” was cited by 3%. “Prefer to refer patients requiring drug therapy to a specialist without initiating treatment” was the most common main reason given by physicians for not prescribing pharmacotherapy to their adolescent patients with depression (29% of physicians).
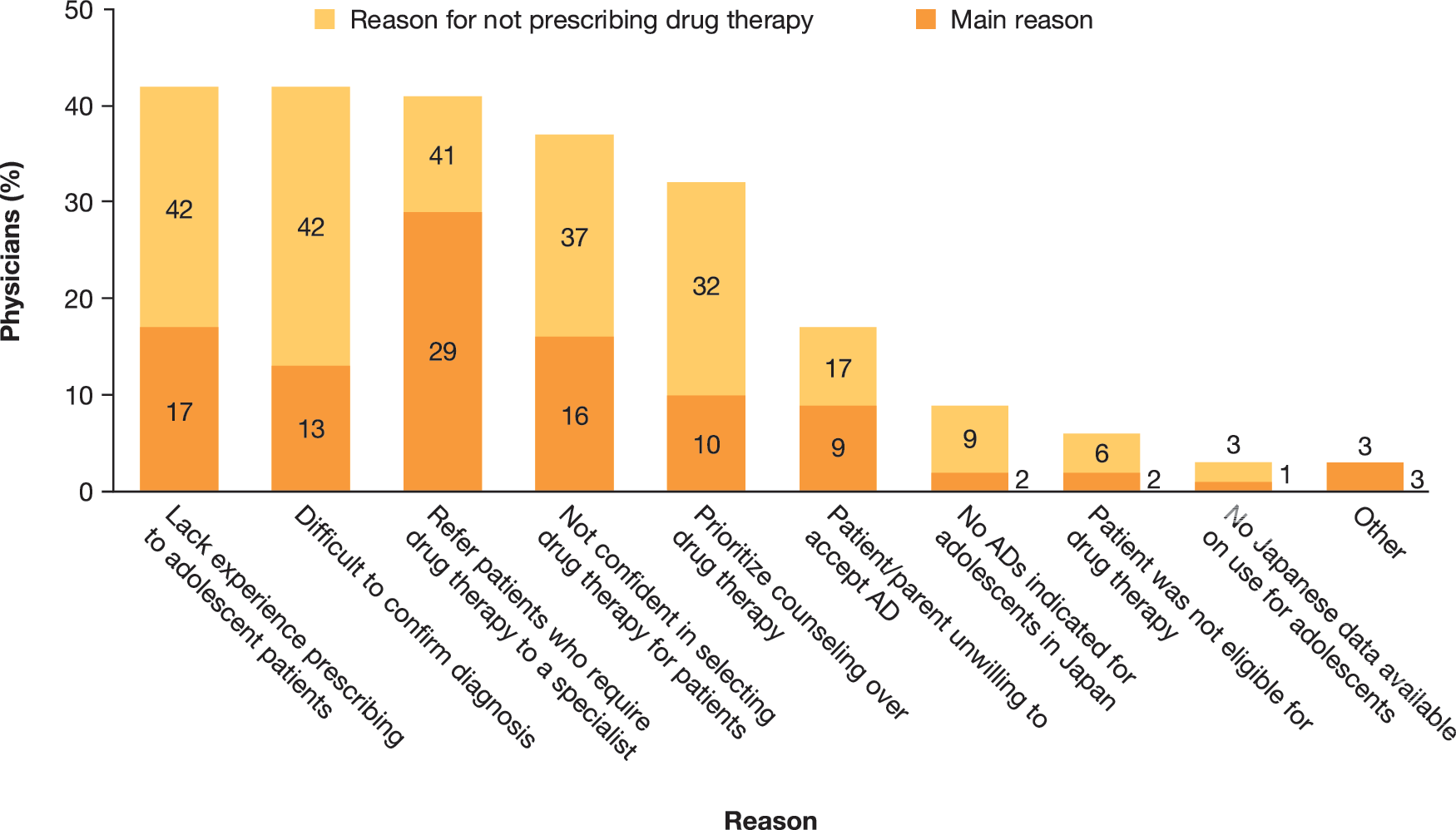
Reasons given by physicians for not prescribing pharmacotherapy to adolescent patients with depression/depressive state (prevalence survey). AD, antidepressant.
There was agreement among the respondents, including the psychiatric specialties, that diagnosing depression in adolescent patients is difficult or complex. Overall, 80% of physicians agreed at least “somewhat,” with the statement, “Diagnosing adolescent depression is difficult,” with 45% reporting that they “Agree” or “Strongly agree.”
Overall, 76% of physicians agreed at least “Somewhat” with the statement, “Drug therapy is an effective option for treating depression in adolescent patients,” with 42% reporting that they “Agree” or “Strongly agree.” Similarly, 75% of physicians agreed at least “Somewhat” with the statement, “Choosing an appropriate drug therapy for adolescent depression is difficult,” with 44% reporting that they “Agree” or “Strongly agree.” With regard to counseling approaches, 64% of physicians agreed at least “Somewhat” that “Counseling is the best way to treat adolescent depression,” with 32% reporting that they “Agree” or “Strongly agree.”
Management of adolescent patients with depression in Japan
Within the sample of 161 physicians, in terms of average patient number over the 12 months before the survey, the 28 certified specialists saw the highest number of adolescents with depression (n = 1005 patients; mean of 36 patients per physician) (Fig. 2). The 60 IMs saw the lowest number of adolescent patients with depression (n = 493; mean of 8 patients per physician), while the 73 psychiatrists saw 1509 adolescent patients (mean of 21 patients per physician). Adolescents comprised 49% of the total population of patients with depression seen by certified specialists, compared with just 7% of those seen by psychiatrists and 14% seen by IMs (Fig. 2).
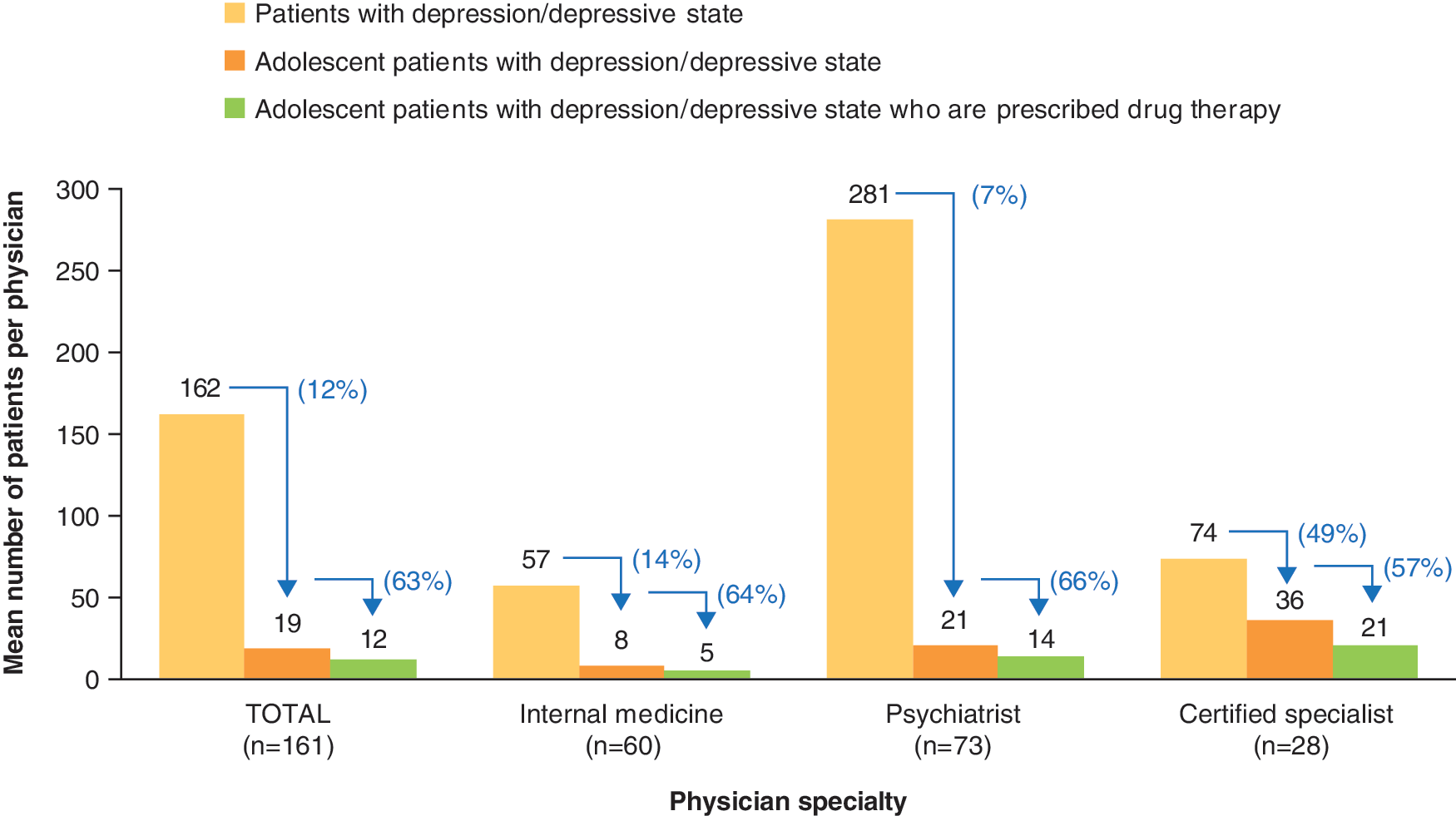
Mean number of patients with depression seen and the mean number of adolescent patients prescribed pharmacotherapy in the 12 months before the survey in the overall survey population (n = 161) and by medical specialty.
Approximately 57% of the certified specialists had seen, on average, at least 20 adolescent patients with depression in the 12 months before the survey. In contrast, only 10% of the IMs had seen an average of at least 20 adolescent patients, while 40% of the IMs had seen, on average, just 1–2 adolescent patients with depression in the previous 12 months.
Among the adolescent patients with depression, 63% had been prescribed pharmacotherapy across all specialties: 57% by certified specialists, 66% by psychiatrists, and 64% by IMs (Fig. 2). Certified specialists had the highest prescription rate in adolescent patients with depression (43% of them had prescribed pharmacotherapy to at least 20 patients in the previous 12 months compared with only 3% of IMs). Over 70% of the patients managed by IMs and psychiatrists had presented directly to them (77% for psychiatrists and 73% for IMs), while 58% of the patients seen by the certified specialists were referred to them from other medical specialties.
Approximately two-thirds (68%) of the 3007 adolescent patients seen by the 161 physicians had mild depression, 26% had moderate depression, and 6% had severe depression. The profile of intensity of depression in the adolescent patients seen by the different medical specialties was similar, with 67%–69% of cases categorized as mild and 5%–8% categorized as severe.
Overall, 57% of adolescent patients with mild depression were prescribed pharmacotherapy, rising to 76% and 77% of those with moderate and severe depression, respectively. One-third (33%) of the adolescent patients with mild depression were treated with counseling only, compared with 17% of the patients with moderate depression and 3% of those with severe depression. Watchful waiting was used for 8%, 2%, and 0% of patients with mild, moderate, and severe depression, respectively. In contrast, 20% of patients with severe depression were referred without initiating treatment compared with 3% and 5%, respectively, of patients with mild and moderate depression.
There were different approaches among the medical specialties regarding treatment of depression in adolescent patients, depending on the severity of the condition (Fig. 3). In patients with mild depression, certified specialists prescribed pharmacotherapy to fewer patients than did the IMs or psychiatrists (48% vs. 60% and 62%, respectively), and they treated more patients with counseling/watchful waiting only (48% vs. 14% and 28%, respectively). However, in patients with severe depression, ∼95% of adolescent patients seen by certified specialists were prescribed pharmacotherapy (compared with 82% and 62% of patients seen by IMs and psychiatrists, respectively) and only 5% of patients were referred without initiating treatment (compared with 32% of patients seen by psychiatrists and 16% of patients seen by IMs).
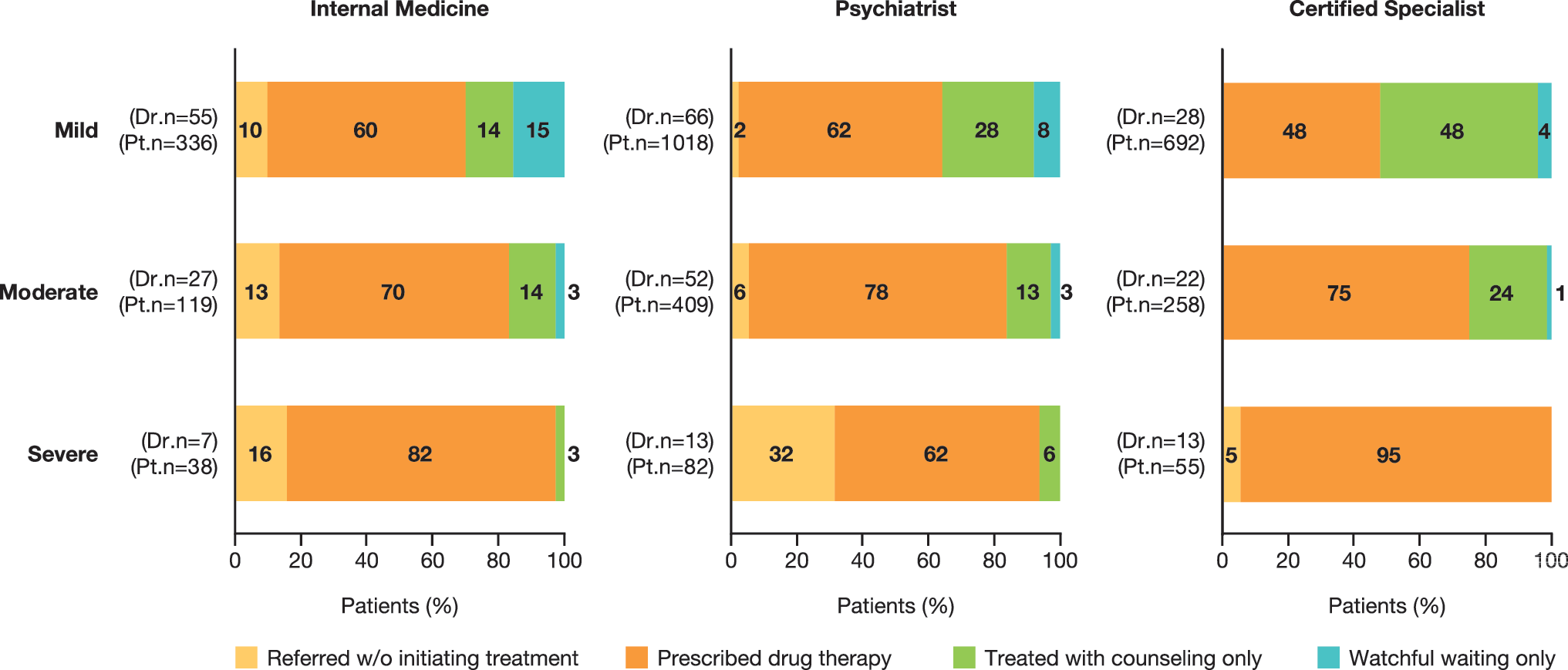
Treatment approaches used by different medical specialists for adolescent patients with mild, moderate, and severe depression. Dr.n, number of physicians; Pt.n, number of patients.
Regarding the treatments prescribed for adolescent patients with depression, physicians were asked which drug therapies they had ever prescribed for adolescent patients and which treatment they considered to be their first-choice agent. Across all medical specialties, anxiolytics were the most commonly prescribed medication overall, with 63% of physicians reporting having used them at least once for their adolescent patients (Fig. 4). Sertraline was the most common first-choice agent (selected by 23% of physicians), followed by anxiolytics (17%) and fluvoxamine (13%), while antipsychotics were the preferred choice for 7% of the respondents.

Drugs prescribed for adolescent patients with depression in Japan (n = 161). AD, antidepressant.
Overall, the most common reasons given by physicians for selecting their first-choice drug for adolescent patients with depression were “Has few side effects” (47% of total respondents), “Familiar with the product” (38%), and “Long history of clinical use in Japan and safety profile known” (29%) (Table 1). These were also the most frequently given reasons by each of the medical specialties; however, some differences between specialties were noted in the relative importance of other reasons given. For example, “Convenient dosing and/or administration” was given as a reason by 32% of IMs compared with 19% of psychiatrists and 21% of certified specialists. In contrast, the reasons “Drug is approved for use in adolescent patient populations overseas” and “Has been studied in adolescent patient populations overseas” were infrequently given by psychiatrists and IMs as reasons for selecting their first-choice drug (<10%); however, 29% and 21%, respectively, of the certified specialists cited these reasons.
Reasons Given by Physicians for First Choice of Drug Therapy Prescribed for Adolescent Patients with Depression/Depressive State
When the 27 physicians who reported an anxiolytic as their first-choice agent for treating depression in adolescent patients were asked for their main reasons, 56% cited “Has few side effects” and 67% cited “Familiarity,” but only 4% selected these agents because they were effective at relieving symptoms. When an antidepressant was selected as the first-choice agent for treating depression in adolescent patients, the SSRIs were the most common class chosen, preferred by 47% of the IMs, 52% of psychiatrists, and 64% of certified specialists.
The most common reason given by physicians overall for selecting fluvoxamine as their first-choice agent was the “Long history of clinical use in Japan and safety profile known” (cited by 48% of respondents). The most common reason given for selecting paroxetine was “Familiarity with product” (given by 53% of respondents), while “Few side effects” was the most common reason for physicians selecting sertraline (46%) or escitalopram (53%). Approximately 27% of IMs and 22% of psychiatrists did not have a preferred class of antidepressant for use in adolescent patients.
Overall, the prescription of anxiolytics for adolescent patients with depression decreased with the increasing severity of depressive symptoms. In patients with mild depression, 22% were prescribed anxiolytics compared with 7% of patients with severe depression. In contrast, the proportion of patients receiving SSRIs increased from 64% in those with mild depression to 74% of those with severe depression.
Differences in prescribing practices were observed among the individual medical specialties (Fig. 5). IMs treated more patients with paroxetine across all depression severities (37%–49%) compared with psychiatrists (9%–24%) or certified specialists (10%–25%), and fewer with mood stabilizers (1%–3% vs. 4%–12% and 9%–17%, respectively) and antipsychotics (1%–6% vs. 6%–10% and 9%–13%, respectively). Certified specialists treated more patients with mild depression with escitalopram (14%) compared with IMs (10%) and psychiatrists (7%). However, more patients with severe depression were treated with escitalopram by psychiatrists (18%) than by IMs (16%) or certified specialists (12%).
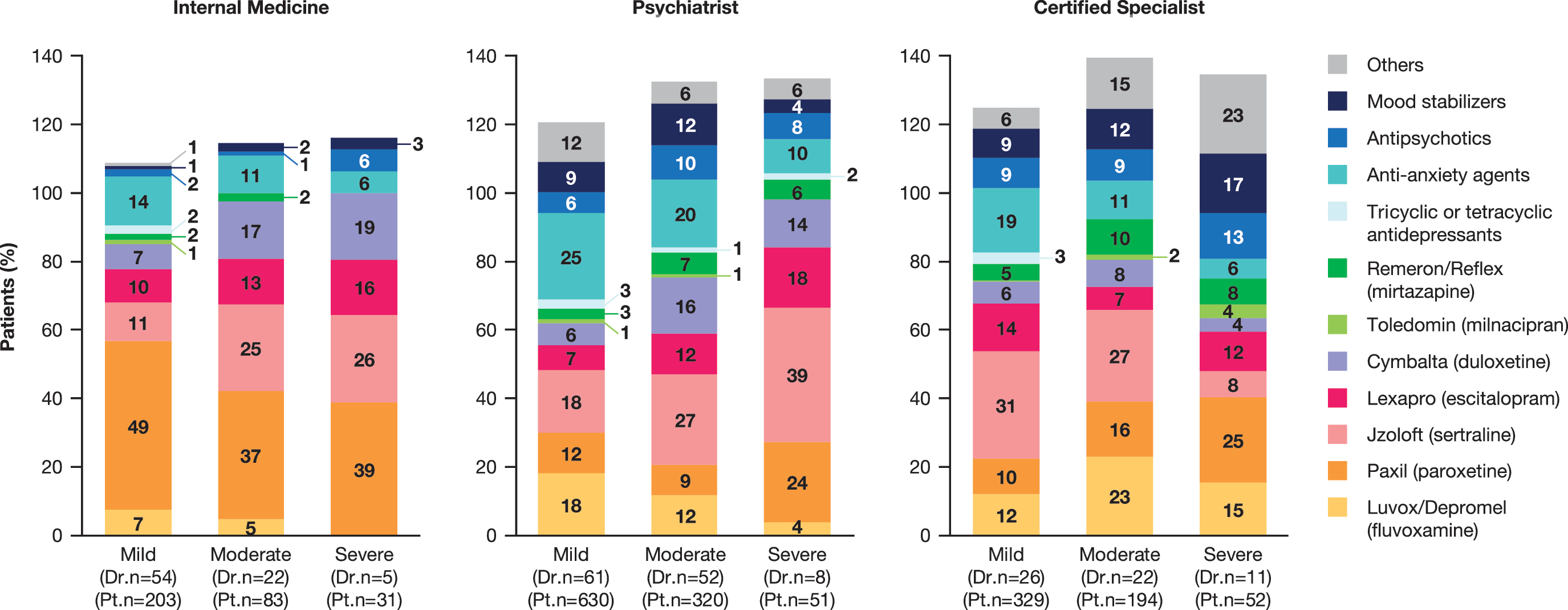
Drug therapies used by different medical specialists for adolescent patients with mild, moderate, and severe depression. Dr.n, number of physicians; Pt.n, number of patients.
Unmet needs among physicians
Overall, 40% of respondents were not satisfied with current options for treating depression in adolescent patients in Japan (responding “Not very satisfied,” “Not satisfied,” or “Not at all satisfied”), while 20% were “Somewhat satisfied” or “Satisfied.” None of the respondents were “Very satisfied.” Of the different medical specialties, the certified specialists were the least satisfied physicians (53% “Not very satisfied” or “Not satisfied”). The most common factor that positively influenced physicians' opinions regarding their satisfaction with the current situation in Japan when treating adolescent patients with depression was that adolescent depression was controllable, while the most common factors that influenced it negatively were lack of efficacy and difficulty of diagnosing depression in adolescent patients (Table 2). In total, 17% of the respondents answered that they did not know or lacked experience to evaluate the current treatment options, either positively or negatively, with the highest rate among IMs (22%).
Reasons Given by Physicians for Their Level of Satisfaction Regarding the Current Situation in Japan When Treating Adolescent Patients with Depression
SSRI, selective serotonin reuptake inhibitor.
The question asked was as follows:
“Why did you answer a certain level of satisfaction regarding the current situation in Japan when treating patients with adolescent depression/depressive state? Please be as specific as possible.”
Overall, the most commonly selected unmet needs in the treatment of depression in adolescent patients were “Lack of treatment guidelines in Japan” (cited by 46% of all respondents and 61% of certified specialists) and “Patient/parent resistance to using antidepressants” (cited by 42%) (Table 3). “Lack of specialists trained to treat adolescent psychiatric patients” and “Difficulty in diagnosing adolescent depression” were cited by 37% and 36% overall, respectively, while “Lack of an antidepressant with an indication for use in adolescent patients in Japan” and “Lack of efficacy and safety data for antidepressants in adolescent Japanese patients” were each cited by 34% of the respondents overall and by more than 50% of the certified specialists.
Unmet Needs Selected by Physicians Regarding Treatment of Adolescent Patients with Depression in Japan
The question asked was as follows:
“What would you consider to be the main unmet needs when treating adolescent depression/depressive state?” Respondents could give more than one answer.
Approximately one in four of the overall respondents indicated that they knew some of the SSRIs were indicated for adolescent depression overseas or had been investigated in this patient population (sertraline by 29% of respondents; escitalopram and paroxetine by 25% each). Approximately half (52%) of the overall respondents “Agreed” or “Strongly agreed” that there is a need for antidepressant treatments that are licensed in Japan for use in adolescent patients with depression (Fig. 6). The main reason that positively influenced the response to this statement was unwillingness to prescribe off-label drugs/better acceptance by the patients (22% of overall respondents and 32% of certified specialists).
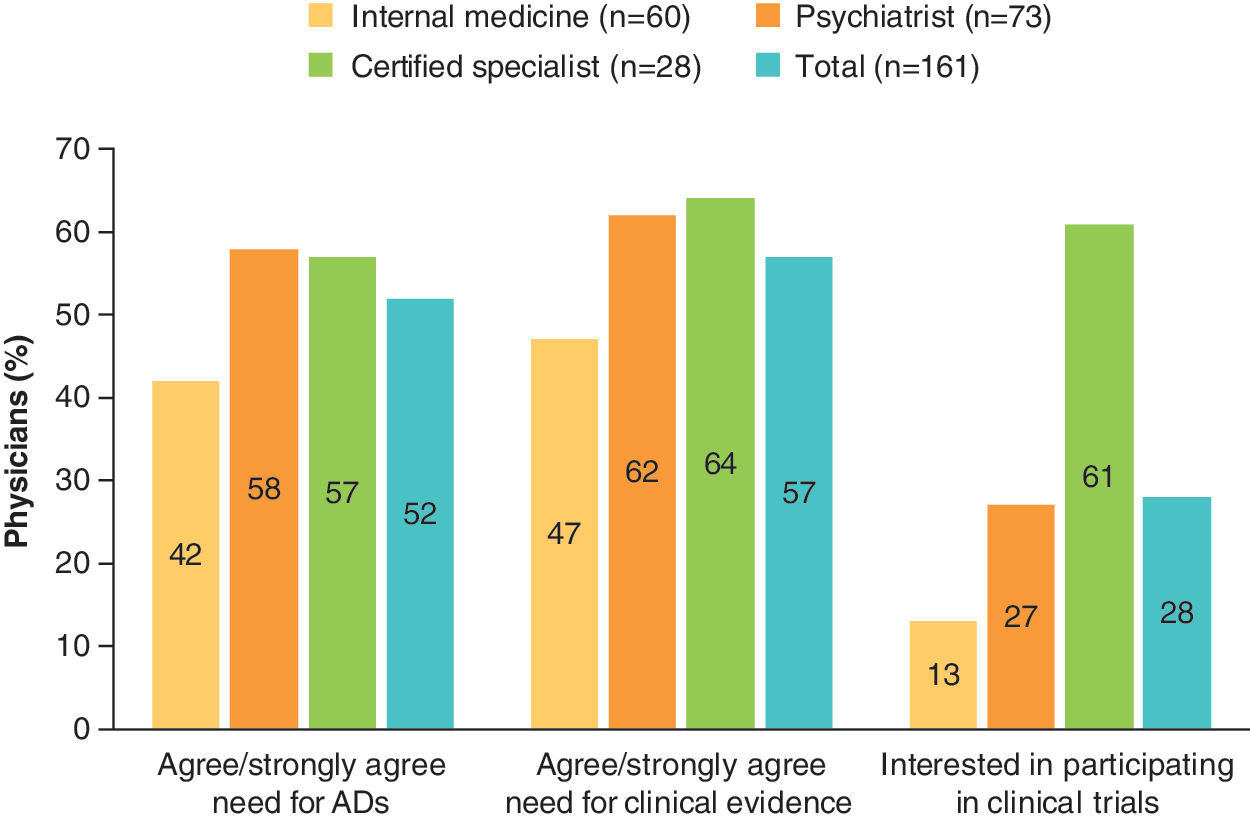
Level of physician agreement with the need for ADs that are indicated for use in adolescents with depression, for clinical evidence based on Japanese patients, and willingness to participate in clinical trials to obtain data in this population, by medical specialty. AD, antidepressant.
Almost 60% of the overall respondents “Agreed” or “Strongly agreed” that there is a need for clinical evidence based on Japanese patients to guide treatment for adolescent patients with depression (Fig. 6).
When asked whether they would be interested in participating in a clinical trial with an antidepressant that has positive data from overseas in adolescent patients with depression to provide scientific data for guiding treatment decisions in Japan, over 70% of overall respondents replied that they were not interested in participating in clinical trials (Fig. 6).
Discussion
This study supports the notion that pediatric depression is prevalent in Japan and may represent about 10% of the overall population of patients with depression. It also confirms that there is a general medical need for treatment of adolescent patients with depression in Japan. This is consistent with reports from outside Japan that depressive disorders are among the most common mental disorders in children and adolescents (Locher et al. 2017). Moreover, the study described which medical specialties are treating these patients, with psychiatrists and IMs accounting for most prescriptions for adolescents.
The drug treatment rate in adolescent patients is relatively high at 64%, and pharmacotherapy as an effective treatment for adolescent depression is generally accepted by all specialties. This picture is consistent with population-based data from other countries in Asia, which demonstrate a relatively high prescription rate in pediatric/adolescent patients, with the most commonly prescribed agents being SSRIs, such as sertraline, fluoxetine, and escitalopram, for depression as the most common indication (Chon et al. 2017; Deng et al. 2018).
The apparently large off-label use reported in these studies might reflect the relative paucity of available proven therapeutic options (Chon et al. 2017; Deng et al. 2018). The results from this study are also in line with population-based data from countries such as Germany and Australia, where the prescription rate is considered to be high in children and adolescents, with most antidepressants being prescribed by child and adolescent psychiatrists, internal- and general-medicine physicians, and pediatricians (Karanges et al. 2014; Franke et al. 2016; Schröder et al. 2017). The most common diagnosis was depression in these studies.
It was concluded that there is a high rate of off-label use, although it was noted that data on dispensing of antidepressants indicated a trend toward prescribing based on guidelines and evidence (Karanges et al. 2014; Franke et al. 2016; Schröder et al. 2017). In the United States, prevalence data show an increase in adolescent patients with major depression, mostly treated in pediatric settings, but they also reveal trends for a growing number of young people with untreated depression (Mojtabai et al. 2016).
In the present study, across all severity categories of depression, more than half of the patients were prescribed drug treatment, ranging from 57% of those with mild depression to 77% of those with severe depression. Approximately, 33% of the patients with mild illness and 3% of those with severe depression were treated with counseling only. There was little agreement among respondents that counseling is the best way to treat adolescent patients with depression.
In the absence of data on Japanese pediatric depression, the choice of drug may be difficult. In Japan, there are currently no approved antidepressant treatments for pediatric patients with depression. In addition, at the time that this survey was conducted, there was a lack of clear treatment guidance for adolescents. The lack of approved antidepressants for adolescents in Japan and lack of data available in Japanese adolescent patients with depression were selected as reasons for not prescribing pharmacotherapy by less than 10% of the physicians. The most commonly cited reasons for not prescribing drugs to adolescent patients with depression were lack of experience in prescribing to adolescent patients, diagnosis being difficult or complex, and patients requiring pharmacotherapy being referred to a specialist.
The guidelines for diagnosis and treatment for depression in adults in Japan were revised in 2016 (Japanese Society of Mood Disorders 2016) and a chapter on child and adolescent depression was added, in response to the increasing prevalence of child and adolescent depression and criticism regarding the lack of guidelines for this age group. Because of the lack of clinical studies in Japan—in particular, double-blind clinical trials assessing efficacy, safety, and tolerability—the chapter was written based on the clinical evidence from outside Japan and on the consensus of Japanese experts in this area. In brief, the chapter recommends, as the first step, a comprehensive diagnostic approach, adequate psychosocial education regarding the illness, and supportive intervention for both the patient and the family.
With regard to pharmacotherapy, escitalopram is recommended for patients older than 12 years, and sertraline for those older than 6 years, with appropriate informed consent that notes these drugs are being recommended off label and have potentially serious side effects such as suicide-related behaviors. The use of tricyclic antidepressants and benzodiazepines is not recommended in these guidelines.
In terms of psychotherapy, cognitive behavioral therapy (CBT) and interpersonal psychotherapy are recommended under the supervision of well-trained therapists, even though there is no evidence in Japan that these approaches are significantly superior to watchful waiting. The Treatment for Adolescents with Depression study (TADS) showed that the combination of fluoxetine and CBT significantly accelerates benefits relative to CBT alone or fluoxetine alone in the treatment of moderate-to-severe MDD in adolescents (March and Vitiello 2009). Consequently, expert clinicians often recommend combined treatment as the treatment of choice in this population.
The usefulness of the Japanese guidelines is clear; for example, in advising against use of benzodiazepines, it should prevent inappropriate drug choices. This survey showed that 17% of physicians chose anxiolytics for first-line treatment of depression, due to familiarity and fewer side effects. Evidence-based guidelines would further improve the treatment of depression in Japanese adolescents; however, evidence from clinical trials in Japanese adolescents with depression is required.
Limitations
This study has some limitations, which may influence the interpretation of the results and which need to be considered. The sample size may be considered small; there were relatively low response rates of ∼23% and ∼14%, respectively, for the prevalence and treatment surveys. In addition, the national prevalence estimates were based on an assumption that the data from the medical specialties sample could be extrapolated to the total population of physicians treating pediatric depression; this assumption introduces a degree of uncertainty. The data may not cover all SSRI or antidepressant dispensing; thus, the results could underestimate the use of antidepressants. Another limitation is the comparison with similar surveys outside of Japan, as there are several studies of antidepressant use, but these are often based on other sources, such as prescription databases.
Conclusion
There is a high prevalence of depression in adolescents in Japan. These patients are seen by different medical specialties; the use of pharmacotherapy is relatively high and includes a variety of medicines, such as antidepressants, anxiolytics, and antipsychotics, even though no psychopharmacotherapy is approved for adolescent depression in Japan. Taken together, these results highlight the need for approved treatments for adolescents with depression in Japan.
Clinical Significance
Depression is a psychiatric disorder characterized by severe and/or persistent symptoms, which can cause considerable distress and interfere with daily activities. Untreated, this may lead to serious risks such as suicide at worst, but also developmental, personal, and societal difficulties, which may compromise school success, work productivity, adult development, and formation of relationships. Patients with depression may require psychological intervention and may benefit from pharmacotherapy.
Footnotes
Acknowledgments
The authors thank the staff at Anterio, Inc. for conducting the survey and analyzing the data. Editorial assistance with the final draft was provided by Janet Dawson of Anthemis Consulting Ltd, funded by H. Lundbeck A/S.
Disclosures
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.F., E.H.R., and M.K.D. are employees of H. Lundbeck A/S. T.S. did not receive any financial support from H. Lundbeck A/S or other sources in regard to this article; he has received personal honoraria from H. Lundbeck A/S for participation in an advisory board relating to vortioxetine. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: data for this article were derived from a clinical survey sponsored by Lundbeck Japan, Tokyo. Under the direction of the authors, the data were analyzed by Anterio, Inc. (Tokyo, Japan). The authors interpreted the data and wrote the article; editorial assistance with the final draft was provided by a medical writer.