
Abstract

Ketamine, an n-methyl-d-aspartate receptor antagonist, was first studied for its antidepressant properties in the 1990s, and is only now gaining popularity as an alternative for treatment-resistant depression in adults (Sanacora et al. 2017; Fitzgerald and O'Malley 2014). It is unique in that it is proposed to exert antidepressant effects through multiple pathways, including dendritic morphogenesis, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid activation, and opioid receptor agonism. Unfortunately, ketamine is still in a rudimentary stage for use in adolescent depression (Cullen et al. 2018; Dwyer et al. 2017). At best, pediatric depression response rates to monotherapy using traditional antidepressants range from 60% to 70%, necessitating alternative treatments in refractory adolescent depression. In this study, we present a case of a youth with severe treatment-resistant depression, with psychotic features, and prolonged inpatient psychiatric hospitalization of >1 year, who responded successfully to a course of ketamine infusions:
A 15 year-old adolescent presented to our inpatient unit after a toxic ingestion of sertraline. Patient reported a 6-month history of worsening depressive symptoms, including suicidal ideation. The teen, diagnosed with major depressive disorder, generalized anxiety disorder, and post-traumatic stress disorder stemming from sexual abuse, showed no benefit from initial treatment with escitalopram 20 mg/day. Patient subsequently failed adequate trials of antidepressants (sertraline, fluvoxamine, imipramine, and venlafaxine), adjunctive anxiolytics (lorazepam and clonazepam), and prazosin for nightmares. The adolescent consequently began to display psychotic symptoms (auditory/visual/tactile hallucinations) and worsening symptoms of regression, suicidality, muteness, self-harm, and medication refusal. Psychological testing indicated severe depression with severe impairment in reality testing. Augmentation with antipsychotics (aripiprazole, olanzapine, chlorpromazine, and ziprasidone) had no effect on symptomatology. Attempts to obtain electro-convulsive therapy were unsuccessful due to the legal controversies in Oregon surrounding this treatment in minors.
Eventually, patient was administered a course of six ketamine infusions dosed at 0.5 mg/kg per infusion for the course of 3 weeks, starting with three infusions a week and gradually tapering down to once a week. We followed symptomatology through patient's subjective report, rating scales (Fig. 1), and clinical observations of mental status. As denoted in the figure, we observed gradual decreases in depressive symptoms (Montgomery–Asberg Depression Rating Scale, Children's Depression Rating Scale), and suicidality (Scale for Suicidal Ideation) after infusions. The only reported side effects were symptoms of derealization and nausea, which were managed with administration of low-dose chlorpromazine preinfusion. It is prudent to note that despite objective improvements in symptomatology, patient continued to subjectively deny improvement until 2 weeks after final infusion.
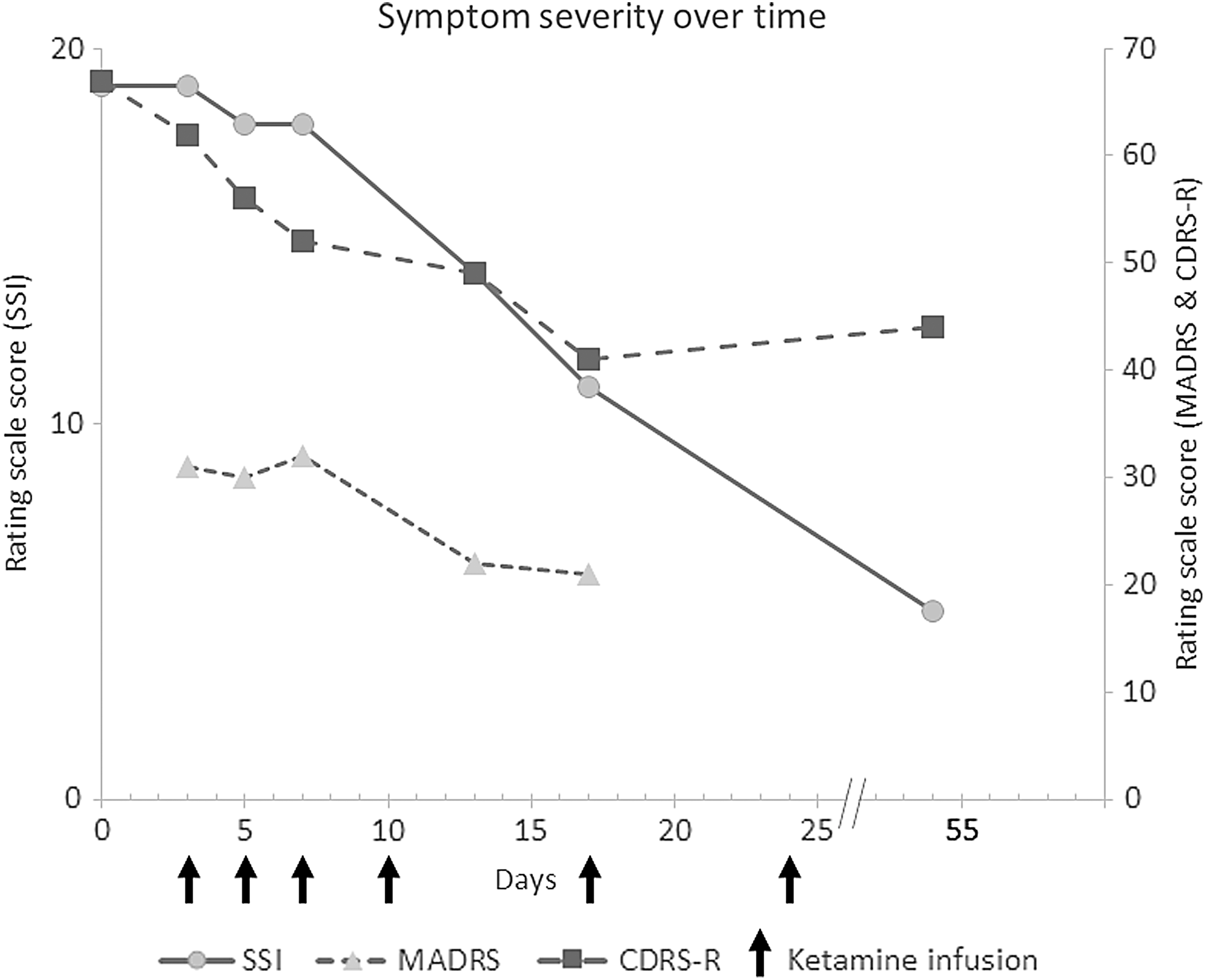
Ketamine infusions (denoted by arrows on X-axis) alongside depressive symptoms (indicated by MADRS and CDRS) and suicidality (indicated by SSI) on Y-axis. CDRS, Children's Depression Rating Scale; MADRS, Montgomery–Asberg Depression Rating Scale; SSI, Scale for Suicidal Ideation.
Patient was successfully discharged into community care 1 month after completion of ketamine infusions on the last medication regimen of venlafaxine, ziprasidone, and prazosin—with the absence of depressive, psychotic, or suicidal symptoms—and continued to do well during our follow-up of the ensuing several months.
Discussion
Ketamine in this case was safely administered to an adolescent with psychotic depression, and significantly reduced both psychotic and depressive symptoms. We estimate that using ketamine may be helpful for other adolescent patients who have exhausted therapeutic options in treatment-resistant and psychotic depression.
Footnotes
Disclosures
No competing financial interests exist.