
Abstract
Objectives:
The prescription of psychotropic medication used to treat psychiatric disorders has increased worldwide over the past two decades and has been discussed widely in the literature; however, limited data have been available for New Zealand. The current article aimed to address this knowledge gap.
Methods:
Prescription data obtained from The Pharmaceutical Management Agency of New Zealand (PHARMAC) were analyzed to obtain prescription dispensing rates and trends for antidepressants, antipsychotics, anxiolytics, sedatives and hypnotics, and stimulants/attention-deficit/hyperactivity disorder medications for youth aged 0–17 years in New Zealand during 2008–2016, including a gender and ethnicity breakdown for 2016 to provide a “snapshot” of prescription demographics. These data sets contained all individual prescriptions dispensed in New Zealand during this time period, alongside a unique encrypted National Health Index number to distinguish individuals and demographic data.
Results:
In 2016, 2.36% of New Zealand youth, totaling 26,175 individuals, were prescribed at least one psychotropic medication, an increase of 65.03% from 2008. Rate of prescription for youth in 2016 and percentage increase since 2008 for each medication class were as follows: antidepressants: 1.07%, 78.33% increase; antipsychotics: 0.37%, 105.60% increase; anxiolytics: 0.15%, 50% increase; and sedatives and hypnotics: 0.22%, 37.50% increase. Stimulants were prescribed to 1.06% of the population, a 41.33% increase since 2011. In 2016 the number of prescriptions was split roughly equally between males and females, with more males receiving stimulant prescriptions and more females receiving antidepressant prescriptions. Stimulants were the medication most likely to be prescribed to Māori, Pacific, and Middle Eastern/Latin American/African groups, with antidepressants most likely for European and Asian groups. Māori tended to be prescribed medications at rates lower than the general population.
Conclusions:
Overall, prescription rates and the increase in prescription of psychotropic medication to children and adolescents in New Zealand fall within the mid range compared to other Western countries worldwide.
Introduction
The prescription of psychotropic medication used to treat psychiatric disorders, such as antidepressants, antipsychotics, and stimulants, has increased worldwide over the past two decades, as seen across countries such as the United Kingdom, the United States, and Australia (Olfson and Marcus 2009; Ilyas and Moncrieff 2012; Stephenson et al. 2013), as well as New Zealand (Wilkinson and Mulder 2018a, 2018b).
This increase has also been evident in the children and adolescent prescribing internationally. For example, Bachmann et al. (2016) reported that the prescription rates of antidepressants for youth in 2012 had increased from 2005 in the United States, United Kingdom, Denmark, the Netherlands, and Germany by 26.1%, 54.4%, 60.5%, 17.6%, and 49.2%, respectively. In Australia, there has been an increase of 16.1% over 3 years between 2009 and 2012 (Karanges et al. 2014). The use of antidepressants for the treatment of mood disorders in children and adolescents is partially supported by research. For example, a recent meta-analysis of data from 34 trials found that fluoxetine was statistically significantly more effective in treating youth than a placebo; however, all other antidepressants were found to be no better than placebo (Cipriani et al. 2016). Antidepressants are also used clinically for other indications, including obsessive–compulsive disorder and some anxiety disorders (Geller et al. 2012).
Similarly, rates of prescriptions for antipsychotics have increased globally. Australian data showed an increase of 22.7% for youth antipsychotic prescriptions during 2009–2012 (Karanges et al. 2014). Kalverdijk et al. (2017) reported an increase from 2005 to 2012 across the United Kingdom, Germany, Denmark, and the Netherlands of 40%, 39.13%, 84.62%, and 32.05%, respectively. Recent meta-analyses indicate that most antipsychotics have some short-term established efficacy in children and adolescents with psychotic disorders (Ayub et al. 2018; Krause et al. 2018), severe irritability in autism spectrum disorder (Volkmar et al. 2014), and conduct problems (Loy et al. 2017); however, the potential for side effects is high, and the authors suggest careful diagnostic evaluation and ongoing monitoring (Ayub et al. 2018). Less is known about longer term efficacy and safety, for example, in the Krause et al. (2018) meta-analysis for psychosis, the trial durations ranged from just 4 to 12 weeks.
With respect to prescription of anxiolytics for young people, global trends suggest that prescriptions have remained more stable, particularly for hypnotics. Steinhausen (2015) noted two studies showing stable trends. In Iceland between 2003 and 2007, the prevalence ranged from 1.5 to 2.0 per 1000 children and adolescents, and Denmark had prevalence rates of 0.44 per 1000-person years across the population in 1996 and 0.33 per 1000-person years in 2010 (Steinhausen 2015). However, a cohort study in the United Kingdom by John et al. (2015) found that while the trend of anxiolytic prescription for those aged 6–14 years has been fairly constant, there has been a significant increase for those aged 15–18 years, from 3.00 to 4.91 cases per 1000-person years. Australian data indicated little change in the rate of anxiolytic dispensing between 2000 and 2011 to the general population (Stephenson et al. 2013). A recent meta-analysis looked at the efficacy of benzodiazepine anxiolytics for the pediatric population (Kuang et al. 2017). While short-term efficacy in a procedural setting (e.g., surgery or dental procedures) was supported, the authors noted that very little literature existed on use for anxiety disorders in children and adolescents (Kuang et al. 2017).
Stimulants belong to a class of medications that have the most research to support their use in children and adolescents, with a recent meta-analysis and systematic review reporting efficacy for 12 weeks (Cortese et al. 2018). Raman et al. (2018) found a pooled prevalence rate across 13 countries of 2.0% for youth aged 3–18 years old. Rates of prescription ranged from 0.7% to 0.9% in Western Europe, Asia, and Australia to 4.5% in North America. Findings also showed that rates had increased in every country, at an average of 14.6% per year, ranging from the lowest at 2.8% per year during 2001–2014 in the United States to the highest in Canada, where there was an increase of 45.1% between 2001 and 2009. Karanges et al. (2014) found an increase of 26.1% for youth attention-deficit/hyperactivity disorder (ADHD) medication prescriptions between 2009 and 2012 in Australia.
New Zealand background
New Zealand has five major ethnic groups. In the 2013 census the population was 74% European, 14.9% Māori, 11.8% Asian, 7.4% Pacific peoples, 1.2% Middle Eastern/Latin American/African, and 1.7% other (Statistics New Zealand 2014). Of note, people were able to identify with more than one ethnic group.
New Zealand's health system provides universal health coverage to residents, and the majority of prescribed medications are heavily subsidized by the government, with a maximum 5 dollar co-payment when medications are dispensed (Ministry of Health 2018). This fee is waived for children under 13 years and low income earners (Ministry of Health 2018).
To date, there are limited published data on prescribing rates and trends for children and adolescents in New Zealand. Hálfdánarson et al. (2017) reported antipsychotic prescription rates during 2005–2014 for 16 countries, including New Zealand. This report included figures for the age group of 0–19 years. The current article sought to document the prescription rates over the last decade of the most commonly used psychiatric medications for children and young people.
Guidelines
Guidelines for the prescription of psychotropic medications for children and adolescents in New Zealand are provided in the New Zealand Formulary for Children (NZFC) (2018), as well as by the National Institute for Health and Care Excellence (NICE) (National Institute for Health and Care Excellence 2019) and practice parameters for various disorders and the use of psychotropic medication in children and adolescents from the American Academy of Child and Adolescent Psychiatry (AACAP) (American Academy of Child and Adolescent Psychiatry 2019). The guidelines provided by NZFC advise caution around prescribing antidepressants to children and adolescents and note links with an increase in suicidal thoughts and behaviors for this age group. The NZFC also advises that only fluoxetine has been shown to have a favorable risk-benefit profile for the treatment of depression for this age group. NZFC guidelines for antipsychotic prescription advise that there is little efficacy and safety information available regarding their use for children and adolescents, and antipsychotic use in young people should be closely supervised (New Zealand Formulary for Children 2018). The NZFC advises that medication therapy in the treatment of anxiety should only be provided by specialists after other psychosocial interventions have been unsuccessful and that the prescription of hypnotics cannot be justified except for occasional use, for example, to sedate for a dental procedure. Guidelines provided by the NZFC advise that stimulants are an approved treatment for ADHD in children and adolescents.
Methods
Prescription data were obtained from the Ministry of Health (MOH). Data were obtained for the medication classes: antidepressants, antipsychotics, anxiolytics, sedatives/hypnotics, and stimulants/other ADHD medications. Other medication classes that came under “Nervous System” categorization by The Pharmaceutical Management Agency of New Zealand (PHARMAC) but were not primarily used to treat mental health problems were excluded (e.g., antiepilepsy medications). See Appendix A1 for a full list of medications included in each class. Every available formulation for each medication was included. The data were broken into individual data sets based on year, from 2008 to 2016.
Each of the data sets contained every prescription dispensed for the specified medications for that year prescribed to a person under the age of 18 years. These data created a unique opportunity for the exact number of prescriptions dispensed to be investigated, as opposed to forming an estimate based on a sample. The data were collected through PHARMAC alongside the encrypted National Health Index (NHI) number of the person receiving the prescription and demographic data for the individual. An NHI number is a unique identifying code given to every person in New Zealand who accesses health services.
A table was provided by MOH which listed when each individual medication has 90% NHI completeness within their records, that is, at least 90% of prescriptions for that medication are recorded with an NHI number, which is the point at which the data can be released. The date range 2008 to 2016 was selected to analyze, as by 2008 most medication data were complete. The exception to this was stimulants, which were mostly complete by 2011, so were analyzed from this year.
The current study looked at the total prescription count per year of each class of medication. This allowed for the analysis of trends over time, including whether the rate of prescribing is increasing, decreasing, or remaining stable. Gender data were also obtained for each of the 9 years to identify whether there were differences in prescription rates across gender. For 2016, the data were analyzed according to ethnicity and age to create a “snapshot” of prescribing patterns in New Zealand for this year.
Population data were obtained from Statistics New Zealand using their population estimator (Statistics New Zealand 2019). This allowed for the percentage of individuals prescribed each medication each year to be more accurately calculated, as opposed to using official census data, which were only available for the year 2012.
Ethnicity categories were based on the categories used by the MOH for consistency with the data provided. These groups were as follows: European, Māori, Pacific Island, Middle Eastern/Latin American/African, Other, and Residual. The use of the Residual category indicated that the person did not know, had refused to answer, their response was unidentifiable, or had not been stated. While a person can identify up to three ethnicity groups to the MOH, we used the person's self-identified primary ethnicity only for analysis.
Statistics
Microsoft Excel was used to analyze the data sets. Data are descriptive and are presented as both total figures, as well as percentage of the population.
Results
National rates
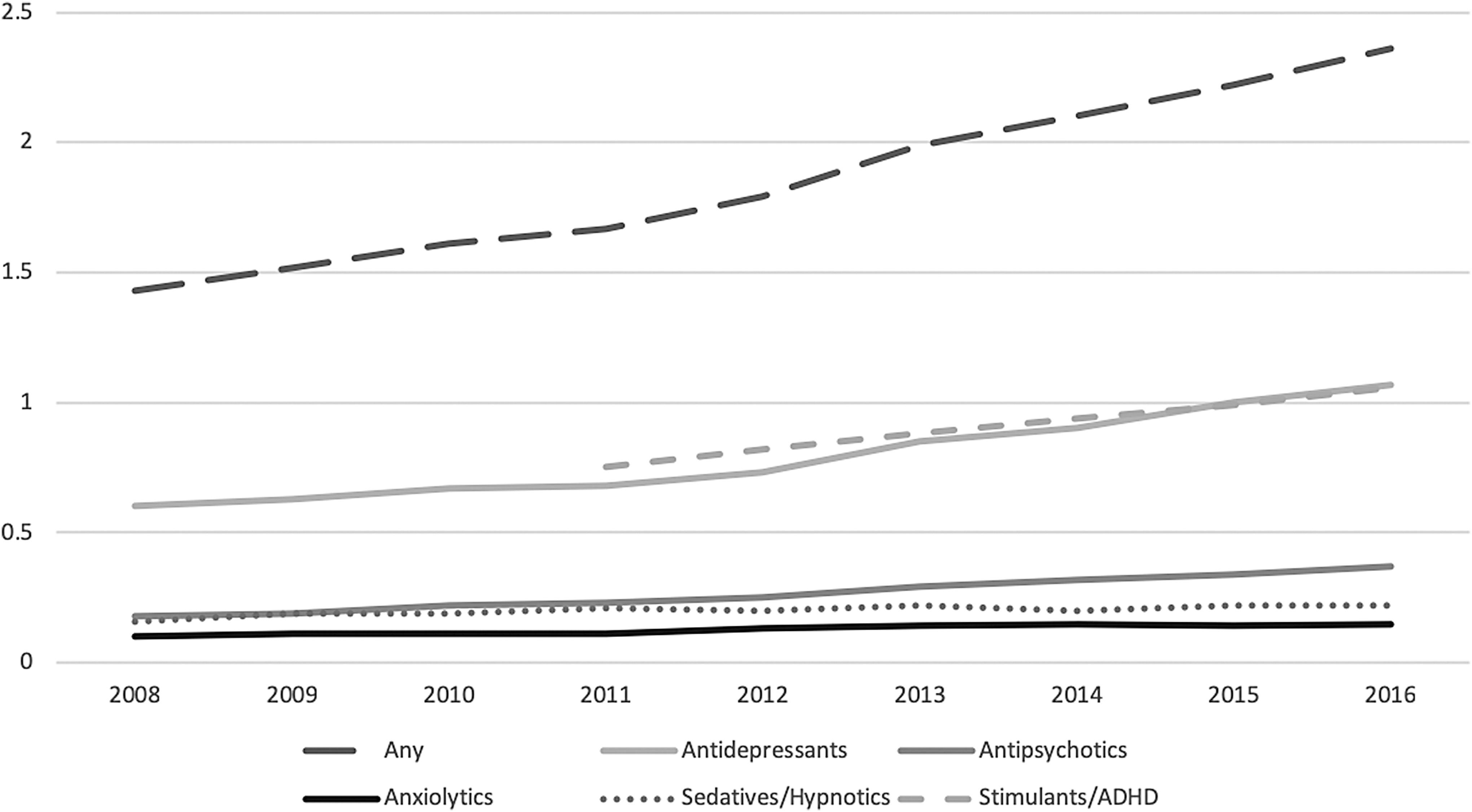
In 2016, 2.36% of all New Zealanders aged 18 years and under were prescribed at least one psychotropic medication, totaling 26,175 individuals. Table 1 shows the percentage of children and adolescents prescribed each medication class, as well as the percentage increase during 2008–2016. Figure 1 shows the prescription trends for each type of medication. The rate of prescription increased each year from 2008, which had a prescription rate of 1.43%, resulting in a 65.03% increase in prescriptions from 2008 to 2016. An increase was seen in the rates of prescription for all medication classes. The rates of antidepressant prescription increased from 0.60% in 2008 to 1.07% in 2016, an increase of 78.33%. Total antipsychotic prescription increased from a rate of 0.18% of youth in 2008 to 0.37% in 2016, an increase of 105.60%. First generation antipsychotics decreased slightly from being prescribed to 0.007% in 2008 to 0.006% in 2016, a decrease of 14.29%. Second generation antipsychotic prescription increased, from 0.17% of youth in 2008 to 0.37% in 2016, an increase of 113.93%. Notably, quetiapine prescriptions increased by 256.70% from 2008 when the prescription rate was 0.059% to 0.211% of youth in 2016. Anxiolytic prescriptions increased from 0.10% in 2008 to 0.15% in 2016, increasing by 50.00%. Sedatives and hypnotic prescriptions were given to 0.16% of youth in 2008 and to 0.22% in 2016, an increase of 37.50%. Stimulant/ADHD medication prescription rates also increased, from 0.75% in 2011 to 1.06% in 2016, an increase of 41.33%.
Percentage of New Zealand children and adolescents prescribed psychotropic medications during 2008–2016, by medication class.
Percentage of New Zealanders Under 18 Prescribed Each Drug Class and Percentage Increase 2008–2016
Stimulant percentage increase is during 2011–2016.
Fluoxetine made up 47.5% of antidepressant prescriptions in 2016. The proportion of different types of antidepressants changed over time; Table 2 provides a breakdown. Individuals may have received a prescription for more than one type of medication over the course of the year, so the percentage of medication types totaled to slightly higher than 100%. In 2008, 31.49% of those receiving an antidepressant prescription received a prescription for a medication in the tricyclic category, and 71.30% received a selective serotonin reuptake inhibitor (SSRI). In 2016, 19.06% received a tricyclic prescription, and 82.15% received an SSRI prescription. The Other category, which included Venlafaxine and Mirtazapine, rose from 2.19% in 2008 to 4.20% in 2016.
Percentage of Individuals Receiving Antidepressant Prescription 2008–2016 Who Received a Prescription of Each Subclass
MAOI, monoamine oxidase inhibitor; SSRI, selective serotonin reuptake inhibitor.
Gender
In 2016, 55.22% of the total prescriptions were for males and 44.78% for females. Figure 2 shows the differences in the gender breakdown for each medication type. The gender balance remained reasonably stable, from 57.46% prescriptions for males and 42.54% for females in 2008. Males were prescribed stimulants at a much higher rate than females and a much lower rate for antidepressants. Sedatives and hypnotics and anxiolytics were prescribed slightly more to females. Antipsychotic prescriptions had an even gender split.

Number of prescriptions given to males and females in 2016, by medication class.
Ethnicity
Figure 3 shows how each ethnicity group's total prescriptions were broken down into medication type in 2016. Youth in the Māori, Pacific Island, and Middle Eastern/Latin American/African groups were more likely to be prescribed stimulants than other medications, whereas antidepressants were more likely to be prescribed for European and Asian groups.

Percentage breakdown of total prescriptions for each medication class in 2016, by ethnicity.
Māori tended to be prescribed medications at rates lower than the general population. Figure 4 shows the percentage of Māori who were prescribed each class of medication, compared with the percentage of the total population who were prescribed each medication. Māori rates are closest to general population rates for stimulants, antipsychotics, and sedatives/hypnotics; however, there are noticeably lower rates of prescription for anxiolytics and antidepressants compared with the total sample.
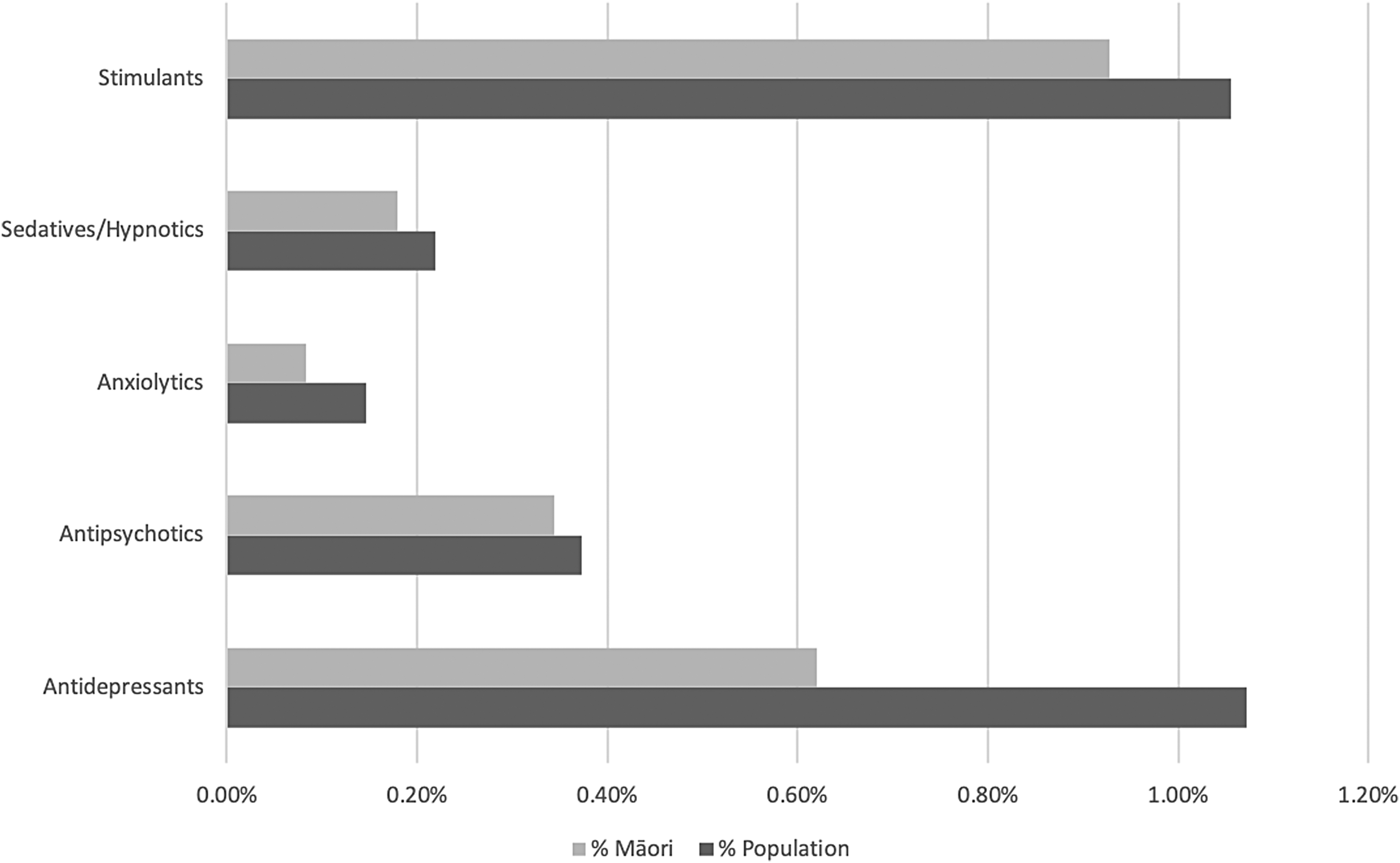
Percentage of the total population and of the Māori population prescribed each drug medication in 2016.
Age
Figure 5 shows the distribution of prescription rates across each age band in 2016. For every classification of medication there was at least one individual prescribed the medication for every age from 0 to 17 years old, with the exception of just two: stimulant prescriptions for ages 0- and 1-year olds. For antidepressants, antipsychotics, anxiolytics, and sedatives/hypnotics, the number of prescriptions increased with age. The exception to this trend was stimulant prescription, peaking at ages 8–10 years, and then declining slightly to age 17.

Percentage of New Zealand children and adolescents prescribed each medication class in 2016, by age in years.
Discussion
Rates and trends
The overall rates of prescription of psychotropic medications for children and adolescents in New Zealand sit near the middle of those reported worldwide. Antidepressant prescription rates at 1.07% are lower than the United States, which have been estimated between 1.6% and 3.9% (Medco 2011; Bachmann et al. 2016). The New Zealand rates are similar to Australia, Denmark, the United Kingdom, and Korea estimated at 0.9%, 1.0%, 1.1%, and 1.1%, respectively, and higher than reported in Germany (0.5%) and the Netherlands (0.6%) (Bachmann et al. 2016; Chon et al. 2017; Sawyer et al. 2017). The antipsychotic prescription prevalence rate of 0.37% was also in the mid range compared to the United Kingdom, Germany, Denmark, United States, and the Netherlands, with rates of 0.14%, 0.32%, 0.48%, 0.79%, and 1.03%, respectively, reported in 2012 (Kalverdijk et al. 2017).
The prescription rate of stimulants of 1.06% for New Zealand youth in 2016 is in the lower range of reported rates worldwide, with prescription rates ranging from 0.7% and 0.9% in Western Europe, Asia, and Australia to 4.5% in North America (Raman et al. 2018). The limited data on the rates of prescription of anxiolytics, sedatives, and hypnotics to children and adolescents in other countries make it difficult to compare New Zealand with them.
Psychotropic medication prescription rates for New Zealand youth are increasing, which is consistent with international trends. Antidepressant increases are similar to those seen in other countries such as Australia and the United Kingdom (Karanges et al. 2014; Bachmann et al. 2016), as well as previously reported New Zealand increases (Exeter et al. 2009; Karanges et al. 2014; Bachmann et al. 2016). An increase in antipsychotic medication has similarly been reported for Australian youth and increases also been noted in the United States, United Kingdom, and Europe (Karanges et al. 2014; Kalverdijk et al. 2017). The stable rate of anxiolytic and sedative and hypnotic prescription rates found across the 9 years for New Zealand youth reflects the stable prescription trends for these medications reported in other countries such as the United Kingdom, Australia, Denmark, and Iceland (Stephenson et al. 2013; John et al. 2015; Steinhausen 2015). Stimulant medication prescription increases are above the pooled worldwide average, but sit in the middle of the range of increases (Raman et al. 2018).
Gender, age, and ethnicity
The rates of overall prescription were split roughly equally between males and females, although rates were slightly higher for males. This is similar to the U.S. gender rates (Medco 2011). Stimulants were more likely to be prescribed to males at a ratio of 3.79 to 1, a rate similar to that seen in other countries worldwide (Raman et al. 2018). This gender difference for stimulant prescription is in line with the gender differences reported for ADHD prevalence in the 2015/16 New Zealand Health Survey (Ministry of Health 2016). More females were prescribed antidepressants, almost double the rate for males. This difference between genders is larger than that reported in Australia (Sawyer et al. 2017). Anxiolytics and sedatives/hypnotics were prescribed to females slightly more than males, similar to gender differences seen in U.S. adults (Moore and Mattison 2017).
Antidepressants, antipsychotics, anxiolytics, and sedatives/hypnotics prescriptions all increased with age, as has been seen in Australia (Sawyer et al. 2017). Similar to Australia, the trend for stimulant prescription was slightly different, with a peak around middle childhood, declining slightly into adolescence (Sawyer et al. 2017). The finding that antipsychotic medications were dispensed to 36 children 4 years of age and under was perhaps somewhat surprising. On further analysis, 55% of these children were 4 years of age, 75% were male, and 85.5% of dispensed medications were risperidone suggesting that the antipsychotic was likely being used for children with an autism spectrum disorder or other neurodevelopmental conditions associated with severe irritability.
Our data showed that Māori were prescribed lower rates of antidepressants and anxiolytics than Europeans, but rates were similar across ethnicity for antipsychotics and stimulants. No comparable data for other countries were found in the literature.
In New Zealand adolescents and young adults under 25 years of age, rates of mental disorders are higher for those of sole Māori identity and those of Māori/other identity than non-Māori, the higher rate remaining for Māori/other even when other socioeconomic factors were controlled for (Marie et al. 2008). Given this information, future research could focus on why Māori are receiving medications at lower rates, and whether or how this disparity needs to be addressed. Wilkinson and Mulder (2018a) reported that Māori received around half the antidepressant prescriptions as European/other, although antipsychotic rates were comparable (Wilkinson and Mulder 2018b). It is possible that the apparent lower rate of prescriptions for Māori is due to scripts not being filled for financial reasons (Jatrana et al. 2011).
New Zealand mental health prevalence rates
According to the 2015/2016 New Zealand Health Survey (Ministry of Health 2016), around 4.3% of youth aged 2–14 years had been diagnosed with “emotional and/or behavioural problems,” which referred to depression, anxiety, or ADHD. The 2015/2016 findings were a considerable increase from a 1.8% prevalence rate in the 2006/2007 survey. Emotional and/or behavioral problems increased with age; in 2015/2016 rates were 0.6% for the 2–4 years age group and 7.0% for the 10–14 years age group. Anxiety disorder had the highest rates in 2015/2016, at 2.7% of youth, followed by ADHD at 1.8% and depression at 0.3%. ADHD had a gender difference; the male rate was 2.7%, whereas females were 0.8%. These rates were not based on official diagnosis records, but on the parent advising they had been told by a doctor that their child had the condition at some time in their child's life. The reported prevalence rate of 1.8% for ADHD may be conservative, as studies have reported a wide range of prevalence rates (Ministry of Health 2001). For example, a rate of 6.7% was reported for children in the Dunedin Health and Development Study (Ministry of Health 2001). Worldwide prevalence estimates for ADHD are around 5%–7% (Raman et al. 2018).
Strengths and limitations
The major strength is that the data sets contained information on every individual prescription dispensed in New Zealand for the specified medications, that is, this was not a sample but a census of all medications dispensed between 2008 and 2016. This means that there is no sampling bias in the data.
The major limitation of the current study is that the data relate solely to the dispensing of medication, so we were unable to determine the indication(s) for treatment. In addition, the data collected by PHARMAC is for prescriptions that have been dispensed; we do not have data on individuals who may have been prescribed a medication but have chosen not to fill the prescription or those who were dispensed a medication but did not take it. In addition, polypharmacy is likely but was not able to be investigated as the data format did not allow for this type of analysis. Finally, it was sometimes difficult to compare rates of prescription across different countries due to differences in the time period evaluated.
Implications
Overall, New Zealand prescription rates of psychotropic medications to children and adolescents are similar to other Western countries, particularly Australia, and generally they appear to be within the average range. The use of some medications, such as fluoxetine if it is prescribed for depression or obsessive compulsive disorder (OCD) and stimulant medications for ADHD, is in accordance with guidelines from the NZFC and other practice parameters and guidelines, but these are not the only medications being prescribed. It is possible that some medications are being used off-label, but our data do not allow us to explore the conditions the medications are being used to treat.
The trend seen in New Zealand is for an increase in psychotropic medication use over time, again similar to other countries. It appears to be an ongoing trend, as previous New Zealand based literature as far back as 1997 showed an increase (Ministry of Health 2007). The question of whether this global increase is justified has been debated. Some have suggested we may be undertreating youth mental health (Taylor 2013), so the increase could be seen as positive and perhaps necessary, particularly when viewed in conjunction with the available data on prevalence rates of mental health problems in New Zealand. In contrast, there has been discussion that we are over diagnosing mental disorders and over prescribing medication, particularly in Western countries, with the suggestion that we are “medicalizing unhappiness” (Dowrick and Frances 2013).
It could be argued that in New Zealand prescribers may be overly conservative in some regards although the rates of dispensing of medications were reasonably close to those of Australia, which is the country most similar culturally. Publicly funded specialist mental health services in both countries are largely composed of multidisciplinary teams, which have a strong emphasis on the provision of broad evidence-based treatments, rather than narrow medication approaches, where indicated. However, New Zealand sits at the lower end of the range of stimulant prescription rates worldwide. Given that the prevalence rates of ADHD in the population are estimated at 5%–7% worldwide (Raman et al. 2018), the low prescription rates for stimulants at 1.1% of youth in New Zealand suggest that under-prescribing may be occurring. It is unclear what factors may be impacting on New Zealand's low rate of prescription for ADHD medications. A number of factors are likely to be contributing to this, including the awareness of and acceptability of ADHD medications for children and their families, lack of identification of possible ADHD by referrers, barriers to access services, the philosophy of care among New Zealand treatment services, and the availability of other supports and other treatments (Raman et al. 2018). Further research into this area would be useful. In New Zealand, stimulant prescriptions must be initiated by a child psychiatrist or pediatrician, and a lack of ready access to prescribers may be serving as a bottle neck for the adequate treatment of children and young people with ADHD. Raman et al. (2018) suggest that patients may be being undertreated in countries that have the lowest rates of stimulant prescribing. These rates are similar to the New Zealand rate. However, given the lack of evidence for positive long-term efficacy and safety of ADHD medications (Cortese et al. 2018), it could equally be argued that New Zealand prescribers are justified in more conservative prescribing rates.
There are a number of issues that are relevant to the relatively low prescribing rate of fluoxetine (47.5%). While fluoxetine is the only medication indicated for depression in children and adolescents in New Zealand, it is noted that escitalopram has been approved by the FDA for use in adolescents 12 years and older with depression (Yan 2009). It is likely that there is modest prescription of other SSRIs for young people with persistent severe depression who do not respond to an adequate trial of psychotherapy and fluoxetine. This would generally occur after consultation with a child and adolescent psychiatrist (Best Practice Advocacy Centre 2016). In addition, it is likely that many prescriptions for SSRIs are for young people with primary anxiety disorders or OCD. In relation to anxiety disorders, the AACAP practice parameter recommends that SSRIs should be considered when anxiety disorder symptoms are moderate to severe, where impairment makes participation in psychotherapy difficult, or where there has been a partial response to psychotherapy (American Academy of Child and Adolescent Psychiatry 2019). In addition, the practice parameter states that there is no empirical evidence that a particular SSRI is more effective than another for treatment of childhood anxiety disorders. There is similar guidance in relation to SSRI treatment of OCD (American Academy of Child and Adolescent Psychiatry 2019).
The increasing prescription rates of hypnotics are of significant concern as there are very few recognized indications for hypnotics in this population. One possible exception to this could be the use of benzodiazepines as an adjunctive treatment for young people with schizophrenia spectrum disorders who may derive benefit for associated anxiety, insomnia, or akathisia (American Academy of Child and Adolescent Psychiatry 2019). It is not known how many prescribers may be primary health care physicians or child and adolescent psychiatrists, but a stronger focus on education for prescribers is warranted. Similar increases in the use of benzodiazepines have been described elsewhere (Sidorchuk et al. 2018).
Conclusion
In conclusion, the current study has established the prevalence rates for the prescription of psychotropic medication to youth in New Zealand 2008–2016. These rates sit in the average range worldwide and are similar to other western countries, with the exception of stimulants, which are in the lower range. The trend for all psychotropic medication prescription rates is one of increase, which is consistent with international trends. This increase is particularly observed for antidepressant and antipsychotic medications.
Clinical Significance
The prevalence of mental health problems in New Zealand is increasing; the New Zealand Health Survey reported an increase of emotional and/or behavioral problems for 2–14-year olds from 1.8% in 2006/2007 to 4.3% in 2015/2016 (Ministry of Health 2016). The increase of prescriptions may therefore seem reasonable. However, as recently discussed by Mulder et al. (2017), there is no evidence that increased prescribing has been associated with a decrease in the burden of mental illness. If anything it has been associated with an increase. More research on long-term outcomes of prescribing could direct whether this increase is improving outcomes for children and adolescents with mental illness.
Disclosures
No competing financial interests exist.