
Abstract
Objective:
This article presents 1-year follow-up of a randomized placebo-controlled trial with open-label extension evaluating the efficacy of a broad-spectrum micronutrient (vitamins and minerals) intervention. The object was to determine if dominant treatment at follow-up was associated with differential psychological outcomes.
Methods:
Ninety percent of the original sample of 93 children with attention-deficit/hyperactivity disorder (ADHD) were followed 52 weeks postbaseline. Assessments included measures of ADHD, mood, anxiety, and general function based on parent/clinician report. Outcome was considered based on dominant therapy at 52 weeks (trial micronutrients [n = 19], medications [n = 21], and no treatment [n = 35]). Nine children were not categorized due to inconsistent therapies.
Results:
Based on dominant treatment, more of those who stayed on trial micronutrients (84%) were identified as “Much” or “Very Much” improved overall relative to baseline functioning, compared to 50% of those who switched to psychiatric medications and only 21% of those who discontinued treatment [χ2(2) = 19.476, p < 0.001]. Fifteen (79%) of those still taking micronutrients, 8 (42%) of those using medications, and 7 (23%) of those who discontinued treatment were considered remitters based on parent-reported ADHD [χ2(2) = 15.3, p < 0.001]. Those who stayed on micronutrients were more likely to have failed medication treatment in the past. The micronutrient group also displayed better outcomes on measures of parent-rated hyperactivity and anxiety, and clinician-rated general function and mood, with moderate to large between-group effect sizes (micronutrients vs. medication: ES = 0.73–1.01; micronutrients vs. no treatment: ES = 0.54–1.01). Most common reasons for stopping trial micronutrients were cost and number of pills to swallow. No continued side effects were associated with micronutrients.
Conclusions:
Children who benefitted from micronutrients in the short term maintained changes at follow-up, without side effects. While both those who continued micronutrients and those who switched to medication showed improved ADHD symptoms, psychiatric medication use was associated with deterioration in mood and anxiety. Inherent selection bias limits generalizability.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a chronic neurodevelopmental condition involving difficulties with attention, hyperactivity, and impulsivity (American Psychiatric Association 2013). Executive function impairments, particularly relating to self-regulation, are thought to contribute to these symptoms as well as other impairments such as social difficulties and problems with mood regulation (Barkley 1997; Willcutt et al. 2005). ADHD is common, affecting 7.2% (or more) of school-age children worldwide, and significantly impacts not only the child diagnosed but also their wider social networks, that is, family, peers, school teachers, and classmates (Thomas et al. 2015). These challenges often persist into adolescence and adulthood, even when ADHD is treated (Biederman et al. 2006; Hechtman et al. 2016).
Pharmacological treatment with stimulant or amphetamine-based medications (e.g., methylphenidate and dexamphetamine) is effective for many children with ADHD, rapidly producing improved attention and concentration (Biederman et al. 2004). However, long-term studies of medication for ADHD find that medications do not result in elimination of symptoms or improved academic performance (Advokat 2010; Currie et al. 2014; Storebø et al. 2015). Sixteen-year outcomes of the Multimodal Treatment Study of Children with ADHD (MTA trial) found medication use was not associated with reduced symptom severity compared with those who had never been medicated, and was also associated with reduced adult height (Swanson et al. 2017). Other authors have suggested that through a process of “neuronal imprinting,” early stimulant treatment of ADHD, while masking symptoms in the short term, may possibly worsen underlying symptoms in the long term (Stern et al. 2017).
Some children with ADHD (20%–30%) either do not respond well to medications or cannot tolerate side effects, which commonly include appetite suppression and sleep disturbance. As such, some families prefer to try other options for their child with ADHD (Thomas et al. 2013; Scholle et al. 2018). Common alternatives include behavioral interventions, supplementation with essential fatty acids, and dietary manipulations. Behavioral interventions are often recommended as a treatment for ADHD; however, it appears that they mainly benefit secondary impairments rather than core ADHD symptoms (Sonuga-Barke et al. 2013; Daley et al. 2014). Essential fatty acid supplementation and artificial food color exclusions show consistently small, but significant effects, reducing ADHD symptoms (Sonuga-Barke et al. 2013; Taylor et al. 2018).
Other approaches to treating ADHD consider the role of broader nutritional factors in the expression of psychiatric symptoms (Oddy et al. 2009; Howard et al. 2011). Optimal levels of nutrition may not be obtained through the diet for a range of reasons, including poor diet, reduced nutrient content in food, and underlying risk factors, resulting in higher nutrient requirements (Popper 2014). Research testing the use of single-nutrient supplementation to treat ADHD has generally showed mixed and inconsistent results; positive findings were fraught with methodological issues and a lack of replication (Cortese et al. 2012; Stevenson et al. 2014; Hariri and Azadbakht 2015). An increasing body of research has indicated that the use of a broad combination of vitamins and minerals (micronutrients) at appropriate doses may prove to have more positive effects than the single-nutrient approaches (Rucklidge and Kaplan 2014). Possible mechanisms of action by which broad-spectrum micronutrient supplementation may improve psychological symptoms involve improving metabolic function in the brain by ensuring an adequate supply of vitamins and minerals to be used as cofactors for a myriad of chemical reactions; improving mitochondrial function and ATP production; reducing inflammation in the gut; and providing sufficiently high levels of nutrients so that even if absorption is reduced, the brain and body may obtain necessary nutrients (Kaplan et al. 2015b).
One such broad-spectrum micronutrient approach has demonstrated some benefit in reducing ADHD and associated symptoms in adults and children, both during clinical trials and longer-term naturalistic follow-up (Rucklidge et al. 2014, 2017; Gordon et al. 2015). A recent double-blind, randomized placebo-controlled trial (RCT) demonstrated that over 10 weeks, although total ADHD symptoms did not improve more than placebo, micronutrient treatment resulted in improved emotion regulation, aggression, and general functioning in children with ADHD (Rucklidge et al. 2018). Inattention also improved more in the micronutrient group relative to placebo based on clinician-rated symptoms, but not parent-rated symptoms.
This research was a naturalistic follow-up study investigating the longer-term function of children with ADHD, who took part in the abovementioned RCT comparing a micronutrient formula with placebo, followed by a further 10 weeks of open-label (OL) treatment with micronutrients. We aimed to investigate whether participants' psychiatric and overall function were associated with their dominant mode of treatment from the end of the OL trial to 1 year postbaseline. Measures included standardized and validated clinician and parent/caregiver measures of attention, hyperactivity and impulsivity, mood, anxiety, emotional dysregulation, aggression, quality of life, and overall psychiatric functioning.
Methods
Both the National Upper South A Health and Disability Ethics Committee and the Human Ethics Committee at the University of Canterbury approved the RCT and follow-up evaluation. The trial was prospectively registered (Australian New Zealand Clinical Trials Registry: Universal Trial No. U1111-113918257).
Participants and entry criteria
The methods have been described in detail elsewhere (Rucklidge et al. 2018) and so will only briefly be described here. Ninety-three children with ADHD 7–12 years of age were recruited in Canterbury, New Zealand, from November 2013 to November 2016. Participants were recruited through public health services, private referrals, and print and online advertisements. Parents or caregivers provided informed consent and participants assented to participate in the follow-up using forms and procedures approved by the ethics committees. Participants were assigned in a 1:1 ratio to 10 weeks of treatment with either micronutrients or placebo (Fig. 1). After 10 weeks, all participants were offered the micronutrient OL for an additional 10 weeks.
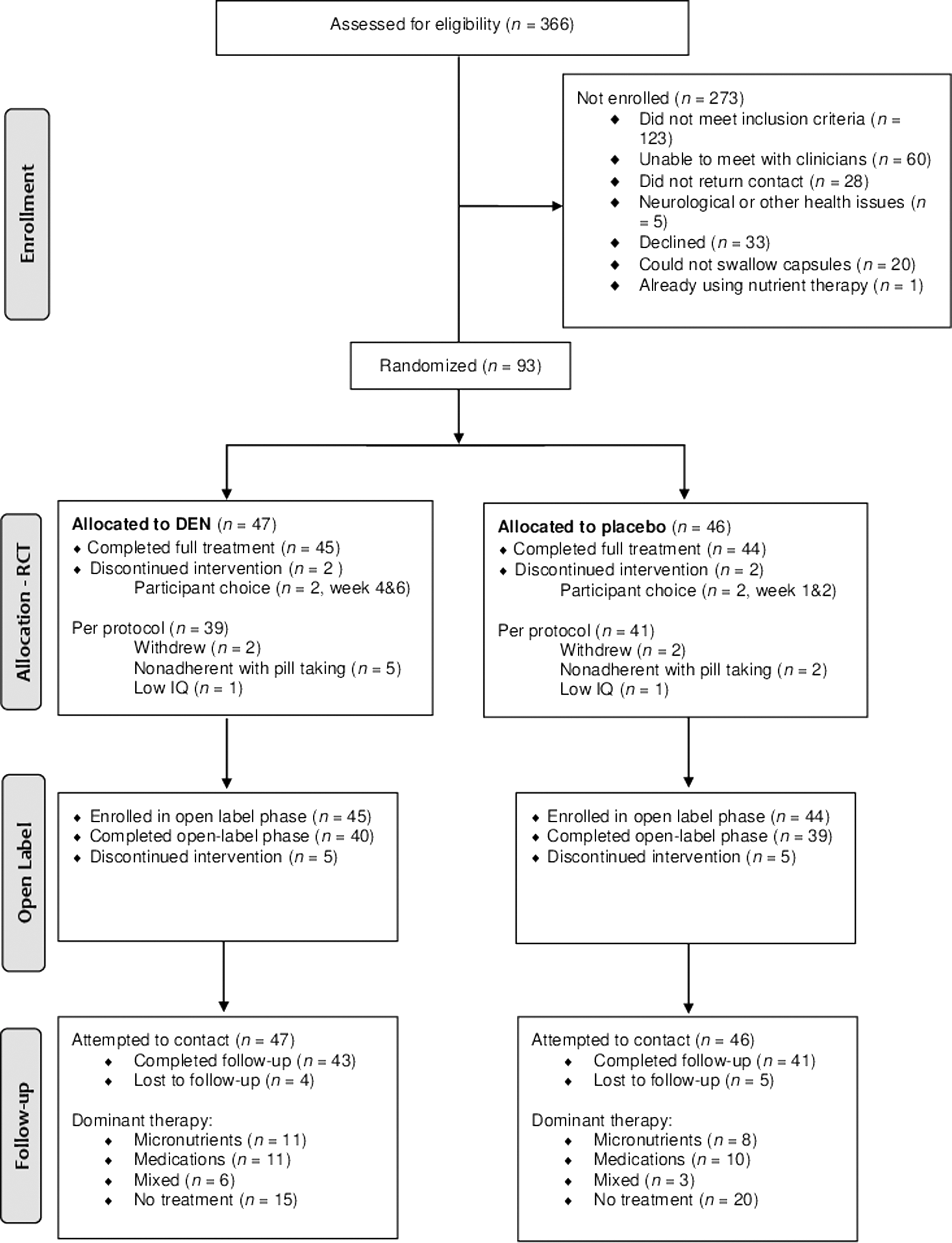
CONSORT flow diagram. DEN, daily essential nutrients.
Participants' ADHD status was established using the Kiddie-Schedule for Affective Disorders and Schizophrenia interview (K-SADS-PL) (Kaufman et al. 1997) and elevations on the Conners' Parent and Teacher Rating Scales (Conners et al. 1998a, 1998b). The K-SADS-PL was also used to assess for comorbid psychiatric diagnoses. Only individuals not taking psychiatric medication for at least 4 weeks were eligible to take part in the study. Participants were excluded if they had any of the following: neurological disorder involving brain or other central function; major psychiatric condition requiring hospitalization; serious medical condition; known allergies to ingredients of the intervention; known abnormality of mineral metabolism; IQ below 75; and autism spectrum disorder. Once baseline assessment was completed, participants were allocated to receive either micronutrient or placebo capsules. See Table 1 for capsule ingredients. Participants started taking 3 capsules per day and increased their dose over a week up to 12 capsules per day, in 3 doses of 4 capsules, taken with food and water.
Ingredients of Capsules
Proprietary blend: Choline bitartrate, alpha-lipoic acid, inositol, acetyl-
Psychiatric assessment
Participants were monitored through in-person meetings, or by telephone where necessary, at screening, baseline, and weeks 2, 4, 6, 8, 10 (end of RCT), 12, 14, 16, 18, 20 (end of OL), and 52 (follow-up). At baseline (with the exception of the CGI-I, which measures change from baseline), and 10, 20, and 52 weeks, clinicians and parents/caregivers completed the following measures of participants' functioning.
Clinician rated
Clinical Global Impressions—Improvement (CGI-I) scale, rating change from baseline in aspects relating to ADHD, Mood, Anxiety, and Overall presentation (Guy 1976). Items are rated on a Likert-style scale from 1 (very much improved) to 7 (very much worse). Clinicians synthesized information from parents/caregivers, completed questionnaires, other sources (e.g., teachers), and observed behavior in the clinic.
The Children's Global Assessment Scale (C-GAS) was used by clinicians to rate participants' overall level of functioning based on all information gathered since the previous assessment. It is a single numerical rating, ranging from 1 to 100 with higher scores indicating better function (Shaffer et al. 1983).
The ADHD Rating Scale IV (ADHD-RS-IV)—Clinician Version was completed by clinicians to rate ADHD symptoms corresponding to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR) diagnostic criteria. Scores can range from 0 to 54, with higher scores indicating the presence of more ADHD symptoms (Faries et al. 2001).
The Child Depression Rating Scale (CDRS) was used to assess depression in children and monitor changes in mood throughout the trial. Based on information from parents/caregivers and participants, as well as observations during assessments, clinicians rated participants' mood. Scores could range from 15 to 61, with higher scores indicating more impaired mood (Poznanski et al. 1979).
Parent rated
Conners' Parent Rating Scale—Revised: Long Version (CPRS-R:L). The CPRS-R:L is a commonly used tool, both clinically and in research, which has parents/caregivers rate their child's behavior over the previous month. Items are rated from 0 (“Not true at all”) to 3 (“Very much true”). The CPRS-R:L includes subscales for DSM-IV-TR inattention, hyperactivity/impulsivity, and total ADHD symptoms. Age- and gender-relevant norms are used to transform raw scores into T-scores; T-scores of 65 and above are considered to fall in the clinical range. Higher scores indicate greater impairment (Conners 1997).
The Strengths and Difficulties Questionnaire (SDQ). Individual items describing the presence (e.g., “Constantly fidgeting or squirming”) or absence (e.g., “Thinks things out before acting”) of symptoms across a number of areas are rated by parents/caregivers as “Not True,” “Somewhat True,” or “Certainly True.” The SDQ is scored to produce ratings of emotional symptoms, conduct problems, hyperactivity and inattention, peer problems, prosocial skills, and a total difficulties score. Possible scores for subscales range from 0 to 10; the total difficulties score can range from 0 to 40. Higher scores indicate more impairment, except for the prosocial skills scale in which higher scores indicate better function. Impact of symptoms is rated in terms of distress, and impact on home life, friendships, classroom learning, and leisure activities. Impact in each domain is rated from 0 (“Not at all”) to 2 (“A great deal”), and the total impact score can range from 0 to 10. A total impact score of 2 or more is considered abnormal (Goodman 2001).
The Child Mania Rating Scale, Parent Version (CMRS). Although this scale is based on the DSM-IV-TR criteria for mania, it provides a measure of emotion dysregulation, which is a common feature in ADHD (van Stralen 2016). Items are rated from 0 (“Never/Rarely”) to 3 (“Very Often”). Examples of items include the following: “Feel irritable, cranky, or mad for hours or days at a time” or “Experience rapid mood swings.” The total score can range from 0 to 63, with a score of 20 used as a clinical cutoff to identify children at risk of severe emotional dysregulation. Higher scores indicate greater emotional dysregulation (Pavuluri et al. 2006).
Screen for Child Anxiety Related Emotional Disorders-Revised (SCARED-R), a 41-item questionnaire designed for parents/caregivers and children to rate the presence of various anxiety-related symptoms in different situations (Muris et al. 1998). Questions are rated on a 3-point Likert-type scale from 0 = “Not True or Hardly Ever True,” 1 = “Somewhat True or Sometimes True,” or 2 = “Very True or Often True.” Higher scores indicate greater number and severity of anxiety symptoms. The maximum possible score is 82; 25 is the clinical cutoff indicative of a possible anxiety disorder (Birmaher et al. 1999).
Other measures
The Eating Behaviors Questionnaire, modified from Baker et al. (2003). Parents/caregivers rated their child's intake of fruit and vegetables and perceived overall diet healthiness, as well as how often they eat healthy amounts of food, desserts or sweets, fast food, and breakfast. Scores can range from 7 to 37, with higher scores indicating a healthier eating pattern.
Acceptability of Treatment: at the 52-week follow-up, parents/caregivers and participants who had not continued taking micronutrients were asked to complete a questionnaire ascertaining reasons for discontinuation. They rated on a 7-point Likert scale (1 = not at all to 7 = very much) how much their decision was influenced by the following: side effects; no symptom benefit; too many pills to take; could not consistently take the pills, remember them; the cost (too high, could not afford); found another treatment that was better (medication, other supplements, and therapy); people close to me do not approve of this treatment; wanted to see if I could manage the symptoms without taking anything; and feeling good, I did not think I needed them anymore. This list of possible reasons for discontinuation was produced based on qualitative information obtained in previous micronutrient research.
Procedures
Approximately 12 months postbaseline, all participating families were contacted for follow-up, regardless of whether they had completed the randomized or OL phases. Where possible, clinicians arranged to meet with participants and their parent or caregiver for assessment; otherwise, measures were completed over the phone or online.
Statistical analyses
Paired samples t-tests (two tailed) were used to compare the changes from baseline to 52-week follow-up and the end of OL treatment to 52-week follow-up. Once all follow-up assessments were completed, the sample was categorized into four groups according to the dominant treatment used since completing the trial: continued use of trial micronutrients, switched to medication, no treatment, or mixed (e.g., both stimulants and some form of vitamin-mineral supplement or inconsistent use of one treatment). Changes from 20 to 52 weeks were compared using analysis of covariance (ANCOVA) with 20-week scores as covariate and summarizing treatment effects as mean differences and 95% confidence intervals. Cohen's d was used to compare effect size between groups, and p-values <0.05 were considered statistically significant. Where results identified significant group differences, pairwise comparisons using Fisher's least significant difference tests were examined. Chi-square tests were used to compare categorical outcomes.
Results
Those followed versus lost to follow-up
Of the 93 children who began the trial, 84 (90%) completed follow-up ∼1 year after their baseline assessments (M = 13.6 months; mode = 12 months; range = 9–37 months). Figure 1 depicts the flow of participants throughout each phase of the randomized controlled trial, OL trial, and naturalistic follow-up. Table 2 lists the baseline demographic and clinical features of those followed up versus those not followed up. Compared to those who were followed up, participants lost to follow-up (n = 9) were more likely to be diagnosed with Conduct Disorder at baseline [t(90) = −4.362, p = 0.000034]. There were no significant differences in any of the other demographic variables, including age, gender, estimated IQ, socioeconomic status, or ethnicity.
Baseline Demographic and Clinical Features of Randomized Controlled Trial Participants Followed (Divided Into Dominant Treatment) and Lost to Follow-Up
Lower scores indicate better functioning for all scales, except the C-GAS, on which higher scores are better.
Intelligence Quotient, assessed using Block Design and Vocabulary subtests of the WISC-IV (Wechsler 2004).
Based on the New Zealand Socio-Economic Index (Davis et al. 1997).
Higher scores indicate better functioning.
Defined as having at least 1 standard score of 85 or below on either reading or spelling of the WRAT3, or previous assessment confirming an LD (Wilkinson 1993).
ADHD, attention-deficit/hyperactivity disorder; CD, conduct disorder; C-GAS, Children's Global Assessment Scale; CGI-S-ADHD, severity of ADHD based on Clinical Global Impressions; CMRS, Child Mania Rating Scale; CPRS-R:L, Conner's Parent Rating Scale—Revised: Long Version; CTRS-R:L, Conner's Teacher Rating Scale-Revised: Long Version; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; H/I, hyperactivity/impulsivity; LD, learning disability; M, mean; n, number of participants; ODD, oppositional defiant disorder; RCT, randomized controlled trial; SD, standard deviation.
Psychiatric status at follow-up
For the overall sample of participants who were followed up, most variables remained similar at 52 weeks compared to the 20-week assessment. Clinician-rated total ADHD symptoms, clinician-rated depression symptoms (CDRS), and parent-rated mood dysregulation (CMRS) deteriorated during the follow-up period, with small to moderate effect sizes. All measures of psychological functioning remained significantly improved at 52 weeks compared to baseline (Table 3). Consistent with the CMRS and CDRS, CGI-S ratings of mood and anxiety indicated significantly more impairment at 52-week follow-up than at the end of OL trial.
Baseline and 20- and 52-Week Data on Outcome Measures for Those Who Completed 52-Week Follow-Up
Lower scores indicate better functioning for all scales, except the C-GAS, on which higher scores are better.
Higher scores indicate better functioning.
p < 0.05; ** p < 0.01; *** p < 0.001.
ADHD-RS-IV, ADHD Rating Scale IV; CDRS, Child Depression Rating Scale; C-GAS, Children's Global Assessment Scale; CI, 95% confidence interval; CMRS, Child Mania Rating Scale; CPRS, Conner's Parent Rating Scale; DSM, Diagnostic and Statistical Manual; SCARED, Screen for Child Anxiety Related Emotional Disorders; SD, standard deviation.
Information on eating behavior was obtained from 71 participants. Based on parent/caregiver responses, the dietary patterns of the participants deteriorated slightly between the end of the OL trial and 52-week follow-up assessment (from a mean of 31.37 to 30.39). Although small, this difference was statistically significant [t(61) = −2.626, p = 0.011, d = 0.33]. ANCOVA did not reveal any significant differences between follow-up groups [F(2) = 1.025, p = 0.365] in dietary patterns at 52 weeks, using 20-week scores as covariates.
Dominant therapy from end of OL to follow-up
To investigate whether dominant treatment at follow-up influenced outcomes, participants and their caregivers were asked during the follow-up assessment how they had managed ADHD symptoms since completing the OL trial. They were then classified based on the dominant therapy used during this time as follows: (A) consistently taking trial micronutrients without psychiatric medications (n = 19); (B) consistently taking psychiatric medications without trial micronutrients (n = 21); (C) no intervention (n = 35); or (D) mixed (n = 9). There were no between-group differences in the demographic variables, age: F(4, 88) = 0.845, p = 0.500; IQ: F(4, 87) = 0.755, p = 0.558; NZSEI: F(4, 88) = 0.548, p = 0.701; gender: χ2(3) = 0.813; or ethnicity: χ2(3) = 0.594, indicating that child's age, gender, IQ, or ethnicity, or family socio-economic status (SES), were not associated with choice of therapy after the end of the trial. However, those who chose to stay on the micronutrients were twice as likely to have tried medications in the past compared with the other groups and been tried on significantly more medications [F (2, 75) = 4.968, p = 0.01], suggesting medications were not conferring adequate relief of symptoms or that side effects were not tolerated (Table 2).
Nineteen participants (23% of the follow-up sample) continued to take the trial micronutrients consistently. The dose used ranged from 8 to 15 capsules per day (mean [M] = 12; standard deviation [SD] = 2.6). Other medications included antihistamines (n = 3), laxatives (n = 1), and Ventolin (n = 1). Seven were also using other dietary supplements, including melatonin (n = 1), fish oils (n = 5), and probiotics (n = 2).
Twenty-one participants (25%) had switched from micronutrients to psychiatric medication after the trial was over. Medications used included a range of ADHD medications (various methylphenidate preparations, n = 19; and atomoxetine, n = 1), and one participant was taking a selective serotonin reuptake inhibitor (fluoxetine). In addition, one participant used antihistamines and three used melatonin. One participant also took an omega 3 supplement and probiotics.
Thirty-five participants (42%) were not using trial micronutrients or psychiatric medication. Two participants had briefly tried and discontinued psychiatric medication. Four used melatonin for sleep.
The mixed group consisted of nine participants (11%) who took trial micronutrients inconsistently, and/or also used them in combination with medications. Five of these participants also took other nutrients such as niacin, magnesium, fish oil, probiotics, and melatonin.
Twelve of the 84 children followed up (14%) had some form of psychological therapy or counseling and 15 (17%) had received respite care (n = 5), educational (e.g., speech and language therapy; n = 7), or other (e.g., occupational therapy; n = 7) intervention during the follow-up phase. Use of psychotherapy was comparable across the different groups.
Given that this study aimed to understand whether the dominant treatment from the end of the OL trial to follow-up was associated with differential outcomes at follow-up, the mixed group (D) was excluded from further analysis.
Compared to those who discontinued treatment or switched to medications, participants who continued taking micronutrients during the follow-up period had significantly lower scores at 20 weeks (i.e., end of OL) on all ADHD measures, both parent and clinician rated, as well as the total difficulties score, conduct problems subscale, hyperactivity and inattention subscale, and impact score of the parent-rated SDQ. The participants who continued taking micronutrients during the follow-up period also had significantly better 20-week scores for emotion dysregulation as rated by parents using the CMRS, and were rated by clinicians as functioning better overall on the C-GAS. Compared to baseline, those who continued to take trial micronutrients, those who switched to medication, and those who discontinued treatment all showed improved depression and anxiety based on the clinician-rated CDRS and parent-rated SCARED-R, and there were no significant differences between groups on these measures at 20 weeks. Overall, the 20-week data indicate that those who stayed on micronutrients at follow-up were more likely to have experienced a positive response during the OL phase relative to those who stopped or switched to medications (Table 4).
Comparison of Change From 20 to 52 Weeks on Outcome Measures Based on Dominant Treatment During Follow-Up Period
Lower scores indicate better functioning for all scales, except the C-GAS and the Prosocial subscale of the SDQ, on which higher scores are better.
A, stayed on trial micronutrients; B, switched to medications; C, no treatment. Effect sizes calculated based on mean changes.
Unadjusted means.
ANCOVA comparing changes from 20 to 52 weeks across the three groups.
Effect size as Cohen's d: mean difference between the estimated marginal means/√mean squared error corrected for unequal group sizes.
Higher scores indicate better functioning.
p < 0.05; ** p < 0.01.
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS-IV, ADHD Rating Scale IV; ANCOVA, analysis of covariance; CDRS, Child Depression Rating Scale; C-GAS, Children's Global Assessment Scale; CMRS, Child Mania Rating Scale; CPRS, Conner's Parent Rating Scale; DSM-IV, Diagnostic and Statistical Manual, Fourth Edition; ES, effect size; SCARED, Screen for Child Anxiety Related Disorders; SD, standard deviation; SDQ, Strengths and Difficulties Questionnaire.
Table 4 displays comparisons between dominant treatment groups for change in clinician- and parent-rated measures from 20 to 52 weeks. These comparisons revealed significant group differences in changes in psychiatric functioning from the end of OL trial to 52-week follow-up for most variables. Post hoc analyses indicated that those who continued to take micronutrients at 52 weeks and those who had switched to medication had significantly lower clinician-rated inattention, hyperactivity/impulsivity, and total ADHD symptoms than those who had discontinued treatment, with large effect sizes (d = 0.88 to d = 1.16 for micronutrients vs. no treatment and d = 0.64 to d = 0.81 for medication vs. no treatment). Effect sizes for the comparison between the micronutrient and the medication groups were negligible to small (d = 0.09 to d = 0.37), indicating that both of these treatments were controlling ADHD symptoms more effectively than no treatment.
Parent-rated ADHD symptoms (CPRS-R:L DSM-IV-TR Inattention, Hyperactivity/Impulsivity, and Total ADHD symptoms) overall favored the micronutrient group. At 52 weeks, there was no significant difference between groups in the amount of change on CPRS-R:L DSM-IV-TR Inattention: group differences observed at 20 weeks were maintained. Although not significant, effect sizes were small to moderate: d = 0.44 for micronutrients versus medication, d = 0.20 for medication versus no treatment, and d = 0.65 for micronutrients versus no treatment. The micronutrient group had improved more on CPRS-R:L DSM-IV-TR Hyperactivity/Impulsivity than those who had switched to medication and those who had discontinued treatment, with moderate to large effect sizes (d = 0.73 and d = 0.93; d = 0.20 for medication vs. no treatment). The micronutrient group improved more on CPRS-R:L DSM-IV-TR Total ADHD symptoms than those who were untreated, but not compared to those who were medicated, again with moderate to large effect sizes (d = 0.90 for micronutrients vs. no treatment and d = 0.68 for micronutrients vs. medication; d = 0.21 for medication compared to no treatment).
Those still taking micronutrients during follow-up improved significantly more between 20 and 52 weeks on the Hyperactivity/Inattention subscale of the SDQ than those taking medications (d = 0.63) or using no treatment (d = 1.26). The other subscales of the SDQ did not show significant group differences in the amount of change from 20 to 52 weeks, although the Total Difficulties score displayed a nonsignificant trend (p = 0.067), again favoring those who stayed on micronutrients, with moderate effect sizes (d = 0.75 for micronutrients vs. medication and d = 0.68 for micronutrients vs. no treatment; d = 0.08 for medication vs. no treatment).
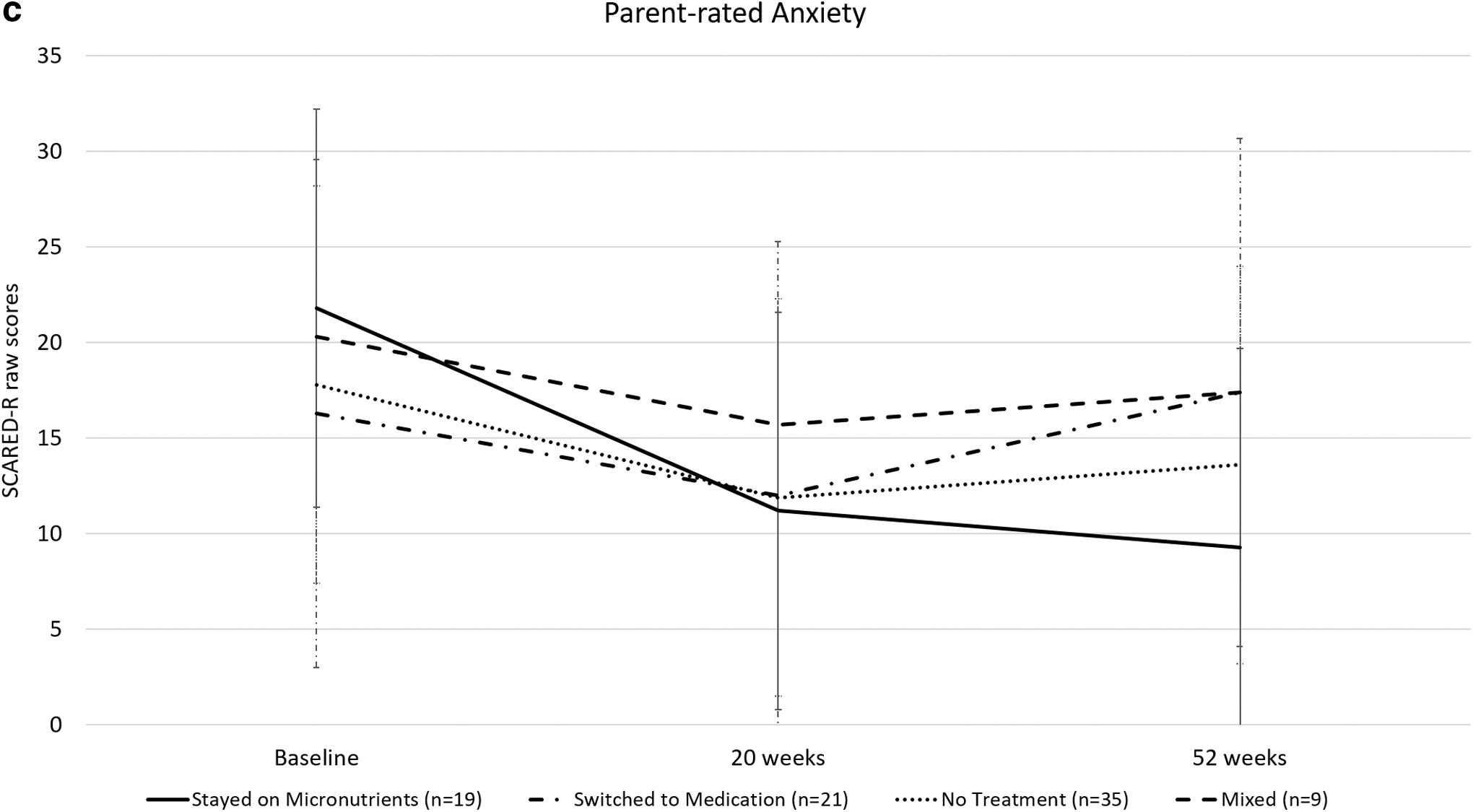
There were no significant differences between follow-up groups in the amount of change on parent-rated emotion dysregulation (CMRS): group differences at 20 weeks were maintained at 52 weeks. Parent-rated anxiety (SCARED-R) had improved significantly more for the group of participants still taking micronutrients at 52 weeks than those on medication (but not those who were untreated), with a large effect size: d = 1.01 for micronutrients versus medication (d = 0.54 for micronutrients vs. no treatment and d = 0.47 for medication vs. no treatment, with the medication group associated with more severe anxiety symptoms than the no-treatment group). This pattern suggests that switching to medication may have been associated with increased anxiety symptoms relative to no treatment, while continued micronutrient treatment was associated with decreased anxiety symptoms. Those still taking micronutrients at 52 weeks had improved more than those on medication or no treatment on ratings of depression (CDRS; d = 0.76 for micronutrients vs. medication and d = 0.63 for micronutrients vs. no treatment; d = 0.12 for medications vs. no treatment) and overall functioning (C-GAS; d = 0.78 for micronutrients vs. medication and d = 1.10 for micronutrients vs. no treatment; d = 0.31 for medication vs. no treatment). Figures 2 to 4 show the pattern of change over time for the three follow-up groups across these different areas of functioning.

C-GAS at baseline and 20 weeks and 52 weeks by dominant treatment at follow-up. C-GAS, Children's Global Assessment Scale.
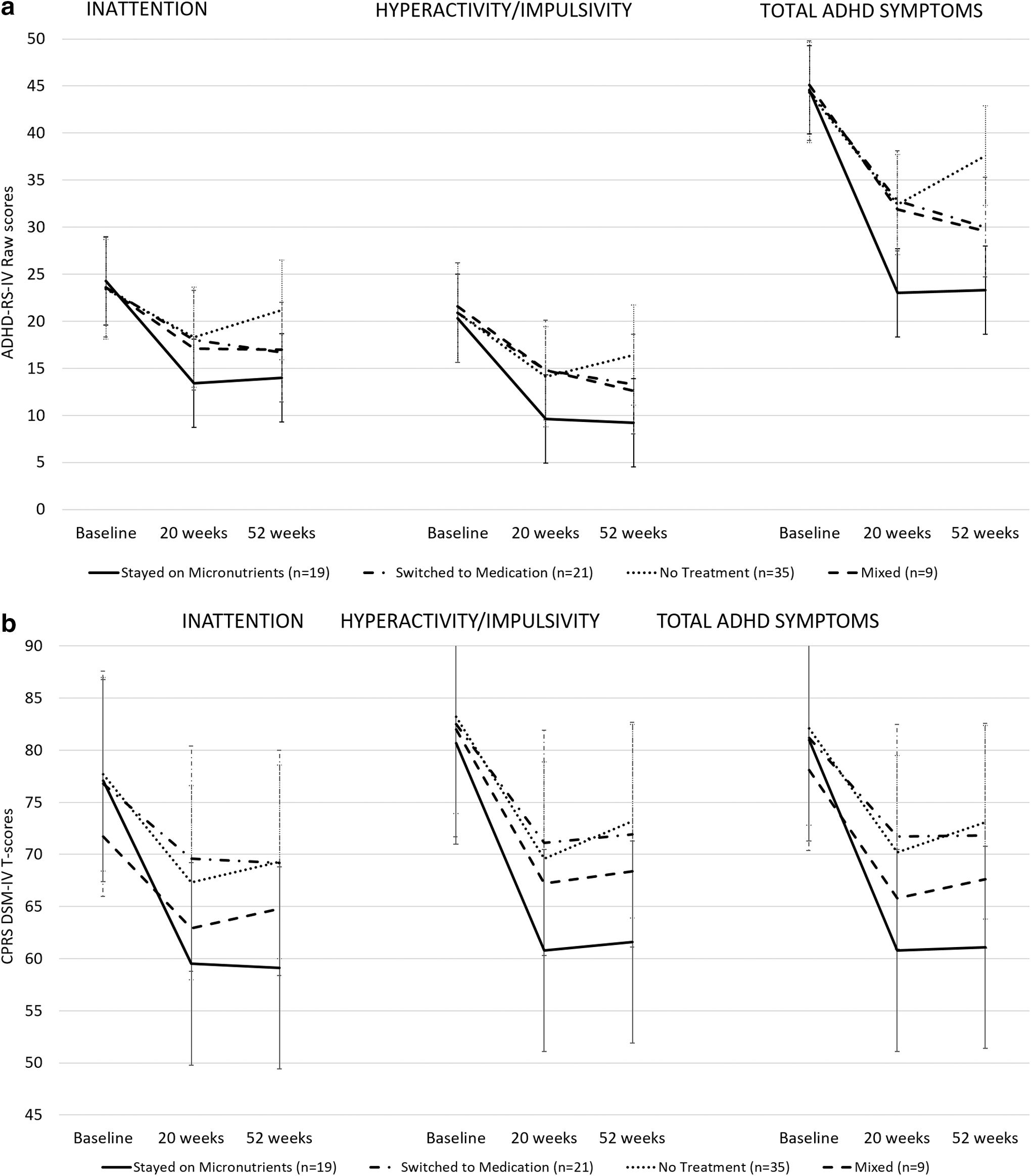
ADHD symptoms at baseline and 20 and 52 weeks by dominant treatment at follow-up.
Side effects
No participant still taking micronutrients at 52 weeks reported any adverse effects that were likely attributable to the micronutrient treatment. One participant with a history of reflux reported increased reflux on discontinuing his reflux medication, and one participant reported the emergence of insomnia. This was not deemed likely to be due to the micronutrient treatment as it emerged more than a year after the participant began to take micronutrients.
Treatment response based on dominant treatment from the end of OL phase to follow-up
At 20 weeks, 84% of those who continued to take micronutrients during the follow-up period were classed as responders (clinician ratings of much or very much improved compared to baseline) on CGI-I-Global, compared to 50% of those who switched to medication, and 60% of those who discontinued treatment. These differences did not reach significance [χ2(2) = 5.397, p = 0.067].
At 52 weeks, 84% of those who continued to use micronutrients were classed as responders, suggesting that those who continued this treatment maintained the gains made during the initial phase of treatment over the subsequent months. Once again, 50% of those who switched to medication were classed as responders at 52-week follow-up, despite this group choosing to change treatment approach. Only 21% of those who were using no treatment at the time of follow-up were considered responders, a decrease of almost two-thirds compared to the 20-week assessment. Chi-square analysis indicated significant group differences [χ2(2) = 19.476, p = 0.000059] and post hoc testing indicated that all pairwise comparisons were significantly different. A significantly larger percentage of those still taking micronutrients at follow-up were classed as responders than those who had switched to medication, and a significantly larger percentage of those taking medication at follow-up were classed as responders than those who were using no treatment (Fig. 5).

Other clinical outcomes at baseline and 20 and 52 weeks by dominant treatment at follow-up.
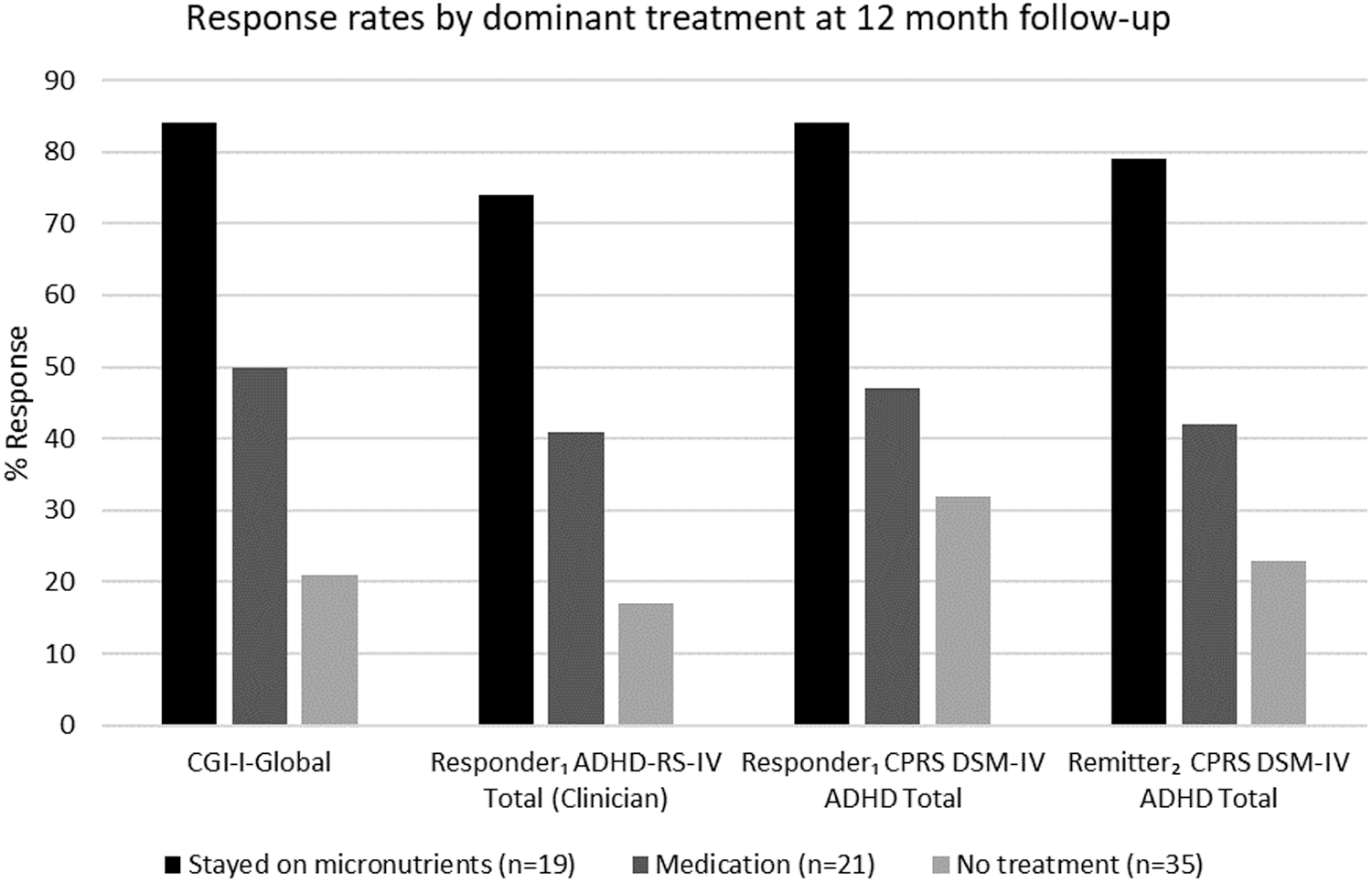
Response rates by dominant treatment at 12-month follow-up. Responder1 defined as a decrease in symptoms of 30% or more. Remitter2 defined as T-score <65.
Taking ≥30% improvement on the CPRS-R:L DSM-IV-TR ADHD Total as an indicator of clinically significant improvement from baseline, there was a significant group difference at follow-up, χ2(2) = 12.8, p = 0.002. Sixteen (84%) of those on trial micronutrients were classed as responders compared to 9 (47%) of those on medications and 10 (32%) of those who stopped treatment. We also identified those participants who at 52 weeks had a score within the nonclinical range on the CPRS-R:L DSM-IV-TR ADHD Total (i.e., T-score <65). Fifteen (79%) of those still taking micronutrients, 8 (42%) of those using medications, and 7 (23%) of those who discontinued treatment were considered remitters on this basis, χ2(2) = 15.3, p = 0.000488. Consistent with these findings, ratings of the Clinician ADHD-RS-IV ADHD Total showed that 74% of those on micronutrients were classed as responders at follow-up (≥30% improvement) compared to 41% of those on medications and 17% of those who stopped treatment, χ2(2) = 15.9, p = 0.000359. Post hoc testing revealed that the percentage of responders or remitters in the micronutrient group was significantly greater than the percentage in either the medication or no-treatment groups for all three comparisons (Fig. 5).
Reasons for choosing to discontinue the micronutrients
The cost and number of pills were identified as the greatest barriers to continuing with micronutrient treatment. These items had the highest means (number of pills: M = 3.75, SD = 2.5 and cost: M = 3.75, SD = 2.36), and were most frequently rated “Very much a reason for stopping.” Side effects were rarely (and disapproval of treatment never) noted as “Very much a reason” for discontinuation; these items also had the lowest means (M = 2.14, SD = 2.03 and M = 1.22, SD = 0.64, respectively).
Discussion
This article presents the first study to report naturalistic outcomes after an RCT followed by OL extension using micronutrients to treat ADHD in children. One year after baseline, the group of participants as a whole had either maintained improvements achieved by the end of the OL trial or regressed slightly. Similar to the MTA trial (MTA Cooperative Group 1999) in which all groups displayed improvements in ADHD symptoms at 3 years relative to baseline (Jensen et al. 2007), participants were still functioning better on all variables at 52-week follow-up compared to when they entered the trial. This improvement was likely a combination of the intervention and attention provided during the clinical trial, ongoing treatment obtained during the intervening months, naturalistic improvement, as well as regression to the mean, an observation consistently reported in other clinical trials (Jensen et al. 2007; Rucklidge et al. 2017).
Although the group as a whole improved from baseline to the end of OL trial, this study showed that the group of participants who chose to stay on the trial micronutrients at 52-week follow-up (20% of the original 93 children) represented those children who generally had better outcomes on most psychological measures at the end of the OL trial, relative to those who stopped the intervention or switched to medications. In other words, participants who continued to take micronutrients appear more likely to do so if they had obtained a good response after at least 10 weeks of micronutrient treatment. Interestingly, this group contained children who had tried more medications before enrolment in the study, and therefore, their good response rate cannot be explained by simply representing children who would have done well anyway. It is possible that children with ADHD who respond poorly to medication may respond well to micronutrients. These observations are remarkably similar to a follow-up trial conducted with adults with ADHD where 18% of the sample continued to take the micronutrients and they represented those individuals who as a group showed the best response to the intervention at the end of the OL phase (Rucklidge et al. 2017).
At the 52-week follow-up, 84% of those who continued taking micronutrients were considered responders (rated “Much” or “Very Much” improved on CGI-I-Global), compared to 50% of those on medications and 21% of those who discontinued treatment. At 20 weeks, the percentage of responders was the same as at follow-up for those who continued on micronutrients or switched to medication. However, for those who stopped all treatment, the response rate was much higher (60%) than it was at follow-up. This indicates that a substantial portion of those who responded to the micronutrients, but chose to stop them and did not replace them with another form of treatment, worsened after discontinuing the trial micronutrients. It is of note that on most ADHD ratings, those who continued to take micronutrients during follow-up showed more, or as much, improvement during this time as those who switched to medications—despite those who switched to medication being more impaired at the start of follow-up and therefore arguably having more “room to move.”
While it makes sense that those who had already responded well to the micronutrient treatment would choose to continue it, and that participants who had not responded well would seek other treatment options, it is surprising that the proportion of treatment responders at the 52-week follow-up among those who had switched to medications was not higher. This may be partly explained by the use of a global measure of improvement from baseline to define treatment response, as ADHD medications target ADHD symptoms specifically and not other domains of function. In contrast, micronutrient treatment appeared to lead to improvements in a number of domains, including ADHD symptoms, anxiety, and mood. The impact of dominant treatment during follow-up on other domains such as mood and anxiety differed according to the mode of treatment. Those who switched to medication and those who stopped all treatment displayed mood deterioration during the follow-up period, while those who continued micronutrients maintained the improvements observed at the end of the OL trial. Although parent-rated anxiety scores continued to improve for those who remained on micronutrients, they remained stable for those who discontinued treatment and worsened slightly for those who switched to medication. This is unsurprising, given that mood and anxiety symptoms are commonly reported side effects of stimulant medication; benefits of micronutrients for these symptoms have been reported in several previous studies (Kaplan et al. 2004, 2015a; Rucklidge et al. 2011; Frazier et al. 2013; Sole et al. 2017). Another explanation may be that the participants who switched to medication represented a group of children who are less likely to benefit from a biological intervention, given that they were also less likely to respond to the micronutrients.
Those who stopped the micronutrients and did not seek other interventions did relatively poorly, which appeared to highlight that stopping the micronutrients tends to result in deterioration in functioning with a minority staying well. Indeed, 60% of these participants were rated as much to very much improved globally at the end of OL trial, compared with 21% at the 52-week follow-up. It is difficult to draw clear conclusions about this group, as they were a heterogeneous mix of participants, including some who had benefitted from micronutrient treatment, but chose to stop it, and others who did not derive benefit and chose to discontinue micronutrients and not try psychiatric medications. Overall, given the significant decline in many of the responders in this group at 52 weeks compared to 20 weeks, the results suggest that the majority of children may need to continue taking micronutrients to derive continued benefit. This observation is consistent with results described by Rucklidge et al. (2017) in their naturalistic follow-up of adults with ADHD 1 year after entering a randomized placebo-controlled trial of micronutrients, and is consistent with the proposed mechanisms of action of micronutrients. If micronutrient supplementation improves psychiatric symptoms by providing nutrients required for optimal physiological function, through mechanisms of action such as correcting possible inborn errors of metabolism or by improving mitochondrial functioning (Rucklidge and Kaplan 2013), then it is plausible that continued supplementation may be necessary to facilitate continued improved function.
We asked participants about their reasons for stopping micronutrients and determined that, similar to the clinical trial on adults with ADHD (Rucklidge et al. 2017), the cost and the requirement to take a large number of pills were the greatest barriers to continuing treatment. Importantly, side effects were not identified as a barrier to treatment, and neither was lack of approval by others. Indeed, at 1-year follow-up, those who stayed on micronutrients did not report any ongoing problematic side effect. This shows that the acceptability of micronutrient use among the families and close communities of children with ADHD was good, even when they did not continue using them after the trial. Unlike micronutrients, psychiatric medications are generally heavily subsidized in New Zealand and available to consumers at minimal cost. However, if an individual is on a benefit, then in some cases, the benefit may also cover micronutrients, especially if medications have been proven to be ineffective in the past, as was the case for half of the children who stayed on the micronutrients. This explains why the SES of those who stayed on was not substantially higher than those who stopped. Given the favorable outcomes, good levels of acceptance, and the lack of side effects associated with micronutrient treatment observed in this study, it is interesting to consider how many would stay on the micronutrients if there was no cost barrier. This could be an important question in future micronutrient studies.
Limitations
Nine participants (<10% of the original sample) could not be assessed at 52 weeks postbaseline. Reasons included researchers being unable to contact them (n = 4), families declining follow-up (n = 1), and changing caregivers (n = 4). While it is possible that the exclusion of this group may have influenced the results of the follow-up study, 90% is a high rate of retention of the original sample. Rucklidge et al. (2017) reported a similar proportion lost to follow-up in their study of adults with ADHD. Those not followed up had slightly higher baseline clinician-rated inattentive ADHD symptoms, but otherwise were very similar to those who were followed up, making it unlikely that group differences observed at 52 weeks postbaseline were due to the exclusion of these participants.
A small group of participants (n = 9) had lacked consistency in the main treatment used during follow-up to be allocated to a specific dominant treatment category and were therefore excluded from analysis. While this was necessary to better understand the outcomes of specific chosen treatment options following an RCT and OL trial, it is possible that excluding these participants may have influenced outcomes. Given this was a naturalistic follow-up, the dominant therapy was not random, but based on family choice. As such, an inherent bias may exist in that, those who stayed on micronutrients may have wished to justify the cost expenditure by reporting favorably on their child's outcome. It is also possible that the clinicians, who were not blind to treatment choice, may have inadvertently had a bias toward rating children who remained on micronutrients positively, given the focus of the laboratory's research on investigating nutritional interventions for psychiatric problems. Having an external rater would have been ideal to assess benefit across different settings, such as a teacher; however, changes in teachers over time made such an extended evaluation over time unfeasible.
The comparison between the medication group versus the micronutrient group is not an entirely level playing field, both because those who switched to medications represented children who appear to possibly be “treatment resistant” and also because the duration on the medication treatment was shorter. The fact that medications tend to work more quickly than micronutrients could partially mitigate this concern.
In addition to financial costs, the number of capsules needed to be taken daily remains one of the most challenging aspects to ongoing micronutrient treatment for psychiatric conditions, and is reportedly a significant contributing factor to poor adherence and treatment discontinuation. Encouragingly, Rucklidge et al. (2018) reported good adherence during a 10-week randomized, placebo-controlled trial of micronutrients with children with ADHD, and only 20 of the 366 children screened were ineligible to enter the trial due to problems swallowing capsules. Due to this concern, the companies producing micronutrient supplements are striving to improve nutrient delivery to allow the same dose to be delivered in fewer capsules.
Conclusions
Broad-spectrum micronutrients as a front-line form of treatment for psychiatric symptoms in both children and adults are gaining increasing research support. This study demonstrates that for those children who stay on micronutrients longer-term (one year), they maintain their short-term benefits alongside a very favorable side-effect profile. A minority of children who are exposed to micronutrients maintain changes even after stopping them; however, most children who stop the micronutrients showed regression in symptoms over the longer period of time. Benefits were observed not only in the core ADHD symptoms, but also across anxiety and mood as well. Compared with those who switched to medications, outcomes were more favorable for those on micronutrients. Future studies could usefully investigate how the micronutrients might exert their effects, with some preliminary studies suggesting potentially small epigenetic effects (Stevens et al. 2018) as well as changes to the microbiome (Stevens et al. 2019).
Clinical Significance
ADHD can be a challenging disorder to treat and often there is not sufficient evidence available about longterm benefits of those treatments. This study, alongside the adult ADHD study (Rucklidge et al. 2017), demonstrate that about 20% of people from the initial randomization sample stay on micronutrients for at least a year and that as a group, their symptoms have reduced into the normal nonclinical range with no concerning long term side effects (Rucklidge et al. 2019). This study provides reassuring data to indicate that for those who benefit in a short term trial, consistent continued use of trial micronutrients leads to long-term benefit, not only in ADHD symptoms, but in other areas of functioning as well, such as improved mood and anxiety. Micronutrient treatment is worthy of consideration as a first step in the treatment of children with ADHD symptoms. Micronutrients may also provide a beneficial treatment option for children who respond poorly to medication. Further research needs to investigate the use of micronutrients alongside standard treatments in order to assess viability of combining treatments in order to further enhance outcomes.
Acknowledgments
The authors thank the families who took part in this research; David Pugh-Williams for assistance with randomization; Leona Manna for cultural consultation; and Lucy Kioa, Kate Harris, Anna Lee, Joanna Lothian, Dr. Brigette Gorman, Dr. Heather Gordon, and Molly Harvie for their assistance with data collection and entry. The authors also thank the Canterbury District Health Board and other private referrers for help with recruitment.
Trial prospectively registered with the Australian New Zealand Clinical Trials Registry (ANZCTR): ACTRN12613000896774.
Disclosures
Hardy Nutritionals provided the micronutrient formula and matched placebo for research at no cost. The 48-ingredient formula has had a number of minor modifications, and is now sold under product names Daily Essential Nutrients, and EMPowerplus Advanced. The authors have declared that they have no competing or potential conflicts of interest.