
Abstract
Background:
Many children and adults with Obsessive-Compulsive Disorder (OCD) fail to respond to first-line pharmacological and behavioral treatments. Glutamate dysfunction may contribute to the development of OCD. N-acetylcysteine (NAC), a glutamate modulating drug, has shown to be a promising agent in adults with OCD.
Methods:
We conducted a double-blind, placebo-controlled clinical trial from July 2012 to January 2017. Children ages 8 to 17 years with OCD were assigned to receive NAC (up to 2700 mg/day) or the matching placebo for a period of 12 weeks. Children were required to be on stable psychiatric treatment (both medication and therapy) but were not required to be treatment-refractory. The primary outcome was OCD symptom severity as measured by the Children's Yale-Brown Obsessive-Compulsive Scale (CY-BOCS). We used linear mixed models to analyze the effect of NAC compared to placebo.
Results:
Due to poor recruitment and eventual expiration of the study medication, enrollment was stopped at 11 children out of a planned sample size of 40. Nonetheless, NAC was associated with significant reduction in CY-BOCS total score compared to placebo (Satterthwaite's test: t (37) = 2.36, p = 0.024) with effects separating from placebo beginning at week 8. Mean CY-BOCS total score decreased in the NAC group from 21.4 ± 4.65 at baseline to 14.4 ± 5.55 at week 12. In the placebo group, mean CY-BOCS total score remained unchanged (21.3 ± 4.65). In the NAC group, 1 out of 5 participants achieved >35% improvement in CY-BOCS total score, while none of the six patients in placebo group reached this improvement level. NAC and placebo were well tolerated. One mild adverse event was reported in each group.
Conclusions:
Our trial suggests that there may be some initial improvement in OCD symptom severity with NAC treatment. NAC was well tolerated in the study population. Future trials should employ multiple sites and have a larger study population to further confirm any benefits of NAC.
Introduction
Obsessive-compulsive disorder (OCD) is characterized by time-consuming obsessions and compulsions that cause disruptions in functioning and significant distress (American Psychiatric Association 2013). Studies show that the prevalence of pediatric OCD is between 1% and 3% (Flament et al. 1988; Douglass et al. 1995). OCD frequently has a major negative impact on quality of life in children (Coluccia et al. 2017).
First-line therapy for moderate to severe pediatric OCD involves the combination of serotonin reuptake inhibitors (SRIs) and cognitive behavioral therapy (Geller et al. 2012). Although most children with OCD experience improvement with these treatments, approximately half of children with OCD do not experience clinical remission after combination treatment (Pediatric OCD Treatment Study (POTS) Team 2004). Many individuals with OCD who do respond to treatment still experience significant residual symptoms. Hence, novel treatment options are needed for children with OCD.
Current evidence suggests that glutamate dysfunction may contribute to the pathophysiology of OCD (Pittenger et al. 2011; Kariuki-Nyuthe et al. 2014). N-acetylcysteine (NAC), a glutamate-modulating drug, has shown to be a promising agent in adults with OCD (Lafleur et al. 2006; Afshar et al. 2012; Paydary et al. 2016). Trials examining the efficacy of NAC in adults with OCD have revealed mixed results (Lafleur et al. 2006; Afshar et al. 2012; Sarris et al. 2015; Paydary et al. 2016; Costa et al. 2017).
To the best of our knowledge, no randomized controlled trial has investigated the effect of NAC exclusively for pediatric OCD. Pediatric NAC trials for other psychiatric conditions have demonstrated that NAC is safe and well tolerated in children (Hardan et al. 2012; Bloch et al. 2013, 2016; Nikoo et al. 2015; Wink et al. 2016). We hypothesized that NAC is safe and effective in improving OCD symptom severity in children. To test this hypothesis, we conducted a double-blind, placebo-controlled clinical trial.
Methods
Setting, study design, and patients
Children ages 8 to 17 years with a primary diagnosis of OCD were recruited through Yale Child Study Center from July 2012 to January 2017. Children were included in the study if they had OCD for more than 6 months and their Children's Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) score was ≥16 at the time of enrollment. Children were recruited through targeted outreach to local providers and through posted study flyers around the Tourette syndrome (TS)/OCD Clinic and Yale Child Study Centers. Recruitment methods were similar to our two previous studies examining NAC in the treatment of trichotillomania and TS (Bloch et al. 2013, 2016).
Exclusion criteria included a comorbid psychotic disorder, bipolar disorder, developmental disorder, intellectual disability (IQ <70), or substance use disorder. Children were not eligible when the dosage of medications with possible effects on OCD severity had been changed in the 4 weeks before enrollment in the study. Both discontinuation of medication and alteration of dosage were considered as changes. If children were taking selective serotonin reuptake inhibitor (SSRI) medications for OCD, children were required to be maintained on SSRI medications for at least 12 weeks before enrolling in the trial. Children were excluded if behavioral therapy for the treatment of OCD was altered within the 4 weeks or initiated within 12 weeks before enrollment. Children who used asthma medication within 3 months of enrollment were also excluded given that there is some evidence that patients with asthma have an increased risk of developing adverse reactions to NAC (Schmidt and Dalhoff 2001; Appelboam et al. 2002).
Other exclusion criteria included known hypersensitivity to NAC, a positive pregnancy test, a positive drug screening test and previous use of >600 mg of NAC for longer than 2 weeks. Finally, children with a proven or suspected diagnosis of cystinuria were not allowed to participate in the study since NAC might increase the risk of forming kidney stones in children with cystinuria. Study medication could be taken as either a stand-alone medication or added to stable existing treatments for OCD.
The Institutional Review Board approved protocol was explained to eligible participants and their parents before enrollment in the study. Written informed assent was obtained from the child and written informed consent from the parents. This trial was registered in the National Institutes of Health Registry of Clinical Trials (identifier: NCT01172275).
Intervention
An investigational pharmacist randomized participants on a 1:1 basis. One arm received NAC (Bioadvantex Brand) effervescent tablets and the other arm received matching placebo effervescent tablets. The tablets were indistinguishable in appearance, odor, and flavor. Children, parents, and investigators were blind to which arm the child was assigned until after assessments were completed at week 12. To determine efficacy of blinding, children and investigators were asked whether they thought the child received NAC or placebo.
The target NAC dosage was 2700 mg/day. Children received one 900 mg tablet (either NAC or placebo) once a day during the first week of the trial. The second week children received one 900 mg tablet twice a day and during week 3 to the end of the study (week 12) they received one 900 mg tablet three times a day and continued on this dose through week 12. After study completion, NAC was offered to children in the placebo arm. At each visit, the participants and their parent(s) were asked about medication compliance. Participants were asked whether they were still taking the medication and whether they had missed any doses. The numbers of remaining tablets were not recorded.
Baseline, efficacy, and tolerance assessments
Baseline data (age, gender, ethnicity, comorbid psychiatric diagnosis, current use of medication, and ongoing or past behavioral therapy) were collected at enrollment. A physical examination, including vital signs, was performed and urine was collected for a drug screening and pregnancy test.
The primary outcome, OCD symptom severity, was measured using the CY-BOCS. The CY-BOCS contains a 5-item subscale for obsessions and a 5-item subscale for compulsions. A score from 0 (no symptoms) to 4 (extreme symptoms) was assigned for each item. Scores from the items were then combined to calculate the subscale scores and the total CY-BOCS score (Goodman et al. 1989). Overall improvement from baseline was assessed using the Clinical Global Impression (CGI) scale. The scale ranges from 1 (very much improved) to 7 (very much worse). A score of 4 indicates no change (Guy 1976). Adverse events were assessed with the Pediatric Adverse Events Rating scale. The Pediatric Adverse Events Rating scale contains 45 questions related to adverse events experienced. A number indicating severity from 0 (not present) to 4 (extreme) was assigned to each question (Shapiro et al. 2009).
CY-BOCS scores were determined at baseline, weeks 2, 4, 8, and 12. Global improvement subscale score and Pediatric Adverse Events Rating scale scores were determined at weeks 2, 4, 8, and 12.
Power calculation and analysis
Based on our sample size calculation (α = 0.05, β = 0.2, Δ = 0.9, dropout rate = 10%), we intended to include 40 children. Due to poor recruitment and eventual expiration of the study medication, enrollment was stopped at 11 children. We believe presentation and publication of negative pediatric NAC trials from our group in related conditions significantly hampered our ability to recruit for this study (Bloch et al. 2013, 2016).
We performed descriptive analyses to summarize data collected at enrollment. We computed frequencies with percentages for categorical variables and means with standard deviations for normally distributed continuous variables.
To analyze the effect of NAC on CY-BOCS total score and CGI scores, we conducted intention-to-treat analyses. We used linear mixed models with an unstructured covariance matrix and restricted maximum likelihood. In this model, we explored intervention, time (repeated assessments within subjects), and intervention by time interaction. When there were missing values, a linear mixed model only excluded these particular missing values from the analysis instead of excluding the whole case. Linear mixed models maximized the use of the available data. Adverse events between groups were compared with Fisher's exact test. All analyses were conducted with the R language 3.4.0.
Results
Study sample
Of the 40 children screened, 19 children declined participation and 10 were not eligible based on inclusion and exclusion criteria. A total of 11 children were eligible and agreed to participate in the study. The investigational pharmacist randomized 5 children to NAC treatment and 6 to placebo. Speculation by children and investigators about randomization suggested that blinding was successful (2 of 3 children receiving NAC and 3 of 6 children receiving placebo guessed treatment assignment correctly at week 12). In the NAC group, two participants did not complete the trial. One child did not complete any follow-up assessments, decided to discontinue after taking one to two tablets (but reported no side effects), and contributed no follow-up data and one child took the medication inconsistently in the setting of family turmoil (impending divorce of parents) and was dropped from the trial after week 4 (Fig. 1).
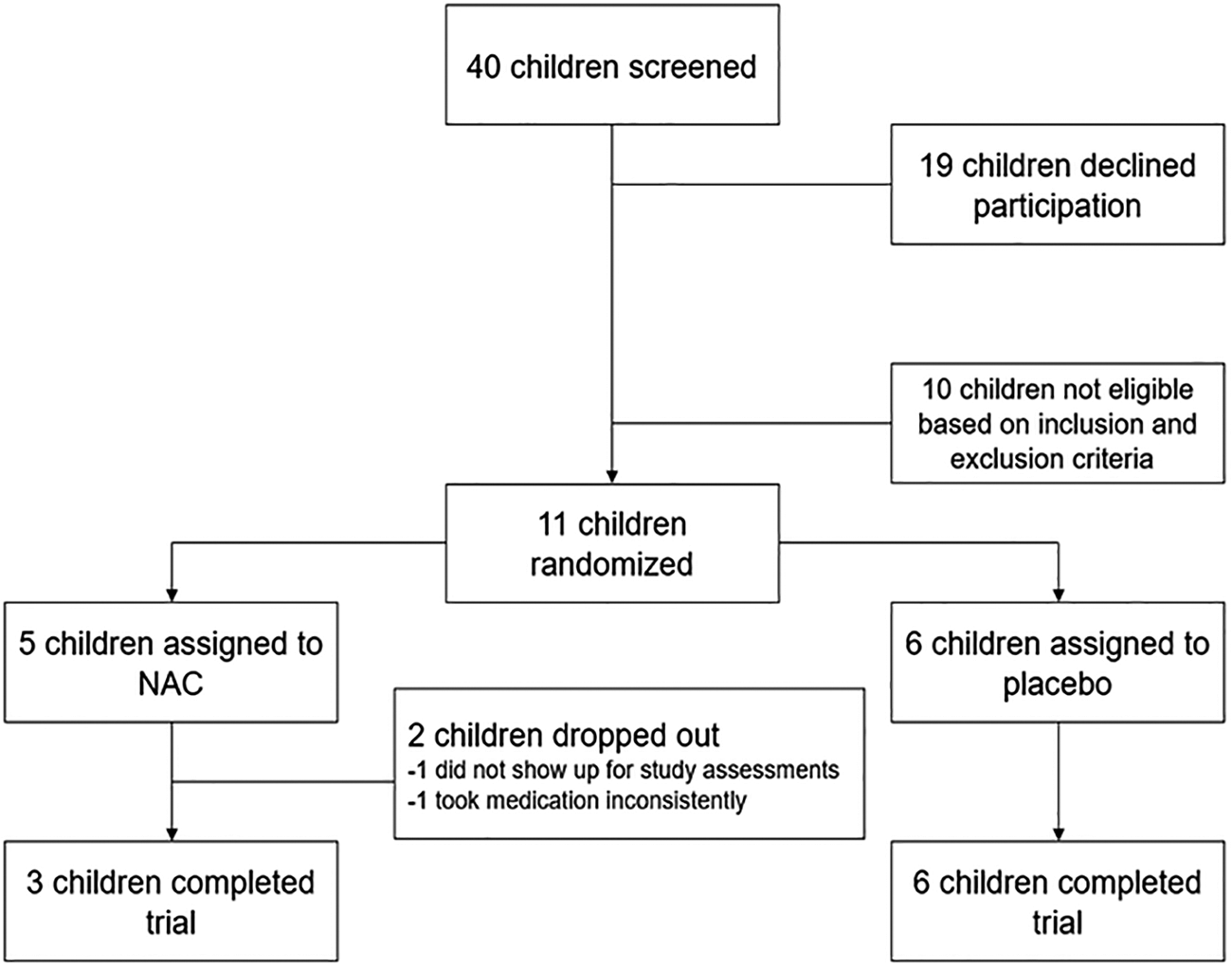
CONSORT diagram. NAC, N-acetylcysteine.
Table 1 summarizes the baseline characteristics of the study population. There was no statistically significant difference between groups at baseline. Average age in the NAC group was 13.4 ± 3.4 years (mean ± standard deviation) and 10.7 ± 1.9 years in the placebo group. The most common comorbidities were attention-deficit/hyperactivity disorder and TS. In both treatment groups, two children were concurrently taking an SRI. Baseline CY-BOCS score was 21.4 ± 4.65 (mean ± standard deviation) for participants in the NAC group and 21.3 ± 4.65 for in the placebo group.
Baseline Characteristics of the Study Population
ADHD, attention-deficit/hyperactivity disorder; CY-BOCS, Children's Yale-Brown Obsessive-Compulsive Scale; MDD, major depressive disorder; NAC, N-acetylcysteine; PTSD, posttraumatic stress disorder; SD, standard deviation; SRI, serotonin reuptake inhibitor.
Efficacy
Figure 2A depicts the effect of on CY-BOCS score over time in the treatment groups. Mean CY-BOCS score decreased in the NAC group from 21.4 ± 4.65 at baseline to 14.4 ± 5.55 at week 12. In the placebo group, mean CY-BOCS scores remained largely unchanged (21.3 ± 4.65 at baseline to 21.3 ± 4.64 at week 12) over the 12-week trial. Linear mixed model analysis suggested a significant benefit of NAC compared to placebo. Significant interaction between the factors of week number and treatment was observed in the mixed model for CY-BOCS score (Satterthwaite's test: t (37) = 2.36, p = 0.024). The contrasts between NAC and placebo groups revealed no difference in CY-BOCS scores between the two groups from baseline to week 4. Average symptom severity, as measured by CY-BOCS score, in the NAC group was significantly less than placebo group in weeks 8 and 12. One out of five patients in the NAC group demonstrated >35% improvement in CY-BOCS score, while no patients in placebo group reached this improvement level. Figure 2B depicts each study subject's trajectory in CY-BOCS ratings throughout the trial.
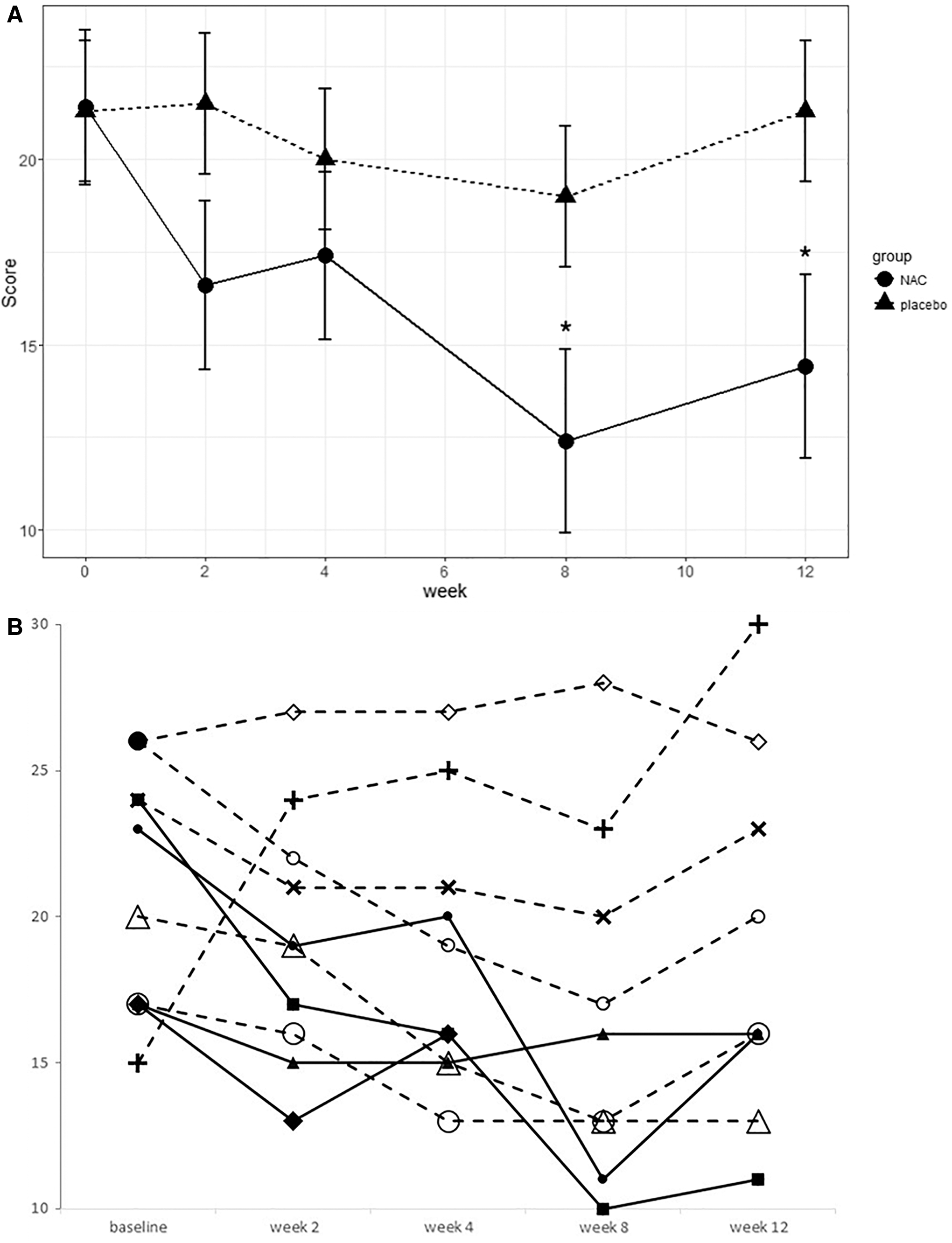
Effects of NAC and placebo on OCD Severity. OCD severity was measured with the CY-BOCS.
No significant effect of NAC was demonstrated for CGI-I ratings (Satterthwaite's test: time: t (29) = −1.79, p = 0.084; treatment: t (20) = −1.41, p = 0.175, time X treatment: t (28) = 1.51, p = 0.141). CGI-I scores of the NAC and placebo groups were 3.2 ± 1.16 and 3.5 ± 0.90, respectively, at study endpoint.
Safety
In the NAC group, 1 subject (20%) reported a skin rash. In the placebo group 1 subject (17%) reported diarrhea. There was no statistically significant difference between groups. Adverse events were mild and not thought to be medication related.
Discussion
This trial examined the efficacy of NAC in pediatric OCD. The study was aborted, before the primary recruitment goal of 40 subjects because of poor recruitment and eventual expiration of the study medication. Limited data in the 11 children suggested some preliminary evidence of improvement in OCD symptom severity with NAC treatment on the CY-BOCS. We did not observe similar improvement on the CGI scale or in terms of OCD treatment responders. NAC was well tolerated in the study population. Two of the children in the NAC group were dropped out early but the dropouts were related to inability to reliably take study medications or failure to complete study assessments rather than side effects of the medication.
Since limited data were collected, our trial is underpowered to detect a treatment benefit. We believe the poor recruitment was primarily related to the presentation and publication of negative NAC trials conducted in pediatric TS and trichotillomania (Bloch et al. 2013, 2016). Negative results from these trials adversely affected physician referral of children to the clinic, and successful recruitment of subjects if referred. Despite the extremely small sample size, several children in the NAC group experienced a substantial improvement in OCD symptom severity, in contrast to the placebo group in which no children experienced improvement. The improvement was noteworthy, statistically significant, and worthy of further investigation.
Five previous randomized, placebo-controlled trials of NAC have been conducted in adults with OCD with mixed results. Two add-on studies have reported a significant benefit (Afshar et al. 2012; Paydary et al. 2016), whereas two other add-on studies did not (Sarris et al. 2015; Costa et al. 2017). A single randomized, placebo-controlled trial compared the effects of starting adjuvant NAC (2400 mg/day) or placebo with citalopram (20–40 mg/day) over 10 weeks with 34 OCD outpatients that included both children and adults (Ghanizadeh et al. 2017). The trial demonstrated significant benefits of adjuvant NAC compared to placebo. The treatment benefit of NAC was large (effect size = 0.83) despite the fact that NAC was started concurrently with citalopram, another medication with benefit for OCD. The NAC was also well tolerated in these trials.
Conclusion
Despite the limited sample size, our study provided some promising initial evidence regarding the efficacy of NAC in reducing OCD symptoms in children. Improvements in OCD symptom severity seen in the NAC group were substantial and occurred early in a few subjects but were not observed with placebo. These benefits contrast with our previous negative trials in pediatric trichotillomania, and TS. Future randomized controlled clinical trials with larger study population and longer follow-up time to elucidate the short-term and long-term effects of NAC on pediatric OCD severity are needed.
We suspect that our inability to recruit for this trial was based on local factors (multiple negative NAC trials in similar conditions compromising recruitment) and not reflective of families' willingness to take NAC to treat OCD. Given that NAC is an over-the-counter supplement, careful characterization of the constituents of the medication is extremely important, as discrepant findings between NAC trials may not only be related to heterogeneity in study design but also actual differences in the quality and content of the NAC medication.
Footnotes
Clinical Significance
Currently, there is a strong evidence base for the efficacy of both SSRI pharmacotherapy and CBT as first-line treatments for OCD. Evidence regarding the efficacy of NAC for the treatment of OCD and related conditions is mixed. This trial, although severely underpowered, provided some initial evidence regarding the possible efficacy of NAC for pediatric OCD. Given that NAC is an over-the-counter supplement, clinicians should be mindful of the quality and content of the NAC supplements as this has been hypothesized to make a difference in potential efficacy.
Disclosures
No competing financial interests exist.