
Abstract
Objectives:
Premonitory urges (PUs) are defined as sensory experiences of pre-tic inner tension. Evidence suggests that most patients with Tourette syndrome experience PUs, which are transiently relived by the expression of tics. However, recent studies have revealed inconsistent results regarding the correlation between the severity of PUs and the severity of tic symptoms.
Methods:
A meta-analysis was performed to confirm the correlation between the severity of the urge and the severity of the expression of the tic. In total, 10 studies involving 626 patients with tic disorders were included in this meta-analysis.
Results:
The correlation coefficient (r) was extracted from each selected study, and a pooled correlation coefficient (r) and its 95% confidence intervals (CIs) were calculated. Sensitivity and subgroup analyses were performed to identify the potential sources of heterogeneity. The pooled correlation coefficient (r) of the relationship between the severity of PUs and tic symptoms was 0.296 (95% CI: 0.215–0.376) with an I 2 of 15.2% (95% CI: 0.00–56.5) based on a fixed effects model. The correlation was stronger in adults than in children (p = 0.03).
Conclusion:
A slight to moderate positive correlation was observed between the severity of PUs and tic symptoms. This correlation may be affected by the age of the patients. Further research should seek to elucidate the relationships among PUs, tic suppression, and tic expression to support the development of behavioral intervention therapies to reduce tic symptoms.
Introduction
Joseph Bliss was the first to describe “uncomfortable bodily feelings” related to tics (Bliss 1980). Subsequently, the term “premonitory urges (PUs)” began to be used to describe these sensory symptoms (Rajagopal et al. 2013; Ganos et al. 2015; Draper et al. 2016). It has been reported that nearly 70%–90% of patients with Tourette syndrome (TS) experience PUs (Gulisano et al. 2015; Sambrani et al. 2016). Although the diagnostic criteria for TS does not include PUs, they are regarded as a core symptom in patients with TS (Houghton et al. 2014; Cox et al. 2018). Notably, PUs play a critical role in psychological interventions for tics because addressing PUs facilitates the more efficient inhibition of tic expression (Banaschewski et al. 2003; Ganos et al. 2012). For instance, Gev reported that “Acceptance of PUs” therapy, which is based on Acceptance and Commitment Therapy, could reduce tic frequency (Gev et al. 2016). Therefore, exploring and understanding the relationship between PUs and the occurrence of tics facilitates the development of new therapies for the treatment of tic disorders.
Recent evidence supports the relationship between PUs and the severity of tics (Reese et al. 2014; Kano et al. 2015). However, some inconsistent results need to be clarified. For example, no correlation was found between PUs and tic severity in several studies (Steinberg et al. 2010, 2013; Gulisano et al. 2015). Other studies have reported a significant positive correlation between PUs and tic severity (Crossley and Cavanna 2013; Ganos et al. 2015; Rozenman et al. 2015). The reason for this inconsistency may be the different age groups or different stages of tic disorders in various studies, but more confirmatory evidence is needed.
Moreover, obsessive-compulsive symptoms are commonly identified in patients with tic disorders (Miguel et al. 2000). Several studies have also reported a significant correlation between the severity of PUs and obsessive-compulsive symptoms (Woods et al. 2005; Neal and Cavanna 2013; Gulisano et al. 2015; Kano et al. 2015). However, negative results have also been reported (Reese et al. 2014). Further studies are needed to clarify this relationship.
Therefore, in this study, a meta-analysis was performed to explore the correlation between the severity of PUs and tics. Another meta-analysis was conducted to elucidate the correlation between PUs and the severity of obsessive-compulsive symptoms in patients with tic disorders. We hypothesized that moderate positive correlations exist between the severity of PUs and tics and between PUs and the severity of obsessive-compulsive symptoms in patients with tic disorders.
Methods
We searched for relevant studies in four databases, namely, PubMed, Web of Science, ProQuest, and PsycINFO. The terms “Premonitory Urges OR Sensory Phenomena” and “tic OR Chronic Tic Disorders OR Tourette Syndrome” were used to identify relevant studies. The publication dates of the studies extended to January 1, 2019. The reference lists of the selected studies were manually cross-checked.
Both the inclusion and exclusion criteria were developed to select relevant studies. The inclusion criteria were as follows: (1) PUs were assessed by a validated scale; (2) the severity of the tic symptoms was assessed by a validated scale; (3) the relationship between the severity of PUs and tic symptoms was reported; and (4) the correlation coefficient was available.
The exclusion criteria were as follows: (1) duplicated studies; (2) the subjects were not patients with tic disorders; and (3) the study was not original research but rather a review article, case report, comment, or other type of publication. In addition, studies reporting a correlation coefficient between the severity of PUs and obsessive-compulsive symptoms were included, and the pooled r was calculated.
Based on the inclusion and exclusion criteria, in total, 10 studies were identified (for more details, see Fig. 1)
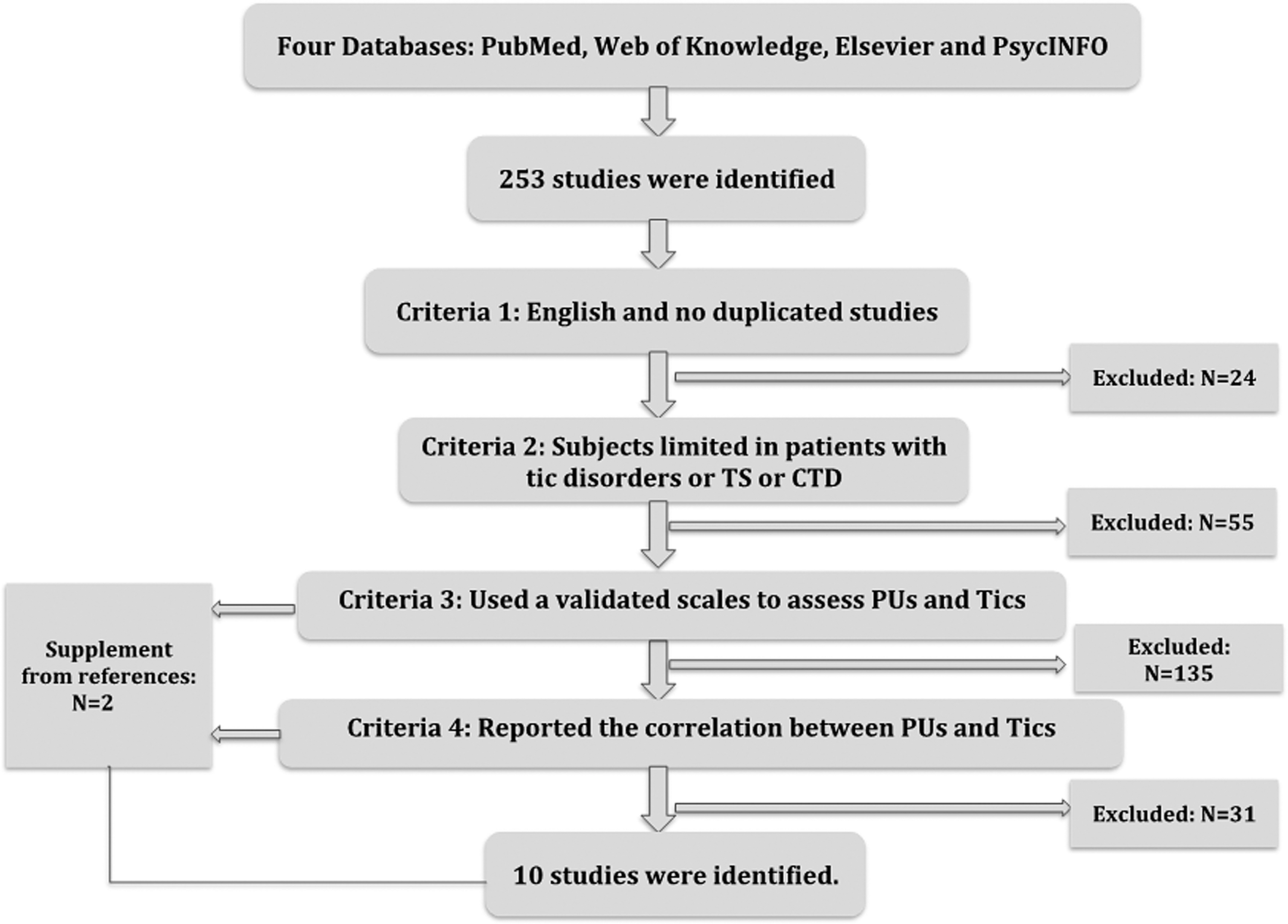
Flowchart of the study identification.
The following information was extracted from each study: authors; publication date; the number of patients; mean patient age and standard deviation (SD); the scale used to assess the PUs, the mean value and SD; the scale used to assess tic severity, the mean value and SD; and the correlation coefficient (r) between the severity of PUs and tics and the p-value if available.
The pooled r and 95% confidence interval (CI) were calculated. The heterogeneity of the pooled r was calculated with Cochran's Q test. If the I 2 was >50% or p was <0.05 (Q test), a sensitivity analysis was conducted to identify the source of the heterogeneity. Subgroup analyses were conducted and stratified by age (≥18 years and <18 years). No publication bias was found based on a Begg's funnel plot (p > 0.05) (Fig. 2). STATA version 11 (Stata Corporation, College Station, TX) was used to perform the analyses mentioned earlier.
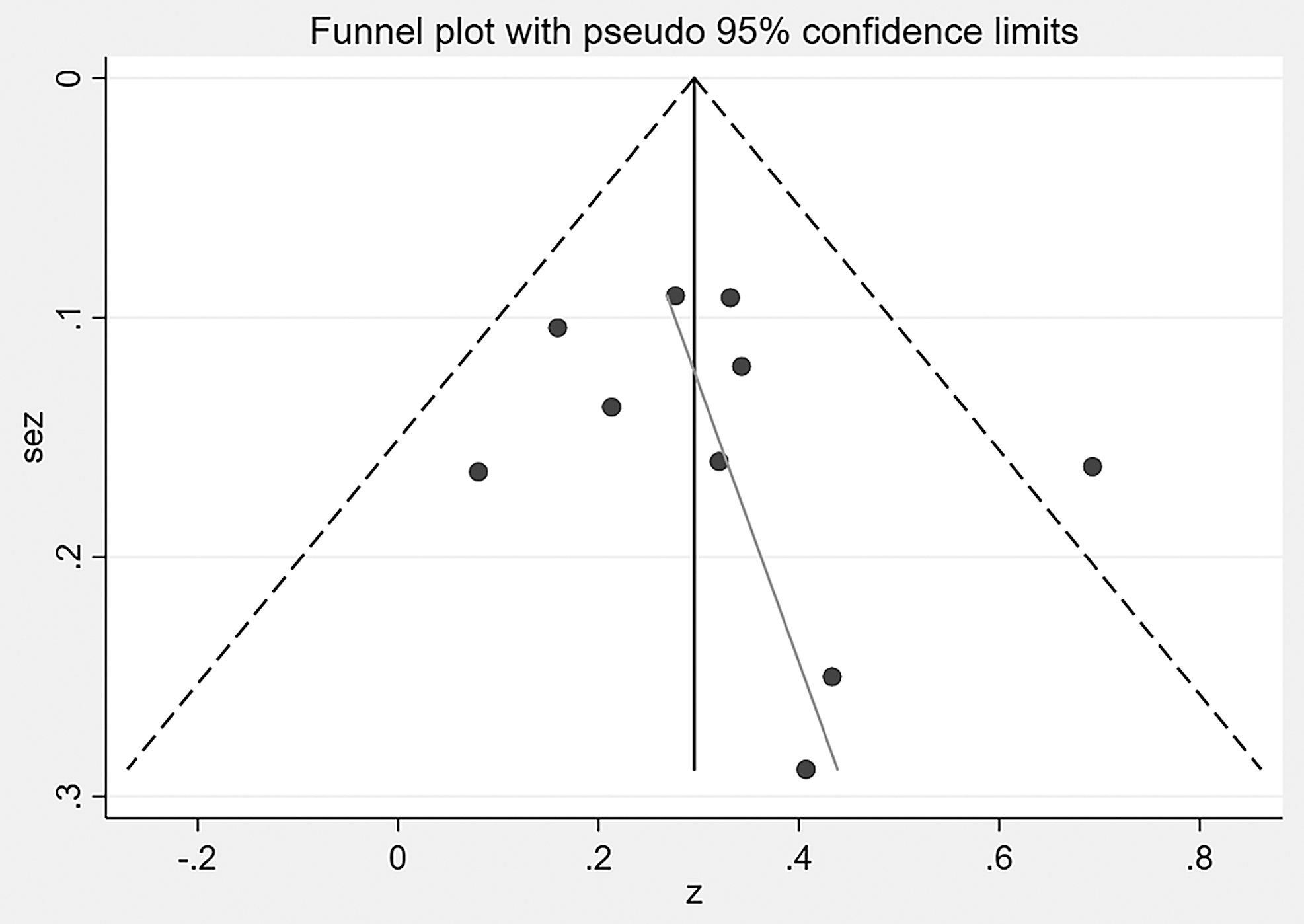
Funnel plot with pseudo 95% confidence limits.
Results
According to the inclusion criteria, 10 studies involving 626 patients with tic disorders were identified. All included studies reported the severity of PUs, which was assessed by the Premonitory Urges for Tics Scale (PUTS), and the severity of the tics was measured with the Yale Global Tic Severity Scale (YGTSS). The extracted data from each selected study are summarized in Table 1. All included studies reported the correlation coefficient of the relationship between the PUTS scores and the YGTSS scores. Six studies also reported the correlation coefficient of the relationship between the PUTS scores and obsessive-compulsive symptoms scores as assessed with a validated scale. The pooled r of the relationship between the PUTS scores and the total YGTSS scores was calculated along with the corresponding heterogeneity. The pooled r was 0.296 (95% CI: 0.215–0.376), and the I 2 was 15.2% (95% CI: 0.00–56.5) based on the fixed effects model. A Q test was conducted, but no significant heterogeneity was found (Q = 10.62, degrees of freedom [df] = 9, p = 0.303). More details are provided in Figure 3.
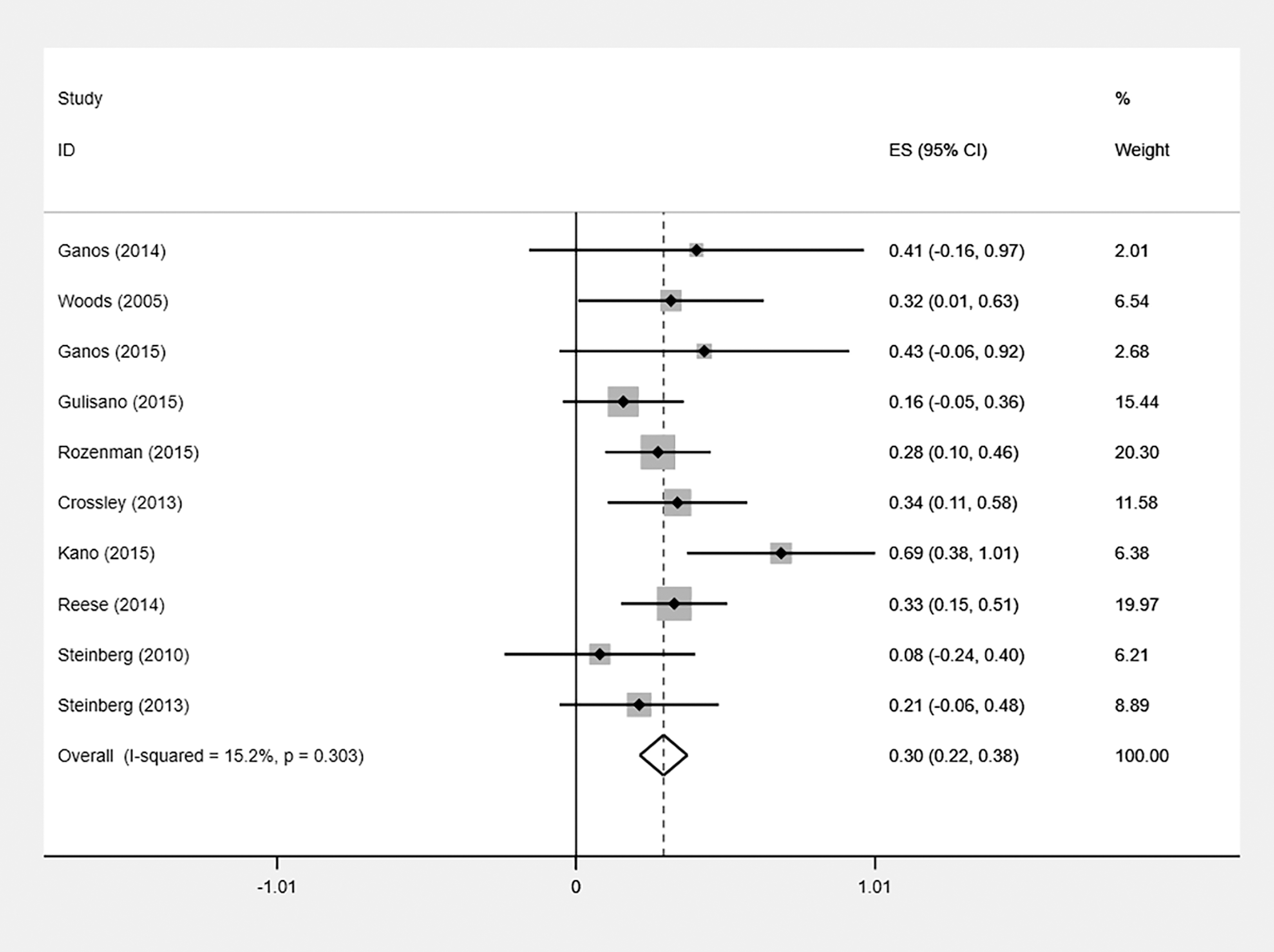
Forest plots of the summary correlation coefficient (r) with corresponding 95% confidence interval for the correlation between the severity of premonitory urges and tic symptoms (N = 10).
Description of the Selected Studies
TS, Tourette syndrome; CTD, chronic tic disorders; PU, premonitory urge; PUTS, Premonitory Urge for Tics Scale; YGTSS, Yale Global Tic Severity Scale; YBOSC, Yale–Brown Obsessive Compulsive Scale; CYBOSC, Children's Yale–Brown Obsessive Compulsive Scale.
In the subgroup analysis stratified by age (adults, mean age ≥18 years; children, mean age <18 years), there was a significant difference between the two subgroups (p = 0.03). More details are provided in Figure 4 and Table 2.

Forest plots of the summary correlation coefficient (r) with corresponding 95% confidence interval for the correlation between the severity of premonitory urges and tic symptoms after subgroup analysis by age.
The Result of Subgroup Analysis
N/A, not available.
In addition, the pooled r of the relationship between the PU scores and obsessive-compulsive symptom scores was 0.334 (95% CI: 0.227–0.440). However, significant heterogeneity was identified (I 2 = 57.1%) (Supplementary Fig. S1), with a positive Q test (Q = 11.65, df = 5, p = 0.04). Therefore, a sensitivity analysis was conducted to identify the source of the heterogeneity, and one study (Reese et al. 2014) was excluded. The pooled r was recalculated after excluding this study (r = 0.45, 95% CI: 0.32–0.58) (I 2 = 0.0%) (Fig. 5).
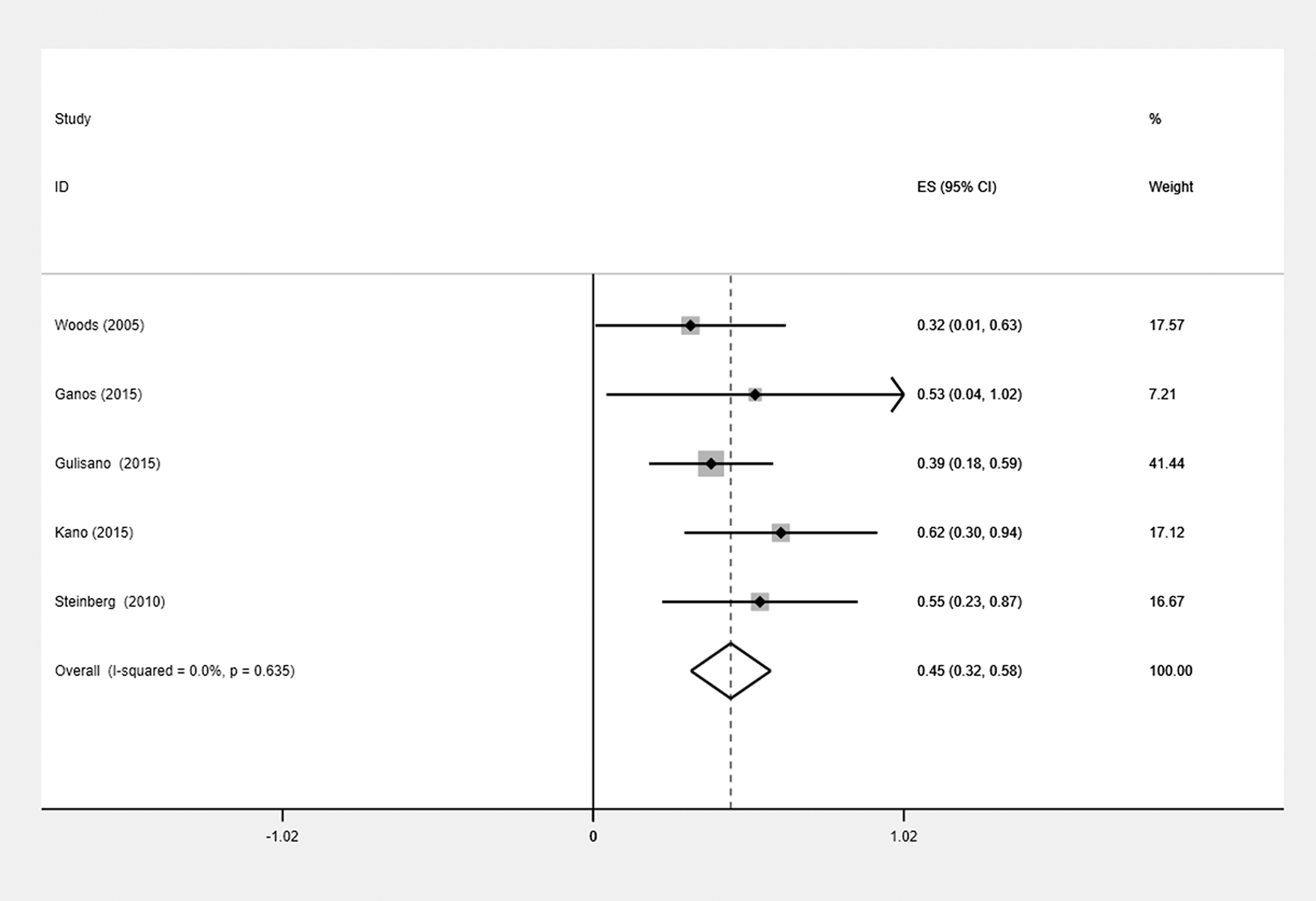
Forest plots of the summary correlation coefficient (r) with corresponding 95% confidence interval for the correlation between the severity of premonitory urges and obsessive-compulsive symptoms after removing one study with heterogeneity (N = 5).
Discussion
In this meta-analysis, we found a slight to moderate positive correlation between the severity of PUs and tic symptoms and a moderate positive correlation between the severity of PUs and obsessive-compulsive symptoms. The correlation in adults was stronger than that in children. This finding indicates that the correlation between the severity of PUs and tic symptoms may be moderated by age.
In this study, the instrument used to assess PUs in the selected studies was the PUTS, which was developed by Woods et al. (2005) and has adequate psychometric properties (Crossley and Cavanna 2013). Although the PUTS has been widely used to assess the severity of PUs, it also has some limitations. Brandt et al. (2016) designed a real-time urge monitor to determine the validity of the PUTS. Based on his results, Brandt et al. (2016) pointed that it would be worthwhile to develop different subscales of the PUTS to assess the intensity and quality of PUs. To the best of our knowledge, the assessment of PUs relies on the patients' ability to report their uncomfortable feelings. Recently, Raines et al. (2018) found that the PUTS has adequate psychometric properties in children >10 years. However, the validity of the PUTS is poor when the age of the patients with TS is <10 years (Banaschewski et al. 2003). It seems that the age of 10 is a critical time for becoming aware of and reporting PUs. For future studies, reliable biological markers are needed to assess PUs in young patients (<10 years old) with TS.
In this study, we found a slight to moderate correlation between the severity of PUs and tic symptoms. This study provided evidence confirming the relationship between the symptom of PUs and tics. Owing to their role in tic expression, PUs have been regarded as a core symptom in patients with TS (Robertson et al. 1999). Additional studies focusing on the relationship between PUs and tics could facilitate the development of assessments and interventions for tics. For example, PUs are included as an indispensable part of the formal evaluation of tic disorders in the statement of the European Society for the Study of TS (Cath et al. 2011). Moreover, PUs have been identified as an important predictor of the quality of life in patients with TS (Cavanna et al. 2012). For intervention for tics, an awareness of PUs could help patients better recognize their tic symptoms and facilitate the suppression of tic symptoms (Himle et al. 2007). In addition, Comprehensive Behavioral Intervention for Tics is a well-developed therapeutic method based on enhancing the patients' awareness of PUs that is effective in reducing tic symptoms (Piacentini et al. 2010; Dutta and Cavanna 2013; Frank and Cavanna 2013).
Based on the results of this study, PUs are not only a preprocess part of tic expression but also an important process that occurs before the generation of obsessive-compulsive symptoms in patients with TS. Notably, ∼90% of TS patients present with other psychiatric disorders, and obsessive-compulsive disorder is one of the most common comorbidities (Lombroso and Scahill 2008; Mula et al. 2008; Eddy and Cavanna 2014). Indeed, as a type of sensory phenomenon, PUs are also often reported by patients with obsessive-compulsive disorder (Kano et al. 2015). Moreover, sensory phenomena are experienced by patients with most movement disorders, such as pain in patients with Parkinson's disease or dystonia and urge phenomena in patients with restless legs syndrome, akathisia, or primary motor stereotypies (Patel et al. 2014). It seems that there are shared sensory abnormalities among various movement disorders. Further imaging or neurophysiological studies are needed to better understand the mechanisms underlying the sensory abnormalities in patients with TS, obsessive-compulsive disorder, and other related movement disorders (Cavanna et al. 2017).
In summary, it is important to elucidate the relationships among PUs, tic suppression, tic expression, and the brain circuits involved (i.e., the insula cortex, cingulate cortex, caudate nucleus, and cortico-striato-thalamo-cortical circuits) in future research regardless of the theoretical or neurobiological perspective.
There were two limitations in this study. First, the number of studies included in the meta-analysis was small, which may reduce the strength of the conclusions. Second, studies with negative results are often not published, and positive or significant results are most often reported. A larger sample size is needed to confirm the correlation between the severity of PUs and tic symptoms and the changes in that correlation based on age. In addition, the assessment of PUs was based on individuals' subjective feelings before tics; however, this assessment may be influenced by the subjects' emotions, cognition, and so on. More accurate devices, such as a polygraph, are needed to assess PUs in future studies.
Conclusion
Despite the limitations of this study, it represents the first meta-analysis of PUs. A slight to moderate correlation was observed between the severity of PUs and tic symptoms. This correlation may be moderated by age. Further research is needed to elucidate the relationships among PUs, tic suppression, and tic expression to facilitate the development of behavioral intervention therapies to reduce tic symptoms.
Clinical Significance
A small-to-moderate positive correlation was identified between the severity of PUs and tic symptoms. Age appears to moderate this correlation. It seemed that new tools are needed for the assessment of PUs in children <10 years. PUs are an important indicator of not only tic expression but also obsessive-compulsive symptoms in patients with tic disorders.
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.