
Abstract
Objectives:
Although tic disorder (TD) is a common mental disorder in children and adolescents, epidemiological data based on real-world evidence (RWE) are insufficient. Using RWE, this study sought to examine the prevalence of treated TD, use of medical utilization, and use of prescription drugs among patients with TD with respect to TD type and comorbid psychiatric illness.
Methods:
We performed a retrospective cross-sectional study. Using the Korean Health Insurance Review and Assessment Service Pediatric Patient Sample data from 2009 to 2016, we analyzed 20,599 patients with TD (Korean Standard Classification of Diseases-6/7 code: F95.x) aged 2–19 years.
Results:
The annual average TD prevalence was 2.6/1000 population (95% confidence interval, 2.3–2.8/1000). Between 2009 and 2016, a slight increase in TD prevalence was observed from 1.9 to 2.9/1000 population. The TD prevalence rate in male patients was four times higher than that in female patients. Differences were observed in health care utilization and drug prescription types between patients with Tourette syndrome and chronic or transient TD. In addition, more than half of patients with TD had comorbid psychiatric disorders, and one-third of patients with TD had attention-deficit/hyperactivity disorder (ADHD). Patients with TD without comorbidities were frequently prescribed aripiprazole, while patients with TD and comorbid ADHD were frequently prescribed atomoxetine, methylphenidate, risperidone, and aripiprazole.
Conclusion:
This study described the epidemiological characteristics of TD based on recent RWE from Korea, and its findings can help establish future TD evidence-based clinical guidelines and related policies.
Introduction
Tic disorder (TD) is a relatively common neurodevelopmental disorder that occurs during the pediatric and adolescent periods. Between 11% and 20% of school-aged children transiently experience TD (Scahill et al. 2014). TD is characterized by voluntary yielding to irresistible urges, or the frequent production of sounds such as sniffing and coughing (American Psychiatric Association 2013). Tourette syndrome (TS) is the most severe form of TD. TS is diagnosed in patients with TD who have persistent vocal and motor tic symptoms lasting more than 1 year. Between 0.4% and 3.8% of school-aged children have been reported to experience TS (Scahill et al. 2014).
The reported prevalence rates of TD and TS vary widely depending on age, disease definition methodology, and regional factors (Knight et al. 2012). In western countries, TD prevalence rates widely range between 3.4% and 24.4% (Robertson 2006). A recent large-scale patient study in China indicated that TD prevalence rates vary between 1.7% and 23.8% and were dependent on the region examined (Rothenberger et al. 2007). There is known to be a genetic effect on the expression of TD (Peterson et al. 1992; Ooki 2005). However, studies on TD epidemiology in Korea are very scarce.
Patients with TD are known to have accompanying psychiatric disorders. Approximately 20% of patients with TD have attention-deficit/hyperactivity disorder (ADHD) (Chen et al. 2013), and 55%–60% of patients with TS were reported to have ADHD (Freeman 2007). Moreover, a high proportion of patients with TD suffer from obsessive-compulsive disorder (OCD), anxiety disorder, or depression (Scahill et al. 2014). Drug and nondrug (e.g., educational treatment, behavioral therapy) treatment strategies for patients with TD vary depending on the patients' comorbid psychiatric disorders. Thus, whether patients with TD also have major comorbid psychiatric disorders is an important factor in providing appropriate medical treatment (Rothenberger et al. 2007).
Various psychotropic drugs, including antipsychotic, cholinergic, norepinephrine, and GABAergic drugs, are used to treat TD (Roessner et al. 2013; Yang et al. 2016). Dopamine receptor dysfunction has been hypothesized to be involved in TD pathogenesis (Cheon et al. 2004). Therefore, antipsychotic drugs targeting the dopaminergic system are commonly used in patients with TD. European guidelines recommend the atypical antipsychotic drug risperidone as a first-line treatment for TD (Roessner et al. 2011), whereas Canadian guidelines instead recommend the antiadrenergic agents clonidine and guanfacine (Pringsheim et al. 2012). Thus, drug prescriptions for patients with TD vary based on country-specific guidelines and comorbid illnesses based on real-world settings. Country-specific drug use studies are therefore of utmost importance.
The aims of the present study were (1) to examine changes in the prevalence rates of TD and the use of medical utilization (i.e., types of health care institutions and regions, physician specialties, number of outpatient visits, and so on) and (2) to evaluate drug prescription characteristics according to comorbidities using real-world population-based data from 2009 to 2016 in Korea. Our study findings will ultimately contribute to the establishment of country-specific evidence-based treatment directions for patients with TD based on real-world evidence (RWE).
Methods
Data sources
To analyze the epidemiological characteristics of pediatric and adolescent patients with TD based on RWE, we used the Korean Health Insurance Review and Assessment Service (HIRA)-Pediatric Patient Sample (PPS) data from 2009 to 2016, which are derived from health insurance claims (data serial nos. HIRA-PPS-2009-0051, 2010-0068, 2011-0077, 2012-0065, 2013-0069, 2014-0053, 2015-0063, and 2016-0059) (HIRA 2018). Because Korea maintains a government-managed single-payer health insurance system, the HIRA data contain the medical records of the entire Korean population and are highly representative. The HIRA-PPS data include yearly medical records of a 10% random sample of all patients who are younger than 20 years of age in South Korea (i.e., inpatient, outpatient, emergency visits, and prescription records for 1 year of ∼1,000,000 pediatric patients). Basic patient demographics (sex, age, and health security program type), medical records (diagnosed illness, treatment, medical department, and prescription drug information), and medical institution information (health care institution type and region, physician specialty, and whether the patient consulted a specialist) can be examined with the HIRA-PPS dataset (Kim et al. 2014). Ethics approval was obtained from the Institutional Review Board at Yonsei University (IRB No. 7001988-201812-HR-506-01E). The need for informed consent from the study population was waived by the Board.
Study population and comorbidities
This study included 20,648 2–19-year-old patients who were diagnosed at least once with TD between 2009 and 2016 based on the HIRA-PPS data. For TD, the following Korean Standard Classification of Disease (KCD) Version 6/7 F95 codes were used, which are derived from and very similar to the International Classification of Diseases: (1) F95.0 (transient TD), (2) F95.1 (chronic motor or vocal TD), (3) F95.2 (TS), (4) F95.8 (other TD), and (5) F95.9 (unspecified TD) (Korean Standard Statistical Classification, 2019). Patients who were <2 years old were excluded from this study because of the uncertainty of their TD diagnoses. In addition, because hospitalization due to TD is very rare (0.2% of total TD patients), only outpatients were included in this study, resulting in a final study population of 20,599 outpatient subjects. To identify the characteristics by type of TD, we classified TD patients diagnosed with KCD-6/7 F95.2 codes as the TS patient group; TD patients diagnosed with F95.1 codes as the chronic TD patient group, and the remaining patients (F95.0, F95.8, or F95.9) as the transient TD patient group. Patients with TD and comorbid psychiatric disorders diagnosed with a KCD-6/7 code F at least once per year were defined as patients with other psychiatric disorders. In this study, the major comorbid psychiatric disorders identified were ADHD (F90.0), depression (F32), affective disorder (F93), schizophrenia (F20), anxiety disorder (F41), and OCD (F42). To analyze drug prescription by comorbid psychiatric disorders, we classified TD patients into those without any mental comorbidities, those with comorbid ADHD, and those with comorbid mental illnesses other than ADHD. ADHD is reported to be the most frequent comorbid mental disorder with TD, one of the most common mental disorders in children and adolescents regardless of comorbidity with TD, and is currently increasing in prevalence in South Korea (Song et al. 2017).
Variables and pharmacological treatments
Sex, age, health security program and health care institution types, comorbidities, and drug prescription data for patients with TD were analyzed. Health security program types were divided into two categories as follows: (1) National Health Insurance (NHI) and (2) medical aid (MA), in which enrollees of low socioeconomic status receive government support. Health care institution regions were categorized as metropolitan (e.g., Seoul, Gyeonggi, and Incheon), other cities, and rural regions. Physician specialties were categorized as psychiatry, nonpsychiatry, and oriental medicine. The number of outpatient visits and referrals for TD evaluation and treatment for each year were also examined.
To analyze patients' psychiatric drug prescriptions, we divided the subjects into those with and without prescriptions. We then surveyed all the medications that patients were prescribed when they visited a medical facility for TD. The medications were categorized using World Health Organization Anatomical Therapeutic Chemical Classification (WHO-ATC) ingredient codes. To examine the recent prescription tendencies of patients with TD, we analyzed the medications frequently prescribed to patients each year. The prescribed medications were categorized as ADHD, antipsychotic, antidepressant, anticholinergic, or anxiolytic medications. We examined the associations of medication types and prescription frequencies with different TD types and comorbidities. ADHD medications included methylphenidate (WHO-ATC code: N06BA04) and atomoxetine (N06BA09). Clonidine, which is a representative alpha-2 adrenergic agonist that can be prescribed for ADHD patients, was not included in this study, as this drug was not listed on the government's drug list until 2015. Antipsychotic medications were divided into first- and second-generation antipsychotics (FGA and SGA, respectively). FGAs included haloperidol (N05AD01) and pimozide (N05AG02), and SGAs included risperidone (N05AX08) and aripiprazole (N05AX12). Antidepressant medications were divided into selective serotonin reuptake inhibitors (SSRIs) and other antidepressants. SSRIs included fluvoxamine (N06AB08), fluoxetine (N06AB03), escitalopram (N06AB10), and sertraline (N06AB06), and other antidepressants included nortriptyline (N06AA10). Anticholinergic medications included benzatropine (N04AC01) and procyclidine (N04AA04). Anxiolytic medications included alprazolam (N05BA12), clonazepam (N03AE01), diazepam (N05BA01), and propranolol (C07AA05). In Korea, amphetamines (N06BA01, N06BA02, and N06BA03 of WHO-ATC code) are not included on the government's drug list, so physicians are unable to prescribe them.
Statistical analyses
This study was a retrospective, population-based, cross-sectional study. The annual TD prevalence rates (i.e., number of people with TD per 1000 population) for each sex were calculated for the 2–19-year-old population using Korean Census data (Korean Statistical Information Service, 2018). The denominator was the total population of youths in the age group 2–19-year age group in Korea, and the numerator was the number of patients who were diagnosed with TD in the same age group. The total number of children aged 2–19 in Korea during the period from 2009 to 2016 is as follows: 10,845,808 in 2009, 10,691,920 in 2010, 10,435,171 in 2011, 10,179,341 in 2012, 9,945,529 in 2013, 9,721,667 in 2014, 9,456,220 in 2015, and 9,211,812 in 2016.
Annual TD prevalence per 1000 population in the age group 2–19 years = (Number of pediatric patients aged 2–19 years with TD/total number of pediatric population aged 2–19 years) × 1000
Descriptive statistics were used to analyze the characteristics of outpatients with TD. To analyze the differences between patients with TD and TS or chronic or transient TD, analysis of variance was used for continuous variables, and the chi-square test was used for categorical variables. To analyze the differences between patients with and without comorbid ADHD, we used a t-test for continuous variables and the chi-square test for categorical variables. All the analyses were performed using SAS statistical software (version 9.4; SAS Institute, Inc., Cary, NC). The significance level was set at p < 0.05.
Results
TD prevalence in children and adolescents
From 2009 to 2016, TD prevalence rates in patients aged 2–19 years continuously increased from 1.9 to 2.9/1000 population. In 2016, the TD prevalence of male subjects increased by 1.5 times than that in 2009 (i.e., from 3.0 [2009] to 4.5 [2016] per 1000 population). In 2016, the prevalence of female subjects increased by nearly 1.7 times than that in 2009 (i.e., from 0.7 [2009] to 1.2 [2016] per 1000 population) (Fig. 1). Although the absolute number of male patients was approximately four times larger than the number of female patients, the rate of increase in TD prevalence was slightly higher in female patients than in male patients.

Prevalence of patients with treated tic disorders between 2009 and 2016 in Korea.
TD epidemiology in children and adolescents
Table 1 shows the basic characteristics of 20,599 patients with TD who visited outpatient departments from 2009 to 2016. The average age of patients with TD was ∼10 years, and about 75% of patients were >8 years or within the school-aged population. Compared with hospitals, clinics were more commonly visited by patients with TD. Health care institution regions were divided as follows: metropolitan (55%–58%), city (26%–29%), and rural (18%–20%). In 2016, 78.3%, 16.8%, and 10.1% of patients with TD visited psychiatry, nonpsychiatry, and oriental medicine specialists, respectively. These percentages were also maintained consistently throughout the study period. On average, patients with TD visited health care institutions 6.5 times in 2009 and 8.0 times in 2013.
Epidemiology of Outpatients with Tic Disorders from 2009 to 2016 in Korea
If a patient visited ≥2 physician specialties, then duplicate results might have been obtained.
In 2009, oriental medicine codes were not generated, which prevented calculations for this year.
ADHD, attention-deficit/hyperactivity disorder; NHI, National Health Insurance; OCD, obsessive-compulsive disorder; SD, standard deviation; TD, tic disorder.
In addition, on average, one-third of patients with TD also had ADHD. The percentage of patients with TD and ADHD increased from 28.5% to 41.0% from 2009 to 2013, after which this percentage slightly decreased to 32.9% in 2016. In 2016, the most common comorbidities of patients with TD were as follows: ADHD (32.9%), depression (15.5%), anxiety (11.3%), emotional disorders with onset specific to childhood (6.8%), OCD (5.5%), and schizophrenia (5.1%). Approximately 60% of patients with TD had no drug prescription history, and 40% had prescriptions for TD and comorbidity-related drugs.
Comparison of Tourette disorders with chronic and transient TD
As shown in Table 2, analyses following the categorization of TD as TS or chronic or transient TD showed that the number of patients with TS increased annually from 5.9% to 18.2% from 2009 to 2016, whereas the number of patients with chronic TD decreased from 14.0% to 8.4% during the same period. Transient TD prevalence rates did not significantly change between 2009 and 2016. The age and sex distributions of patients with TS and chronic TD were similar, with over 80% of patients being male. In contrast, over 20% of patients with transient TD were female, and the percentage of female patients with transient TD was higher than the percentage of female patients with TS and chronic TD. Approximately 80% of patients with TS and chronic TD had at least one comorbid psychiatric disorder. Of these patients, 46.2% and 44.1% of those with TS and chronic TD had ADHD, respectively. Moreover, 20.4% and 13.2% of patients with TS and chronic TD had depression, respectively. In contrast, about 60% of patients with transient TD did not have comorbid psychiatric disorders. Of these patients, 23.1% had ADHD comorbidity.
Comparison Between Patients with Tourette Syndrome and Transient or Chronic Tic Disorders
If a patient visited ≥2 physician specialties, then duplicate results might have been obtained.
ADHD, attention-deficit/hyperactivity disorder; IQR, interquartile range; NHI, National Health Insurance; OCD, obsessive-compulsive disorder; SD, standard deviation; TD, tic disorder; TS, Tourette syndrome.
TD Patients with comorbid ADHD
Table 3 shows the results of a comparison between patients with only TD without comorbid psychiatric disorders and patients with TD and ADHD. In this analysis, TD referred to all TD types, including TS. Compared to patients with TD or TS only, patients with TD and ADHD consisted of a significantly higher proportion of pediatric and adolescent boys (88.6% vs. 76.9%) as well as adolescents between 13 and 19 years (29.5% vs. 16.5%). Patients with ADHD visited medical institutions eight times annually because of TD; in contrast, patients with TD alone visited medical institutions only twice a year. Only 27.4% of patients with TD without comorbidities received drug prescriptions, whereas 55.1% of patients with TD and ADHD received drug prescriptions.
Comparison Between Patients with Only Tic Disorders or Tourette Syndrome and Those with Tic Disorders or Tourette Syndrome and Attention-Deficit/Hyperactivity Disorder
If a patient visited ≥2 physician specialties, then duplicate results might have been obtained.
ADHD, attention-deficit/hyperactivity disorder; IQR, interquartile range; NHI, National Health Insurance; SD, standard deviation; TD, tic disorder; TS, Tourette syndrome.
Pharmacoepidemiology patterns of patients with TD
The SGAs risperidone and aripiprazole were the most frequently prescribed drugs. From 2009 to 2016, the prescription frequency of risperidone decreased, whereas that of aripiprazole continuously increased. The next most frequently prescribed medications for patients with TD were the ADHD drugs methylphenidate and atomoxetine. During the study period, the prescription rate of methylphenidate decreased from 26.4% to 19.1%; however, the prescription rate of atomoxetine increased from 14.4% to 24.4%. Moreover, benzatropine and haloperidol were prescribed frequently, and their prescription rates did not significantly change during the study period (Fig. 2).
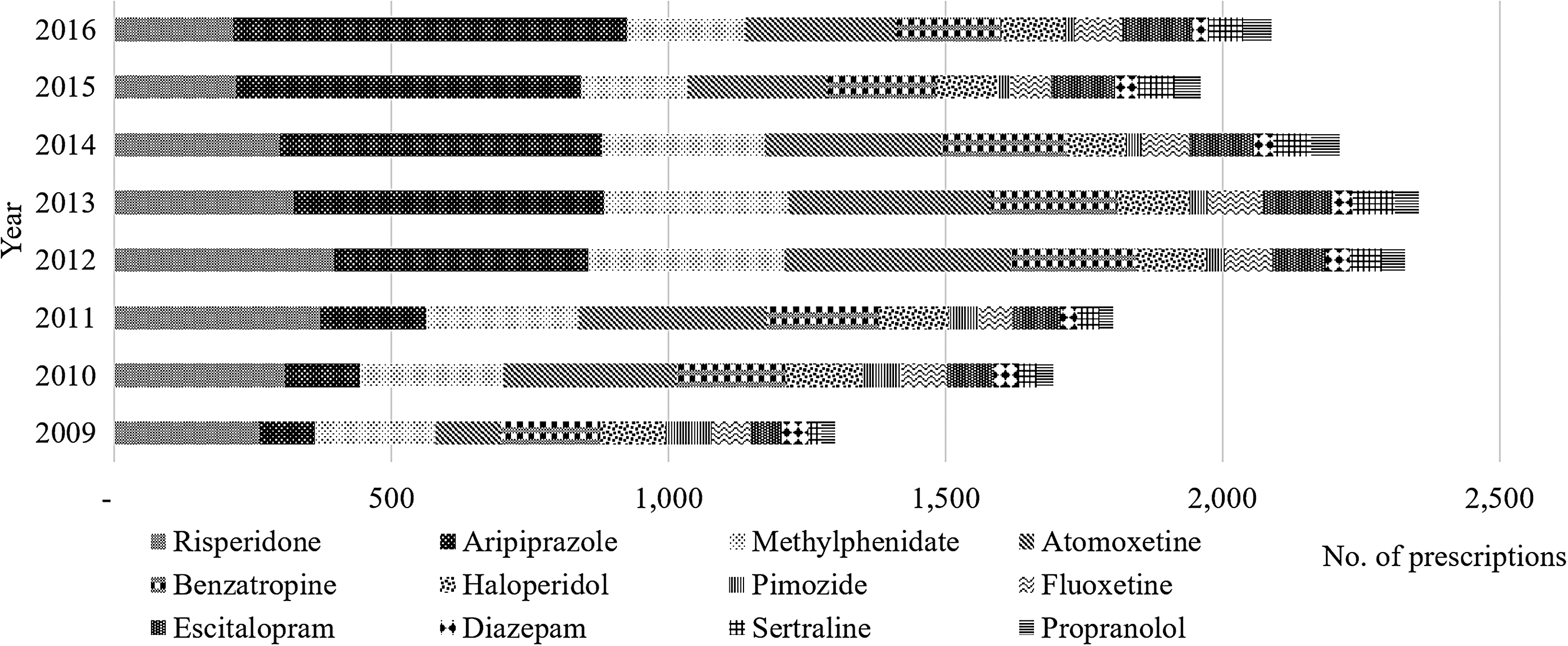
Prescription drug changes in patients with treated tic disorders from 2009 to 2016 in Korea.
Table 4 shows the prescription trends for the following three groups: TD or TS without comorbidities, TD or TS with ADHD, and TD or TS with non-ADHD psychiatric comorbidities. More than half of patients with TD and ADHD (3980/7226 × 100 = 55.1%) were prescribed medication; however, only about one-quarter of patients with only TD (2291/8360 × 100 = 27.4%) without any other psychiatric comorbidities were prescribed medication. The proportion of SGA prescriptions was high for all of the groups. In addition, about one-quarter of TD patients with ADHD were prescribed methylphenidate or atomoxetine, respectively. We observed relatively higher rates of SSRI prescription among TD patients with comorbid ADHD (15.9% = 1.9% +5.0% +5.7% +3.3%) than among patients with TD without other psychiatric comorbidities (0.6% = 0.2% +0.2% +0.1% +0.1%). The most frequently prescribed SSRI was escitalopram in TD patients with ADHD as well as in patients with other psychiatric disorders. Moreover, a higher anxiolytic prescription rate (5.2% = 1.6% +1.9% +1.7%) was observed in patients with TD and other psychiatric comorbidities than in patients with TD and ADHD (2.5% = 0.4% +1.1% +1.0%).
Psychotropic Prescription Trends in Patients with Tic Disorders or Tourette Syndrome With or Without Comorbidities
Other comorbidities included depression, anxiety, schizophrenia, and obsessive-compulsive disorder.
ADHD, attention-deficit/hyperactivity disorder; TD, tic disorder; TS, Tourette syndrome.
Discussion
This study analyzed the drug use trends and basic epidemiological characteristics of pediatric and adolescent patients with TD using population-based RWE from 2009 to 2016 in Korea. We found that TD prevalence in 2–19-year-old patients was 2–3/1000 population. Moreover, the measured TD prevalence was lower than the prevalence of patients with TS (0.77%) or transient TD (2.99%) reported by a previous meta-analysis (Knight et al. 2012).
The TD prevalence of patients in Korea was much lower than that reported among patients in China (6.1%), despite these nations being localized in the same Asian region (Rothenberger et al. 2007). We hypothesize that the low TD prevalence rate in Korea is significantly affected by sociocultural views on pediatric and adolescent psychiatric disorders rather than by ethnic or genetic differences. In Korea, seeking medical treatment for psychiatric disorders in adolescence and childhood is considered taboo (Park and Jeon 2016). Guardians often believe that receiving medical treatment from the NHI can lead to future rejection by private insurance companies or cause social misunderstandings. Consequently, there are significant obstacles to treating pediatric and adolescent psychiatric disorders. Because these sociocultural characteristics can lead to TD treatment being conducted outside the scope of health insurance, the management of patients with TD is often underestimated. Therefore, multifaceted efforts are needed in Korean society to better assess pediatric and adolescent psychiatric disorders. Having recognized these problems since the late 2000s, the Korean Academy of Child and Adolescent Psychiatry (KACAP) has attempted to advocate for early intervention in pediatric and adolescent psychiatric disorders and to prevent private insurance enrollment rejections at the national level. In our study, the gradual increase in TD prevalence observed in recent years may reflect changing views concerning pediatric and adolescent psychiatric disorders due to KACAP efforts.
In 2016, the prevalence of TD was nearly 3.8 times higher in male than in female patients (4.5 vs. 1.2/1000 pediatric population). This is similar to the results of a previous study, in which the prevalence of TDs was higher in males than in females (Knight et al. 2012; Bachmann et al. 2015). The onset of TD and TS is known to be affected by genetic factors; however, there is no confirmed genetic risk factor for TD or TS (Ooki 2005). Sex hormones establish sexual dysplasia of the brain early in the development of the central nervous system. As such, there has been ongoing debate over effects of androgens, which are sex hormones, on the expression of TD (Peterson et al. 1992). The present study also reported differences in tic prevalence between males and females, suggesting that the expression of TD may be related to the genetic influence of sex hormones.
Meanwhile, a previous study that analyzed pediatric and adolescent patients with psychiatric disorders found that the proportion of patients with MA was higher, and a relationship between patient socioeconomic status and psychiatric disorders was observed (Lee et al. 2018). However, in our study, 4% of patients with TD utilized MA, which was not significantly different from the percentage of MA enrollees in the total population (3.5%–4.0%) (Song 2009). The relationship between socioeconomic status and the prevalence of TDs is controversial (Khalifa and Von Knorring 2005; Miller et al. 2013). The current study used cross-sectional analysis to determine socioeconomic status by fragmentally segmenting it into enrollment in MA and non-MA (NHI). Thus, it is necessary to conduct further in-depth analyses of the relationship between socioeconomic status and the prevalence of TDs through longitudinal research.
In this study, patients with TD exhibited around a 3.5%–5.5% prevalence of OCD and a 3.9%–12.1% prevalence of anxiety disorder. These were lower prevalence rates than those reported in previous studies (Angst et al. 2004), suggesting that the low age sample in this study may have impacted these results. Previous studies have shown that nonclinical or subclinical OCD symptoms are usually observed during childhood and adolescence, and the onset age of OCD and anxiety disorder is usually in early adulthood (Ruscio et al. 2010; de Lijster et al. 2017). In this study, the analysis was conducted using a sample with a mean age of 10 years, and such a low sample age is thought to have resulted in the lower prevalence in this study compared with other studies. Meanwhile, the comorbidity rate of depression was 9.4% to 15%, slightly higher than the 9.7% comorbidity rate of TDs reported in a previous prevalence study (Kurlan et al. 2002).
In Korea, the SGAs risperidone and aripiprazole are prescribed at a high frequency for patients with TD. Aripiprazole is a dopamine D2 receptor partial agonist and has similar effects as those of haloperidol and risperidone in alleviating tic symptoms (Yang et al. 2015). Moreover, aripiprazole induces a relatively small amount of sedation and weight gain (Khanna et al. 2013). Therefore, aripiprazole is the preferred tic suppressant for use in Korea. In this study, the gradual observed increase in aripiprazole prescriptions suggests that Korean pediatric psychiatrists prefer aripiprazole. We also confirmed the variance in psychotropic prescription trends by psychiatric comorbidity. Patients with TD and ADHD had a relatively higher probability of receiving a prescription (55%) compared to those without ADHD (27%). A previous study indicated that ADHD presence is not significantly related to tic symptom severity (Pringsheim 2017). Moreover, adjuvant use of risperidone is helpful when ADHD is comorbid with other behavioral disorders (Jahangard et al. 2017). These findings may reflect a tendency to prescribe medication to control ADHD symptoms rather than tic symptoms. TD patients with comorbid ADHD had a higher usage rate of SSRIs compared to patients with TD alone. This suggests that the likelihood of emotional problems is higher in cases with comorbid ADHD than in cases without ADHD, suggesting that doctors need to focus more on patients' emotional problems when they identify a comorbidity of ADHD.
The greatest strength of this study is that it elucidated the nationwide epidemiological characteristics of patients with TD through the analysis of recent long-term data. These findings may reflect the epidemiology of all pediatric and adolescent citizens of Korea and have high generalizability. However, when interpreting the present results, the following limitations must be considered. First, the HIRA data are derived from a secondary database and consist of illness diagnosis codes and prescription records. Accordingly, diagnostic accuracy in these patients should be high. In addition, in these patients, medication is often administrated by guardians rather than by the patients themselves. Thus, medication adherence should not be low. Second, there was a lack of information on drugs prescribed for off-label usage. Therefore, it is possible that fewer drug prescriptions were reflected in this study than were actually prescribed for patients with TD. Third, ∼10% of patients with TD received oriental medicine treatment; however, oriental medicine prescription records were incomplete. The medications prescribed by oriental medicine specialists are different from those prescribed in psychiatric and nonpsychiatric medical institutions. Thus, there is a possibility that oriental medicine treatments for patients with TD were underestimated in our data.
Conclusions
This study showed that the prevalence of TD steadily increased from 2009 to 2016 in Korea. Moreover, medications prescribed to patients varied based on TD and comorbid psychiatric disorder types. By integrally evaluating the comorbid psychiatric disorders of patients with TD, our findings will help with the selection of treatment options for these patients. In the future, a follow-up study of patients with TD is needed to construct a basis for appropriate drug treatment and establish the effectiveness and safety of drug treatment in clinical practice.
Clinical Significance
This study generated RWE on the basic epidemiology of TD in the pediatric population based on nationally representative insurance claims data as follows: (1) we estimated the yearly prevalence of treated TD at 2.6/1000 population between 2009 and 2016, and it was found to be lower than in other countries; (2) patients with TS or chronic TD have different patterns of health care utilization compared to patients with transient TD; (3) approximately, one-third of patients with TD were concomitantly diagnosed with ADHD and frequently prescribed atomoxetine or methylphenidate with aripiprazole or risperidone. In addition, (4) we observed relatively higher rates of SSRI prescription among TD patients with ADHD than among those with TD only. This suggests that TD patients with comorbid ADHD are more likely to have emotional problems than those without psychiatric comorbidities.
Footnotes
Disclosures
The authors do not have any competing financial ties or conflict of interests to declare. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors and was not supported by any statistical consultants.