
Abstract
Objective:
Electroconvulsive therapy (ECT) is a well-recognized treatment of refractory mood disorders in adults. However, relatively little is known about its use for similar conditions in adolescents. Based on a chart review, we describe its use and outcome in a sample of adolescents with severe, refractory mood disorders (unipolar or bipolar disorder) hospitalized in an academic medical center.
Methods:
The sample was drawn from referrals to an adolescent psychiatry service. After obtaining approval from the ethics board, medical records of 54 adolescents with refractory mood disorder were examined. Participants (males 24, females 30; mean age 15.8 ± 1.5 years) had received their first course of ECT before the age of 18 years during the period 1996–2010. Response to treatment was examined after the initial treatment and during a 1-year follow-up.
Results:
Following the index course of ECT (mean number of treatments = 13.7 ± 6.3), a 52.8% response rate (defined as a Clinical Global Impressions [CGI] score ≤2) was noted, while 15.1% achieved remission (CGI = 1). The response rate was 82.4% after a 1-year follow-up with a remission rate of 23.5%. The Children's Depression Rating scores declined significantly from pre-ECT to the end of the index course (70.7 ± 16.4 to 52.5 ± 18; p ≤ 0.00). A reduction in suicidal ideation and self-injurious behaviors along with increased school attendance was noted. Cognition, monitored by the Mini-Mental State Examination, did not decline significantly. Minor side effects were limited to the day of the treatment. Prolonged seizures (>2 minutes) were common during ECT (74% of subjects experienced one or more). The only side effect noted at the 1-year follow-up was self-reported memory loss involving events during and around the index treatment course.
Conclusions:
In this severely impaired sample of adolescents, ECT was found to decrease suicidal behavior, reduce depressive symptoms, and improve overall functioning, as indexed by school attendance at follow-up after 1 year. Prospective studies using large samples are needed to determine its effectiveness and safety in refractory mood disorders in adolescents.
Introduction
Depression and other mood disorders are common conditions in adolescence (Lewinsohn et al. 1998; Avenevoli et al.
Pharmacotherapy of adolescent depression and bipolar (BP) disorder is of limited value in severe cases who have failed to respond to two or three antidepressants and/or mood stabilizers. A large controlled study of first-line treatment of adolescents with unipolar (UP) depression had found a 23% remission rate after 12 weeks and 60% after 36 weeks of treatment [Treatment of Adolescent Depression Study (Kennard et al. 2006, 2009)]. However, in adolescents who had previously failed even a single selective serotonin reuptake inhibitor (SSRI) (Treatment of SSRI-Resistant Depression in Adolescents study), a lower response rate of 50% was found at week 12 when an SSRI or venlafaxine was combined with cognitive behavioral therapy and ∼40% response rate was noted with pharmacotherapy alone. The remission rate on the other hand was only 39% for the entire sample at week 24 (Brent et al. 2008; Emslie et al. 2010).
It is notable that there are no systematic studies involving adolescents who fail to respond to two or more antidepressants and treatment at that point is often based on the clinician's personal experience. In general, factors associated with a poor response rate in adolescent depression include greater severity of self-rated depression, hopelessness, suicidal ideation (SI), nonsuicidal self-injury, subsyndromal manic symptoms, poor sleep, and family conflict (Asarnow et al. 2009; Maalouf et al. 2012; Shamseddeen et al. 2012). Regarding BP depression, with the exception of the Food and Drug Administration-approved combination of olanzapine and fluoxetine (Detke et al. 2015) and lurasidone (Delbello et al. 2017), there are no other widely accepted and safe treatments. Therefore, an important question in clinical practice is how to effectively treat adolescents with a severe mood disorder who have failed to respond to multiple medications and in whom waiting for a positive treatment response to other agents may result in further deterioration and even death.
In such adolescents, electroconvulsive therapy (ECT) is sometimes considered as a treatment option. However, the understanding of ECT in adolescents is largely based on studies in adults, some of which have reported prompt improvement in depressive symptoms with a 75% remission rate after a relatively short treatment course (Husain et al. 2004). The few studies published in adolescents also suggest that ECT can be effective (Zhang et al. 2012; Grover et al. 2013; Puffer et al. 2016; Mitchell et al. 2018). Bertagnoli and Borchardt (1990) reviewed all the publications between 1947 and 1990 on patients between 5 and 18 years of age and found a positive response to ECT in every publication with the exception of a single report involving four cases by Guttmacher and Cretella (1988). Similarly, Rey and Walter (1997) found 90% improvement in depression in an extensive review involving 396 patients (age ≤18 years), which included all publications in English and other languages published until 1996. The same authors found marked improvement in half of 42 participants (age range = 14–18 years) who had been treated at different institutions and had received ECT as the treatment of last resort after having failed multiple treatments (Walter and Rey 1997).
On reviewing 39 recent publications in youth ages 13–18 years, Lima et al. (2013) concluded that ECT was an effective treatment choice. This was supported by Puffer et al. (2016) who found a 77% improvement rate at the end of the acute treatment phase in 51 adolescents (mean age = 16.8 ± 1.6; females = 30) diagnosed with a range of psychiatric disorders (mood disorders, psychotic disorders, or catatonia). However, despite the generally positive conclusions of these studies, most of the findings are based on small samples; isolated case reports; clinically heterogeneous groups, which had combined mood and psychotic disorders; lack clarity about the time of assessment of treatment response; cross-sectional assessment conducted at the end of a course; and the use of largely subjective outcome measures. The current report attempts to address some of these shortcomings by examining the response to ECT over a follow-up period of 1 year in a relatively large sample of adolescents with either depression or BP disorder.
Methods
After obtaining the approval of the institutional review board, medical records and all available information from patients younger than 18 years of age, with a diagnosis of severe mood disorder, and who had received their first course of ECT at an academic medical center from 1996 to 2010 were examined. Refractory mood disorder was defined as the failure to respond to three or more mood-modulating medications (antidepressants and/or mood stabilizers) combined with psychotherapy. The indications for ECT for this group included a severe mood disorder, which had resulted in recurrent hospitalizations (∼4 per case in our sample), suicide attempts (∼2 per case in our sample), and/or failure to respond to past trials (average of seven failed medication trials combined with psychotherapy in the majority). The failure to elicit an adequate antidepressant response was based on information gathered from a parent or a past provider on whether the agent had not resulted in a clinically meaningful improvement, the medication was administered for a minimum of 6 weeks, the patient had been compliant with the agent, and the dosage was adequate given the patient's age. Since the adolescents were treated at a single center, the patient selection criteria for ECT and the procedures used during ECT and other treatment variables remained broadly consistent over the years and across cases.
Treatments administered were consistent with recommendations of the American Academy of Child and Adolescent Psychiatry (AACAP) practice parameters (Ghaziuddin et al. 2004). These included consensus for ECT reached by three child psychiatrists (this is based on Michigan state law; rules vary by state), a written informed consent completed by a parent/legal guardian, assent of the patient obtained whenever possible (unless illness severity precluded it), and a general medical evaluation. The following laboratory tests were completed: electrocardiogram, complete blood count with a differential count, comprehensive metabolic profile, thyroid function tests, serum pregnancy test, and magnetic resonance imaging of the brain. History of failure to respond to past medication trials was established at the time of determining the appropriateness of ECT, when the treating psychiatrist also verified the past history of the treatment described above.
Additional assessments were completed by anesthesiology and neuropsychology (unless the patient was too ill to participate in a meaningful way). Target symptoms were identified, and standardized scales were completed at baseline and subsequently at follow-up, including the Clinical Global Impressions (CGI) Scale (Guy 1976), the Children's Depression Rating Scale-Revised [CDRS-R; Poznanski et al. (1984)], and the Hamilton Rating Scale for Depression [HRSD; Hamilton (1960)]. Psychotropic medications were discontinued in the majority of cases if there was potential for interference with ECT: antiepileptic mood stabilizers because of concern for raising the seizure threshold; antidepressants because of lack of response and concern for lowering the seizure threshold; and trazodone for lowering the seizure threshold (Curran 1995). Patients fasted overnight before each treatment, and skilled nursing care was provided during the course of the treatment.
Treatment was administered using the MECTA (MECTA Co., Taulatin, OR) or the Thymatron® device. Treatment was initiated using the lowest available electrical charge (12 mC) on the ECT device, and additional 1–3 stimulations were used during the first treatment, if necessary, to identify the seizure threshold. The charge corresponding with the seizure threshold was raised at the next treatment (doubled if using bilateral electrode placement or increased 5- to 7-fold for unilateral placement) and future increases in the electrical charge were based on seizure duration. This method for determining the seizure threshold and subsequent increases in the charge is based on experience in adult patients (van Waarde et al. 2013). Treatment was initiated in the majority using bilateral placement based on the AACAP practice parameters for the use of ECT in adolescents, which suggest this mode in patients who are severely ill (refusal to eat or drink, severe suicidality, florid psychosis, or catatonia) (Ghaziuddin et al. 2004). Medications used for anesthesia and muscle relaxation included methohexital sodium (1 mg/kg) and succinylcholine (0.8 mg/kg). Glycopyrrolate (0.5 mg) was administered to reduce salivary and bronchial secretions and for its cardioprotective effect (Kellner and Bryson 2013); all dosages were calculated based on the weight of the individual. Flumazenil, a benzodiazepine receptor-blocking agent, was administered (0.5–1 mg) to cases receiving a benzodiazepine (Krystal et al. 1998).
The index course of treatment involved administration of ECT three times per week. In some cases, however, maintenance ECT was administered after the index course. This was defined as ECT given at a reduced frequency (1–2 times per week).
The primary outcome measure following ECT was the CGI Scale, which was based on information gathered from the patient and a parent about his/her depressive symptoms. The CGI score was computed independently by two nonblinded clinicians (using all information available in the chart) who assigned a final consensus score. Treatment response was defined as a CGI score of 1–2, while remission was defined as a CGI score = 1. CDRS-R and the HRSD are reported where available, but the CGI Scale was chosen over these instruments due to missing data and lack of reliability training for staff who had completed the depression questionnaires. An additional advantage of the CGI Scale is that it retains high construct and face validity in retrospective trials (Huber et al. 2011). CDRS-R was available for 40 cases at pre-ECT baseline, 17 at post-ECT, 7 at 3 months, 1 at 6 months, and for none at the 12-month assessment, while HRSD was available for 25 cases at pre-ECT baseline, 22 cases at post-ECT, 13 at 3 months, 6 at 6 months, and 1 at 12 months. Assessment of suicidality included self-injurious behavior (SIB) or SI. These items were recorded separately and were rated as present if reported by the parent or the child and were significant enough to cause concern. Getting along with family and friends was defined as positive when the majority of the interactions were reported as being desirable by the parent and the child. School attendance was assessed using parental report and was defined as the child being able to attend school on most days and/or being able to comply with a modified schedule if any.
Psychotropic agents were introduced on completion of the index course of ECT. Agents were selected on a case-by-case basis, using past trials (such as introducing an agent perceived to be more effective in the past or an agent that was previously not tried), or to target prominent residual symptoms (mood stabilizers such as lithium in cases with marked mood lability and/or SI; antipsychotic agents in cases with prominent impulsivity). In each case, the medications were adjusted during the 1-year follow-up. At the time of transition of care to the referring provider, medication compliance was emphasized as an important treatment component that could prevent relapse. All patients were urged to remain engaged in psychotherapy throughout treatment and upon completion of the ECT.
Information was collected on paper records and then entered into SPSS (Statistical Package for the Social Sciences; IBM). The demographic features and the outcome were examined for the entire group treated with ECT, with frequency presented for categorical variables and mean ± standard deviation (SD) for continuous variables. Between-group comparisons were computed for cases with UP or BP disorders using an independent-sample t-test, chi-square (χ 2), or Fisher's exact test (FET). For clinical outcomes, analyses were conducted twice for each outcome; first, using observed cases (OC), and a second time, using the last observation carried forward (LOCF) for those who were lost to follow-up. Generalizing estimating equation (GEE) models were conducted to examine change in SIB, SI, and school attendance over time. Whenever the model was significant, post hoc analyses were conducted to compare each time point post-ECT with pre-ECT. p-Values <0.05 were considered as statistically significant; however, for the GEE models performed for the four outcomes (SI, SIB, school attendance, and Mini-Mental State Examination [MMSE]), the analysis was adjusted for multiple comparisons and a p-value <0.0125 (i.e., 0.05/4 = 0.0125) was considered to be significant.
Results
Characteristics of the group are presented in Table 1. Age of first psychiatric contact was 11.2 ± 3.6 years. The group scored in the severely impaired range based on the global assessment of functioning score (mean = 22.4, SD = 9.6). Suicide attempts were relatively common in this sample (mean number = 2.0, SD = 2.2). Fourteen (25%) participants had made at least one suicide attempt in the year before receiving ECT.
Demographic and Clinical Features of Cases Treated with Electroconvulsive Therapy
ECT, electroconvulsive therapy; GAF, global assessment of functioning; HRSD, Hamilton Rating Scale for Depression; MDD, major depressive disorder; mood disorder NOS, mood disorder not otherwise specified; NSSRI, non-serotonin reuptake antidepressant; SSRI, selective serotonin reuptake inhibitor; SD, standard deviation.
The mean number of past, unsuccessful, antidepressant medication trials was 4 (SD = 1.8), while the mean number of psychotropic medication trials, which included antidepressants, antipsychotic agents, and mood stabilizers, was 7 (SD = 3.2). Failure to respond to a medication was determined using duration (>6 weeks) and evidence of compliance confirmed using parental, patient, and provider reports. Most of the patients received psychotherapy (n = 49 [91%]); however, details about the type of psychotherapy were not clear (cognitive behavior therapy = 5, supportive therapy = 5, and undetermined type = 39). The duration of psychotherapy, known in 22 cases, ranged from 4 to 468 weeks with a median duration of 57.5 weeks (∼1 year), with 21 among the 22 cases receiving the treatment for at least 11 weeks.
Comparison of the participants with BP or UP disorder found that cases with a BP diagnosis were relatively younger at their initial contact with psychiatric services (9.9 ± 3.2 years BP vs. 11.9 ± 3.7 years UP; t = 2.7, p < 0.00); had a history of more frequent psychiatric hospitalizations (5.1 ± 2.7 vs. 3.2 ± 1.7; t = 3.9, p < 0.00); and had a higher, but not statistically significant, number of relatives who had attempted suicide (n = 8 [47%] vs. n = 7 [21%] χ 2 [1, n = 50] = 0.2, p = ns). There was no statistically significant difference between BP and UP for completed suicide among relatives (n = 4 [24%] vs. n = 10 [30%] χ 2 [1, n = 50] = 0.5, p = ns).
Comorbid Axis I disorders (nonmood diagnoses) were present in the majority of patients, with only one case having no comorbid diagnosis (Table 2). Anxiety disorders were the commonest comorbid diagnoses present in 32 (59%) patients.
Comorbid Axis 2 Disorders in Mood Disorder Cases Treated with Electroconvulsive Therapy
Anxiety disorder: GAD, panic, phobia, OCD, PTSD, or anxiety disorder NOS.
Psychotic disorders: schizophrenia, schizoaffective disease, psychosis NOS, or psychotic symptoms.
Eating disorder: anorexia nervosa, bulimia nervosa, or eating disease NOS.
Substance abuse: alcohol and/or substance abuse.
ADHD, attention-deficit/hyperactivity disorder; CD, conduct disorder; CNS, central nervous system; GAD, generalized anxiety disorder; GI, gastro-intestinal; OCD, obsessive compulsive disorder; ODD, oppositional defiant disorder; PTSD, post traumatic stress disorder.
ECT treatment variables, vital signs, and side effects
The mean number of treatments received during an index ECT course was 13.7 (SD 6.3). Continuation or maintenance ECT was administered to 22 (41%) patients. Highest recorded vital signs during the treatment were as follows: mean systolic blood pressure 157.1 (SD 22.3); mean diastolic blood pressure 90.5 (SD 13.2); and mean heart rate 137.4 (SD 26.8). The mean number of prolonged electroencephalograph (EEG) seizures (>2 minutes) per subject was 4.1 (SD 2.6), noted in the majority of cases (74%). Headache was the most common side effect. All side effects, including headache, fatigue, subjective memory loss, and confusion (Table 3), were limited to the day of the treatment and were managed conservatively (recovery in a quiet room; reduced schedule on the day of treatment; and medications given for pain, nausea, or dehydration). See Table 3 for details about the electrical charge used, pulse width, motor and EEG seizure durations, and side effects.
Electrical Parameters, Hemodynamic Variables, and Side Effects Following Electroconvulsive Therapy in Mood-Disordered Adolescents
Defined as seizure duration >2 minutes.
ECT, electroconvulsive therapy; BP, blood pressure; SD, standard deviation; EEG, electroencephalograph.
Outcome
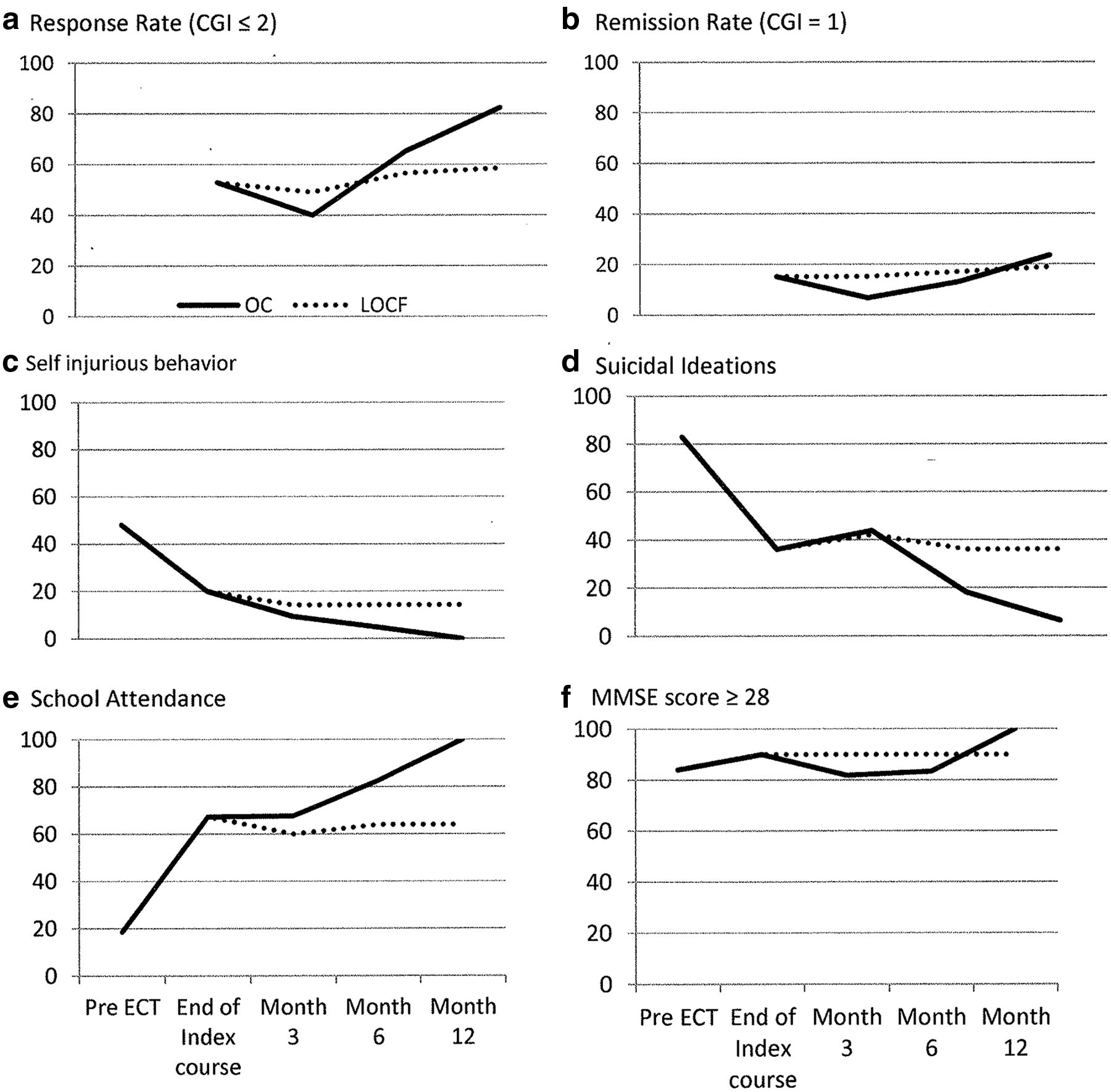
A positive treatment response (CGI score = 1, 2) was noted in 28/53 cases at the end of the index treatment (OC response rate = 52.8%); in 12/30 cases at 3 months (OC response rate = 40.0% and LOCF rate for the 53 cases = 49.1%); in 15/23 cases at 6 months (OC response rate = 65.2%; LOCF rate for the 53 cases = 56.5%); and in 14/17 cases at 12 months (OC rate = 82.4%; LOCF rate for the 53 cases = 58.5%; Fig. 1a).
Percentage of patients with
On the other hand, remission, defined as CGI score = 1, was observed in 8/53 cases at the end of the index treatment (OC remission rate = 15.1%); in 2/30 cases at 3 months (OC remission rate = 6.7%; LOCF rate for the 53 cases = 15.1%); in 3/31 case at 6 months (OC remission rate = 13.0%; LOCF rate for the 53 cases = 17.0%); and in 4/17 cases at 12 months (OC remission rate = 23.5%; LOCF rate for the 53 cases = 18.9%; Fig. 1b).
Using paired t-tests, the pre-ECT CDRS-R declined significantly from 70.7 ± 16.4 at baseline to 52.5 ± 18 post-ECT (t = 6.8, df = 13, p ≤ 0.00) at the end of the index course, while Hamilton Depression Rating Scale declined from 21.6 ± 5.9 pre-ECT to 8.5 ± 7.0 post-ECT (t = 5.3 df = 9, p < 0.001) at the end of the index course. We did not identify any clear statistical advantage of continuation and/or maintenance ECT over those who had only received an index course.
There was no difference in response or remission rates between UP and BP groups immediately on completion of the index ECT course (χ 2 = 0.30, p-value = 0.58), at 3 months (χ 2 = 0.10, p-value = 0.75), 6 months (FET, p-value = 1.00), or 12 months postcompletion of ECT (FET, p-value = 1.00). Sensitivity analysis was repeated using LOCF, but with no change in findings.
Using the GEE model, SI reduced significantly (Fig. 1d) over the course of observation (p < 0.01 for both OC and LOCF models), with each time point after ECT being significantly lower than pre-ECT in both OC and LOCF models. Similarly, SIB was found to significantly decrease over time (p < 0.01 for both models; Fig. 1c). In the OC model, compared with the pre-ECT rate of SIB, the rate was significantly lower at each time point post-ECT except at the 12-month interval, which was lower, but not statistically significant (p = 0.99). However, in LOCF, all time points were found to have significantly lower rates than pre-ECT.
Similarly, the ability to attend school increased significantly after treatment (p < 0.01 for both OC and LOCF models; post hoc analysis was similar to that of the SIB). School attendance at pre-ECT was at 18% compared with 67.3% at completion of index ECT; 67.7% at 3 months post-ECT (LOCF = 60.0%), 82.6% at 6 months post-ECT (LOCF rate = 64%), and 100% at 12 months post-ECT (LOCF rate = 64%) (Fig. 1e).
It was not possible to compare the number of hospitalizations at pre-ECT versus post-ECT or the number of visits to the ED because time spans for these variables were different; pre-ECT numbers included lifetime events, while post-ECT numbers were cumulative events following the completion of ECT. Additionally, psychiatric hospitalization or visits to the psychiatric emergency department were infrequent events; therefore, meaningful comparisons were not possible.
Medications administered
In keeping with the clinical practice at our institution, psychotropic medications were only started when the frequency of ECT was titrated down to one or two treatments per week. The medications received by participants following ECT included SSRI or non-SSRI antidepressants among 34/49 (69%), antipsychotic agents among 20/49 (41%), and mood stabilizers among 16/49 (32%) participants. Lithium was prescribed to 9 of 16 participants who were receiving a mood stabilizer, while benzodiazepines were administered to 12. The commonest medication combination received included an antidepressant and trazodone (the latter to help with sleep). More than one-half of the participants were not receiving an antipsychotic agent at the time of the post-ECT evaluation, whereas 41 among 54 participants (81%) were receiving an antipsychotic agent before ECT.
Side effects associated with ECT
Minor side effects were frequently experienced on the day of the treatment with headache being the commonest side effect. This was followed by subjective report of memory loss and fatigue. See Table 3 for details of side effects and Figure 1f for MMSE, which was used as a measure of cognition.
Discussion
The findings of the present study suggest that ECT can be a useful option in treatment-refractory adolescents with severe mood disorders. At the end of the index treatment and approximately 4 weeks after the treatment was initiated, 52.8% of the patients showed a positive response and 15% achieved remission based on CGI scores, which were used for the assessment of depressive symptoms. These rates further increased to 65% response and 13% remission, respectively, at 6 months and to 82.4% response and 23.5% remission, respectively, at 12 months following the completion of the index course. Besides a decrease in SI and SIB, an increase in participation in normal activities such as returning to school and an improvement in the ability to get along with family and friends were noted. At 1-year follow-up, the response was sustained in the overall level of functioning, notably in suicidal behavior. On balance, therefore, our findings suggest that ECT could be considered as a viable treatment option, perhaps earlier in the treatment course to prevent morbidity, rather than as a treatment of last resort. When considering this option, clinicians should remain cognizant of the well-documented, severe adverse outcomes associated with untreated, adolescent mood disorders (Bardone et al. 1998; Kim-Cohen et al. 2003; Ferguson et al. 2005, Copeland et al. 2009).
Although the treatment response was generally positive in the present study, it is worth noting that the initial response and remission rates (at the end of the index course) were relatively modest. However, these rates increased progressively at 6 and at 12 months' follow-up, underscoring the progressive and the sustained nature of the positive outcome in a highly treatment-refractory group with a history of failure to respond to seven previous mood-modulating trials along with psychotherapy. The lower initial response rates found in our sample are not consistent with the findings of some of the recent publications about the use of ECT in adolescents (Zhang et al. 2012; Lima et al. 2013; Puffer et al. 2016). The reasons for these lower initial rates of improvement are not entirely clear, but may include the effect of higher treatment resistance and the delayed use of ECT (as suggested by an average of seven failed trials in our group). Furthermore, age-related diagnostic differences could be another factor such as the likelihood of underdiagnosis of the BP disorder because severe mood disorders during adolescence are more likely to be a BP illness than UP illness (Chilakmarri et al. 2011), which are also associated with greater chronicity and comorbidity (Perlis et al. 2004). Comorbidity due to cluster B personality traits could have also contributed to the lower response rate, but this was difficult to assess and control for based on a chart review. Between-study diagnostic differences may be a factor as well; the present study has exclusively studied mood-disordered adolescents, while the 77% initial response reported by Puffer et al. (2016) involved a diagnostically mixed sample and the 74% initial response reported by Zhang et al. (2012) was derived from a sample of adolescents with first-episode psychosis.
The young age of the sample raises the possibility that ECT might be less effective in adolescents compared with adults. However, existing literature does not support this hypothesis. ECT has been found to be effective across the age span, with the greatest benefit likely over the age of 65 years in patients with UP depression (O'Connor et al. 2001). However, there is sparse literature involving adolescents, and a hypothetical negative effect of young age is not supported by studies involving this age group. Despite the limitations of this literature, which includes studies with a relatively small number of subjects, reviews of the existing publications, diagnostic differences, and inconsistent methods used for assessing outcome, positive response, and remission rates overall have been reported (Bertagnoli and Borchardt 1990; Rey and Walter 1997; Zhang et al. 2012; Lima et al. 2013; Puffer et al. 2016). However, other effects of age such as a slower speed of response or the need for a greater number of treatments should be examined systematically in future studies.
Regarding the benefit of receiving a longer course of ECT, we did not identify a clear statistical advantage of continuous or maintenance ECT over an index course alone. This finding is inconsistent with the published literature (Odeberg et al. 2008) and also does not support our earlier publication involving a small number of severely refractory cases, where five of the six cases had achieved premorbid functioning as a result of continuation or maintenance treatment (Ghaziuddin et al. 2011). The lack of benefit in the current study may be due to the progressive loss of cases (even though we attempted to provide close follow-up for approximately a year after completion of the treatment) or due to a relatively short follow-up period.
Side effects of ECT in the present study were minor and limited to the day of the treatment. These mainly consisted of severe headache and prolonged seizures. The former is well documented as a side effect of ECT and can result from several factors. Regarding prolonged seizures, the most likely reason is the well-recognized, lower seizure threshold in younger patients (Boylan et al. 2007; Rasimas et al. 2007; Pettrides et al. 2009). This finding has also been consistently reported in other studies in adolescents. The initial setting of the electrical protocol is an unlikely factor as it was always selected at the lowest available setting in the ECT device with subsequent total charge increases (increased by 100% if using bilateral placement or a 5- to 7-fold increase if using unilateral placement); however, this titration was based on adult data and warrants further examination in adolescents. Regarding the impairment of memory, comparison of pre- and post-ECT MMSE scores did not reveal any significant differences. Due to lack of access to neuropsychological evaluations, we could only present the scores of the MMSE (Folstein et al. 1975; Pangman et al. 2000), which were available for 22 participants post-ECT. However, standardized cognitive assessment is essential and should include comparison of pre- and post-treatment cognitive measures. Our finding using the MMSE is consistent with a relatively small, but compelling, body of literature, which suggests that memory deficits in adolescents treated with ECT resemble those noted in adults. Additionally, findings have supported that adolescents do not experience lasting neurocognitive deficits when pre- and post-ECT outcomes are compared (Ghaziuddin et al. 1996, 2000). Furthermore, ECT-treated adolescents have been found not to significantly differ in their cognitive functions from other psychiatric controls (Cohen et al. 2000).
Taken together, our findings replicate and extend those of earlier studies that have supported the effectiveness of ECT as a treatment in adolescents with refractory mood disorders (Bertagnoli and Borchardt 1990; Rey and Walter 1997; Zhang et al. 2012; Puffer et al. 2016). While encouraging, these findings should be considered in the context of the strengths and limitations of the present study. Limitations include the following: most of the data were extracted from chart review; diagnoses were based on Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 2000) criteria without the use of standardized instruments; and missing data involving the CDRS-R and HRSD compelled us to base the treatment outcome on the CGI Scale. While we acknowledge the limitation of using the CGI score as the main outcome measure, we should also point out that the CGI Scale (the aggression subscale) has been shown to have high construct and face validity in retrospective trials (Huber et al. 2011). Other limitations include not being able to provide details of past medication trials; possible contribution of cluster B traits to the presentation; and the effects of comorbid diagnoses, each with its unique neuro-circuitry—thus, the unknown impact of these factors on treatment response. Last, there was a progressive attrition of patients, which we attempted to account for by LOCF. Notable strengths of the study, on the other hand, are that we used standardized patient selection criteria; participants were homogeneous in their mood disorder diagnosis; all the participants received ECT at a single location using a standardized protocol; and we provided longitudinal assessment of the outcome over a year following completion of the index ECT course. These positive findings should prompt systematic, multicenter long-term studies to examine the role of ECT in the treatment of refractory mood disorders in adolescents.
Conclusion
In a sample of adolescents with severe mood disorders, at the end of an index course of electroconvulsive therapy comprising of an average 14 treatments, response and remission rates were 52.8% and 15.1%, respectively. At one year follow up, with continued treatment, the respective response and remission rates increased to 82.4% and 23.5%. In addition to the reduction in depressive symptoms, adolescents experienced a decline in self-injurious behavior and suicidal ideation and improved overall functioning as measured by school attendance. Cognitive adverse effects, as measured by the Mini Mental State Examination, were minimal. Study limitations include a lack of a control group, absence of measures of personality, and a limited sample size.
Clinical Significance
The current practice of the treatment of resistant mood disorders in adolescents includes pharmacotherapy and psychotherapy; treatment resistant is defined as the failure to respond to at least two pharmacological interventions in combination with psychotherapy when appropriate. Findings of the present study suggest that ECT can be an alternative, effective, and safe treatment for adolescents with resistant mood disorders.
Disclosures
N.G. is coeditor of the book Use of ECT in Children and Adolescents (Oxford University Press, New York, 2013). Drs. W.S., G.G., and M.G. have disclosed no conflicts of interest.