
Abstract
Objectives:
To describe the substance use profiles of youth impacted by commercial sexual exploitation (CSE) and explore associations between substance use with mental health diagnoses and child welfare involvement.
Methods:
Data were systematically extracted from the court files of 364 youth who participated between 2012 and 2016 in Los Angeles County's Succeeding Through Achievement and Resilience (STAR) Court, a juvenile delinquency specialty court for youth impacted by CSE. Descriptive statistics and multivariate regression analyses were conducted to quantify associations between youths' substance use with mental health diagnoses and child welfare involvement.
Results:
Of the 364 youth impacted by CSE involved in the STAR Court, 265 youth had documented contact with a psychiatrist while in court—of whom, 73% were diagnosed with at least one mental health challenge. Before STAR Court participation, 74% of youth were the subject of one or more child welfare referral; of these youth, 75% had prior out-of-home care. Eighty-eight percent of youth reported substance use, the most prevalent illicit substances were marijuana (87%), alcohol (54%), and methamphetamine (33%). Controlling for age and race, youth impacted by CSE with a diagnosed general mood disorder had more than five times the odds of reporting substance use compared with those without a mood disorder diagnosis (adjusted odds ratio [AOR]: 5.80; 95% confidence interval CI: 2.22–18.52; p < 0.001); and youth impacted by CSE with prior child welfare placements had more than two times the odds of reporting substance use (AOR: 2.24; 95% CI: 1.04–4.86; p = 0.039) compared with youth without prior placements. The association between substance use and general mood disorder was significant and positive for all substance use types (AOR = 3.3, p = 0.033 marijuana; AOR = 4.01, p = 0.011 concurrent alcohol and marijuana; AOR = 9.2, p < 0.001, polysubstance use).
Conclusions:
High prevalence of substance use among juvenile justice-involved youth impacted by CSE combined with strong associations between substance use with both mental health diagnoses and child welfare system history underscores the need for comprehensive, specialized substance use treatment. Findings suggest an important opportunity for multidisciplinary collaboration among mental health providers, child welfare professionals, juvenile justice practitioners, and other care providers for these youth.
Introduction
Commercial sexual exploitation (CSE), also known as sex trafficking, refers to the exchange of any sexual act for something of value, including money, shelter, goods, or acts of service (U.S. Congress 2000). CSE of minors is a form of child abuse. Following the federal passage of the Trafficking Victims Protection Act of 2000 and the subsequent adoption of state Safe Harbor legislation to codify and enhance the federal law at the state level, there has been a marked increase in the decriminalization and identification of youth experiencing CSE.
Youth experiencing CSE represent a vulnerable population. CSE disproportionately affects racial and ethnic minority youth (Phillips 2015). The public health ramifications are significant, with exploitation resulting in a myriad of health and safety consequences (Shields and Letourneau 2015; Greenbaum 2018). Youth impacted by CSE often face high rates of medical, mental health, and substance use problems as a result of their exploitation (Collins et al. 2013; Muftić and Finn 2013; Ottisova et al. 2016; Greenbaum 2018). These youth are at risk for violence-related injuries, including fractures, traumatic brain injuries, and anogenital injuries (Zimmerman et al. 2006, 2011; Muftić and Finn 2013). The combination of ongoing violence (e.g., rape), high-risk health behaviors (e.g., intravenous drug use), and limited access to health care increases the risk for youth impacted by CSE to contract infectious diseases, experience unplanned pregnancy, or develop medical complications as a result of untreated chronic illness (Zimmerman et al. 2011; Greenbaum 2018).
Exposure to violence, coercion, and unsafe living conditions, lack of social support, and high rates of prior abuse experienced by commercially sexually exploited youth compound their risk for severe mental health conditions, including mood disorders, post-traumatic stress disorder, complex trauma, substance use, self-harming behaviors, and suicide ideation (Basson et al. 2012; Cole et al. 2016). Furthermore, a history of abuse and mental health problems may affect a youth's sense of self-efficacy and judgment, increasing the risk for further victimization, negative relationships, maladaptive coping, and poor health outcomes (Basson et al. 2012). Youth impacted by CSE are often cited as having a high burden of mental health and substance use disorder treatment needs (Curtis et al. 2008; Cole et al. 2016), yet the prevalence of behavioral health conditions has not been well documented due to the challenge of finding a robust sample of youth impacted by CSE. Medical literature on the health needs of youth with histories of CSE is growing; however, little is known about the intersectionality of contributing factors from childhood and subsequent trauma resulting from CSE. One study involving a nationally representative sample of youth on prevalence and correlates of exchanging sex for drugs or money found that the odds of having exchanged sex were higher for youth with substance use histories (Edwards et al. 2006); however, that study did not measure CSE as it is defined by current law and relied exclusively on self-report measures of exchanged sex and substance use.
The adverse childhood experiences (ACEs) framework provides a lens for understanding and measuring the impact on childhood trauma on psychological and physical health outcomes, including into adulthood (Felitti et al. 1998). The ACEs framework is also widely used to understand the behavioral and health outcomes of marginalized, incarcerated, and maltreated children (Levenson et al. 2017; Rebbe et al. 2017; Clements-Nolle and Waddington 2019). ACEs and other social determinants of health are driving factors associated with entry into CSE (Naramore et al. 2017). Contributing factors for CSE that have been empirically documented include the following: familial poverty, housing insecurity, and lack of educational resources (Clarke et al. 2012); family participation in the commercial sex industry (Fedina and DeForge 2017); sexual assault and polyvictimization (Fedina and DeForge 2017; Hopper 2017); cognitive or intellectual impairment (Reid 2018); runaway behaviors (Fedina and DeForge 2017); self-identification or being perceived as a member of the lesbian, gay, bisexual, transgender, and queer community (Greenbaum 2018); experiences of child maltreatment, most significantly childhood sexual abuse (Roe-Sepowitz 2012; Reid et al. 2017; De Vries and Goggin 2018); substance use and addiction (Massey et al. 2014; Reid et al. 2015); and involvement in criminal activity and the juvenile justice system (Greenbaum 2018). These factors may lead to disrupted family bonds, social support scarcity, and developmental trauma, and exacerbate youths' risk of recruitment by peers or traffickers (Cecchet and Thoburn 2014).
Prior research has demonstrated strong associations between youth involvement in the child welfare or juvenile justice systems and negative adolescent behavioral health outcomes, including mental health conditions and substance use (Steinberg et al. 2011; Kretschmar et al. 2015; Logan-Greene et al. 2017; Clements-Nolle and Waddington 2019). For youth impacted by CSE, these associations may be even more pronounced. CSE often occurs while youth are under the legal supervision of dependency and delinquency court systems (Fong and Berger Cardoso 2010; Latzman et al. 2018). Specifically, recruitment and return to CSE commonly occur while youth are residing in child welfare residential placements, and youths' underlying vulnerability to exploitation often strongly interrelates with their histories of abuse or neglect that led to involvement in the child welfare system (CWS; Institute of Medicine and National Research Council 2013). Factors related to abuse histories are believed to intertwine with prior and resultant mental health conditions, which can exacerbate patterns of substance use, a known trigger and perpetuating factor for sexual exploitation (Institute of Medicine and National Research Council 2013). Yet, behavioral health profiles of youth impacted by CSE are largely absent from existing literature. Furthermore, few empirical studies have examined the relationship between childhood adversity, as measured by child welfare referrals, and mental health diagnoses, with the substance use outcomes of CSE (Reid and Piquero 2014; Reid et al. 2017). To address these gaps, this study (1) describes the behavioral health profiles of juvenile justice-supervised youth impacted by CSE, and (2) quantifies associations between youths' substance use with mental health diagnoses and CWS involvement.
Methods
We partnered with the Succeeding Through Achievement and Resilience (STAR) Court, an innovative diversion court program designed specifically for youth impacted by CSE in Los Angeles (LA) County. LA County has the nation's largest juvenile justice system and was identified by the Federal Bureau of Investigations as a high-intensity area for child sex trafficking (U.S. Department of Justice 2009). Since 2012, the STAR Court has provided specialized services to youth identified for their at-risk or confirmed status with CSE. The STAR Court utilizes a therapeutic, trauma-informed, multidisciplinary team approach to link youth with rehabilitative and health-related services. The voluntary program relies on interagency collaboration among LA County's Department of Probation, Public Defender's Office, Department of Children and Family Services (DCFS), Department of Public Health, Department of Mental Health (DMH), and community-based service providers.
Approach
An exhaustive review was conducted of all available court files pertaining to the youth who were served by the STAR Court between January 2012 and December 2016 (N = 364). Data contained in court files included administrative data from the Department of Probation and DCFS, school reports, mental health records from the DMH and affiliated mental health agencies, and court documents. Data were extracted from paper court files and entered into a secure electronic REDCap database in compliance with the Health Insurance Portability and Accountability Act of 1996. All research study procedures were approved by the UCLA Institutional Review Board and the LA County Superior Court.
Descriptive statistics were generated to characterize the sample using sociodemographic information, CWS involvement, mental health diagnoses, and substance use. Using percentage distributions, we explored the CWS history and out-of-home placement profiles of youth impacted by CSE, and present the mental health and substance use profiles of the sample. The purpose of the analysis was to (1) characterize the profile of youth impacted by CSE using summary statistics, (2) explore univariate associations between a dichotomous substance use variable and independent variables measuring demographic factors, mental health, and child welfare involvement, and (3) explore how the aforementioned independent variables are associated with two different substance use outcomes: any substance use and a categorical variable indicating types of substances used.
Mental health diagnoses, documented within mental health provider records, were coded using dichotomous yes or no categories that were not mutually exclusive, and included the following: depression diagnoses, sleep disorders, unspecified mood disorders, disruptive behavior disorders, traumatic stress disorders, attention-deficit/hyperactivity disorder, bipolar disorder, and anxiety diagnoses. Indicators of substance use were extracted from probation case reports and were coded as a dichotomous yes or no variable for each substance, and included the following: tobacco, marijuana, alcohol, methamphetamine, cocaine, ecstasy, or misuse of prescription drugs. We also utilized two interval variables related to CWS history before STAR Court entry: (1) number of DCFS referrals and (2) number of out-of-home placements.
Substance use, as an outcome, was explored in two different ways. First, substance use was coded dichotomously as any substance use versus no substance use (the reference group). Second, substance use was divided into four mutually exclusive categories: (1) no substance use (the reference group), (2) marijuana use only, (3) alcohol use, with or without marijuana, and (4) polysubstance use, including methamphetamine, cocaine, ecstasy, or prescription drugs, with or without alcohol or marijuana use. General mood disorder included individuals diagnosed with depression, bipolar disorder, and/or mood disorder before court entry.
Univariate logistic regressions were initially conducted to quantify associations between any substance use as the outcome and independent variables that measured mental health (i.e., sleep disorder and general mood disorder), demographic factors, and CWS involvement. Multivariable logistic regression was conducted to quantify the association between any general substance use and documented mood disorder. Multinomial logistic regression was conducted to evaluate the association between the second four-category substance use outcome variable and documented mood disorder history. For both regression models, the youths' race, age at STAR Court entry, and CWS placement history were additional covariates. A three-category variable was used to categorize race, conflating race and ethnicity (i.e., African American, Hispanic, other), with African American as the reference category. CWS history before STAR Court entry was measured using two dichotomous variables: (1) DCFS involvement and (2) out-of-home placement. Adjusted odds ratios (AORs) controlled for all other independent variables. p-Values were considered significant at the α = 0.05 level. All statistical analyses were performed in R software (R Version 3.0.0, GNU project).
Results
The sociodemographic profiles of the 364 youth impacted by CSE involved in the STAR Court between 2012 and 2016 are displayed in Table 1. Nearly all youth were cisgender female (99%), with the remaining participants identifying as cisgender male or transgender female (1%). The sample was predominantly African American (70%), while 23% were Hispanic, 5% were white, 1% was Asian, and 1% of the sample was categorized as “other.” The average age at referral to STAR Court was 16 years, with ages ranging from 12 to 19 years.
Demographic Characteristics
SD, standard deviation.
Figure 1 presents percentage distributions corresponding with CWS referrals to DCFS and placement history profiles of youth. Before STAR Court entry, 74% of the youth had been the subject of at least one child maltreatment report by DCFS. The referral counts averaged 7.5 referrals per youth, with 15% of the sample having 15 or more maltreatment reports. Among those with CWS history, 75% had been placed in out-of-home care before STAR Court entry, averaging 3.5 different placements per youth. Of the youth who had been in foster care, 30% experienced six or more unique placements. Out-of-home episodes experienced before STAR Court entry included a mix of group home (57%) and foster family home (41%) placements.
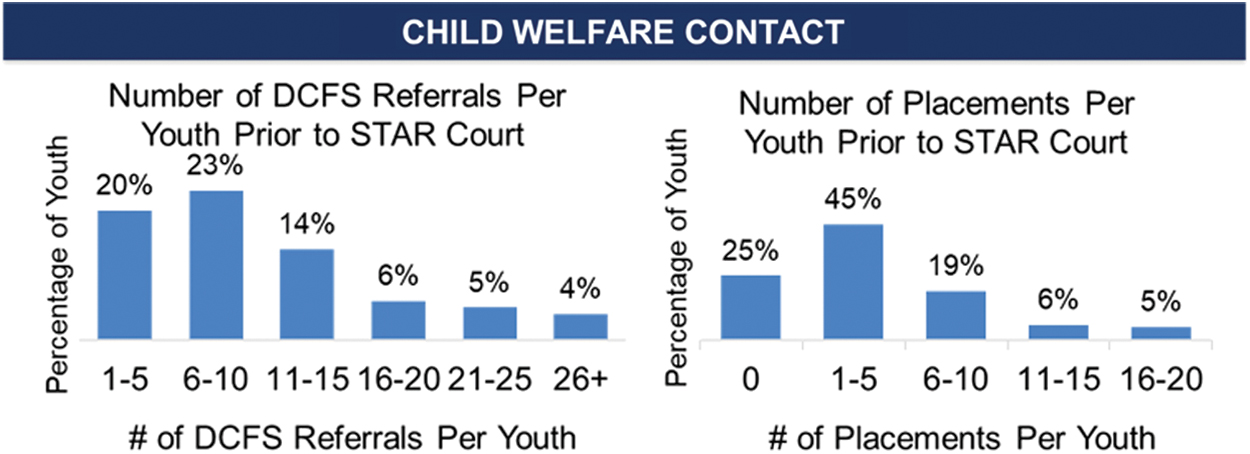
Child welfare system profiles of youth before court entry (N = 364). Color images are available online.
Figure 2 displays the percentage distribution of documented mental health diagnoses of youth (n = 265) while involved in STAR Court. Roughly three-quarters of the sample had a documented mental health condition (72.8%) upon entering STAR Court, a majority of whom had more than one documented diagnosis (88%). Before STAR Court, more than one-third of the sample had a psychiatric hospitalization (34%), and 16% had at least one documented suicide attempt.
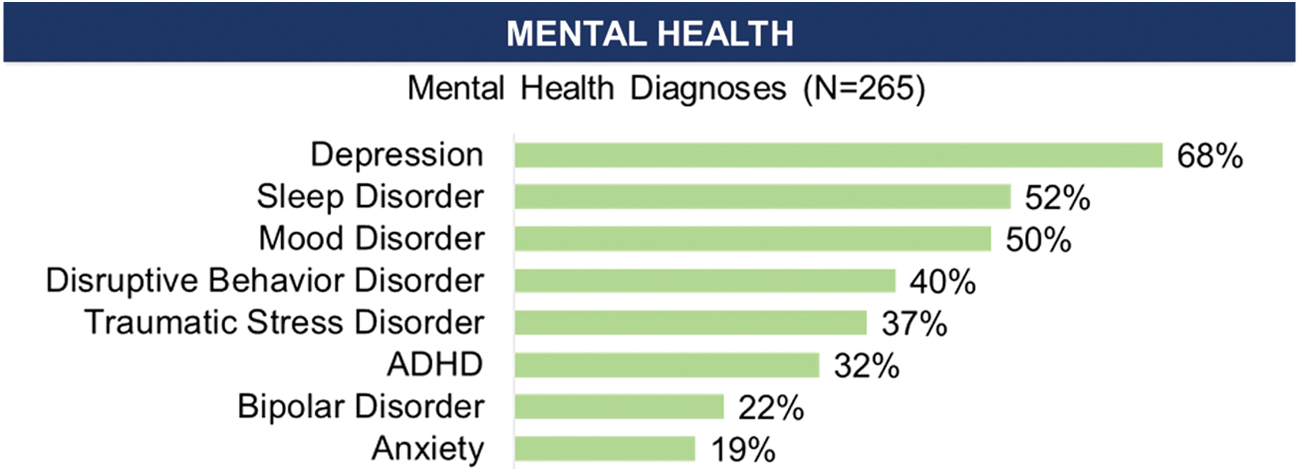
Mental health profiles of youth (n = 265). Color images are available online.
Figure 3 displays the percentage distribution of substance use profiles of all youth (N = 364) during STAR Court involvement. Eighty-eight percent of the youth self-reported substance use, the majority of whom described polysubstance use. The most commonly reported substances were marijuana (87%), alcohol (54%), and methamphetamine (33%). With regard to the classification of types of substances use, 23.1% were classified as having used marijuana only; 23.1% had consumed alcohol (with or without marijuana), but no other substances; and 41.5% had indicators of polysubstance use, which included methamphetamines, cocaine, ecstasy, or misuse of prescription drugs, as well as marijuana or alcohol use. The average age of self-reported first use was 12.8 years for marijuana, 13.5 years for alcohol, and 13.6 years for methamphetamine. While participating in the STAR Court, 40% of youth received substance abuse treatment.
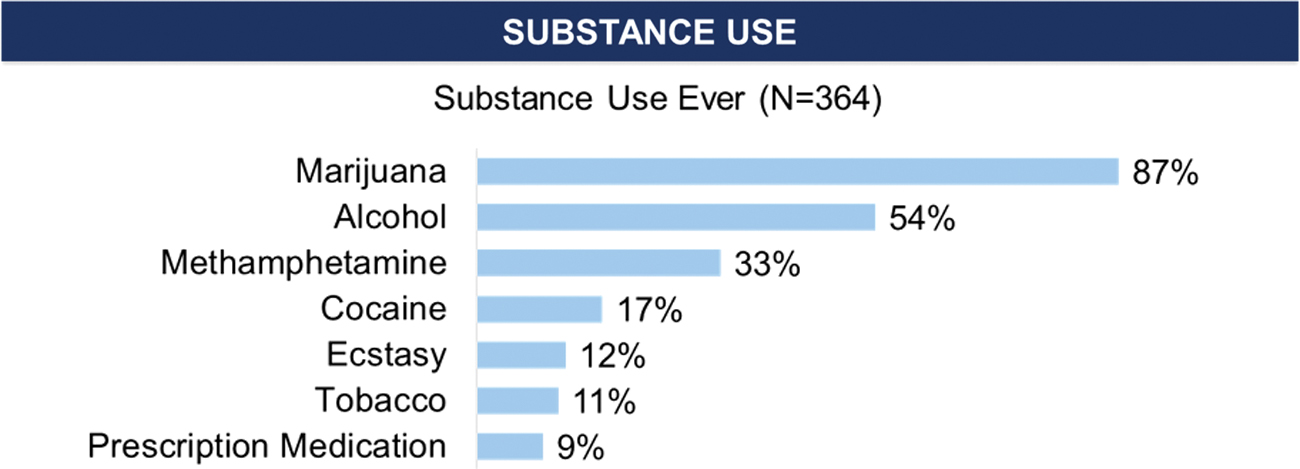
Substance use profiles of youth (N = 364). Color images are available online.
Mental health indicators and substance use
Table 2 presents our logistic regression findings. A univariate regression analysis revealed that the odds of reporting any substance use were significantly higher for those with general mood disorder compared with those without (UOR: 9.04; 95% confidence interval [CI]: 3.73–27.02; p < 0.001). The same was also found to be true for youth with a documented sleep disorder when compared with youth who had no known sleep disorder (unadjusted odds ratio [UOR]: 9.36; 95% CI: 1.97–167.80; p = 0.029). Controlling for sociodemographic factors and CWS contact, a multivariate regression found that youth with a documented general mood disorder had more than five times the odds of reporting any substance use compared with those without (AOR: 5.80; 95% CI: 2.22–18.52; p < 0.001).
Multivariable Logistic Regression Models Showing Relationship Between Substance Use with Mental Health Diagnoses and History of Child Welfare System Involvement Among Youth (N = 364)
General mood disorder includes depression, mood disorder, and bipolar disorder.
DCFS, Department of Child and Family Services; UOR, unadjusted odds ratio; AOR, adjusted odds ratio; CI, confidence interval; STAR, Succeeding Through Achievement and Resilience.
Results from the multinomial logistic regression analysis are presented in Table 3. After controlling for confounders, the estimated odds of marijuana use among youth with a documented mood disorder before court were 3.3 times higher compared with youth without a history of mood disorder (AOR: 3.31; 95% CI: 1.10–9.95; p = 0.033). The estimated odds of alcohol consumption, with or without marijuana use, were 4.1 times higher among youth with a documented mood disorder compared with those without any known mood disorder history, controlling for all other covariates (AOR: 4.13; 95% CI: 1.38–12.39; p = 0.011). Finally, the estimated odds of polysubstance use among those with a mood disorder were 9.2 times that than those without any documented mood disorder, after controlling for all other covariates (AOR: 9.21; 95% CI: 3.20–26.8; p < 0.001). The odds of substance use were not significantly different for youth with or without known suicidality before STAR Court across any of the three substance use categories after controlling for all other covariates.
Multinomial Logistic Regression Models Showing Relationship Between Different Types of Substance Use with Mental Health Diagnoses and History of Child Welfare System Involvement Among Commercially Sexually Exploited Youth (N = 364)
Bold p-values indicate significance.
AOR, adjusted odds ratio; CI, confidence interval; STAR, Succeeding Through Achievement and Resilience.
Child welfare placement and substance use
CWS referrals and placement history before STAR Court entry were associated with higher odds of substance use (Table 2). For every additional placement, the unadjusted odds of substance use was 1.13 times higher (UOR: 1.13; 95% CI: 1.02–1.27; p < 0.001) Controlling for sociodemographic and mental health factors, commercially sexually exploited youth with CWS placements before STAR Court entry had more than twice the odds of reporting substance use (AOR: 2.24; 95% CI:1.04–4.86; p = 0.039), compared with youth without placements before STAR Court. Specifically, youth with a history of CWS out-of-home placement before STAR Court had higher estimated adjusted odds of alcohol consumption with or without marijuana use (AOR: 4.32; 95% CI: 1.62–11.53). Placement history was not significantly associated with any other substance-type usage (Table 3).
Demographic indicators and substance use
As shown in Table 2, there were no age or race effects on the odds of any substance use before or after controlling for all other variables. Age at STAR Court entry did not appear to affect substance use in any of the categories after controlling for all other covariates. However, significant differences in polysubstance use were found by race/ethnicity in the multinomial logistic regression model. Compared with African American youth in the sample, the odds of polysubstance use were 3.4 times higher among Hispanic youth, after controlling for age at STAR Court entry, a history of mood disorder, suicidality before STAR Court, and child welfare placement history (AOR: 3.43; 95% CI: 1.03–11.49; p = 0.045). The effect of race was not found for the other substance use categories (Table 3).
Discussion
This study contributes to the growing literature on the behavioral health and substance use profiles of youth impacted by CSE in the juvenile justice system. Consistent with prior research, our study demonstrated a high burden of mental health disorders and significant substance use among youth impacted by CSE (Curtis et al. 2008; Cole et al. 2016). The study also quantified the relationship between prior CWS involvement and youth with histories of CSE, a well-documented risk factor for victimization (Institute of Medicine and National Research Council 2013). Youth impacted by CSE are often subjected to all forms of child maltreatment, including physical, sexual, and emotional abuse and neglect—all of which can directly increase substance use risk and can lead to contact with the CWS, which in turn can also increase substance use risk. A conflagration of risks—mental health diagnoses, CWS involvement, and CSE itself—strongly intersect with substance use and have important implications for substance use prevention and treatment among youth impacted by exploitation.
Recognizing the high burden of substance use among sexually exploited youth
Clinicians should be aware that substance use is common and often severe among youth impacted by CSE, including for youth who present at young ages. The overwhelming majority of youth in our sample had used at least one substance, and about two-fifths used three or more substances (43%). The substance use rates among the youth impacted by CSE were much higher than the general youth population; in 2012, 45% of U.S. high-school youth reported using marijuana (Partnership for a Drug Free America 2013), compared with 88% of youth in our sample. However, the observed high prevalence of polysubstance use aligns with rates observed among CWS-involved youth documented in the 2016 National Study of Child and Adolescent Well-Being (Yarnell et al. 2016). This finding suggests that screening approaches and thresholds adopted for the broader population of CWS-involved youth may be directly applicable to youth impacted by CSE. Yet, despite the high levels of substance use among our sample, the prevalence of substance use treatment was only 40%, underscoring the gap between treatment need and treatment receipt among youth impacted by CSE (Yonek et al. 2019). Accordingly, increasing linkages to substance use prevention and treatment services and interagency collaboration among systems of care are essential to facilitating access to needed services for youth impacted by CSE (Howell et al. 2004; Chuang and Wells 2010). Finally, the age of onset of substance use for our populations was relatively early, with most youth initiating use of marijuana, alcohol, and methamphetamine between ages 12 and 14, suggesting that early substance use prevention efforts for youth are warranted.
Predicting risk for substance use
In examining risk for substance use among youth impacted by CSE, we observed that both mood disorder diagnosis and CWS involvement were strongly associated with substance use. In particular, our finding that three-quarters of youth had both child welfare service involvement and that child welfare placement doubles the odds of substance use underscores the intersection between substance use and child welfare. It is well established that mood disorders co-occur with substance use and that youth with CWS involvement are at higher risk for substance use issues. In addition, placement instability is especially associated with increased risky behaviors and negative outcomes. Presence of mood disorder and CWS placement history may indicate a hallmark of substance use risk that warrants further exploration by clinicians and researchers. Furthermore, although our findings do not provide information on causality, our study suggests that substance use prevention and treatment interventions for youth impacted by CSE need to address the high likelihood of comorbidity of mood disorder as well as likely prior childhood abuse or neglect and placement instability (Ford et al. 2010). Unraveling the underlying mechanisms for the associations between CWS involvement, mental health disorders, and substance use treatment need among youth impacted by CSE may lend insight into optimal clinical approaches. It is critical that providers become attuned to the interrelationship between CSE victimization, unresolved trauma (often largely related to child abuse and prior child welfare involvement), and substance use to authentically meet youths' treatment needs.
Culturally attuned interventions
Study findings demonstrate differences in substance use rates and usage patterns among justice-involved Hispanic youth, compared with their African American counterparts (Teplin et al. 2002). The observed higher odds of polysubstance use among Hispanic youth impacted by CSE suggest that the pathway for substance use disorder development in Hispanic youth, compared with African American youth, may be different. As such, culturally tailored approaches to substance use prevention and treatment services that account for race and ethnicity may increase the benefits of these interventions (Gil et al. 2004).
Need for substance use screening
The observed high prevalence and severity of substance use among youth impacted by CSE and the interrelationship between prior CWS placements indicate a high-yield opportunity for screening for substance use treatment need. Screening for substance use problems is the critical first step in the sequential “behavioral health services cascade of care” model for justice-involved youth, which is a framework for examining how justice-involved youth transition through systems of care and identifying gaps across critical transition points (Belenko et al. 2017). Systematic and ongoing screening for substance use and co-occurring mental health disorders can reduce the unmet substance use treatment need among youth impacted by exploitation and may facilitate prevention. Implementing periodic, brief screening tools that are empirically validated, such as the Screening Brief Intervention Referral Treatment (Agerwala and McCance-Katz 2012; Cook et al. 2018) model and the National Institute on Alcohol Abuse and Alcoholism Youth Alcohol Screen (NIAAA), in juvenile justice and CWS may signify a dramatic step toward identifying substance use treatment need, an important aspect in improving outcomes.
Treatment considerations
While concerns for the immediate safety of youth may prompt service providers to focus interventions on cessation of involvement in CSE, the current findings provide preliminary evidence that experiences of maltreatment and displacement influence substance use behaviors among youth impacted by CSE. Prioritizing delivery of substance use prevention and treatment services is key, ideally through a process that recognizes and addresses the interrelated factors and traumas contributing to substance use risk. Prior research indicates that when delivering treatment services, youth or with histories of CSE or current experience of CSE need to be approached with respect, rather than blame or judgment (Ijadi-Maghsoodi et al. 2018). Providers will need to work closely with youth impacted by CSE to ensure treatment “buy-in” or engagement so that substance use treatment compliance is enhanced (Barnert et al. 2019). By adapting these clinical approaches when treating youths' substance use treatment needs, providers can take an important step toward improving substance use outcomes among youth impacted by CSE.
Limitations
These findings represent juvenile justice-involved youth impacted by CSE in LA County participating in a specialty court for youth at-risk of or with confirmed histories of CSE, rather than the traditional court system. Thus, our findings are not representative of all judicially involved youth with histories of CSE in the area, as it is estimated that only three-quarters of eligible youth opt-in to the diversion program. Furthermore, our sample was almost exclusively cisgender females, despite evidence that CSE impacts boys and transgender youth as well (Curtis et al. 2008; Reid et al. 2015). Thus, results may not be generalizable across different regions in the United States or for youth impacted by CSE overall, due to participant demographics. An additional limitation was our reliance on administrative data (i.e., court records) in the paper case files. Specifically, substance use history was reliant on probation records in combination with self-report data, and did not capture information about frequency of usage (i.e., rare, occasional, or chronic use). Despite these limitations, this analysis offers insight into the psychosocial experiences and behavioral patterns of an understudied subpopulation of youth, often challenging to identify.
Conclusions
In sum, collaboration and communication between psychiatric clinicians and other behavioral and primary health care providers who deliver care that is trauma informed, culturally informed, and that recognizes the multiple factors contributing to substance use among youth impacted by CSE are necessary. Structural changes at the systems level to implement screening for substance use and mental health disorders in the child welfare and juvenile justice systems signify a promising approach and are essential for coordinating services across multiple providers and their respective agencies. Additional attention is needed to develop and implement evidence-based interventions tailored to the unique needs of youth experiencing CSE, accounting for their racial/ethnic backgrounds and the impact of prior system involvement. Attention to substance use prevention and treatment needs among youth impacted by CSE should be a priority focus for juvenile justice and child welfare agencies, as well as health providers.
Clinical Significance
Within the juvenile justice and CWSs, youth impacted by CSE often present with a wide range of risk factors and behavioral health needs that, unaddressed, may sustain or heighten their vulnerability to ongoing system involvement and exploitation. Clinicians seeking to have maximal impact in serving youth impacted by CSE should be aware of these interrelated risks and treatment needs. The current article highlights this critical service gap and underscores the importance of conducting brief, routine screenings to identify psychiatric and substance use treatment needs with this population.
Footnotes
Acknowledgments
We thank Judge Catherine Pratt and the Los Angeles County STAR Court for their partnership. We also thank the participating youth and partner agencies, including Amber Davies of Saving Innocence and Michelle Guymon of the Los Angeles County Department of Probation Child Trafficking Unit.
Disclosures
All authors, including Dr. E.B., reports no biomedical financial interests or potential conflicts of interest. All authors report no financial relationships with any of the pharmaceutical companies.