
Abstract

Use of melatonin in the pediatric population for treatment of insomnia is increasing. There are multiple formulations available and no clear recommendations for dosing or administration. Typical dosing ranges from 0.5 to 10 mg 30–60 minutes before the desired bedtime (Gringras et al. 2017). Limited data exist on adverse effects and toxicology in this population. Reported cardiovascular effects of melatonin include reductions in arterial blood pressure and plasma noradrenaline levels while standing (Ray 2003).
This case highlights unexpected severe delayed hypotension in an adolescent after a suspected melatonin overdose.
A 16-year-old girl with unspecified depressive, anxiety, and attention-deficit/hyperactivity disorders, and asthma was transferred to our university hospital after ingesting twenty 9 mg (180 mg) melatonin tablets. On arrival, the patient was lethargic with Glasgow Coma Scale of 15. Vital signs were blood pressure 126/99 mmHg, pulse 82 beats/min, respiratory rate 14 breaths/min, and pulse oximetry was 100% on room air. Laboratory results were unremarkable, except for mild leukocytosis (11.7 k/μL). Electrocardiogram showed normal sinus rhythm and QTc-interval.
In addition to melatonin, the patient reported ingesting her prescribed fluoxetine 40 mg and hydroxyzine 50 mg and twice her prescribed daily dose of guanfacine immediate-release (4 mg total) and methylphenidate extended-release (72 mg total) 17 hours before arrival. However, urine drug screen showed only fluoxetine, diphenhydramine, dextromethorphan/dextrorphan, hydroxyzine/cetirizine metabolite, and trimethoprim.
Upon arrival to the behavioral health unit (hospital day 2), patient was drowsy, minimally responsive, and complained of tingling sensations and an inability to focus her eyes. Blood pressure was 68/50 mmHg, which improved to 80/60 mmHg after patient had ad lib oral fluid intake. However, 10 hours later, orthostatic vital signs revealed a 45/24 mmHg decrease in blood pressure from supine (107/69 mmHg) to sitting (62/45 mmHg) (Fig. 1).
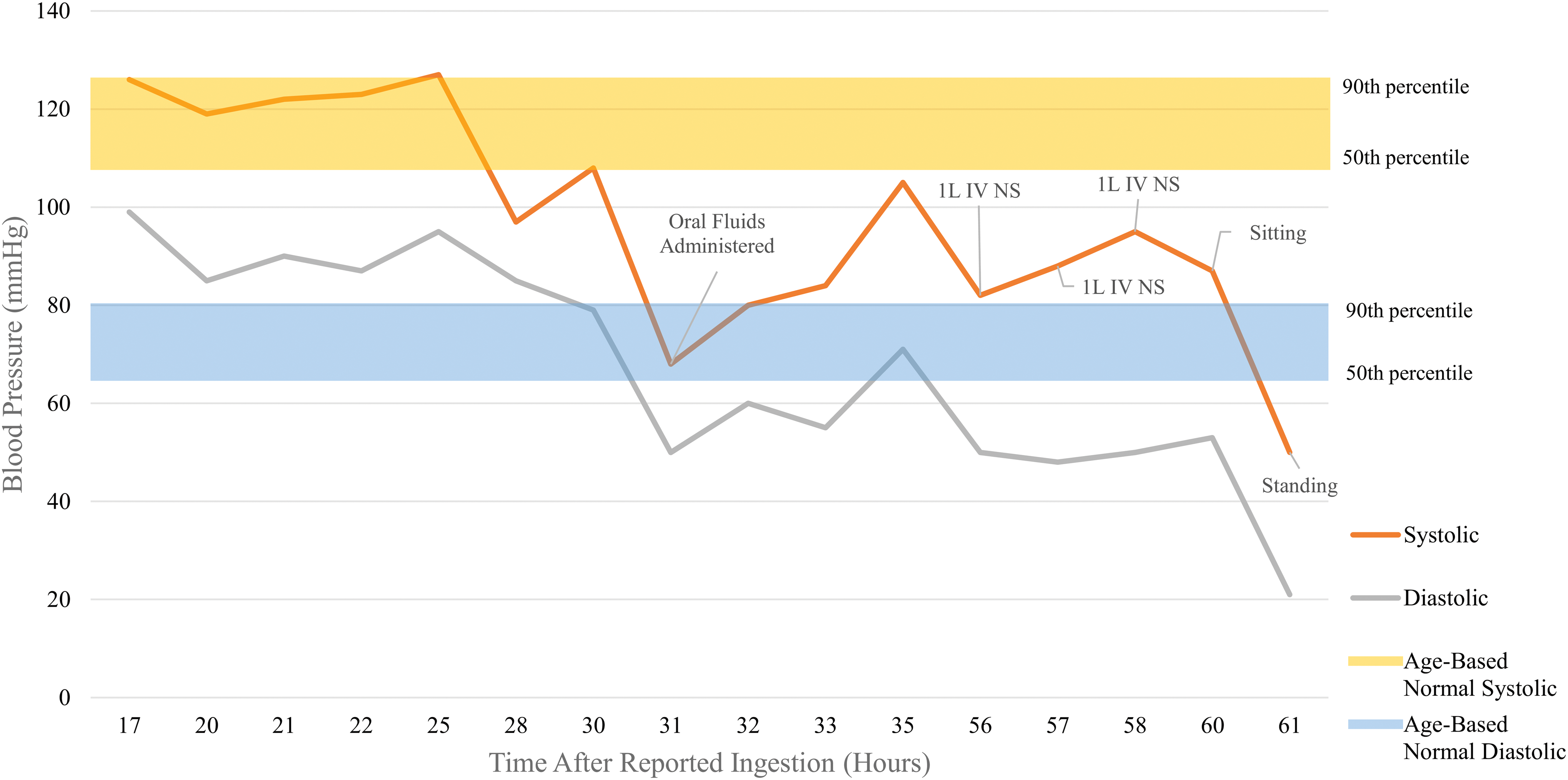
Blood pressure after melatonin ingestion. “Age-based normal” blood pressure ranges from: Flynn et al. (2017). IV, intravenous; L, liter; NS, normal saline. Color images are available online.
On hospital day 3, the patient became increasingly hypotensive. Despite receiving 3 L of intravenous normal saline, her standing blood pressure remained extremely low at 50/21 mmHg and she reported severe dizziness. She was then transferred to a pediatric hospital where she received maintenance intravenous fluid therapy for 18 hours. Blood pressure stabilized without vasopressor support after 24 hours.
This case is reported to highlight the paucity of information on melatonin toxicology. There are limited reports of overdose and reported cases ingested lower quantities than seen in our patient. Symptoms reported include drowsiness, dizziness, blurry vision, and confusion (Holliman and Chyka 1997). This patient exhibited similar symptoms, as well as significant orthostatic hypotension. The mechanism of melatonin's blood pressure lowering effects remains unclear, but may be related to nitric oxide formation causing vasodilation, parasympathetic stimulation, or calcium metabolism (Pechanova et al. 2014).
Our case suggests a temporal relationship between melatonin overdose and severe orthostatic hypotension. Ingestion of a prolonged-release formulation may have contributed to the delayed and extended hypotensive effects (Gringras et al. 2017). The interaction between melatonin and reported co-ingested medications, and other drugs, is not well understood and could have also contributed to our patient's symptoms. It is important for prescribers to be aware of this possible effect and consider extended monitoring of orthostatic vital signs after ingestion of prolonged-release melatonin.
Footnotes
Disclosures
No competing financial interests exist.