
Abstract
Objectives:
To determine the effects of methylphenidate treatment on child growth in Thai pediatric patients with attention-deficit/hyperactivity disorder (ADHD).
Methods:
The medical records of children and adolescents with ADHD, between 5 and 18 years of age, who received pharmacological treatment with methylphenidate as a sole psychiatric medication for ≥1 year between 2001 and 2018 at the Rajanagarindra Institute of Child Development, Thailand, were retrospectively reviewed. Data on anthropometric parameters and methylphenidate use were extracted. Height and weight were converted to age- and gender-corrected standard scores (z-scores) using norms from the Thai pediatric population. Changes in height and weight z-scores were assessed using a paired t-test or one-way repeated measures ANOVA with the Bonferroni correction.
Results:
In this retrospective observational study, 911 children and adolescents were eligible, with the mean age of 95.0 ± 19.5 months at baseline, the cumulative duration of methylphenidate treatment of 39.4 ± 23.5 months, and the average daily dosage of 14.1 ± 6.2 mg/day. Comparative analysis found no statistically significant change in height z-scores between baseline and last recorded measurement (mean difference = 0.0017, confidence interval [95% CI] = −0.0004 to 0.0038, p = 0.107), while a slight, but significant increase in weight z-scores was observed (mean difference = 0.0271, 95% CI = 0.0179–0.0362, p < 0.001). Longitudinal analysis observed that weight z-scores were significantly decreased during the first year of therapy, but regained in the second year and continued to increase in subsequent years of therapy.
Conclusion:
Treatment with methylphenidate in our cohort of Thai pediatric patients with ADHD was not associated with growth deficits, except for a slightly significant decrease in weight during the first year of therapy.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most commonly diagnosed neurodevelopmental disorders in pediatric populations, with estimated prevalence of 5%–7% in school-aged children and adolescents (Polanczyk et al. 2007; Faraone et al. 2015; Thomas et al. 2015). It is characterized by three major behaviors, that is, inattentiveness, impulsiveness, and hyperactivity, which make the patient's difficulty staying focused and controlling behaviors (Thapar and Cooper 2016). The management of ADHD includes nonpharmacological interventions and pharmacological treatments, aiming at reducing ADHD symptoms and associated impairment, as well as making such symptoms more manageable (Taylor et al. 2004; Subcommittee on Attention-Deficit/Hyperactivity Disorder, Steering Committee on Quality Improvement and Management 2011; Bolea-Alamanac et al. 2014). In the past few decades, the prescription of ADHD medication has markedly increased in a number of countries across multiple regions (Beau-Lejdstrom et al. 2016; Renoux et al. 2016; Bachmann et al. 2017; Man et al. 2017; Raman et al. 2018).
Methylphenidate is one of the most frequently prescribed drugs for the treatment of ADHD in children and adolescents (Connolly et al. 2015; Briars and Todd 2016). It is a recommended stimulant agent in most guidelines for the management of ADHD (Subcommittee on Attention-Deficit/Hyperactivity Disorder, Steering Committee on Quality Improvement and Management 2011; Hodgkins et al. 2013; Bolea-Alamanac et al. 2014) as it is proven to be effective and associated with improved ADHD symptoms in pediatric patients (Storebo et al. 2015; Chan et al. 2016; Catala-Lopez et al. 2017; Cortese et al. 2018; Padilha et al. 2018). In the management of ADHD, many children do require stimulant medication in the long term; as a result, the potential negative impact of such medication on child growth is of particular concern among the parents of treated patients (Vitiello 2008). Despite a number of studies conducted over the past four decades, the effects of methylphenidate treatment on child growth remain a controversial issue (Poulton 2005; Clavenna and Bonati 2017; Groenman et al. 2017).
In Thailand, hundreds of thousands of Thai children and adolescents suffer from ADHD, with estimated prevalence of 5.1%–6.5% (Benjasuwantep et al. 2002; Wacharasindhu and Panyyayong 2002). Methylphenidate is the most prescribed ADHD medication for the treatment of pediatric patients in Thailand as it is the only stimulant available in most settings (Trangkasombat 2008). Evidence suggests that responses to stimulant agents, including adverse drug reactions, are somewhat influenced by race and ethnicity (McGough et al. 2009; Hart et al. 2012); however, there have been limited studies examining the effects of methylphenidate treatment on child growth in Asian population, resulting in no clinical practice guidance applicable to this group of population (Kim et al. 2014). Therefore, this study aimed to determine the effects of methylphenidate treatment on physical growth of Thai pediatric patients with ADHD, for which little or no information is available.
Methods
Study design and setting
This retrospective observational study followed the Methodology for Conducting Retrospective Chart Review Research in Child and Adolescent Psychiatry (Gearing et al. 2006) and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies (von Elm et al. 2007). The study proposal was approved by the Human Research Ethics Committee of the Rajanagarindra Institute of Child Development.
A retrospective review of medical records at the Rajanagarindra Institute of Child Development, Thailand, was conducted, with rigorous methodological considerations as previously suggested (Vassar and Holzmann 2013). A cohort of pediatric patients with ADHD was initially identified through computerized database system. At the Rajanagarindra Institute of Child Development, a diagnosis of ADHD was established by a psychiatrist or a pediatrician based on the Diagnostic and Statistical Manual of Mental Disorders fourth edition-text revision (DSM-IV-TR) or more recent DSM-5 criteria (American Psychiatric Association 2000, 2013). This study was restricted to children and adolescents, between 5 and 18 years of age at baseline, who received methylphenidate treatment for 1 year or more between 2001 and 2018, inclusively. Patients who took any other psychiatric medications at baseline or had other illnesses that might affect physical growth were excluded from the analyses in line with this study's objective to focus on the effects of methylphenidate treatment exclusively. Non-Thai patients were also excluded from analysis.
Sample size determination
We conducted a priori power analysis in G*power 3.1.9.2 for Windows for paired samples to determine the minimum sample size required. The t-test was applied to detect the difference of 0.05 in z-scores between two dependent values (at baseline and last recorded measurement), with an estimated value of 0.3 in standard deviation of z-scores, the precision and confidence level of 95% (α = 0.05), and 80% power (β = 0.2). With this assumption, an observational study would require, at least, a total of 285 patients. An ad hoc approach with no less than a priori estimate of sample size was used in this study where it was feasible to identify all patients' medical records.
Data collection and measurement
Data were obtained retrospectively from the medical records at multiple, consecutive visits, until the last visit that the patients received methylphenidate as the only psychiatric medication for the treatment of ADHD. At the first visit of methylphenidate treatment, collected baseline data included gender, date of birth, nationality, domicile, primary diagnosis, comorbidities, date of medication start, formulation of methylphenidate (i.e., an immediate-release formulation of methylphenidate [Ritalin®] or an extended-release formulation of methylphenidate [Concerta®]), medication dosage (mg/day), height (cm), and weight (kg). In other subsequent visits, collected data included date of a follow-up, formulation of methylphenidate (i.e., Ritalin or Concerta), medication dosage (mg/day), height (cm), and weight (kg).
At the Rajanagarindra Institute of Child Development, anthropometric data had been measured by a nurse at an outpatient clinic using a ruler attached to the wall and a calibrated weight scale. Height (cm) and weight (kg) were converted to age- and gender-corrected standard scores (z-scores), which are widely accepted as the most valid anthropometric method for assessing a child's growth and development (WHO Multicentre Growth Reference Study Group 2006; de Onis 2013). In this study, height and weight were standardized by age and gender using the THAI-Z program, of which its database was generated using the anthropometric data of Thai children and adolescents derived from the latest national growth references for height and weight (Ekwattanakit et al. 2017). A z-score of 0 indicates that the height or weight value is approximately at the mean of Thai children and adolescents within the same age and gender, where a z-score of +1 or −1 indicates a measurement of one standard deviation more or less than the mean, respectively.
Statistical analysis
Descriptive statistics were used to describe information about variables in the dataset. Since this study was framed retrospectively, there were missing data in the medical records at various time points. We treated missing values by imputing the value using an averaging strategy (Worster and Haines 2004). Comparison of height and weight z-scores between different time points was executed using a paired t-test or one-way repeated measures ANOVA with the Bonferroni correction, as appropriate. The association between demographic variables or use of methylphenidate regimens and changes in a height or weight z-score was examined using multivariable regression analysis. All statistical tests were two sided, and a p-value of less than 0.05 was considered to indicate statistical significance. All statistical analyses were performed using SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.).
Results
Demographic characteristics
Of 2958 medical records identified in the database between 2001 and 2018, 911 were eligible for this study. Baseline characteristics of 911 eligible patients are shown in Table 1. The majority of patients were male (84.6%) and lived in Chiang Mai (81.2%), with the mean age of 95.0 ± 19.5 months (range 60–168 months). Most patients (98.9%) started the treatment with methylphenidate before the beginning of the teenage stage. Two-third of the patients (68.4%) had ADHD as a sole underlying condition, while one-fourth of the patients (25.4%) had a learning disorder as another comorbidity. The cumulative duration of methylphenidate treatment was 39.4 ± 23.5 months (range 12–136 months), with the average daily dosage of 14.1 ± 6.2 mg/day (range 3.1–50.0 mg/day). The majority of patients (86.8%) received methylphenidate treatment with the average daily dosage of less than 20 mg/day. An immediate-release formulation of methylphenidate (Ritalin) was used as the only stimulant agent throughout the course of ADHD treatment in most patients (88.1%), while an extended-release formulation of methylphenidate (Concerta) was prescribed to replace multiple daily doses of immediate-release formulation in a relatively few patients (11.9%) at some follow-up visits.
Characteristics of Eligible Patients
The values represent n (%).
The values represent mean ± SD.
SD, standard deviation.
Study outcomes
Overall, there was no statistically significant change in height z-scores between baseline and last recorded measurement (p = 0.107), while a mean weight z-score was 0.1283 ± 0.2612 at baseline and 0.1554 ± 0.3020 at last recorded measurement, resulting in a 0.0271 increase in weight z-scores (p < 0.001) (Fig. 1). Multivariable regression analysis found that gender and treatment duration were statistically significantly associated with changes in height and weight z-scores (Table 2). Changes in height and weight z-scores were more obvious in boys than in girls (0.0030 ± 0.0322 vs. −0.0060 ± 0.0273, p = 0.002; 0.0318 ± 0.1416 vs. 0.009 ± 0.1340, p = 0.017, respectively). There was also a small, but statistically significant positive association between treatment duration and changes in height and weight z-scores (B = 0.000, SE = 0.000, β = 0.075, confidence interval [95% CI] = 0.000–0.000, p = 0.027; B = 0.001, SE = 0.000, β = 0.171, 95% CI = 0.001–0.001, p < 0.001, respectively).
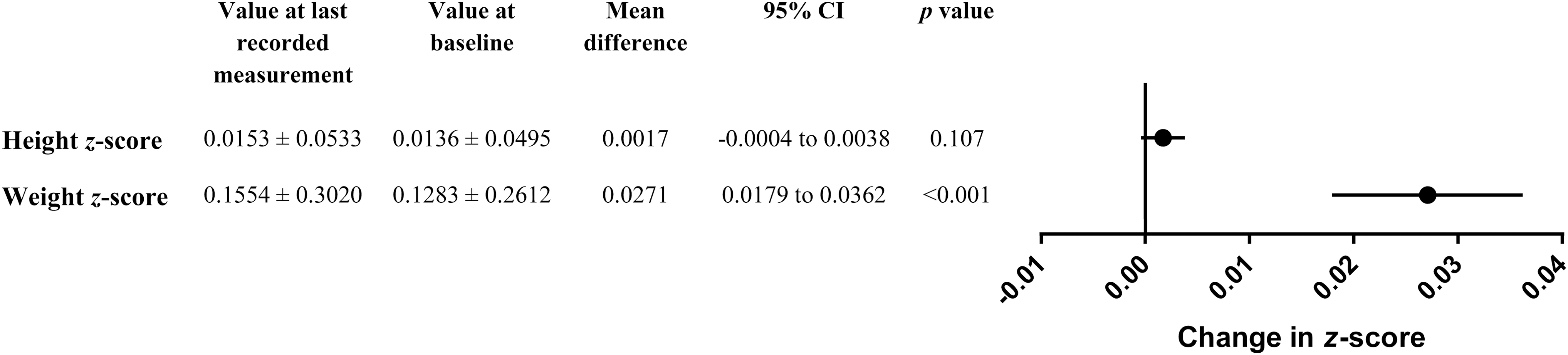
Changes in height and weight z-scores of the patients. CI, confidence interval.
Multivariable Regression Analysis
For the whole population, height z-scores were not significantly altered throughout the study period; the only exception during the first 5 years of medication was the value at the fifth year of medication, which was significantly higher than the value at baseline (Fig. 2 and Table 3). Nevertheless, weight z-scores were statistically significantly decreased during the first year of medical therapy, but regained in the second year and continued to increase in the third and fourth years of medical therapy. From the third year of methylphenidate treatment onward, the weight z-score was significantly higher than the value at baseline (Fig. 3 and Table 3).
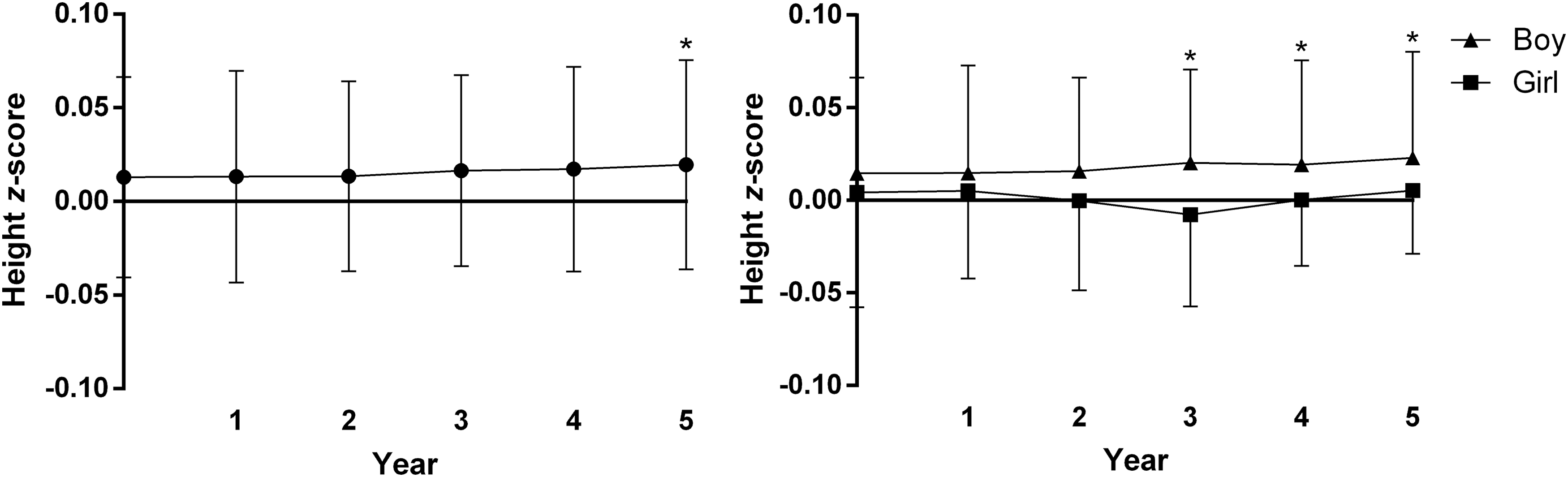
Height z-scores of the patients. *Statistically significant when compared to baseline.
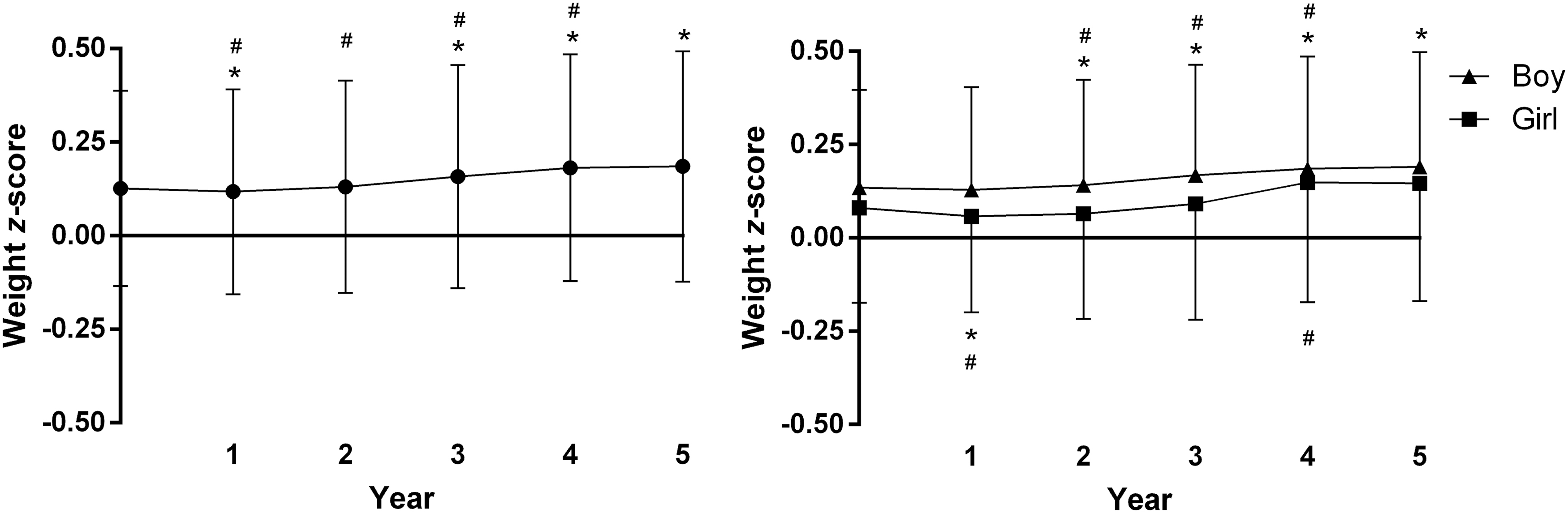
Weight z-scores of the patients. *Statistically significant when compared to baseline. #Statistically significant when compared to the preceding value.
Height z-Scores and Weight z-Scores of the Patients
Discussion
To the best of our knowledge, this is the largest observational study examining the impact of methylphenidate treatment on child growth in Thai children and adolescents with ADHD. It involved almost a thousand of methylphenidate-treated pediatric patients during 18 years of experience of methylphenidate use in clinical practice at the Rajanagarindra Institute of Child Development. The results indicate that ADHD treatment with methylphenidate is not associated with growth deficits in Thai pediatric patients. Our findings could be used to consolidate evidence-based guidelines for the treatment of children and adolescents with ADHD, particularly for Thai population. At this moment, the data do not support the rationale for using drug holidays in normally growing Thai children and adolescents treated with methylphenidate. However, child growth should still be regularly monitored in all stimulant-treated pediatric patients so as to identify some children who may develop an abnormal pattern of growth and require management or changes in the treatment regimen in a timely manner (Spencer et al. 2006).
Despite a controversial debate about the possible negative effects of methylphenidate on height deficit, this study found no evidence of height deficit following the initiation of methylphenidate treatment. At baseline, our cohort of pediatric patients with ADHD was approximately the expected height for their age and gender, with a height z-score of slightly more than 0. The patients gained height steadily throughout the study period, and by the end of the study, the height z-score increased slightly, suggesting that height growth in these children was not inhibited. Nevertheless, literature is still inconsistent in the association between height growth and treatment with methylphenidate. Some studies report a significant delay in height among children treated with methylphenidate (Poulton and Cowell 2003; Swanson et al. 2006, 2007; Faraone et al. 2008; Ptacek et al. 2009; Zhang et al. 2010; Poulton et al. 2013, 2016; Kim et al. 2014; Powell et al. 2015; Lentferink et al. 2018), whereas some others do not observe any significant change in height between baseline and follow-up visits (Kramer et al. 2000; Biederman et al. 2003, 2010; Harstad et al. 2014; Kang et al. 2016; Diez-Suarez et al. 2017; McCarthy et al. 2018).
It is reasonable to assume that relatively lower doses of methylphenidate used in this study (<20 mg/day in most patients), when compared to other previous studies with positive results in Western countries, might be one of the possible reasons why significant growth deficits, if any, were not acknowledged (Lisska and Rivkees 2003; Zhang et al. 2010). Evidence suggests that the negative effect of methylphenidate treatment on child growth may be dose dependent (Lisska and Rivkees 2003; Zhang et al. 2010; Powell et al. 2015), and growth deficits are observed less frequently when methylphenidate is used at doses not exceeding 20 mg/day (Poulton 2005; Faraone et al. 2008). Although there are still ongoing discrepancies in the literature on this subject, lines of evidence suggest that a history of methylphenidate treatment in childhood does not affect ultimate adult height (Spencer et al. 1996; Poulton and Cowell 2003; Pliszka et al. 2006; Swanson et al. 2007; Biederman et al. 2010; Renes et al. 2012; Harstad et al. 2014; Kim et al. 2014). Likewise, long-term use of methylphenidate does not significantly affect growth hormone or insulin-like growth factor (IGF)-I in children and adolescents (Toren et al. 1997; Bereket et al. 2005). Therefore, methylphenidate seems to have no clinically significant impact on patient height in a long run.
In this longitudinal study, it was observed that the weight z-scores of the patients were significantly decreased during the first year of methylphenidate treatment, but regained in subsequent years of therapy. Our finding is consistent with other previous studies, where treatment with methylphenidate led to a significant deceleration in weight, but not in height of the patients during the first year of therapy (Gross 1976; Charach et al. 2006; Jasper et al. 2009; Schwartz et al. 2014). Correspondingly, a negative impact on weight seems to be a temporary condition across multiple independent studies as weight can be regained later and the extent of negative consequences is less distinctive thereafter (Sund and Zeiner 2002; Zhang et al. 2010; Gerlach et al. 2013). Continued treatment with methylphenidate seems to be a favorable option, despite a reduction in weight during the first few months after initiating medication. A transient weight suppression could be outweighed straightforwardly by expected benefits when young children are treated with methylphenidate (Storebo et al. 2015, 2016). Although the undesirable effect of methylphenidate treatment on weight seems not to be of clinical significance, there are no specific guidelines for what magnitude of weight deficit should trigger changes in the treatment regimen (Graham et al. 2011).
Reduced food intake may be a plausible explanation of the flattening in weight curve during the first few months of methylphenidate treatment since loss of appetite is renowned as the most common adverse effect of methylphenidate in the literature (Dura-Trave et al. 2012; Bou Khalil et al. 2017; Storebo et al. 2018). Moreover, studies conducted in Asian countries showed a relatively higher rate of decreased appetite among patients treated with methylphenidate than those conducted in Western countries (Gau et al. 2006; Lee et al. 2007; Graham et al. 2011). Evidence suggests that some endogenous peptides (e.g., ghrelin, adiponectin, or leptin) may play a key role in underlying neurobiological mechanisms of methylphenidate-related anorexigenic effect (Sahin et al. 2014; Gurbuz et al. 2016). However, one previous retrospective chart review observed weight loss in some methylphenidate-treated children, whose parents did not notice any change in their child's appetite (Poulton and Cowell 2003). Weight reduction during the first year of methylphenidate treatment can also be assumed to be the drug action through the dopaminergic and adrenergic pathways (Engert and Pruessner 2008; Gamo et al. 2010; Faraone 2018). This may be another explanatory biological mechanism of methylphenidate-associated deficits in expected weight (Kuczenski and Segal 1997).
In regression analysis, gender was found to be associated with changes in height and weight z-scores, whereas age at baseline was not. Boys were more sensitive to the effects of methylphenidate treatment on child growth than girls. However, there was gender imbalance in our study population, 84.6% of which were boys. In most previous studies, there is no observed difference in the effects of methylphenidate treatment on child growth between boys and girls (Kramer et al. 2000; Biederman et al. 2003, 2010; Zhang et al. 2010; Kim et al. 2014). On the other hand, methylphenidate treatment starting from an early age did not affect growth deficits in a greater extent than an older age in our study. This finding provides evidence to inform clinicians and parents when methylphenidate is needed for the treatment of ADHD in young children. Medication is usually started at the age of 6–8 years because ADHD symptoms commonly appear to cause negative consequences to children's learning around first to third grades. Of note, literature is still inconsistent on this subject as some evidence suggests that growth deficits are more evident in young children, when compared to their older counterparts (Spencer et al. 1996; Swanson et al. 2007; Faraone et al. 2008; Diez-Suarez et al. 2017), whereas others report the opposite (Powell et al. 2015).
The strengths of this study include the longitudinal analysis of a large cohort of Thai pediatric patients with ADHD, using a reliable method for the assessment of child growth of Thai children and adolescents. Longitudinal analysis is sensitive for detecting changes in height and weight z-scores, with a mean follow-up period of ∼40 months in this study. Changes in z-scores are more reliable to detect growth deficits than using growth percentile calculators because working in child growth percentiles may distort the data due to the nonlinear relationship and may fail to demonstrate a significant effect accordingly (Poulton and Cowell 2003). In addition, this study was designed to examine the effects of methylphenidate treatment exclusively, without the confounding effects of other psychiatric medications or medical illnesses that may influence appetite or growth parameters.
Although our findings provide insights into the effects of methylphenidate on child growth, there were some limitations due mainly to a retrospective approach. This study investigated naturalistic data from a cohort of children and adolescents for whom their anthropometric parameters were regularly monitored at follow-up in clinical practice. Thus, it is reasonable to assume that, in some cases, clinicians were probably reviewing child growth curves and might have made advice to correct any emerging growth deficit through diet and/or changes in treatment regimens. Some children with growth deficits might cease medication or change treatment regimens earlier than 1 year or at some points during the study period so that they were excluded from our analysis. Therefore, the effects of methylphenidate treatment on child growth in this study might be underestimated due to possible sampling bias toward responders. Moreover, with available databases, we could not monitor patients' compliance. Thus, it is possible that some patients might not take methylphenidate as prescribed. The relationship between methylphenidate treatment and child growth may still need to be confirmed in further studies.
Lack of a control group (i.e., untreated patients) might be considered another limitation of this study. However, in clinical practice settings, the number of patients with mild to moderate ADHD who were receiving no pharmacological treatment for a period of time were rather limited because of progressive psychosocial and/or educational deterioration. Setting up such a control group is not only proven to be impractical but also unethical. Use of individual control oneself is often considered an alternative, acceptable design. Child growth was assessed using z-scores, which compared each patient to standardized norms. With this study design, it assumes that changes in z-scores reflected the effects of methylphenidate treatment rather than other factors, such as diet, eating habits, sleep disorders, physical activity, lifestyle, or any other unmeasured confounders, which may not necessarily be the case.
Last, but not least, the results of this study should be interpreted with caution. The formulation of methylphenidate used in our cohort of Thai pediatric patients with ADHD was primarily an immediate-release formulation. Thus, the results may not be generalizable to some other settings where extended-release formulations are more commonly used. Furthermore, the findings, which were derived predominantly from male patients, may not be representative of growth effects on female patients.
Conclusions
In conclusion, treatment with methylphenidate was not related to growth deficits in the cohort of Thai pediatric patients with ADHD, except for a slightly significant decrease in weight during the first year of therapy. This study provides further evidence that the negative effects of methylphenidate on child growth are unlikely to be of clinical concern for the majority of Thai children and adolescents with ADHD. However, a regular growth monitoring in children and adolescents treated with methylphenidate is still needed so as to identify ones who may require changes in treatment regimens.
Clinical Significance
This study provides further evidence of the impact of methylphenidate treatment on child growth, particularly for Thai pediatric patients with ADHD. The results do not support the rationale for using drug holidays in the majority of Thai children and adolescents, including those who even have weight loss during the first few months after initiating methylphenidate treatment. However, in regard to inconsistent results reported in a number of previous studies involving various groups of population, a regular growth monitoring is apparently necessary and should be a requisite for every clinical practice setting wherever children and adolescents are being treated with methylphenidate.
Footnotes
Acknowledgments
We thank study nurses and administrative staff at the Rajanagarindra Institute of Child Development for their assistance in data entry. We are thankful to Dr. Vip Viprakasit and Dr. Supachai Ekwattanakit for providing the THAI-Z (worksheet based) program for calculating height and weight z-scores of Thai children and adolescents.
Disclosures
All authors declare that they have nothing to disclose regarding institutional or corporate/commercial relationships going back 36 months, which might pose a conflict of interest regarding publication of this article.