
Abstract
Objectives:
We evaluated the pharmacokinetics (PK) of an investigational immediate-release amphetamine (AMP) sulfate formulation (AR19) designed to deter nonoral administration versus reference racemic amphetamine sulfate (RA-AMPH). We investigated AMP bioavailability from AR19, the effect of taking AR19 with food or sprinkling the capsules on food, and dose proportionality.
Methods:
Participants received AR19 (20 mg) or reference RA-AMPH (20 mg) (bioequivalence study) or AR19 5 or 30 mg (dose comparison study). Food effect study participants received AR19 (20 mg) as intact capsule while fasted or after high-fat/-calorie meal, or as pellets sprinkled on applesauce or yogurt (≥6-day washout). Blood samples were analyzed for dextroamphetamine (d-AMP) and levoamphetamine (l-AMP) PK: Cmax, AUClast, AUCinf, λz, T½, and Tmax. Safety was assessed.
Results:
Bioequivalence, dose comparison, and food effect studies included 36, 24, and 36 participants. The 90% confidence intervals (CIs) of Cmax, AUClast, and AUCinf for AR19 20 mg versus reference RA-AMPH or AR19 with intact capsule and meal or sprinkled AR19 pellets on food versus fasted were between 80% and 125%. Dose-normalized Cmax/D, AUClast/D, and AUCinf/D for AR19 5 versus 30 mg had CIs within 80%–125%. Mean ± standard deviation (SD) Tmax was comparable for AMP (d-AMP; l-AMP) following AR19 20 mg (2.84 ± 1.05; 3.05 ± 1.22) versus reference RA-AMPH (2.52 ± 0.75; 2.75 ± 1.00), and AR19 5 mg (2.48 ± 0.57; 2.65 ± 0.65) versus AR19 30 mg (2.55 ± 0.56; 2.72 ± 0.65). Mean ± SD Tmax for AMP (d-AMP; l-AMP) was higher with intact capsule and meal (5.59 ± 1.57; 5.59 ± 1.59) versus fasted (2.85 ± 0.76; 2.97 ± 0.79). No serious adverse events were reported.
Conclusion:
AR19 was bioequivalent to reference RA-AMPH. Bioavailability was similar at doses between 5 and 30 mg and was not impacted by meal consumption or sprinkling on food. AR19 at tested doses was well tolerated.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurobehavioral condition characterized by inattention, hyperactivity, and/or impulsivity (Wolraich et al. 2011). It is estimated to affect ∼11% of children (aged 4–17 years) and 8% of adults worldwide (Visser et al. 2014; Ustun et al. 2017). If left untreated, ADHD can interfere with daily functioning, academic achievement, and social interactions (American Psychiatric Association 2013).
Prescription stimulants such as amphetamines (AMP) are the first-line pharmacotherapy choice in the treatment of ADHD (Wolraich et al. 2011; Faraone et al. 2015). Several AMP formulations are available, providing a range of release profiles, salt forms, and isomeric compositions (dextroamphetamine [d-AMP] and levoamphetamine [l-AMP]). This range of therapeutic options enables clinicians to tailor treatment regimens for each patient (Markowitz and Patrick 2017).
Despite their demonstrated efficacy, prescription stimulants have high potential for nonmedical use (NMU) and are classified as Schedule II drugs under the Controlled Substances Act owing to the euphoric effects and enhanced alertness associated with their use (Clemow and Walker 2014; Romach et al. 2014; Faraone et al. 2015; Compton et al. 2018). Prescription stimulant NMU is the use of prescription stimulants without a prescription or in a way that differs from how it was prescribed, including actions that can be considered either misuse or abuse (Center for Behavioral Health and Statistics and Quality 2017). In 2017, an estimated 5.8 million U.S. individuals aged ≥12 years reported past-year prescription stimulant NMU (Center for Behavioral Health and Statistics and Quality 2017). Prescription stimulant NMU is associated with serious adverse health outcomes and places a substantial burden on health care facility utilization (Substance Abuse and Mental Health Services Administration 2013; King et al. 2018; Faraone et al. 2019).
Nonoral routes of administration are frequently reported with prescription stimulant NMU. In a nationally representative survey, in which 10,000 U.S. adults reported prescription stimulant NMU, 11%–40% used intranasal administration, and 1%–11% and 1%–6% used intravenous administration or smoking, respectively (Cassidy et al. 2015). Emerging evidence suggests that nonoral prescription stimulant NMU may be associated with increased incidence of adverse medical outcomes compared with oral NMU and no NMU (Faraone et al. 2019).
AR19 is an investigational formulation of immediate-release (IR) racemic AMP sulfate that has been developed with Intac® technology (Grünenthal GmbH, Aachen, Germany). The AR19 formulation was developed with the intention of impeding manipulation of the pellets in the capsules for intranasal, intravenous, or smoking routes of administration. AR19 is based on a U.S. Food and Drug Administration (FDA)–approved IR formulation of AMP sulfate in a 1:1 racemic mixture of d- and l-AMP (RA-AMPH) that is already in clinical use for the treatment of children and adolescents with ADHD (Evekeo®; referred to as reference RA-AMPH in this publication) (Childress et al. 2015; Evekeo Package Insert 2016). Reference RA-AMPH has been demonstrated to significantly improve ADHD symptoms compared with placebo and was well tolerated in children aged 6–12 years in a laboratory classroom study (Childress et al. 2015; Evekeo Package Insert 2016).
The AR19 formulation of RA-AMPH is in development to help deter abuse via intranasal and intravenous routes of administration. The AR19 formulation employs physical and chemical characteristics that are designed to create a barrier to manipulation for use via unintended administration methods, such as intranasal administration, injection, and smoking. Therefore, we aimed to establish that these barriers used in the formulation do not affect the pharmacokinetics (PK) of AMP when AR19 is administered orally, as intended, at a range of different doses. In addition, it is known that most AMP formulations demonstrate dose proportionality such that increased dosage results in increased exposure (Markowitz and Patrick 2017). Therefore, we also aimed to demonstrate that the AR19 formulation has a dose-proportional PK profile, with the hypothesis that the AR19 formulation does not impact the dose range of exposure of AMP as it compares with reference RA-AMPH.
Food may also interfere with absorption and systemic delivery of orally administered drugs, leading to potential reductions in drug bioavailability and therapeutic effects (Won et al. 2012). In addition, individuals with ADHD, particularly children and adolescents, may have difficulty swallowing pills and may adhere to treatment regimens more closely if pill contents are sprinkled on food (Patel et al. 2015; Jagani et al. 2016). As a result, PK studies are necessary to confirm consistent drug delivery when drugs are administered as intact capsules with meals or as sprinkled pellets on food (Ermer et al. 2016; Sikes et al. 2017; Wang et al. 2019).
We conducted three studies (bioequivalence, dose comparison, and food effect) in healthy volunteers to assess the effect of the novel AR19 formulation with intended manipulation-deterrent properties on the PK of AMP as intact capsule with food or pellets sprinkled on food.
Methods
Study participants
All three studies included healthy male and female participants, aged 18–45 years, with body mass index 18–30 kg/m2 and body weight ≥50 kg. Exclusion criteria for all three studies included history or presence of a clinically significant condition that, in the opinion of the investigator, may have jeopardized the safety of the participant or validity of the results, particularly, any history of serious cardiovascular conditions or psychosis, mania, bipolar disease, or depression; history or presence of tics or Tourette syndrome, marked anxiety, tension, or agitation, or allergic or adverse response to AMP sulfate; abnormal diet during the 4 weeks before the first dose of study medication, or participation in another clinical trial within 30 days before the first dose of study medication; treatment with any known drugs that are moderate or strong inhibitors of cytochrome P450 enzymes, or consumption of beverages or foods known to alter drug metabolism (e.g., grapefruit); or history of substance abuse or treatment within the past 2 years, or positive urine screen for substance abuse. Additional exclusion criteria in the food effect study were presence of braces or retainer, unwillingness or inability to consume an entire standard high-fat/high-calorie meal in ≤30 minutes before dosing, or allergic reaction to or unwillingness to eat applesauce or yogurt.
Study design
Study protocols and other study documents were reviewed and approved by an independent Institutional Review Board that operates in accordance with the Code of Federal Regulations (21 CFR Part 56). Written informed consent was obtained from all participants before any study procedures were performed. All studies were conducted as single-dose, open-label, randomized crossover studies during which participants received treatments following a ≥10-hour overnight fast, with a ≥6-day washout period between treatments. The bioequivalence and dose comparison studies were two-period, two-treatment, and two-sequence studies, and the food effect study was a four-period, four-treatment, and four-sequence study.
In the bioequivalence study, conducted December 8–16, 2017, the primary objective was to compare the plasma concentration–time curve and absorption of AMP from AR19 versus reference RA-AMPH, and the secondary objective was to evaluate the safety of AR19. Participants received a single dose of AR19 (1 × 20-mg pellets in capsule) in one period followed by a single dose of reference RA-AMPH (2 × 10-mg tablets) in the second period, or vice versa.
The primary objective of the dose comparison study conducted November 30–December 8, 2018, was to compare the PK of AMP from AR19 given as a 5-mg (2 × 2.5 mg) versus a 30-mg single dose under fasted conditions. The 5-mg dose was derived based on the lowest AR19 dose strength (2.5 mg), which was doubled to ensure that the analytical method used was above the limit of quantitation. Participants received AR19 5 mg in one study period, followed by AR19 30 mg in the next study period, or vice versa.
The food effect study was conducted from April 21–May 14, 2018, with a primary objective to compare the plasma concentration–time curve and absorption of AMP from AR19 20 mg when administered as an intact capsule under fasted or fed conditions and as sprinkled capsule pellets in the fasted state. The secondary objective was to evaluate the safety of AR19 20 mg when administered as an intact capsule under fasted or fed conditions, or when sprinkled as pellets on applesauce or yogurt. Participants received a single AR19 dose (20 mg) as an intact capsule while fasted or after a high-fat/high-calorie meal or as pellets sprinkled on applesauce or yogurt. Participants were randomized to receive each of the following treatments in one of four sequence groups (ABDC, BCAD, CDBA, and DACB). Treatment A was AR19 20 mg as an intact capsule following a ≥10-hour overnight fast. Treatment B was AR19 20 mg as an intact capsule following consumption of a standard FDA-recommended high-fat/high-calorie meal of two eggs fried in butter, two strips of bacon, two slices of toast with butter, four ounces of hash brown potatoes, and eight ounces of whole milk, totaling ∼800–1000 calories (FDA 2002). Treatment C was AR19 20 mg as capsule pellets sprinkled on applesauce, and treatment D was AR19 20 mg as capsule pellets sprinkled on yogurt.
The three studies had similar methods for administration and blood sample collection. Each participant received the oral dose of the assigned formulation with 240 mL (8 fl oz) of room-temperature water. Participants then fasted for 4 hours. Water was allowed ad libitum during the study, except for 1 hour before through 1 hour after each dose. Drug administrations were separated by a washout period of ≥6 days. Blood samples (6 mL) were collected at predose (0 hours); at 2, 5, 10, 15, and 30 minutes postdose; and then at 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 5.5, 6, 6.5, 7, 8, 10, 12, 24, 36, and 48 hours postdose (25 samples total per study participant) and analyzed for d- and l-AMP.
The PK parameters analyzed in all three studies included the peak concentration in plasma (Cmax), area under the concentration–time curve from time-zero to the time of the last quantifiable concentration (AUClast), area under the plasma concentration–time curve from time-zero extrapolated to infinity (AUCinf), elimination rate constant (λz), terminal half-life (T½), and time to peak concentration in plasma (Tmax).
Safety
Study investigators evaluated safety using physical examinations, vital sign measurements, clinical laboratory evaluations, electrocardiograms, and reported or observed adverse events (AEs). Medical Dictionary for Regulatory Activities versions 20.1, 21.1, and 21.0 were used to characterize AEs in the bioequivalence, dose comparison, and food effect studies, respectively.
Statistical analyses
Statistical analyses were performed in SAS® (version 9.4, SAS Institute, Inc.) using the Mixed Procedure and Phoenix™ WinNonlin® (Version 6.3; Certara USA, Inc., Princeton, NJ) with the Linear Mixed Effects Model. Two comparisons were performed in the bioequivalence and dose comparison studies, and four were performed in the food effect study following FDA guidelines (FDA 2002, 2001).
Data were included in analyses for participants who did not remain in the study for all study periods. In the bioequivalence and food effect studies, a sample size of 36 participants was predicted to provide 90% power to obtain 90% confidence intervals (CI) within the 80%–125% range for bioequivalence or comparative bioavailability at an α = 0.05, assuming a within-subject coefficient of variation of 25% and a true difference between formulations of ±5% (FDA 2001). The sample size in the dose comparison study was not based on statistical considerations, and the number of participants planned for enrollment was considered sufficient to achieve the study objectives.
In each study, analysis of variance and one-sided t-tests were used for statistical comparisons. In the bioequivalence study, the log-transformed PK exposure parameters Cmax, AUClast, and AUCinf were compared for d- and l-AMP from AR19 20 mg versus reference RA-AMPH (FDA 2019). An exploratory analysis assessed dose linearity with AR19 5 and 30 mg from the dose comparison study and AR19 20 mg from the bioequivalence study. The analysis compared dose-normalized d- and l-AMP exposure parameters: Cmax/Dose (D), AUClast/D, and AUCinf/D. In the food effect study, the log-transformed PK parameters Cmax, AUClast, and AUCinf were compared for d- and l-AMP following treatments A–D.
Comparative bioavailability in the bioequivalence and food effect studies and PK linearity in the dose comparison study were assessed by calculating least squares geometric mean ratios and associated 90% CI. Plasma concentration–time data for d- and l-AMP were analyzed by noncompartmental methods for all studies.
Results
Participant disposition and baseline characteristics
In the bioequivalence study, all 36 enrolled participants (16 women and 20 men) completed both study periods (Table 1). The total AMP sulfate dosage administered to each participant who completed both study periods was 40 mg.
Baseline Characteristics
BMI, body mass index; SD, standard deviation.
In the dose comparison study, of 24 total healthy participants (16 women and 8 men), 23 (95.8%) completed both study periods (Table 1). One participant withdrew consent before dosing in the second study period. The total AMP sulfate dosage administered to each participant who completed both study periods was 35 mg.
In the food effect study, 29 (80.6%) of 36 total healthy participants (22 women and 14 men) completed all four study periods (Table 1). Seven (19.4%) participants discontinued early from the study. In the first study period, one participant withdrew consent for personal reasons. In the second study period, one participant was discontinued after being unable to consume the entire high-fat/high-calorie meal in ≤30 minutes, two participants were discontinued due to positive urine drug screen, and one participant withdrew consent for personal reasons. In the third study period, one participant was discontinued due to positive urine screen, and one participant withdrew consent for personal reasons. The total AMP sulfate dosage administered to each participant who completed all four study periods was 80 mg.
Participant baseline characteristics were similar across all three studies (Table 1).
Bioequivalence
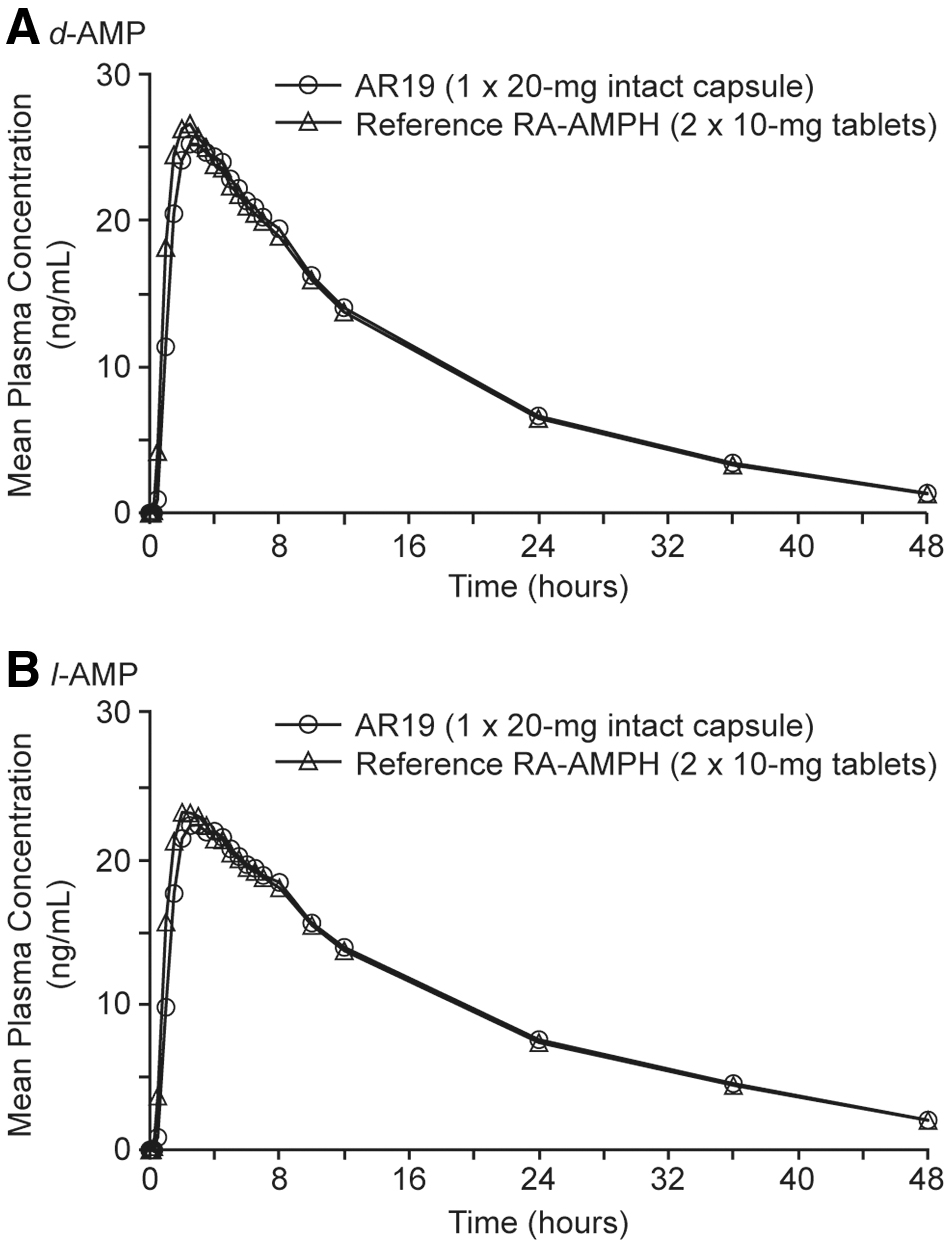
Mean plasma concentration–time data for d- and l-AMP from AR19 20 mg and reference RA-AMPH are summarized in Figure 1. Log-transformed PK parameters for d- and l-AMP (Cmax, AUClast, AUCinf, λz, and T½) were similar for AR19 20 mg and reference RA-AMPH (Table 2). AR19 and reference RA-AMPH had similar d-AMP Tmax values (mean ± standard deviation [SD], 2.84 ± 1.05 and 2.52 ± 0.75, respectively; Table 2). AR19 and reference RA-AMPH also had similar l-AMP Tmax values (mean ± SD, 3.05 ± 1.22 and 2.75 ± 1.00, respectively). The 90% CI for comparing the maximum exposure, based on log-transformed Cmax, and for comparing the total systemic exposure, based on log-transformed AUClast and AUCinf, were within the accepted 80%–125% range for bioequivalence for both d- and l-AMP (Table 3).
Mean plasma
Pharmacokinetic Parameters of d- and l-AMP Comparing AR19 (20 mg) Versus Reference Racemic Amphetamine Sulfate (Bioequivalence Study) and AR19 5 Versus 30 mg (Dose Comparison Study)
All results reported as mean ± standard deviation.
Cmax/D, AUClast/D, and AUCinf/D are calculated as log-transformed, dose-normalized values in the dose comparison study for AR19 5 and 30 mg.
λz, elimination rate constant; AMP, amphetamine; AUCinf, area under the plasma concentration–time curve from time-zero extrapolated to infinity; AUClast, area under the plasma concentration–time curve from time-zero to the time of the last quantifiable concentration; Cmax, peak concentration in plasma; D, dose; d-AMP, dextroamphetamine; h, hour; l-AMP, levoamphetamine; RA-AMPH, racemic amphetamine sulfate; Tmax, time to peak plasma concentration; T½, terminal half-life.
Statistical Analysis of d- and l-AMP Comparing AR19 (20 mg) Versus Reference Racemic Amphetamine Sulfate (Bioequivalence Study) and AR19 5 Versus 30 mg (Dose Comparison Study)
Geometric means for AR19 5, 20, and 30 mg and reference RA-AMPH based on least squares means of log-transformed parameter values.
Ratio calculated as geometric mean for AR19/geometric mean for reference RA-AMPH.
Cmax/D, AUClast/D, and AUCinf/D are calculated as log-transformed, dose-normalized values in the dose comparison study for AR19 5 and 30 mg.
AMP, amphetamine; ANOVA, analysis of variance; AUCinf, area under the plasma concentration–time curve from time-zero extrapolated to infinity; AUClast, area under the plasma concentration–time curve from time-zero to the time of the last quantifiable concentration; CI, confidence interval; Cmax, peak concentration in plasma; CV, coefficient of variance; D, dose; d-AMP, dextroamphetamine; l-AMP, levoamphetamine; RA-AMPH, racemic amphetamine sulfate.
Dose comparison
Mean plasma concentration–time data for d- and l-AMP with AR19 5 and 30 mg are summarized in Figure 2. Log-transformed dose-normalized PK parameters for d- and l-AMP (Cmax/D, AUClast/D, AUCinf/D) were similar for AR19 5 and 30 mg (Table 2). In addition, λz and T½ values were similar for AR19 5 and 30 mg (Table 2). Tmax values for d- and l-AMP were comparable following administration of AR19 5 mg (mean ± SD, 2.48 ± 0.57 and 2.65 ± 0.65, respectively; Fig. 2a and Table 2) and 30 mg (2.55 ± 0.56 and 2.72 ± 0.65, respectively; Fig. 2b and Table 2). The 90% CI comparing log-transformed dose-normalized PK parameters for maximum exposure (Cmax/D) and total systemic exposure (AUClast/D and AUCinf/D) were within the accepted 80%–125% range for AR19 5 versus 30 mg for both d- and l-AMP (Table 3).

Mean plasma
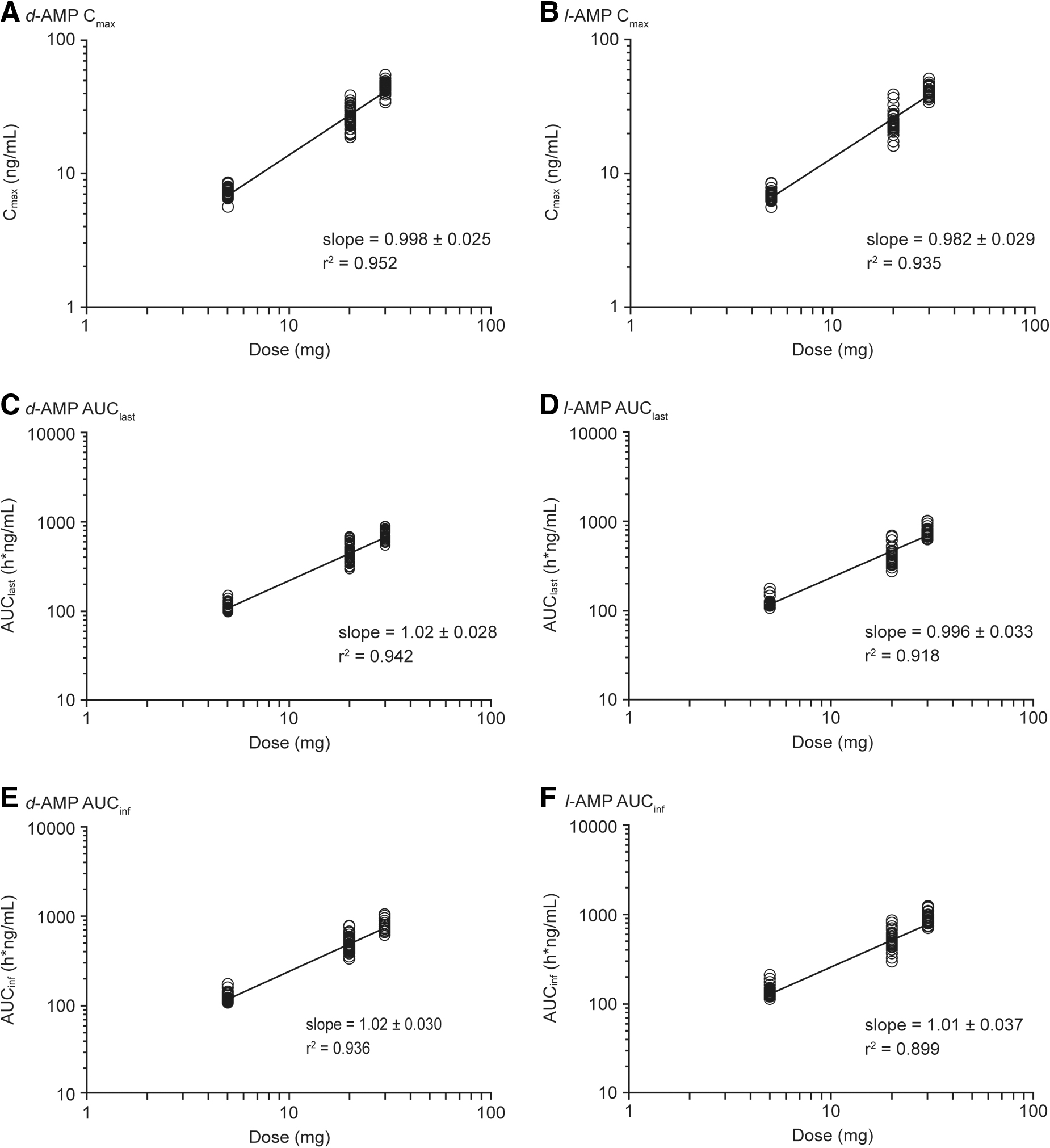
Exploratory analyses evaluated the dose-dependent relationship of PK parameters with AR19 5 and 30 mg compared with the 20-mg dose used in the bioequivalence study. The maximum and total d- and l-AMP exposures, as measured by Cmax/D, AUClast/D, and AUCinf/D, were similar to or slightly higher after AR19 5 and 30 mg compared with AR19 20 mg. Slope values from the linear regression analysis for AR19 5, 20, and 30 mg were close to 1 (ranging from 0.982 ± 0.029 to 1.02 ± 0.028), suggesting that d- and l-AMP exposure increases in a linear manner with increasing AR19 dose (Fig. 3). All PK exposure parameters were within the accepted 80%–125% range for comparative bioavailability of AR19 5 versus 20 mg and AR19 30 versus 20 mg for both d- and l-AMP (Table 4).
Linear dose proportionality of AR19 (5–30mg) for
Exploratory Statistical Analysis of d- and l-AMP Comparing AR19 (20 mg) (Bioequivalence Study) and AR19 5 Versus 30 mg (Dose Comparison Study), Dose Normalized
Geometric means for AR19 5, 20, and 30 mg based on least squares means of log-transformed parameter values.
Ratio calculated as geometric mean for AR19.
Cmax/D, AUClast/D, and AUCinf/D are calculated as log-transformed, dose-normalized values.
AMP, amphetamine; ANOVA, analysis of variance; AUCinf, area under the plasma concentration–time curve from time-zero extrapolated to infinity; AUClast, area under the plasma concentration–time curve from time-zero to the time of the last quantifiable concentration; CI, confidence interval; Cmax, peak concentration in plasma; CV, coefficient of variance; D, dose; d-AMP, dextroamphetamine; l-AMP, levoamphetamine.
Food effect—intact capsules
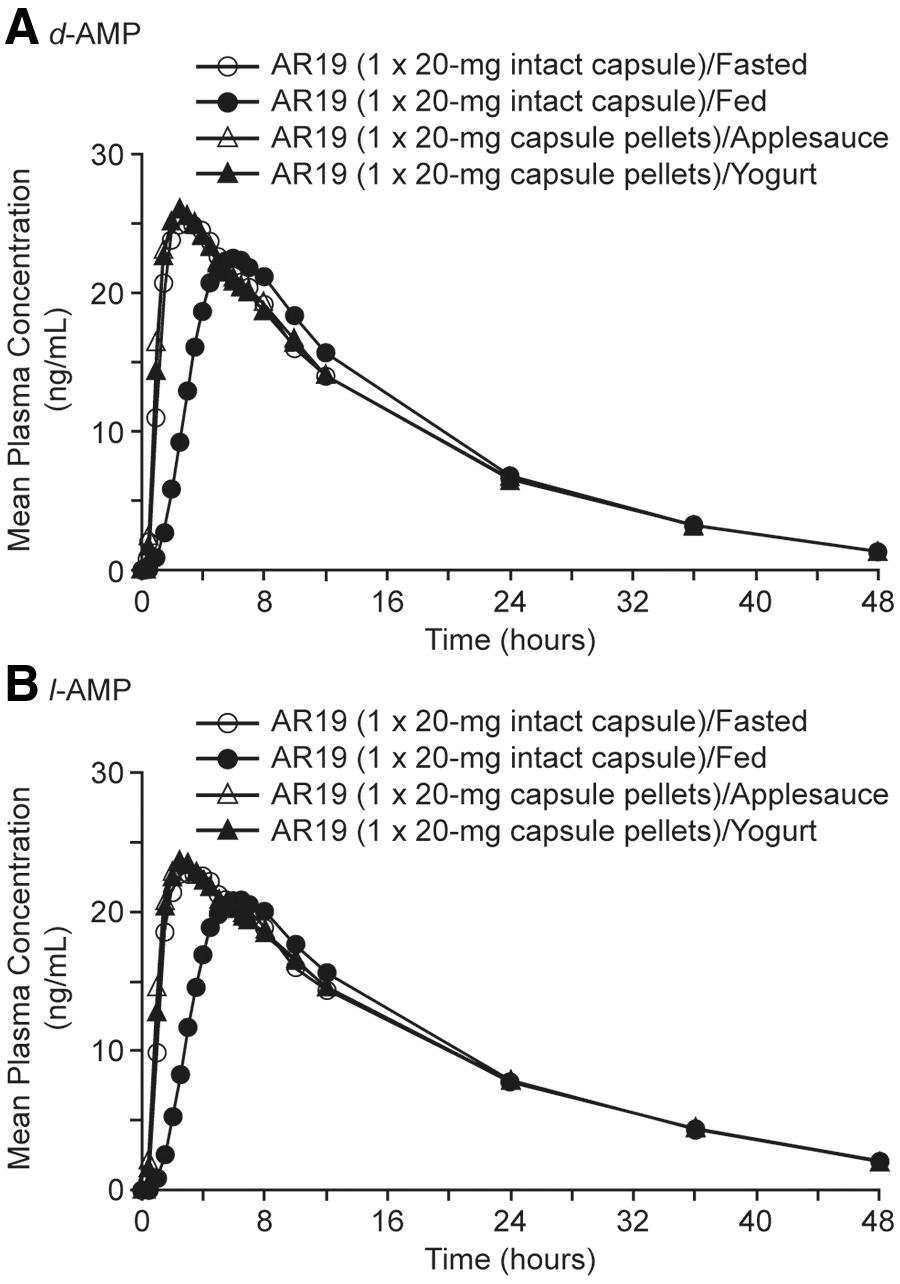
Mean plasma concentration–time data for d- and l-AMP with AR19 20 mg under fed or fasted conditions are summarized in Figure 4. There were no significant differences in overall log-transformed exposure parameters (Cmax, AUClast, and AUCinf) for d- and l-AMP comparative bioavailability with intact capsule and high-fat/high-calorie meal versus fasted (Table 5). Mean ± SD Tmax values for d- and l-AMP were higher following administration of intact AR19 capsule and high-fat/high-calorie meal (5.59 ± 1.57 and 5.59 ± 1.59, respectively) compared with the fasted condition (2.85 ± 0.76 and 2.97 ± 0.79, respectively; Fig. 4 and Table 6).
Mean plasma
Statistical Analysis of d- and l-AMP Following Administration of AR19 Intact Capsule While Fasted or With Meal Versus Sprinkled AR19 Pellets on Applesauce or Yogurt (Food Effect Study)
Geometric means based on least squares means of log-transformed parameter values.
Ratio calculated as geometric mean for AR19.
Under fed or fasted conditions, AR19 was administered as an intact capsule. AR19 was administered as capsule pellets with applesauce or yogurt.
AMP, amphetamine; ANOVA, analysis of variance; AUCinf, area under the plasma concentration–time curve from time-zero extrapolated to infinity; AUClast, area under the plasma concentration–time curve from time-zero to the time of the last quantifiable concentration; CI, confidence interval; Cmax, peak concentration in plasma; CV, coefficient of variance; d-AMP, dextroamphetamine; l-AMP, levoamphetamine.
Pharmacokinetic Parameters of d- and l-AMP Following Administration of AR19 Intact Capsule While Fasted or Fed Versus Sprinkled AR19 Pellets on Applesauce or Yogurt (Food Effect Study)
All results reported as mean ± standard deviation.
λz, elimination rate constant; AMP, amphetamine; AUCinf, area under the plasma concentration–time curve from time-zero extrapolated to infinity; AUClast, area under the plasma concentration–time curve from time-zero to the time of the last quantifiable concentration; Cmax, peak concentration in plasma; d-AMP, dextroamphetamine; h, hour; l-AMP, levoamphetamine; Tmax, time to peak concentration; T½, terminal half-life.
Food effect—sprinkled pellets
Mean plasma concentration–time data for d- and l-AMP with AR19 20 mg administered as pellets sprinkled on applesauce or yogurt or as intact capsule while fasted are summarized in Figure 4. There were no significant differences in overall log-transformed exposure parameters (Cmax, AUClast, and AUCinf) for d- and l-AMP comparative bioavailability with sprinkled AR19 pellets on applesauce or yogurt versus intact capsule while fasted (Table 5). Similar mean ± SD Tmax values for d- and l-AMP were found following administration of AR19 as pellets sprinkled on applesauce (2.57 ± 0.89 and 3.10 ± 1.69, respectively) or yogurt (2.83 ± 0.98 and 2.93 ± 1.06, respectively; Fig. 4 and Table 6).
Safety
In the bioequivalence study, 7 of 36 total participants reported 13 AEs. Four participants reported five AEs after AR19 (20 mg) administration. Six participants reported eight AEs following reference RA-AMPH administration. All 13 AEs were mild in severity. Four participants reported treatment-related AEs, including headache (n = 2), as well as palpitations, nausea, increased energy, disturbance in attention, dizziness, and psychomotor hyperactivity (each n = 1).
In the dose comparison study, 5 of 24 total participants reported nine AEs. Two participants reported four treatment-emergent AEs following AR19 (5 mg). The majority of AEs were mild in severity; however, one AE after AR19 (5 mg) was moderate in severity (pharyngitis). Three participants reported five treatment-emergent AEs following AR19 (30 mg). Five participants reported treatment-related AEs, including euphoric mood (n = 2), as well as dry mouth, asthenia, feeling jittery, dystonia, headache, and agitation (each n = 1).
In the food effect study, 8 of 36 total participants reported 20 AEs following AR19 administration. After administration of AR19 intact capsule, six participants reported 11 AEs and two participants reported 2 AEs under fasted or fed conditions, respectively. Following administration of AR19 pellets sprinkled on applesauce or yogurt, two participants reported four AEs and three participants reported three AEs, respectively. The majority of AEs were mild in severity; however, there were two AEs after AR19 (20 mg intact capsule/fasted) that were moderate in severity (hand fracture and headache). Overall, the most frequently reported AEs were palpitations (n = 3), headache (n = 3), and euphoric mood (n = 2).
There were no serious AEs, no AEs that led to study discontinuation, and no deaths in any of the three studies. No clinically significant abnormalities in vital signs, electrocardiograms, laboratory values, or physical examinations were observed.
Discussion
The current studies in their totality have established the bioequivalence of AR19 (20 mg) compared with reference RA-AMPH, as well as a similar PK profile between AR19 (5, 20, 30 mg) and reference RA-AMPH. In addition, the current studies demonstrate comparable bioavailability of AR19 20 mg when administered as an intact capsule with a meal versus fasted or as capsule pellets sprinkled on food. An exploratory analysis in the dose comparison study also assessed the dose-normalized exposure of AR19 5 and 30 mg compared with 20 mg, which suggested dose-dependent increases in d- and l-AMP with AR19 and a dose-linear effect on exposure parameters, consistent with the known linear PK profile of AMP (Markowitz and Patrick 2017). The food effect study confirmed that the presence of food did not alter the d- and l-AMP exposure parameters of intact or sprinkled AR19.
The results of the bioequivalence and dose comparison studies show that the PK properties of AR19 are not altered relative to reference RA-AMPH. Patients benefit when clinicians have an armamentarium of treatment options from which to tailor therapy to address patient needs (Markowitz and Patrick 2017). Based on the data described here, AR19 has the potential to serve as an alternative option to reference RA-AMPH, particularly among patients for whom the potential of prescription stimulant NMU is a concern, as AR19 was developed to deter manipulation for unintended routes of administration.
The AR19 food effect study showed that the high-fat/high-calorie meal with AR19 intact capsule increased Tmax of d- and l-AMP, although it had no effect on Cmax, indicating delayed absorption but similar exposure versus fasted. These results show that AR19 can be administered with or without food. The lack of food effect means patients are not limited by the need to time dose administration relative to meals (Ptacek et al. 2014). The current study suggests that the effect of food on AR19 is similar to the effect of food on the orally disintegrating tablet (ODT) formulation of RA-AMPH. A high-fat meal does not affect the Cmax and AUC of RA-AMPH ODT, but it does slightly increase the Tmax, which indicates slightly delayed absorption, as was found with AR19 (Evekeo ODT Package Insert 2019). PK studies of IR analgesics and extended-release (ER) prescription psychostimulants demonstrate similar effects of food on Tmax (Moore et al. 2015; Sikes et al. 2017). IR analgesics demonstrate delayed absorption when administered with a meal, yet, no overall differences in bioavailability (Moore et al. 2015). Likewise, ER AMP administered under fed versus fasted conditions shows generally unaltered PK aside from lower early exposure and later peak plasma concentrations under fed versus fasted conditions (Sikes et al. 2017). A different ER AMP formulation administered with a breakfast meal resulted in reduced AMP plasma concentrations, demonstrating potential for clinically significant effects of a meal on drug bioavailability (Auiler et al. 2002).
In the AR19 food effect study, there were no significant alterations in d- and l-AMP bioavailability when AR19 was administered as pellets sprinkled on food. This is consistent with a study on an ER formulation of mixed AMP salts that found no significant differences in the PK of AMP when sprinkled on food or swallowed whole (Tulloch et al. 2002). Likewise, sprinkling capsule pellets of modified-release IR/ER and ER formulations of prescription methylphenidate has been shown to have no clinically significant effects on drug bioavailability (Pentikis et al. 2002; Lee et al. 2003; Liu et al. 2019). To the best of our knowledge, the current study is the first to evaluate the effect of sprinkling drug pellets on food on the PK of IR AMP.
AR19 was well tolerated, and AEs were similar across all three studies. The safety of AR19 20 mg is comparable to the safety of reference RA-AMPH, which has been previously established to be associated with only mild treatment-emergent AEs (Childress et al. 2015).
A limitation of the bioequivalence and dose comparison studies is that they were separate studies and were not conducted in parallel, which may explain the increased least squares geometric mean ratios with the dose comparisons of AR19 5 mg with 20 mg, and 20 mg with 30 mg. The increase in least squares geometric mean ratios compared with the values reported for comparisons of AR19 20 mg with reference RA-AMPH was likely due to variation in study participants between the bioequivalence and dose comparison studies.
A limitation of the food effect study is the age group tested, as children and adults may have different rates of gastric emptying that could alter drug PK when administered with food (FDA 2002). On the contrary, a meta-analysis found that meal type, and not age, was a significant factor in the rate of gastric emptying (Bonner et al. 2015).
Further study of AR19 would seek to evaluate if it may deter manipulation that could lead to nonoral routes of administration. However, it should be noted that despite formulation advancements, the potential risk for dependence with any prescription stimulant remains.
The PK parameters of AR19 show bioequivalence to reference RA-AMPH when administered orally, as intended, and demonstrate that it may be taken with a meal or sprinkled on food. The food effect study demonstrates the potential for flexibility in the dosing schedule, allowing patients to take AR19 with meals or by opening the capsule and sprinkling on food.
Conclusions
The AR19 formulation designed to deter manipulation for nonoral routes of administration is bioequivalent to reference RA-AMPH when administered as a 20-mg dose in healthy participants. Overall, the presence of a high-fat/high-calorie meal with intact AR19 capsule or the sprinkling of AR19 capsule contents on applesauce or yogurt did not alter d- and l-AMP bioavailability from an intact capsule. AR19 was well tolerated by healthy participants when administered as 5, 20, or 30-mg doses.
Clinical Significance
The current studies identify the potential for use of AR19 in the treatment of patients with ADHD. AR19 is an investigational IR formulation of IR racemic AMP that was designed to reduce individuals' ability to manipulate and extract the active pharmaceutical ingredient for unintended routes of administration. AR19 demonstrates comparable bioequivalence to reference RA-AMPH across a range of doses, highlighting its use as an alternative treatment strategy with similar IR action. As AMP exposure and bioavailability from AR19 are not affected by administration with a meal or when sprinkled on food, AR19 may be a desirable candidate for ADHD patients who desire to take their medication with a meal or sprinkled on food, particularly for patients who may be at risk for nonoral prescription stimulant NMU.
Footnotes
Acknowledgments
The study sponsor and authors are grateful to the participants who took part in the studies. Statistical consultants: support from employees of Worldwide Clinical Trials led by Xu Wen (bioequivalence and dose comparison) and Sarah Andrews (food effect).
Disclosures
S.C. and T.S. are employees of Arbor Pharmaceuticals, LLC. Both authors analyzed and interpreted the study data, critically reviewed the drafts, and approved the final version for submission. Writing and editing assistance was provided by Caryne Craige, PhD, and Sarah Thornburg, MS, of Fishawack Communications, Inc.