
Abstract
Objective:
To examine parent's perceptions of deep brain stimulation (DBS) and whether DBS is perceived to be a viable and safe treatment for their adolescent child presenting with a severe, treatment-resistant neurological or psychiatric condition.
Method:
Two hundred and seventy-nine parents completed an online survey using Amazon Mechanical Turk (MTurk). Participants were presented with five vignette scenarios involving adolescents with severe, treatment-resistant neurological or psychiatric conditions: Rett syndrome, autism spectrum disorder, epilepsy, obsessive-compulsive disorder, and Tourette syndrome. Parents were then asked to evaluate each scenario and rate overall acceptability of using DBS to improve their child's core symptoms. Data were collected over a period of 2 weeks in the month of October 2018.
Results:
We found that parents reported favorable impressions of DBS regardless of the target condition, especially when greater improvement could be assured and when their child had the capacity to assist in the treatment decision-making. Parents indicated some reluctance to use DBS when possible safety concerns were present. Familiarity with DBS was directly associated with attitudes.
Conclusions:
The findings highlight an overall parental willingness to consider DBS as a treatment option for key symptoms of neurological and psychiatric conditions in adolescents.
Introduction
As deep brain stimulation (DBS) has demonstrated efficacy and become more common in treating an array of neurological disorders in adults (e.g., Parkinson's disease, essential tremor, epilepsy), patients of younger ages have been studied with promising results in movement disorders (Marks et al. 2009; Hale et al. 2018; Yan et al. 2018; Elkaim et al. 2019). DBS is offered under an Food and Drug Administration (FDA) Humanitarian Device Exemption for children (≥7 years old) with intractable dystonia (no age limit in Europe), and there are numerous clinics and research studies conducting DBS in children with Tourette syndrome, dystonia, and other movement disorders (Marks et al. 2009; Lipsman et al. 2010; Haridas et al. 2011; Cif and Coubes 2017; Yan et al. 2018).
As invasive neuromodulation technologies and safety both advance, it is foreseeable that their use in children and adolescents with intractable psychiatric and neurological conditions will increase. However, thus far no studies have empirically examined whether the use of invasive neuromodulation (i.e., DBS) in children and adolescents is deemed acceptable by parents. Invasive neuromodulation in young people raises a number of clinical and ethical concerns that could limit parental acceptability regarding the use of DBS (Johnco and Storch 2016; Zuk et al. 2018). A recent study examined parents' perceptions of transcranial direct current stimulation (tDCS; a noninvasive neuromodulation treatment) among children and adolescents (Wagner et al. 2018). Recruited from an online forum, 227 adults (only 38% were parents) responded on whether they would be willing to use tDCS with children for a variety of indications. Most of the sample would not use tDCS to enhance cognitive capacity, although rates differed as a function of the child's capacity (i.e., capacity was inversely related to willingness). A significant portion of respondents (58%) were willing to consider tDCS if their child's mood was below average. Respondents were generally not in favor of bans against improving youngsters' mood if below average, but only if the intervention was deemed safe and in the best interests of the child. Modest concern was expressed about safety, use of tDCS for means that do not serve the self-interests of the child, and unease about the unnaturalistic aspect of cognitive enhancement. Parents were more negative toward tDCS than nonparents.
While these data help us to begin understanding parental attitudes toward the use of neurotechnologies in children, tDCS is a noninvasive intervention, and enhancement differs greatly from the use of invasive neurotechnologies (e.g., DBS) for managing treatment-resistant disorders in minors. For example, there is a dearth of safety and effectiveness data in minors; a possibility that minors may outgrow the symptoms without invasive neuromodulation; concerns about whether the risks of neurosurgery are worth the potential, sometimes uncertain, benefits; uncertainty regarding how to adequately balance the interests of caregivers, children, and clinicians when considering pediatric DBS; and limited information on the potential impact of DBS on personal identity in adolescents at a sensitive stage of identity development. In this study, we examined parents' perceptions of DBS and whether they consider DBS to be a viable and safe treatment for their adolescent child presenting with one of five severe, treatment-resistant neurological or psychiatric conditions; Rett syndrome, autism spectrum disorder, epilepsy, obsessive-compulsive disorder, and Tourette syndrome.
Method
Participants
Participants were recruited online through Amazon Mechanical Turk (MTurk). MTurk is a web-based crowd-sourcing service that allows businesses, institutions, or entities to distribute small jobs called human intelligence tasks (HITs) to a large pool of workers. Most tasks involve the completion of surveys in exchange for monetary compensation. In the present study, parents older than the age of 18 years and who spoke English proficiently were recruited. Workers who met these qualifications and had an MTurk approval rating greater than 95% (indicating 95% of previous MTurk tasks were appropriately completed) were accepted to complete the HIT. Workers were compensated $2.50 in exchange for the successful completion of the survey. Data were collected over a period of 2 weeks in the month of October 2018, with a total of 379 participants completing the questionnaire.
Procedures
All procedures were approved by the Institutional Review Board at Baylor College of Medicine. After clicking on the MTurk HIT, participants were directed to an external online survey link and were presented with the Institutional Review Board's approved consent document, in which consent was implied by participation. Online administration of the questionnaire battery followed. Data were cleaned to clear any possible invalid, duplicate or careless responding, resulting in exclusion of 100 (26.4%) participants. Seventeen participants did not meet inclusion criterion (i.e., no children). Twenty-nine participants had extremely fast response times indicating careless responding (those in the 10th percentile of response speed, spending less than 5 minutes completing the survey). Fifty participants were excluded for misrepresentation, such as providing falsified or plagiarized data from online sources (e.g., Wikipedia). Finally, four participants were excluded from analysis for missing responses (i.e., three did not respond to any items regarding attitudes toward other treatments; one did not respond to any items regarding DBS acceptability). This left a final sample for study analysis that consisted of 279 (73.6% of the sample) parents, 24–68 years old (M = 35.47; SD = 9.09). Participants were 58% male and 75% Caucasian, with 90% reporting at least some college education. Demographic characteristics of the final study sample are presented in Table 1.
Demographic Characteristics and Overall Acceptability of Deep Brain Stimulation Reported by the Present Sample
Means and standard deviations were reported for continuous variables, and counts and relative percentages were reported for categorical variables.
GED, general educational development test.
Survey instrument
The 30-minute self-report questionnaire battery was created in Qualtrics (2014) for the purpose of the present study. The survey was divided into two parts. First, parents completed basic demographic questions (e.g., respondents' gender, age, race, number of children, age of children, employment, and so on). Parents were then asked to rate their comfort with using six treatments other than DBS (i.e., antidepressants, psychotherapy, alternative medicine, electroconvulsive therapy, self-help, and residential/hospitalization) to treat neurological and psychiatric symptoms in their child. Responses were 0 (extremely uncomfortable), 1 (moderately uncomfortable), 2 (slightly uncomfortable), 3 (neither comfortable nor uncomfortable), 4 (slightly comfortable), 5 (moderately comfortable), or 6 (extremely comfortable). Preexisting knowledge and familiarity with DBS was then assessed (0 = No, never heard of it, 1 = Yes, I have heard of it, but am not familiar with DBS, or 2 = Yes, I have heard of it, and am familiar with DBS).
For the second part of the survey, respondents completed the vignette-based DBS acceptability measure (Supplementary Data S1). This measure was developed based on existing literature (Patel et al. 2016; Wagner et al. 2018) and expertise of study authors. Respondents were first presented with an introductory paragraph describing DBS, which was then followed by five vignette scenarios involving adolescents with severe, treatment-resistant neurological or psychiatric conditions, and identifying a core symptom that would be the target of DBS. The conditions (and core symptoms) were Rett syndrome (movement control), autism spectrum disorder (self-injurious behavior and self-harm), epilepsy (seizures), obsessive-compulsive disorder (OCD symptoms), and Tourette syndrome (tics). Beyond the severity of each condition, these disorders were chosen either because DBS is currently taking place for pediatric patients (e.g., Tourette, epilepsy) and adult patients (e.g., OCD, autism spectrum disorder) and/or could be a potential target (e.g., Rett). Participants were asked to evaluate each scenario imagining that their child had the described condition and to then rate overall acceptability of using DBS to improve their child's symptoms. Acceptability ratings were captured on an 11-point Likert scale ranging from 0 (Totally Unacceptable) to 10 (Totally Acceptable). In addition, for each vignette scenario, respondents were asked to indicate whether they agreed or disagreed with five statements relating to treatment acceptability (Supplementary Data S1). Statements were rated using a 5-point Likert scale, ranging from 0 (strongly disagree) to 4 (strongly agree).
Analytic plan
Responses from the comfort with treatments for neurological and psychiatric symptoms were combined and averaged for analysis as the item pairs were strongly correlated (rs ranged from 0.77 to 0.87, ps < 0.001). Multiple regressions were conducted for each disorder to examine whether preexisting comfort with alternative methods of treatment predicted overall acceptability of DBS for the disorder. Results are displayed in Table 2.
Comfort with Alternate Treatment Methods: Descriptive Data and Regression Results from Prediction of Deep Brain Stimulation Acceptability by Comfort with Different Treatment Methods for Psychological and Neurological Disorders
ASD, autism spectrum disorder; OCD, obsessive compulsive disorder; Rett, Rett syndrome; Tourette, Tourette syndrome.
Next, t-tests were used to examine potential differences in DBS acceptability for each disorder between participants previously familiar with DBS and those who were not. For this analysis, the few participants who responded “Yes, I have heard of it, and am familiar with DBS” (n = 21) were combined with participant who responded, “Yes, I have heard of it, but am not familiar with DBS” (n = 189) and compared to the group who responded that they had never heard of DBS (n = 68). Results are displayed in Table 3.
Comparisons Between Parents With and Without Preexisting Knowledge of Deep Brain Stimulation on Deep Brain Stimulation Acceptability Ratings
ASD, autism spectrum disorder; DBS, deep brain stimulation; OCD, obsessive compulsive disorder; Rett, Rett syndrome; Tourette, Tourette syndrome.
Chi-square tests for goodness of fit were conducted to determine if item agreement rates differed among the options available for each individual willingness item. Willingness items B, C, and D specifically examine enthusiasm for DBS based on prospective benefits and child decision-making capacity. To examine differences in response patterns based on the differential item content across these items, chi-square tests for independence were conducted (three items by five response categories). To examine differences in overall acceptability scores across disorders, an omnibus test of group means was conducted via multigroup structural equation modeling, using robust maximum likelihood estimation (directly analogous to a robust analysis of variance procedure) and pairwise group comparisons were conducted using Wald tests. Multigroup structural equation models were implemented using Mplus Version 8 (Muthén and Muthén 2017), and chi-square and regression analyses were conducted using R version 3.5.1 (R Core Team 2015), with chi-square-based analyses conducted using the package “rcompanion” (Mangiafico 2016) and regressions using the R package “lavaan” (Rosseel 2012).
According to criteria provided by Cohen (1988), correlations of 0.1, 0.3, and 0.5 represent small, medium, and large effect sizes, respectively. We used these anchors to evaluate effect size results from the 3 × 5 chi-square tests for independence, which were reported in the correlational analog of Cramer's V. For each set of analyses, multiple comparisons were addressed using the false discovery rate (FDR) method (Benjamini and Hochberg 1995).
Results
Willingness to consider DBS: individual items
Response patterns for each individual willingness item evaluated can be found in Figure 1. On average, parents reported high overall acceptability ratings for DBS treatment across all disorders. The willingness to use DBS was endorsed more strongly when the proposed benefits of treatment were more favorable for all disorders. Significant differences in response patterns within each individual item were also observed for each item regarding each disorder (Supplementary Table S1), indicating that parents showed significant preferences regarding willingness to engage in DBS for all items.
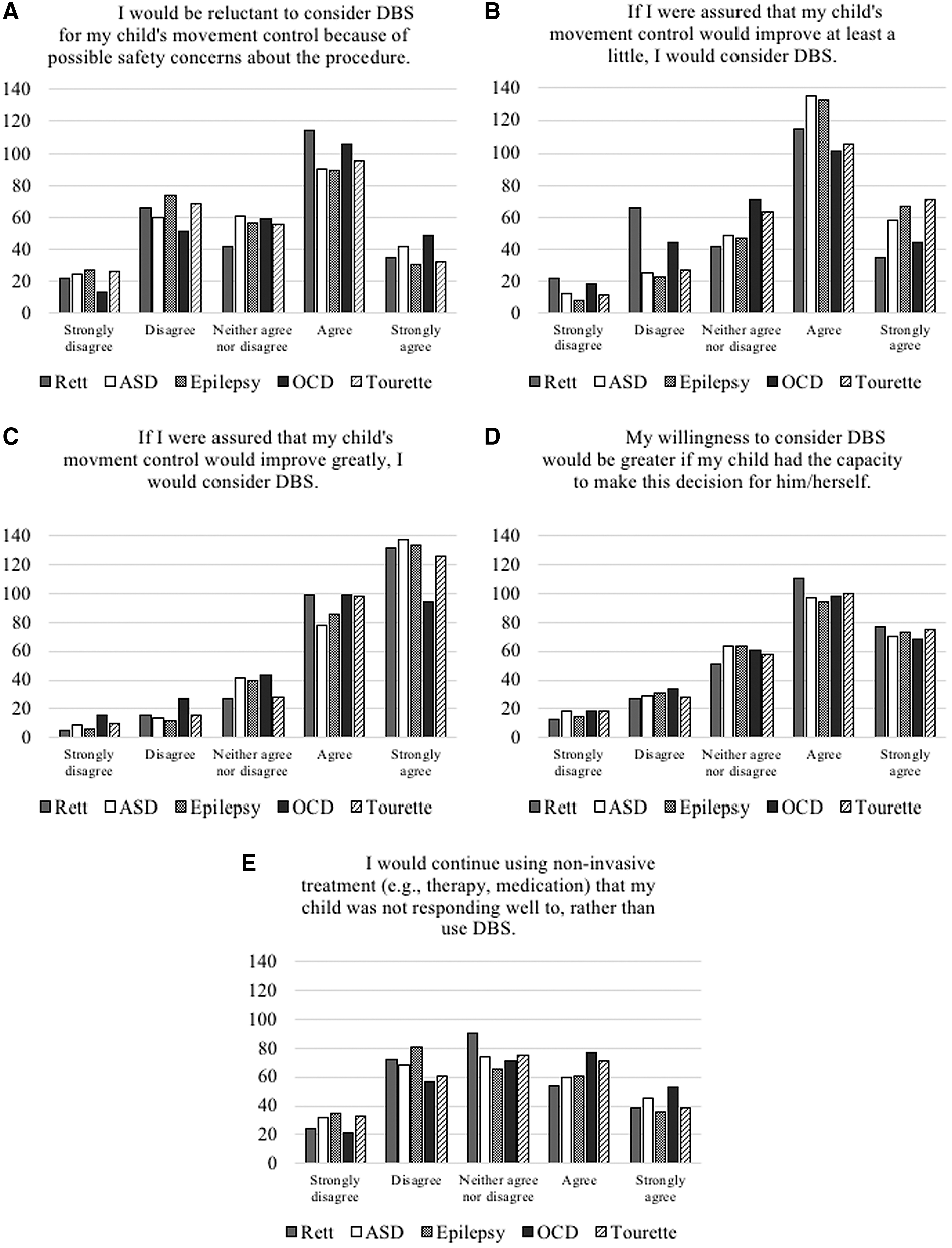
On average, parents demonstrated willingness to use DBS for the treatment of all evaluated disorders if they were assured that treatment outcome would improve “a little” (item B) or “greatly” (item C), or if their children were able to make the treatment-engagement decision for themselves (item D). Parents reported some reluctance to use DBS when there were possible safety concerns (item A). Parents also showed some ambivalence regarding continued use of ineffective noninvasive treatments in lieu of DBS (item E), with some showing preference to continue previously ineffective treatments, while others disagreed with this approach.
Willingness to consider DBS: differences across items
Significant differences in willingness to consider DBS (items B, C, and D) across items were found for all disorders evaluated, including Rett syndrome (p < 0.001, Cramer's V = 0.203), autism spectrum disorder (p < 0.001, Cramer's V = 0.206), epilepsy (p < 0.001, Cramer's V = 0.191), obsessive-compulsive disorder (p < 0.001, Cramer's V = 0.133), and Tourette syndrome (p < 0.001, Cramer's V = 0.182). This reflects that the level of willingness to engage in DBS differed as a result of the degree to which symptoms would “improve greatly” in comparison to “at least a little.” The level of this difference across items was in the small to small-medium range for all disorders evaluated.
Overall acceptability of DBS: differences across disorders
Comparisons of model-estimated means found that overall acceptability of DBS treatment ratings (rated 0–10) were significantly lower for obsessive-compulsive disorder (M = 7.35, SD = 3.32) than acceptability scores for Rett syndrome (M = 8.42, SD = 2.52, p < 0.001), autism spectrum disorder (M = 8.38, SD = 2.75, p < 0.001), epilepsy (M = 8.68, SD = 2.43, p < 0.001), and Tourette syndrome (M = 8.37, SD = 2.73, p < 0.001). Despite these differences, on average, DBS was rated as acceptable for all disorders. No other differences in acceptability were observed across disorders when controlling for the FDR.
Relationship of overall acceptability of DBS and parental comfort with different treatment approaches
Results from analyses assessing the relationship between overall acceptability of DBS and parental comfort with different treatment approaches for psychiatric and neurological symptoms can be found in Table 2. Average comfort with different treatments for pediatric psychiatric or neurological symptoms were relatively low, ranging from 1.46 for electroconvulsive therapy (ECT) (moderately to slightly uncomfortable) to 4.35 for self-help (slightly comfortable) on average on a 0 to 6 scale. Comfort with treatment was particularly low for ECT, residential/hospitalization, and antidepressant/psychoactive medication treatments. Parental comfort with antidepressant treatment for psychiatric and neurological symptoms was positively associated with overall acceptability of DBS for Rett syndrome (p < 0.001, β = 0.20) and obsessive-compulsive disorder (p < 0.007, β = 0.21). Parental comfort with ECT was negatively associated with overall acceptability of DBS for epilepsy (p < 0.001, β = −0.31).
Differences in DBS acceptability ratings based on preexisting DBS knowledge
Results from analyses comparing DBS acceptability ratings for each disorder by whether parents reported preexisting knowledge of DBS are displayed in Table 3. Significant small differences between knowledge groups were found for Rett syndrome, t(253) = 2.90, p = 0.004, g = 0.41; autism spectrum disorder, t(254) = 3.22, p = 0.001, g = 0.45; OCD, t(252) = 2.56, p = 0.011, g = 0.36; and epilepsy, t(250) = 2.01, p = 0.045, g = 0.29, indicating that preexisting knowledge of DBS significantly predicts acceptability of using DBS for these disorders. However, no significant difference was found between groups for Tourette syndrome, t(252) = 0.73, p = 0.464, g = 0.11.
Discussion
The current study examined parents' perceptions of DBS. The online survey presented vignettes for five treatment-resistant conditions in adolescents, and asked parents whether they considered DBS to be an acceptable treatment for their child if she/he were to have one of these conditions. Overall, parents reported favorable impressions of DBS for all disorders, especially in situations where greater improvement could be assured and when their child had the capacity to assist in the treatment decision-making. Unsurprisingly, parents indicated some reluctance to use DBS when possible safety concerns were present.
When asked about potential treatment options for their own child, parents were largely ambivalent, reporting not being highly comfortable or uncomfortable with most of the alternative options provided. Parents were more decidedly uncomfortable with the most physically invasive or restrictive treatments (i.e., ECT, psychoactive medications, residential/hospitalization) and comfortable with the least invasive (i.e., self-help). After being asked to imagine being the parent of a child with a specific psychiatric or neurological disorder, parents on average reported very high levels of acceptability of DBS as a treatment for the child's symptoms. In nearly all cases, the previously reported comfort or discomfort with alternative treatments did not affect acceptability of DBS. Moreover, parents who reported having preexisting knowledge of DBS were on average significantly more accepting of DBS as a treatment for all disorders except Tourette syndrome. It appears that familiarity and knowledge of DBS is associated with increased acceptability of the procedure. This might have some implication for the dissemination of DBS. Exposing parents to DBS as a viable treatment option for these disorders in multiple contexts may increase their likelihood to consider DBS for their child. However, the level of familiarity of DBS was not assessed, with most parents reporting that they had at least heard of the procedure. Thus, while knowledge of DBS appears to increase acceptability, the data from the current study do not allow for a more granular understanding of what level of knowledge is required to impact acceptability. Further research is needed to better understand these initial findings.
Comfort with antidepressant treatment was associated with increased acceptability of DBS for Rett syndrome, OCD, and epilepsy. Interestingly, parents who expressed comfort with ECT were significantly less likely to endorse acceptability of DBS for epilepsy, even though DBS is an FDA-approved treatment for adults with refractory epilepsy, perhaps parents view ECT as a less invasive alternative to DBS. Comfort with all other alternative treatments did not indicate increased acceptability of DBS for any disorder.
On average, parents reported similarly high levels of willingness to consider DBS as a treatment for adolescents with any of the psychiatric or neurological conditions if assurance could be made of some level of improvement. Although still high on average, levels of acceptability and willingness to consider DBS as a treatment for OCD were significantly lower than the other disorders. This might be due to parents perceiving OCD as less of a brain-based disorder in need of neurological intervention and more of an environmentally controlled disorder in need of a cognitive behavioral intervention compared to the other disorders.
The present findings increase our understanding of parent perception of DBS as a treatment for different disorders. However, there are study limitations to be considered when interpreting the findings. Participants were recruited using MTurk and remote data collection may result in increased inattentive responding, although efforts were made to screen inattentive responders out of the data. In addition, research indicates that MTurk collected data to be similar to, and with regard to diversity perhaps superior to, more traditional data collection methods (Casler et al. 2013). While all participants were parents, few, if any likely had children with severe manifestations of these disorders and thus were asked to imagine having a child with a disorder to answer the questions. The study thus represents attitudes toward DBS in the general public. However, the extent to which these attitudes extend to parents of children with these disorders is yet to be established, and should be the focus of future research, along with disorder-specific features that may be related to DBS acceptability.
In general, the findings indicate overall high levels of parental willingness to consider DBS as a treatment option for key symptoms of Rett syndrome, autism spectrum disorder, epilepsy, Tourette syndrome, and OCD in adolescents. It appears that past familiarity with DBS might increase the likelihood of parents to consider DBS as a treatment option for their child. Thus, efforts should be made to increase awareness of DBS for those conditions for which it is considered safe and effective.
Conclusion
Overall, in a sample of 279 parents who completed an online survey, respondents reported favorable impressions of DBS regardless of the target condition. This was particularly the case when greater improvement could be assured and when their child had the capacity to assist in the treatment decision making. There was some evidence that acceptability differed as a function of disorder with ratings of acceptability being lower for OCD relative to other conditions assessed. Parents indicated some reluctance to use DBS when possible safety concerns were present. Finally, pre-existing knowledge of DBS significantly predicted acceptability of using DBS for varied disorders.
Clinical Significance
As DBS has demonstrated efficacy and become more commonplace in treating an array of neurological disorders in adults (e.g., Parkinson's disease, essential tremor, epilepsy), patients of younger ages have received this procedure with promising results in movement disorders. However, there has been limited work examining parents' perceptions of DBS and whether they consider DBS to be a viable and safe treatment for adolescents with impairing symptomology. Our study findings highlight an overall parental willingness to consider DBS as a treatment option for neurological or psychological conditions in adolescents. Data also suggest that past familiarity with DBS might increase the likelihood of parents to consider DBS as a treatment option for their child. Thus, efforts should be made to increase awareness of DBS for those conditions for which it is considered safe and effective.
Footnotes
Acknowledgments
We acknowledge the contributions of Wayne Goodman. We also thank an anonymous donor for generously providing funding for this project. The views expressed are those of the authors alone, and do not necessarily reflect views of the NIH, Texas State University, or Baylor College of Medicine.
Contributors
All authors confirm that the final version of the article has been read and approved and that there are no other persons who satisfied the criteria for authorship but are not listed. All authors further confirm that the order of authors listed in the article has been approved by all.
Disclosures
Dr. Storch receives research support from NIH, International OCD Foundation, Greater Houston Community Foundation, Texas Higher Education Coordinating Board, and the American Red Cross. He has received royalties from Elsevier Publications, Springer Publications, American Psychological Association, Wiley, Inc., and Lawrence Erlbaum. Dr. Storch is on the Speaker's Bureau and Scientific Advisory Board for the International OCD Foundation. Dr. Schneider received grant funding from the Texas Higher Education Coordinating Board and the American Red Cross. Dr. Sheth is a consultant for Boston Scientific, Medtronic, Koh Young, Theracle, and Zimmer. All other authors report no financial disclosure. We report no other potential conflicts of interest.
Supplementary Material
Supplementary Data S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.