
Abstract
Objective:
Although methylphenidate and atomoxetine have positive effects in reducing core symptoms and emotional/behavioral problems of attention-deficit/hyperactivity disorder (ADHD), little is known about their efficacy in improving social adjustment problems among youths with ADHD.
Methods:
A total of 168 drug-naive youths, 7–16 years of age, with DSM-IV-defined ADHD, were recruited and randomly assigned to osmotic-release oral system methylphenidate (n = 83) and atomoxetine (n = 85) in a 24-week, open-label, head-to-head clinical trial. Efficacy measurement was based on the parent-rated and self-rated Social Adjustment Inventory for Children and Adolescents (SAICA). Evaluation time points were set at baseline and weeks 8, 16, and 24.
Results:
At week 24, methylphenidate was associated with improvement in school functions (parent report: Cohen d = −0.82; self-report: Cohen d = −0.66) and peer relationships (parent report: Cohen d = −0.50; self-report: Cohen d = −0.25); and atomoxetine was associated with improvement in school functions (parent report: Cohen d = −0.62; self-report: Cohen d = −0.34) and peer relationships (parent report: Cohen d = −0.33; self-report: Cohen d = −0.65). In terms of parent-reported and self-reported ratings, there were no significant differences between the two treatment groups in mean reduction in the severity of school dysfunctions, impaired peer relationships, and behavioral problems at home at week 24.
Conclusions:
Our findings lend evidence to support that both methylphenidate and atomoxetine were comparably effective in improving social adjustment in youths with ADHD, including school functions and peer relationships.
Introduction
Attention-deficit/hyperactivity disorder (ADHD), characterized by the core symptoms of inattention, hyperactivity, and impulsivity, is a neurodevelopmental disorder with an evident neurobiological basis (Volkow et al. 2005; Shang et al. 2013). The presence of ADHD in youths is associated with significant functional impairments in a variety of life domains, including disrupted parent/child relationships (Gau 2007), peer rejection (Kawabata et al. 2012), behavioral problems at home (Gau 2007), and poor academic performance (Barbaresi et al. 2007). For example, children with ADHD are less well liked, and more often rejected by their classmates in school settings (Hoza et al. 2005b). Children with ADHD were reported by their parents to have fewer close friendships and more peer rejections (Bagwell et al. 2001). Difficulty in social adjustment has been found in children with ADHD as early as during preschool years (DuPaul et al. 2001), and previous studies have shown the links of early social disability with increased emotional/behavioral problems and global impairments (Mrug et al. 2012). Given that poor social adjustment may have crucial influence on the short-term and long-term prognosis of patients with ADHD, identifying these problems is of significant importance not only for assessment of the current difficulties in daily life but also for prevention from adverse outcome (Nijmeijer et al. 2008). Hence, the social functional impairments have been recognized as essential reasons for clinical referral and treatment (Waxmonsky et al. 2010; Chou et al. 2018).
Methylphenidate and atomoxetine are widely used in the treatment of ADHD. Previous studies have demonstrated the comparable effectiveness of methylphenidate and atomoxetine in improving the ADHD symptomatology (Shang et al. 2015; Briars and Todd 2016), emotional/behavioral problems (Shih et al. 2019), and neuropsychological functions (Ni et al. 2013).
As parents frequently seek treatment for impaired social adjustment and school functions of their children with ADHD (Bussing et al. 2005; Charach et al. 2006; Gau et al. 2010), it is crucial to assess the medication effects on these domains of life. Previous studies have shown mixed results for the effectiveness of methylphenidate and atomoxetine in improving the social adjustment in patients with ADHD. For example, treatment with methylphenidate is associated with improving social interactions, including decreasing negative reciprocal social interactions initiated or directed toward the treated children with ADHD (Abikoff et al. 2004). Significant improvements in social functioning (Wender et al. 2011) and academic performance (Evans et al. 2001) have been reported in ADHD patients with methylphenidate treatment. In contrast, the multimodal treatment study of ADHD shows that impaired peer relationships remain in those subjects receiving the 14-month treatment with psychostimulants (Hoza et al. 2005a). A systemic review of long-term treatment with medications treating ADHD reveals little evidence for improvement in academic performance with psychostimulant treatment (Schachar et al. 2002). Similarly, several studies show significant associations of atomoxetine treatment with functional improvements in social skills (Waxmonsky et al. 2010). Significant effectiveness of atomoxetine has been reported in improving grades (Bakken et al. 2008; Wietecha et al. 2009) and school interactions (Waxmonsky et al. 2010). However, some trials document a minimal effect on academic performance and prosocial behavior after treatment with atomoxetine (Weiss et al. 2005; Brown et al. 2006). Given the significant variations in study design, samples, and measures across psychopharmacological studies, further clinical trials are needed to examine the effectiveness of methylphenidate and atomoxetine in improving the social adjustment in patients with ADHD.
The area of social problems in patients with ADHD is relatively understudied, which may be due to a paucity of useful assessment tools (Nijmeijer et al. 2008). The Social Adjustment Inventory for Children and Adolescents (SAICA) is a validated and reliable instrument to assess social adjustment in different environments and interactions with parents, siblings, and peers (John et al. 1987). However, only a few studies have used the SAICA to measure the effects of methylphenidate or atomoxetine in the social adjustment in patients with ADHD. For example, an early observation study shows that treatment with methylphenidate is associated with less severe problems at school and better academic performance measured by the SAICA (Gau et al. 2006). In a single-arm, open-label, 8-week study to investigate the effectiveness of switching from immediate-release (IR)-methylphenidate to osmotic-release oral system (OROS)-methylphenidate in children with ADHD, the school function, peer relationships, and home behaviors of the SAICA subscales improve significantly after switching the medication (Chou et al. 2018). A naturalistic observation study has shown that OROS-methylphenidate is superior to IR-methylphenidate in children with ADHD in terms of improvement in problems with peers and social behavior in school assessed by the SAICA (Tzang et al. 2012). Atomoxetine has also been reported to be effective in improving the scores of the school functioning subscale of the SAICA in children with ADHD, including grades, school interaction, and school behavioral problems (Shang and Gau 2012). Further information indicating whether methylphenidate and atomoxetine have comparable efficacy in reducing the social dysfunctioning in patients with ADHD is still required.
To our best knowledge, no direct comparative trial has been conducted to examine the differential therapeutic effects of methylphenidate and atomoxetine on the social dysfunctioning in patients with ADHD. Longitudinal studies are essential to comprehensively investigate the treatment outcomes of social adjustment in ADHD (Nijmeijer et al. 2008). The present head-to-head, open-label, 24-week randomized clinical trial aims to directly compare the effectiveness of long-term treatment with methylphenidate and atomoxetine in improving social adjustment problems in drug-naive youths with ADHD.
Methods
Participants
Drug-naive participants, 7–16 years old, who met the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) diagnostic criteria for ADHD (American Psychiatric Association 1994), were recruited from the National Taiwan University Hospital. We used the Chinese version of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiological Version (K-SADS-E) to confirm their ADHD and another psychiatric diagnosis (Gau et al. 2005). The Chinese K-SADS-E has been proven to be a reliable and valid instrument to assess child psychiatric disorders and has been used extensively in a variety of studies regarding childhood mental disorders in Taiwan (Shang et al. 2013, 2016, 2017; Chiang et al. 2015, 2016, 2019; Chou et al. 2015; Gau et al. 2015; Lin et al. 2015). Participants were excluded if they had comorbid psychiatric conditions, including psychosis, bipolar disorders, autism spectrum disorders, substance use disorders, intellectual disability (full-scale intelligence quotient <80), or had a history of major medical or neurological problems; or had ever used psychotropic medications before the study. The details about the study participants have been reported elsewhere (Shang et al. 2015; Shih et al. 2019). Part of this head-to-head randomized clinical trial has been published regarding the symptom changes (Shang et al. 2015) and improvement in emotional and behavioral problems (Shih et al. 2019).
Procedures
The present study was approved by the Research Ethics Committee of National Taiwan University Hospital, Taiwan, before implementation (IRB ID, 200812153M;
Based on computer-generated random sequence, participants were randomly assigned to either the OROS-methylphenidate group or the atomoxetine group at a 1:1 ratio in this 24-week, open-label, head-to-head randomized clinical trial. All the participants would receive seven assessments: at baseline (visit 1), week 2 (visit 2), week 4 (visit 3), week 8 (visit 4), week 12 (visit 5), week 16 (visit 6), and week 24 (visit 7). After being assessed at baseline, they started to take the medication with OROS-methylphenidate (an initial dosage of 18 mg/day, administered as a single morning dose) or atomoxetine [an initial dosage of 0.5 mg/(kg·d), administered as once-daily dose]. The dosage of methylphenidate and atomoxetine would be titrated at visits 2–7 (weeks 2–24) according to clinical response and adverse effects. The maximum daily dosages of methylphenidate and atomoxetine were 54 mg daily and 1.2 mg/kg daily, respectively. Bodyweight, body height, and blood pressure were assessed by the investigators at each visit, from visit 1 through visit 7 (weeks 0–24).
Efficacy measure
The Chinese SAICA
The social adjustment of all the subjects was assessed through parent-reported and self-reported ratings on the SAICA, which was a 77-item semistructured interview scale designed to evaluate the level of social functions across a wide range of domains for children and adolescents, including school functions, peer relationships, and home behaviors (John et al. 1987). The items of SAICA were rated on a 4-point Likert scale, with higher scores indicating more severe social problems or poorer school functions. The Chinese version of SAICA has been demonstrated to be a valid and reliable instrument for assessing the treatment effects with methylphenidate (Gau et al. 2006) and atomoxetine (Shang and Gau 2012) for ADHD. Parent-reported and self-reported SAICA was gathered at baseline, visit 4 (week 8), visit 6 (week 16), and visit 7 (week 24). The Chinese version of SAICA has also been widely used in clinic-based (Gau et al. 2015; Chiang et al. 2018) and school-based (Tseng et al. 2014; Chen et al. 2017; Tsai et al., in press) child and adolescent studies in Taiwan.
Statistical analyses
We used SAS version 9.2 (SAS Institute, Inc., Cary, NC) to conduct data analysis. Demographics and assessments of social adjustment were presented in numbers and the corresponding percentage for categorical variables and mean score and standard deviation (SD) for continuous variables. The intent-to-treat principle and the last-observation-carried-forward method were used in statistical analyses. One-way repeated-measures analysis of variance was used to determine the differences in the scores of the parent-rated SAICA. We used hierarchical linear mixed-effect models to address the lack of statistical independence of repeated assessments within the same participants over the study period. In particular, both intercepts and slope (time) effects in the linear mixed model with time-dependent variables were treated as random effects, to account for variations among subjects in baseline values, and slopes for individual trajectories of changes in SAICA scores over visits, in addition to the main treatment and fixed-time effects of the two treatment groups. To test the difference in the slope of change between the methylphenidate group and the atomoxetine group, the interaction terms between visits × drugs were tested. The α value was preselected at the level of p < 0.05. We used Cohen's d to compute the effect sizes for comparing the SAICA scores between week 8 and baseline and between week 24 and baseline, with small, medium, and large effect sizes as Cohen's d 0.2–0.5, 0.5–0.8, and ≥0.8, respectively.
Results
Sample description and medication
Of the 182 patients screened, 168 who met the inclusion and exclusion criteria were enrolled and randomly assigned to the methylphenidate (n = 83) (mean age, 9.61 ± 2.41; 72 males, 86.75%) or atomoxetine (n = 85) (mean age, 9.84 ± 2.71; 74 males, 87.06%) group. There were no statistically significant differences in demographic characteristics and baseline severity of social problems measured by the parent-reported SAICA between the two treatment groups (Table 1). Supplementary Table S1 shows the reasons for dropouts and missing data for SAICA in the two treatment groups at week 24 (Supplementary Data).
Demographics and Baseline Social Adjustment Between the Two Treatment Groups
IQ, intelligence quotient; SAICA, Social Adjustment Inventory for Children and Adolescents; SD, standard deviation.
At week 8, the completion rates of SAICA were 77.1% (64/83) for methylphenidate and 83.5% (71/85) for atomoxetine. At week 24, the completion rates of SAICA were 45.8% (38/83) for methylphenidate and 47.1% (40/85) for atomoxetine (Fig. 1). There were no significant differences in the completion rates of SAICA between the two groups at week 8 (p = 0.295) and week 24 (p = 0.868). The mean final administered dose for methylphenidate was 28.37 (SD = 12.52) mg/day or 0.82 (SD = 0.33) mg/(kg·d). The mean final administered dose for atomoxetine was 31.62 (SD = 9.39) mg/day or 0.92 (SD = 0.3) mg/(kg·d). There was no significant difference in drug adherence between the two treatment groups.
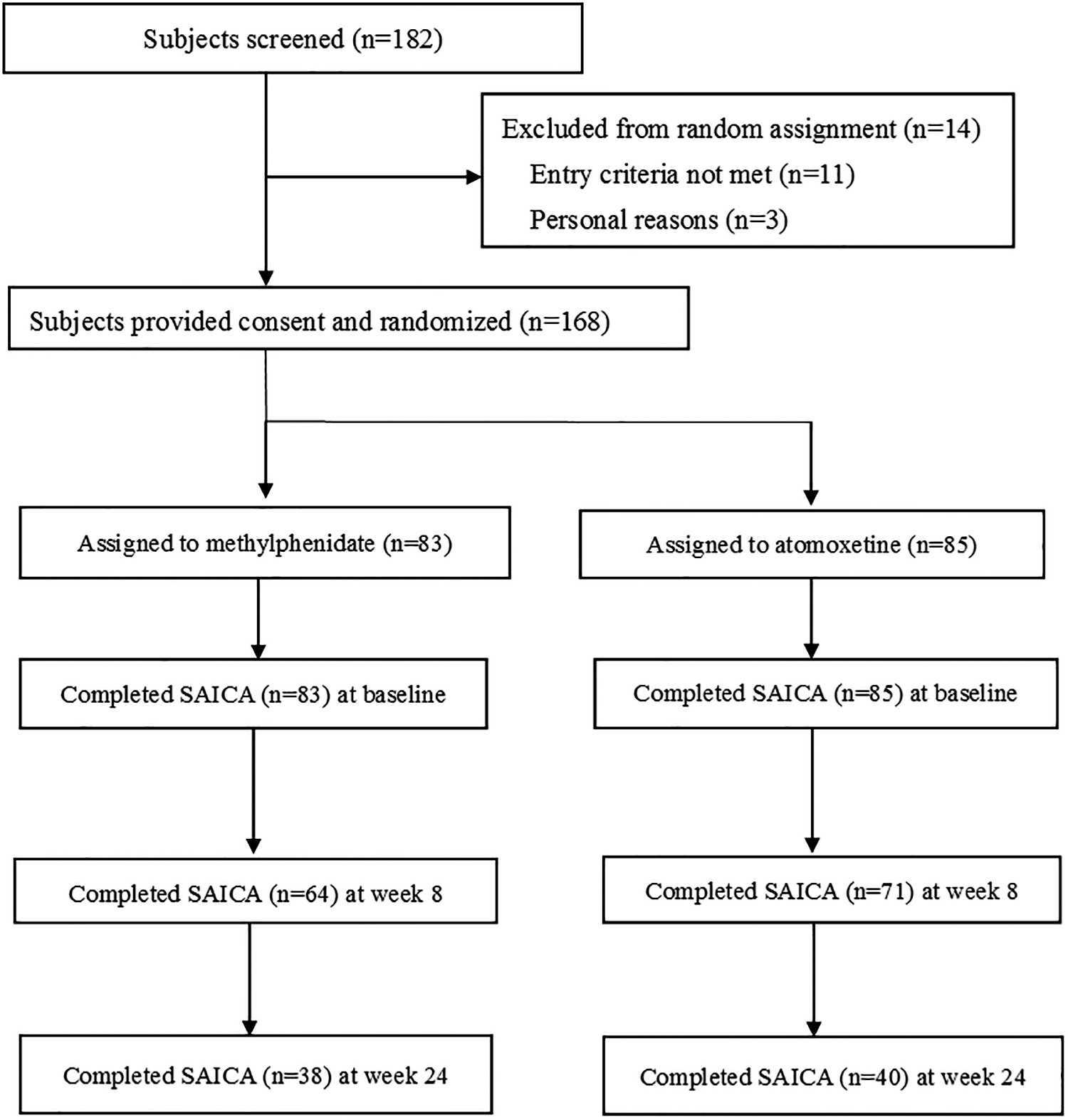
Flowchart of the randomization procedure. SAICA, Social Adjustment Inventory for Children and Adolescents.
Efficacy on school functions
Tables 2 and 3 show that at week 24, mean changes from baseline in the scores of overall school functions were 0.35 points (Cohen's d, −0.82) for parent ratings and 0.31 points (Cohen's d, −0.66) for self-ratings in the methylphenidate group with medium to large effect sizes; and 0.26 points (Cohen's d, −0.62) for parent ratings and 0.19 points (Cohen's d, −0.34) for self-ratings in the atomoxetine group with small to medium effect sizes. No significant group differences in the mean change of school functions reported by both informants from baseline to week 24 were found between the two treatment groups. There was no significant effect of the drug by visit interaction on parent-rated school functions (p = 0.125) (Fig. 2A). There was a significant effect of the drug by visit interaction on self-rated school functions (p = 0.045) (Fig. 2B).
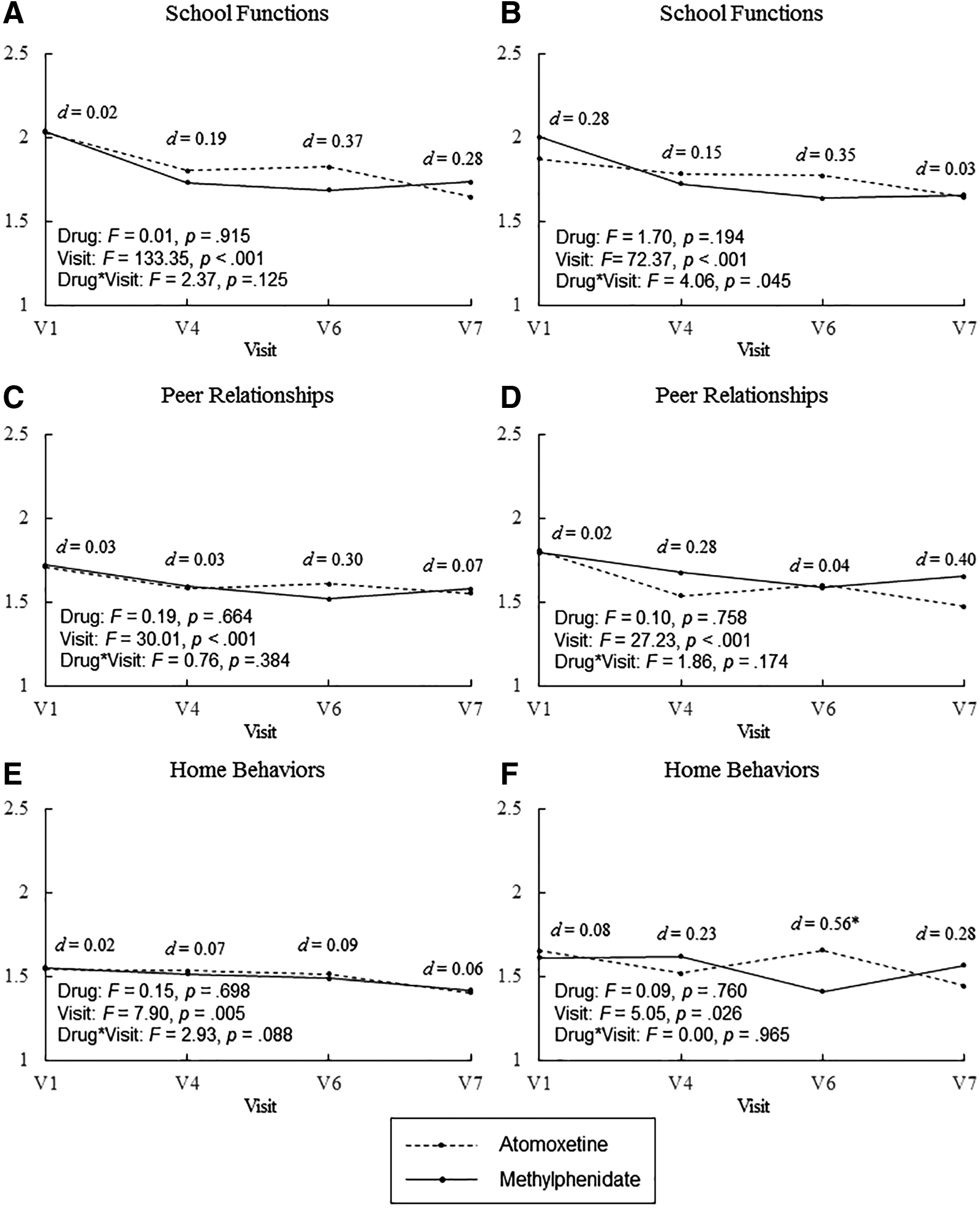
Improvements in the SAICA scores in youths with ADHD randomly assigned to treatment with either methylphenidate or atomoxetine.
Change in Parent-Rated Social Adjustment Inventory for Children and Adolescents from Baseline to Week 8 and to Week 24 (Endpoint) in the Two Treatment Groups
p < 0.05, ** p < 0.01, *** p < 0.001.
SAICA, Social Adjustment Inventory for Children and Adolescents; SD, standard deviation.
Change in Self-Rated Social Adjustment Inventory for Children and Adolescents from Baseline to Week 8 and to Week 24 (Endpoint) in the Two Treatment Groups
p < 0.05, ** p < 0.01, *** p < 0.001.
SAICA, Social Adjustment Inventory for Children and Adolescents; SD, standard deviation.
Efficacy on peer relationships
Tables 2 and 3 show that at week 24, mean score changes from baseline in the domain of peer relationships were 0.15 points (Cohen's d, −0.50) for parent ratings and 0.15 points (Cohen's d, −0.25) for self-ratings in the methylphenidate group with small effect size; and 0.11 points (Cohen's d, −0.33) for parent ratings and 0.3 points (Cohen's d, −0.65) for self-ratings in the atomoxetine group with small to medium effect sizes. No significant group differences in the mean change of the scores of parent-rated and self-rated peer relationships from baseline to week 24 were found. Neither parent ratings (p = 0.384) (Fig. 2C) nor self-ratings (p = 0.174) (Fig. 2D) showed significant effect of the drug by visit interaction on peer relationships.
Efficacy on home behaviors
Table 2 shows that at week 24, mean change from baseline in the scores of parent-rated home behaviors was 0.1 point (Cohen's d, −0.27) in the methylphenidate group with a small effect size. At week 24, there was no significant change in the scores of parent-rated home behaviors for the atomoxetine group or self-rated home behaviors for both methylphenidate and atomoxetine groups (Tables 2 and 3). No significant group differences in the mean change of the home behaviors domain reported by both informants from baseline to week 24 were found. Neither parent ratings (p = 0.088) (Fig. 2E) nor self-ratings (p = 0.965) on the home behaviors (Fig. 2F) showed significant drug by visit interaction effects.
Discussion
This is the first randomized, head-to-head, prospective treatment study to compare the effects of methylphenidate and atomoxetine on a wide range of social adjustment in drug-naive youths with ADHD. We found that both methylphenidate and atomoxetine are effective in improving school functions and peer relationships assessed by the parent-reported and self-reported Chinese version of the SAICA. These improvements are maintained throughout the 24-week study period for both medications. The magnitudes of improvement across 24 weeks for the two medications did not differ regarding the impairments in school functions and peer relationships. Our findings lend evidence to support that both methylphenidate and atomoxetine are effective in decreasing the severity of social maladjustment, particularly improving the functions at school and peer relationships in youths with ADHD. However, our findings provide some evidence to support that only methylphenidate is effective in improving parental observation of the behaviors at home, for example, relationships with parents and siblings, and behavioral problems at home.
Our findings of beneficial effects of 24-week treatment with methylphenidate on several domains of social adjustment in youths with ADHD, including school functions, peer relationships, sibling relationships, and behavioral problems at home, are consistent with the results of previous studies (Evans et al. 2001; Abikoff et al. 2004; Prasad et al. 2013). Methylphenidate may influence social behaviors by improving ADHD symptomatology (de Boo and Prins 2007), cognitive functions (Swanson et al. 2011), the theory of mind (Maoz et al. 2014), emotional regulation (Kutlu et al. 2017), and self-control (de Boo and Prins 2007). For example, psychostimulant-induced reductions in ADHD symptoms have been demonstrated to be a significant mediator of improvement in social adjustment (de Boo and Prins 2007). In children with ADHD treated with methylphenidate, improvement in social functioning is significantly correlated with reductions in the severity of inattention and hyperactivity/impulsivity (Kim et al. 2015). Methylphenidate has been reported to exert positive effects on classroom performance such as note-taking and the quality of written expression, which may translate into long-term academic performance for patients with ADHD (Evans et al. 2001). Our previous work has found significant associations between deficits of spatial working memory and school dysfunction in children with ADHD (Chiang and Gau 2014), and extensive research shows that treatment with methylphenidate is associated with improvement in spatial working memory in those with ADHD (Bedard et al. 2004; Ni et al. 2013). Further studies are needed to identify the underlying mechanisms for improvement in social adjustment following the administration of methylphenidate.
Compared with the core symptoms of ADHD, the effects of atomoxetine on the domains of school functions and peer relationships are less evaluated. Previous studies have demonstrated the effectiveness of atomoxetine in improving school behavioral problems (Waxmonsky et al. 2010), grades (Bakken et al. 2008), school interaction (Waxmonsky et al. 2010), and interpersonal relationships (Matza et al. 2007). Our findings show small-to-medium effects of treatment with atomoxetine in the realm of school functions (Cohen's d = −0.62 for parent ratings and −0.34 for self-ratings at week 24) and peer relationships (Cohen's d = −0.33 for parent ratings and −0.65 for self-ratings at week 24), comparable with those reported in the existing literature (Matza et al. 2007; Waxmonsky et al. 2010). The beneficial effects of atomoxetine in social adjustment may be associated with improvements in the severity of ADHD symptoms (Matza et al. 2007) and cognitive functions (Shang and Gau 2012). For example, after treatment with atomoxetine, improvement in interpersonal relationships is significantly correlated with change in the self-rated and clinician-rated measures of ADHD symptom severity (Matza et al. 2007). Atomoxetine is simultaneously associated with improvements in school functioning and several cognitive functions, including visual memory, sustained attention, and response inhibition (Shang and Gau 2012). Future research is warranted to investigate factors associated with the beneficial effects of atomoxetine on school functions and peer relationships.
Despite significant improvement in school functions based on parental reports, the self-ratings on the school functions show no improvement in attitude toward school work for atomoxetine and school social interaction for methylphenidate and atomoxetine from baseline to week 24, inconsistent with parent ratings of treatment response on these items. Although both youths with ADHD and their parents are essential informants for the difficulties in social adjustment, future studies are warranted to explore the underlying factors related to the inconsistent ratings between parents and youths with ADHD on the specific domains of social adjustment.
Our findings demonstrate no beneficial effects of methylphenidate or atomoxetine on interactions of ADHD youths with their parents, in contrast to a previous study showing that methylphenidate is effective in improving interaction with the mother (Tzang et al. 2012). This disparity may be attributable to differences in study design (randomized clinical trial vs. naturalistic observation study) and medication history of the subjects (drug-naive vs. no ADHD medication for 4 weeks). Our previous study has also reported that methylphenidate-treated children with ADHD still encounter significant impairments in interactions with their parents (Gau 2007). A clinical trial demonstrates that treatment with atomoxetine has a positive effect on the coping abilities of children with ADHD, whereas the parent-rated emotional climate in the family does not improve with atomoxetine (Svanborg et al. 2009). Similarly, patients with ADHD treated with atomoxetine show no improvement in functioning within the family social context (Wietecha et al. 2012). The impaired parent/child interactions of individuals with ADHD may result from an interplay of multiple factors not entirely ameliorated by methylphenidate or atomoxetine. Several studies show that behavioral and parental interventions are associated with improvements in parent/child interactions in patients with ADHD (Wells et al. 2000, 2006). More research is needed to examine whether medication combined with behavioral and parental interventions will be an optimal treatment strategy for the difficulties in parent/child interactions in families with ADHD youths.
Several methodological limitations of the present study need to be considered. First, because methylphenidate is a controlled medication in Taiwan, we are unable to conduct a double-blinded, placebo-controlled study as a clinical trial entirely initiated by the investigators. Whether the improvements in school functions and peer relationships may be attributed to the placebo effect requires further clarification. Second, parents may have fewer direct opportunities to observe performance and peer interaction in school settings. Other measures of social behavior, such as school observations and sociometric ratings, will also be useful to examine the treatment effects. Third, despite no standardized titration schedule for adjusting medications, the doses of methylphenidate and atomoxetine in the present study are consistent with the package information of these two medications. Fourth, the stimulant comparator in the present study is OROS-methylphenidate, and thus, our findings may not generalize to other formulations of methylphenidate. Fifth, as the participants in the present study are recruited from one medical center in northern Taiwan, our findings may not be generalized to other ethnic populations. Finally, missing data and dropouts in the 24-week study period may result in an insufficient sample size to achieve adequate power for detecting statistically significant differences in efficacy between methylphenidate and atomoxetine.
Conclusion
Our findings suggest that the Chinese version of the SAICA used in the present study is sensitive for assessing improvement in terms of the effects of methylphenidate and atomoxetine on a wide range of social adjustment in youths with ADHD.
Clinical Significance
The present study provides support for the positive effects of methylphenidate and atomoxetine on school functions and peer relationships, suggesting that pharmacotherapy is a promising treatment for improving social functions in drug-naive youths with ADHD. In addition, information about a wide range of social adjustment, for example, the SAICA, should be collected from both youth participants and their parents in assessing the response to the treatment with methylphenidate and atomoxetine in youths with ADHD.
Footnotes
Acknowledgment
The authors express thanks to Ming-Fang Chen, MS, for assistance in data analysis.
Disclosures
C.-Y.S., H.-H.S., Y.-L.P., H.-Y.L., and S.S.-F.G. were investigators. C.-Y.S., H.-Y.L., and S.S.-F.G. have conducted a clinical trial on behalf of Orient Pharma Co., Ltd., Taiwan. H.-H.S. and Y.-L.P. have no conflict of interest to be disclosed.
Supplementary Material
Supplementary Data
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.