
Abstract
Objectives:
The present study characterized the psychiatric diagnoses and symptoms that led to the administration of antipsychotic medications in children and adolescents with cancer, and to evaluate the benefits and tolerability of these drugs in a large hospital-based pediatric hematology–oncology practice.
Methods:
Efficacy and adverse effects of two second-generation antipsychotics were retrospectively analyzed in 43 patients 2.9–19.6 (mean 12.1) years of age. The Clinical Global Impression-Severity (CGI-S) Scale and Improvement (CGI-I) Scale were used to evaluate psychiatric symptom severity before and following treatment, while the incidence of side effects and drug–drug interactions were collected from medical records.
Results:
Olanzapine was administered to 58% of patients and risperidone to 42%; the choice of drug was at the discretion of the treating psychiatrist. The common psychiatric diagnoses among these patients included adjustment disorder (37%) and medication-induced psychiatric disorders (23%). The most common psychiatric-medical symptoms included irritability/agitation (79%) and depressed mood (74%). CGI-S improved significantly (p < 0.001) between assessments, with no statistically significant difference between olanzapine- and risperidone-treated patients. CGI-I scores at reassessment indicated superiority of olanzapine as compared with risperidone. Adverse effects of treatment were mild.
Conclusions:
Olanzapine and risperidone can be well tolerated and ameliorate severe psychiatric-medical symptoms in children and adolescents with cancer. The potential palliative benefits of these second-generation antipsychotics (e.g., rapid onset of action, antiemesis, sedation, and appetite stimulation) increase the utility of their use in children treated in oncology and bone marrow transplant units.
Introduction
The diagnosis and treatment of childhood cancer presents a multitude of challenges and sources of stress for patients and their parents (Sohn et al. 2017). Many patients experience depressed mood, anxiety, and irritability as part of a panoply of negative emotions. Depressive disorders, anxiety, and stress-related disorders are among the most common psychiatric diagnoses in children with cancer (Mitchell et al. 2011). The prevalence of depression and anxiety disorders in children with cancer differs between studies, with a range of 7%–32% (Honda and Goodwin 2004; Harter et al. 2007; Kersun and Elia 2007; Dalton et al. 2009; Mitchell et al. 2011). Treatment-related effects, premorbid family psychosocial distress, and the presence of preexisting psychiatric illness add to the psychiatric morbidity seen on the pediatric oncology ward. Additionally, medical interventions such as irradiation of the central nervous system and neurosurgery can contribute to the development of psychiatric illness.
Unaddressed suffering and distress secondary to psychiatric disorders may have a significant impact on the quality of life of young cancer patients, affecting participation in and compliance with the complicated treatment regimens that are most often employed in the pediatric oncology ward (Shemesh et al. 2002; Kennard et al. 2004; DeJong and Fombonne 2007; Bender et al. 2014; Shim et al. 2018). As a widespread recognition of its importance, nonadherence in critically ill patients was addressed in Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5; American Psychiatric Association 2013). Thus, medical and psychiatric comorbidities can often result in cumulative deterioration in both diseases.
As part of the multidisciplinary approach, the use of psychotropic medications in this population can improve quality of life in patients afflicted by persistent distress (Pao et al. 2006). Interestingly, published studies exploring the use of psychopharmacological treatments in children with cancer tend to focus on the use of antidepressants, with little attention devoted to the use of antipsychotic drugs in children in the cancer setting (Gothelf et al. 2005; DeJong and Fombonne 2007; Kersun and Elia 2007; Caruso et al. 2013; Thekdi et al. 2015).
Prescription of antipsychotic medications for children has become increasingly common over the last two decades (Edelsohn et al. 2017). In parallel, and in spite of limited scientific data, the use of antipsychotic medication for pediatric oncology patients has dramatically increased over the last two decades. Both oncologists and psychiatrists have contributed to this trend (Cullivan et al. 1998). Data on the safety and benefits of antipsychotic agents in the pediatric oncology population are limited, but recently many reports have been published. In general, antipsychotics have been found beneficial in decreasing psychiatric-medical symptoms, such as irritability, loss of appetite, sleeping problems, and nausea (Flank et al. 2015, 2016, 2017; Patel et al. 2017; Dupuis et al. 2019). Since no large controlled studies have been undertaken, guidelines for the psychopharmacological treatment of the children with cancer and comorbid psychiatric diseases are lacking. Treatment strategies are most often extrapolated from the adult literature and the clinical experience of local consultants.
The goal of this retrospective study is to describe our experience with the administration of antipsychotic medications in a large pediatric Hematology–Oncology service. Our aim is to evaluate the benefits and tolerability of these drugs, while paying special attention to potential drug interactions with medications that children with cancer are already receiving.
Experimental Procedures
Study design
A review of computerized medical charts from July 2010 to September 2017 was conducted at the Hematology–Oncology Department of the Schneider's Children Medical Center in Israel. The department treats ∼200 new oncology patients each year, and includes an inpatient unit, a stem cell transplantation unit, and a day hospital.
Study population and data collection
The charts of children and adolescents treated in the Hematology–Oncology Department who had been evaluated by five different child psychiatrists at the request of the patient-care team and who had been treated with antipsychotic medication were reviewed. Exclusion criteria were: treatment with antipsychotic medication before an initial psychiatric assessment and absence of full documentation, including full demographic information and two psychiatric assessments, before and after receiving the medication. The benefit of these pharmacological interventions was evaluated by the same psychiatrist in the “second assessment” follow-up. The second assessment was scheduled as needed for each patient. For this study we only included first and second assessments. Extraction of deidentified data was undertaken by two trained clinical pharmacists (O.P. and I.V.).
This retrospective computerized medical chart review was approved by the Institutional Review Board of the Rabin Medical Center, Petah Tikva, Israel.
Measures
Demographic and Clinical characteristics
Demographic data were collected. Concurrent medications were recorded and evaluated for drug–drug interactions with risperidone or olanzapine for each patient. Severity and response of symptoms were measured by the Clinical Global Impression-Severity (CGI-S) and the Clinical Global Impression-Improvement (CGI-I).
Psychiatric-medical symptoms
Major psychiatric-medical symptoms, as noted by the medical team and by the liaison psychiatrist were listed, including: irritability/agitation, depressed mood, insomnia, anorexia, anxiety, nonadherence, suicidality, psychosis, hypomania/mania, involuntary movement disorders, and somatization. Somatization was defined as symptoms such as pain or neurological problems that may be related to a physical cause, but cause excessive level of distress (American Psychiatric Association 2013).
Psychiatric diagnoses
Diagnoses were made by child psychiatrists in accordance with the DSM-5 criteria. Psychiatric diagnoses that were considered to be secondary to the patient's medical condition or to side-effects of medications the patient received were noted.
CGI-S scale
The symptomatic severity at the time of referral as part of clinical care, was assessed by the liaison psychiatrist using the CGI-S scale that uses seven gradations ranging from 1 (“not ill at all”) to 7 (“very ill compared with other patients”) (Guy 2000).
The CGI-I scale
The effects of treatment with olanzapine and risperidone were assessed by the CGI-I scale. Similar to the CGI-S, it is a 7-point rating change from baseline as 1 (“very much improved”), 2 (“much improved”), 3 (“minimally improved”), 4 (“no change”), 5 (“minimally worse”), 6 (“much worse”), and 7 (“very much worse”), with Zero representing “not assessed” (e.g., patient stopped medication before second assessment) (Guy 2000).
Antipsychotic-induced adverse events
Occurrence of untoward effects of the antipsychotic medications was collected from patients' electronic records. Treatment tolerability was retrospectively evaluated on the basis of Common Terminology Criteria for Adverse Events (CTCAE 2017).
Drug–drug interactions
Potential drug–drug interactions between patients' preexisting medications and olanzapine and risperidone were assessed and listed (Clinical_Pharmacology 2019; Lexicomp 2019; Micromedex 2019).
Statistical analyses
Analyses were conducted using the Statistical Package for the Social Sciences Version 20 (IBM; SPSS, Chicago, IL). Descriptive data are presented as mean ± standard deviation, or rates (%). Two-tailed Student's t-test was used to compare continuous variables (e.g., age) between those treated with risperidone compared with olanzapine. Chi square test or Fisher's exact test were used as necessary to compare categorical parameters (e.g., gender, oncological diagnoses, psychiatric diagnoses rates, and psychiatric-medical symptoms) between those treated with risperidone compared with olanzapine. Multivariate General Linear Model was used to compare changes in CGI-S scores over time between the two groups. Similarly, univariate analysis of variance (ANOVA) was used to compare CGI-I between the two groups, where interval of days between assessments was used as a covariate. ANOVA was used to compare the length of time to psychiatric consultation between the four malignancy groups.
Results
Demographic and clinical characteristics
The initial sample consisted of 59 computerized medical charts of children and adolescents who had been evaluated by a child psychiatrist and had been treated with antipsychotic medication. One patient was excluded because he received periciazine. Five were excluded because they started risperidone or olanzapine before consultation. Ten patients for whom full documentation was not available were excluded from this analysis. There were no statistically significant differences between the excluded group and the study cohort in terms of age, gender, and psychiatric symptoms.
The final study group consisted of 43 patients between the ages of 2.9–19.6 years (mean age of the total cohort was 12.1 ± 5.2 years). The median time interval between primary oncologic diagnosis and a psychiatric evaluation was 5.4 months, with a range of 22 days to 9.7 years.
At the time of psychiatric evaluation, 58% of the patients were already receiving one or more psychoactive medications (14% were taking ≥2 drugs). Fifty-four percent were already receiving benzodiazepines (clonazepam 35%, brotizolam 12%, lorazepam 5%, midazolam 2%), 13% were treated with antidepressants (escitalopran 7%, sertraline 2%, fluvoxamine 2%. mirtazapine 2%), cannabinoids 7%, promethazine 5%, and psychostimulants 5%. None of the patients in this sample was being treated with mood stabilizers or with antipsychotics at the time of first psychiatric evaluation.
At the time of psychiatric evaluation, 23 patients were receiving nonpsychiatric medications likely to induce neuropsychiatric adverse events. These medications included supraphysiological (19%) or tapering (7%) doses of corticosteroids (hydrocortisone [7%], dexamethasone [7%] and prednisone [12%]), levetiracetam (9%), and voriconazole (14%) (Zonios et al. 2008). Corticosteroids are often associated with behavioral and mood changes, and even with frankly manic and psychotic symptoms (Caplan et al. 2017). Levetiracetam may also be associated with neuropsychiatric symptoms such as aggression, agitation, anxiety, depression, apathy, and depersonalization in pediatric populations (Keppra [package insert], 2009). Voriconazole might be associated with visual hallucinations, which have been reported in 2.4% of patients during clinical trials (VFEND (voriconazole; package insert; New York).
The antipsychotic medications prescribed in this report were either olanzapine or risperidone. Twenty-five (58%) patients were treated with olanzapine, mean dose 3.5 ± 1.7 mg (2 ± 0.68 mg in preschoolers [<6], 2.5 mg in school-aged [6–12 years], 4.01 mg ±1.67 in adolescents and young adults [>12]) and 18 (42%) patients with risperidone, mean dose 0.8 ± 0.9 mg (0.34 ± 0.15 mg in preschoolers [<6], 0.5 mg in school-aged [6–12 years] and 0.83 ± 0.66 in adolescents and young adults [>12]). The choice of drug was made after consultation with clinical pharmacists. Demographic characteristics of the two groups, including distribution of oncological diagnoses and disease phases are presented in Table 1. Malignancies were grouped into one of four major categories (Chmielecki et al. 2017). There were no statistically significant differences between the four malignancy groups in the length of time to psychiatric consultation. Nineteen percent of patients were receiving treatment for relapsed or refractory malignancy at the time of consultation with the liason psychiatrist.
Demographic and Clinical Characteristics of the Study Population (n = 43)
BMT, bone marrow transplantation; NS, nonsignificant; SD, standard deviation.
Psychiatric-medical symptoms identified by the oncology team
The most prevalent symptoms that required psychiatric consultation were depressed mood (42%), irritability/agitation (37%), and anxiety (21%). Other symptoms included nonadherence with medical therapy (16%), insomnia (7%), anorexia (7%), and psychosis (5%). Twenty-five (58%) patients had two or more psychiatric symptoms as the cause for referral for psychiatric consultation.
Psychiatric-medical symptoms identified by the liaison psychiatrist
The psychiatric-medical symptoms identified by the liaison psychiatrists are presented in Table 2. Psychiatric-medical symptom approach. Ninety-three percent of patients had more than one psychiatric symptom (40 patients out of 43). Seven percent had only two symptoms, 30% had three symptoms, 21% had four symptoms, 21% had five, 12% had six, and 2% had seven. Seventy-four percent of patients had depressed mood (32 patients out of 43). Seventy-five percent of patients with depressed mood and 27% of patients without depressed mood reported insomnia (p < 0.01), 63% of patients with depressed mood and 27% of patients without depressed mood reported loss of appetite (p < 0.05).
Prevalence of Psychiatric-Medical Target Symptoms for Treatment with Antipsychotics in Pediatric Oncology and Bone Marrow Patients (n = 43)
The psychiatric-medical symptoms identified by the medical team and by the liaison psychiatrist were not compared, as the psychiatric-medical symptoms' list was not available to the medical team at the time of referral for psychiatric consultation.
Psychiatric diagnoses
A variety of psychiatric diagnoses were recorded for the 43 patients reviewed in this study (Table 3). Forty four percent of the patients had more than one diagnosis. The representation of psychiatric diagnoses was similar among both olanzapine- and risperidone-treated patients. Ninety percent of medication-induced psychiatric disorders were associated with corticosteroid usage. Psychiatric disorders due to another medical condition were prevalent in 14% of the children. Medical conditions included: brain tumors and metastases, neurosurgery, and graft versus host disease.
Psychiatric Diagnoses of the Study Population (n = 43)
CGI scores
The mean CGI-S score at first assessment of the entire study sample was 5.3 ± 1.1 (5.2 ± 1.1 in the olanzapine group and 5.4 ± 1.1 in the risperidone group, with no statistically significant difference). Following the initiation of treatment with either olanzapine or risperidone, patients were reassessed at a median of 10 days, (quartile percentiles: 25%: 7 days, 50%: 10 days, 75%: 22 days). The mean CGI-S at reassessment (3.5 ± 1.3), was significantly improved as compared with the first time point [F(2, 39) = 284, p < 0.001, Fig. 1] with no statistically significant difference between olanzapine- and risperidone-treated patients (3.2 ± 1.2 vs. 3.9 ± 1.3, p > 0.20). Univariate ANOVA did not reveal any significant effect of reassessment intervals on the model [F(2, 39) = 107, p > 0.80].
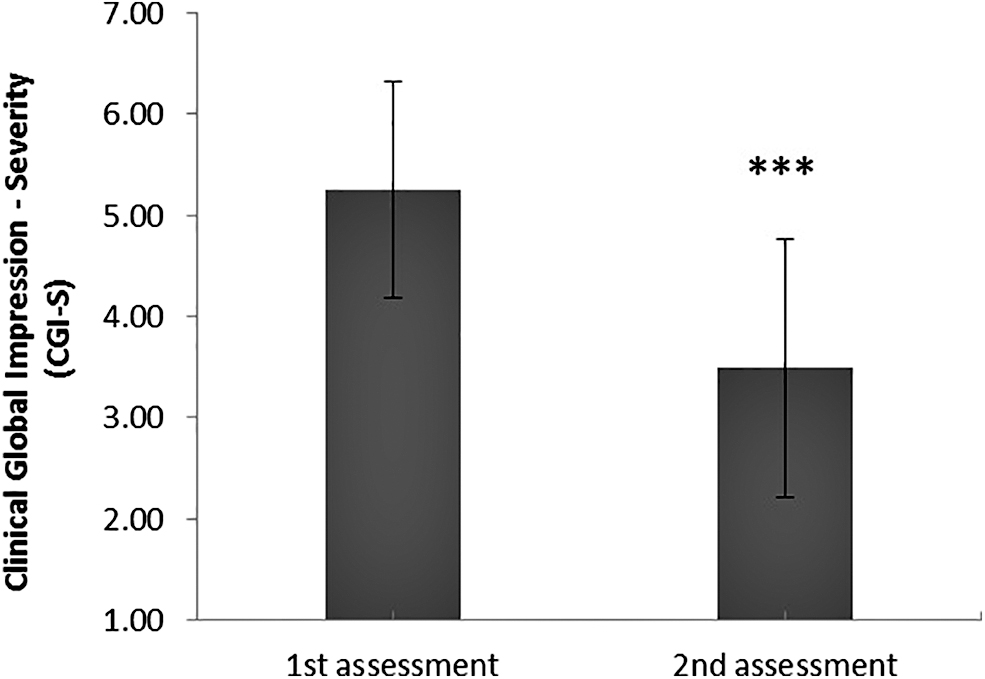
CGI-S scores (n = 43) before and after antipsychotic treatment. Mean CGI-S scores at first and second assessments of whole study cohort were 5.3 ± 1.1 and 3.5 ± 1.3, respectively. Antipsychotic treatment significantly [F(2, 39) = 284, p < 0.001] reduced CGI-S, without significant effect of the number of days between assessments between groups [F(2, 39) = 107, p > 0.80]. ***p < 0.001. CGI-S, Clinical Global Impression-Severity.
CGI-I scores at reassessment indicated lower scores with olanzapine as compared with risperidone (2.3 ± 1.0 vs. 3.0 ± 1.1, F = 4.38, p < 0.05, Fig. 2) the lower the score, the better the improvement. The number of days between assessments was used as a covariate (F = 0.31, p > 0.50).
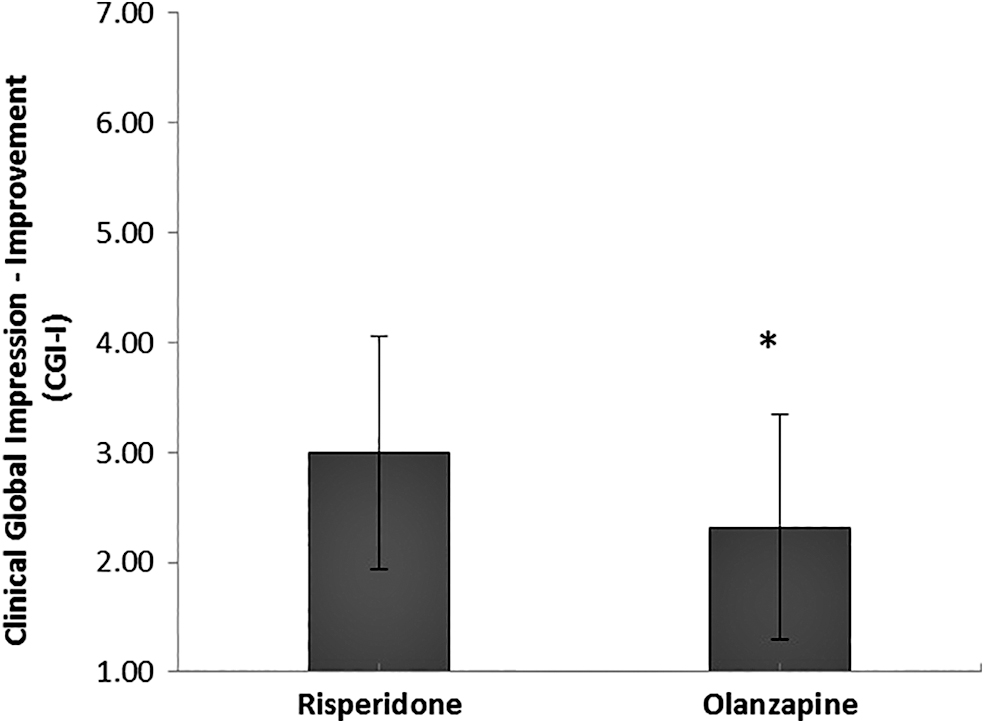
CGI-I scores (n = 43). Significant difference was found between CGI-I scores of olanzapine and risperidone groups (2.3 ± 1.0 and 3.0 ± 1.1 respectively, F = 4.38, p < 0.05). The lower the score, the higher the improvement, without significant effect of the number of days between assessments (F = 0.31, p > 0.5). *p < 0.05. CGI-I, Clinical Global Impression-Improvement.
Antipsychotic-induced adverse events
A total of seven patients (16%; four olanzapine- and three risperidone-treated patients) experienced six different adverse events that were due to the treatment with olanzapine or risperidone (Table 4). Three of them had more than one side effect. However, most of the adverse events were reported to be mild (grade 1–2, evaluated by the CTCAE (2017). In spite of the mild side effect, three out of the seven discontinued antipsychotic medication due to these side effects.
Antipsychotic Adverse Events in the Pediatric Oncologic Patients (n = 43)
CTCAE, Common Terminology Criteria for Adverse Events v5.0.
Rash, pruritus, and rhinorrhea.
Drug–drug interactions
The drug of choice as well as dose adjustments were tailored according to drug–drug interactions assessment and the medical condition of each patient. Potential drug–drug interactions between patients' pre-existing medications and olanzapine and risperidone were assessed and are listed in Table 5. Pharmacodynamic interactions are classified according to cumulative potential effects, while pharmacokinetic interactions are classified according to their mechanism (Clinical_Pharmacology 2019; Lexicomp 2019; Micromedex 2019).
Review of the Interaction Profile of the Antipsychotic Medications (Olanzapine and Risperidone) with the Specific Medications Administered to the Forty-Three Patients
Clinical_Pharmacology (2019); Lexicomp (2019); Micromedex (2019).
CYP1A2 mediates metabolism of olanzapine and CYP3A4 and P-glycoprotein of risperidone.
CNS, central nervous system; GABA, gamma-aminobutyric acid; SSRI, serotonin selective reuptake inhibitors; 5HT3, 5-hydroxytryptamine type 3; BRAF, B-rapidly accelerated fibrosarcoma; ACE, angiotensin-converting enzyme; Pgp, P-glycoprotein.
Discussion
A busy pediatric oncology unit is a place where parents and children with cancer must cope with a multitude of medical issues mixed with psychological distress (fears, anxieties, and concerns). Psychopharmacologic interventions are frequently used to help children deal with the burden of their disease, its treatment, and the psychiatric comorbidities that are often seen (and unmasked) during the course of the treatment of children with cancer (Levine et al. 2017).
This retrospective study reviews the use of two antipsychotic medications that were prescribed by liaison psychiatrists at the Pediatric Hematology–Oncology Department of the Schneider children's Medical Center in Israel. Real-time consultation with a clinical pharmacist enabled the use of these medications despite potential adverse reactions and drug interactions with the many medications that patients were already receiving. The use of antipsychotics in children with cancer has become increasingly widespread with growing data published in the last decade (Turkel et al. 2013; Flank et al. 2014, 2016, 2017, 2018; Kearney et al. 2016; Samsel and Muriel 2017; Samsel et al. 2018).
The psychiatric assessment of oncology patients can be challenging (Ruland et al. 2009). Identifying psychiatric-medical symptoms (such as depressed mood, sleep disturbances, irritability, anxiety, and loss of appetite) in these patients is often complicated and confusing for psychiatrists, resulting in frequent over- or underdiagnosis (Mavrides and Pao 2014). The primary disease and side effects of treatment can often mimic or mask antecedent psychopathology (Shemesh et al. 2002). Among the most challenging of symptoms are the somatic ones (such as pain, gastrointestinal complaints, and neurological symptoms) as they may be secondary to either the oncological disease, anxiety, and depression or somatoform disorders.
Further complicating psychiatric evaluation of children with cancer is the lack of standardized scales designed for this specific population. Scales that are routinely used for evaluation of psychiatric disorders cannot differentiate between medical-related symptoms and symptoms that may be indicative of a psychiatric disorder and hence are inadequate in this patients group (Cohen-Cole and Stoudemire et al. 1987; Canning and Kelleher et al. 1994; Knapp and Harris 1998). Thus, in this research, we have developed a list of symptoms that can help in selecting medication choice.
The most frequent psychiatric-medical symptoms observed by the consulting psychiatrist in the patients who in this study were irritability/agitation (79%), depressed mood (74%), and insomnia (63%). Agitation may result from multiple causes in children with cancer; antipsychotics can be effective and fairly well tolerated. (Cummings and Miller 2004).
In our study, the most frequent psychiatric diagnosis was adjustment disorder (37%), followed by medication-induced psychiatric disorders (23%) and major depressive disorder (23%), findings similar to those reported in adults with cancer (Cullivan et al. 1998). Most medication-induced psychiatric disorders in our patients were related to the use of systemic corticosteroids that can induce behavior and mood changes to frank psychotic symptoms (Caplan et al. 2017). Importantly, corticosteroid-related psychopathology can occur during therapy, during steroid taper or following discontinuation of the drug (Drozdowicz and Bostwick 2014).
We noted “Depressed mood” as a symptom in 42% of the children in our study. However, mood disorders were diagnosed in only 23% of the patients indicating that most of our patients with depressive symptoms did not fulfill criteria of a major depressive disorder, as has been previously reported by others (Mavrides and Pao 2014). Some of these patients who reported to have depressive symptoms finally met criteria for adjustment disorders and not major depressive disorder. They were treated with antipsychotic medications due to their severe psychiatric-medical symptoms, such as sleeping problems, loss of appetite, and anxiety. Given the diagnostic difficulties with comorbid psychiatric and other medical symptoms, a symptom-based treatment approach in oncology patients is warranted. Therefore, we advocate the use of a symptom-oriented approach, as previously proposed, to guide therapeutic decisions (Fleishman 2004; Pao et al. 2006).
We emphasize that antipsychotic treatment may be appropriate to patients with depression only when antipsychotic-targeted comorbidities are present. Targeted comorbidities may include medication/medical condition-induced neuropsychiatric symptoms (e.g., agitation/irritability, mania, psychosis) and medical indications (e.g., nausea, sleeping problems, and loss of appetite). Neither adjustment disorder nor depressed symptoms alone were sufficient for antipsychotic medication prescription.
We observed a disparity in the symptoms that precipitated psychiatric consultation requests by the pediatric oncology staff and the symptoms that were recorded by the consulting psychiatrists. Psychopathology may be underdiagnosed by the oncology team in these complicated patients, and determination of psychiatric-medical symptoms by the nonmedical staff can be unreliable. This suggests the need for a more active and preemptive role for the psychiatrist consultant on the pediatric oncology ward (Keller and Sarvet 2013).
The therapeutic effect revealed by severity scores was similar for both olanzapine and risperidone, however, olanzapine use resulted in significantly improved scores. There was a modest sideeffect prevalence, with mild symptoms that resulted in some discontinuation. We cannot distinguish greater side-effect burden between the two antipsychotics, given the equivalent discontinuation rate and low sample size.
Importantly, we demonstrated a combined clinical and pharmacological approach allowing treatment with antipsychotic medications, which is tolerable with benefits that outweigh adverse reactions.
In this study, a multidisciplinary team consisting of a child psychiatrist, clinical pharmacist, and pediatric oncologist displayed a clinical approach that enabled effective and fairly well-tolerated administration of olanzapine and risperidone to reduce symptom burden of children with cancer (Pao et al. 2006; Keller and Sarvet 2013).
Antipsychotic medications offer several advantages as compared with antidepressants in children with cancer. Both olanzapine and risperidone have a rapid onset of action and allow patients to achieve a clinical improvement of symptoms in a period as short as several days. Additionally, antipsychotic medications can improve the palliation of cancer-treatment side effects that have a negative impact on the patients' quality of life, such as weight loss, nausea, and vomiting (Bauer et al. 2011). The increased appetite and weight gain can often be a “desired” side effect in these patients; malnutrition has been associated with reduced response to chemotherapy (Murry et al. 1998), poorer disease-free survival (Dewys et al. 1980), and diminished quality of life (Hammerlid et al. 1998; Huhmann and Cunningham 2005) in children with cancer. Sedation, a common adverse effect of antipsychotics, may be beneficial in children with cancer who suffer from insomnia. To summarize, antipsychotics can ameliorate some neurovegetative depression symptoms and other medical cancer-related symptoms that secondarily can improve depression due to better quality of life.
Olanzapine, which blocks 5-hydroxytryptamine type 3 receptors (Bymaster et al. 1996; Kast and Foley et al. 2007) has demonstrated efficacy in the prevention and treatment of chemotherapy-induced nausea and vomiting in pediatric oncology patients (Flank et al. 2015) and has been incorporated in practice guidelines for the treatment of otherwise refractory chemotherapy-associated nausea and vomiting (Hesketh et al. 2017). The different on- and off-target therapeutic effects of olanzapine are attributed to the variable affinity of the drug for dopaminergic, serotonergic, and histaminergic receptors, which are associated with its antipsychotic, anxiolytic, antidepressant, antiemetic and sedative properties (Kast 2001; Kast and Foley et al. 2007).
Drug–drug interactions of psychiatric agents play a significant role in selecting medications from the psychiatric pharmacopeia; treatment should be maximally effective but also reliably safe. In addition, concurrent use of medications which share similar side-effect profiles with antipsychotic drugs may result in pharmacodynamic interactions. Pharmacokinetic interactions include inhibitory activity or induction of metabolic pathways. Therefore, decreased or increased elimination and respective elevated or reduced plasma concentrations might occur. Table 5 illustrates a useful chart of drug–drug interaction profile demonstrating that the primary metabolic pathway of olanzapine is mediated by CYP1A2 and CYP2D6, and of risperidone by CYP3A4 and P-glycoprotein.
The major limitations of this study are primarily its retrospective nature and its sample size. In addition, the symptom assessment was based on the clinical global impression of the psychiatrist at the time of examination in an unblinded process (the evaluator knew both that medication had been given and which agent had been used, potentially affecting his or her symptom assessment of the magnitude of improvement). Nausea was not included in the list of psychiatric-medical symptoms as it was not formally examined by the psychiatrist. Standardized scales for psychiatric disorders or side effects have not been used, including extrapyramidal symptom scales. Traumatic events and medical complications were not recorded during the treatment period. Finally, the current study presents the practice patterns in one treatment center; its results require confirmation in other institutions.
Conclusions
The antipsychotic medications (olanzapine and risperidone) used in this population in this study were found to be tolerable and have benefits that allow them to play a role in ameliorating severe psychiatric-medical symptoms in children and adolescents with cancer. Moreover, clinicians in oncology units may take advantage of some of the palliative benefits of these second-generation antipsychotics, such as rapid onset of action, antiemesis, sedation, and appetite stimulation.
Clinical Significance
Our findings have important implications for pediatric oncologists, pediatricians providing supportive care for children with cancer in the outpatient setting, and for child psychiatrists. Our study emphasizes the importance of a psychiatric evaluation for children with cancer before starting therapy, so as to methodically categorize specific symptoms and diagnoses, management, and monitoring. The antipsychotic medications used in this population in this study were found to be beneficial and tolerable. However, larger, prospective clinical trials are needed to explore the relative benefits of specific antipsychotic medications and to validate the results that we have shown in our study. Such studies will facilitate the elaboration of specific guidelines for the use of antipsychotics for critically ill patients.
Footnotes
Acknowledgments
The authors thank Meital Avishi, MD and Lior Adler, MD (Department of Psychological Medicine, Schneider Children's Medical Center of Israel, Petah Tikva, Israel), and Asaf Yaakoby, MD (Geha Mental Health Center, Petah Tikva, Israel), for their help in psychiatric assessments, and Georgina Martin, MD (Royal Preston Hospital, United Kingdom), for her invaluable help as a research assistant.
Disclosures
No competing financial interests exist.