
Abstract
Objectives:
Pediatric acute onset neuropsychiatric syndrome (PANS) is a clinically heterogeneous disorder presenting with: unusually abrupt onset of obsessive compulsive disorder (OCD) or severe eating restrictions, with at least two concomitant cognitive, behavioral, or affective symptoms such as anxiety, obsessive-compulsive behavior, and irritability/depression. This study describes the clinical and laboratory variables of 39 children (13 female and 26 male) with a mean age at recruitment of 8.6 years (standard deviation 3.1).
Methods:
Using a mathematical approach based on Artificial Neural Networks, the putative associations between PANS working criteria, as defined at the NIH in July 2010 (Swedo et al. 2012), were explored by the Auto Contractive Map (Auto-CM) system, a mapping method able to compute the multidimensional association of strength of each variable with all other variables in predefined dataset.
Results:
The PANS symptoms were strictly linked to one another on the semantic connectivity map, shaping a central “diamond” encompassing anxiety, irritability/oppositional defiant disorder symptoms, obsessive-compulsive symptoms, behavioral regression, sensory motor abnormalities, school performance deterioration, sleep disturbances, and emotional lability/depression. The semantic connectivity map also showed the aggregation between PANS symptoms and laboratory and clinical variables. In particular, the emotional lability/depression resulted as a highly connected hub linked to autoimmune disease in pregnancy, allergic and atopic disorders, and low Natural Killer percentage. Also anxiety symptoms were shown to be strongly related with recurrent infectious disease remarking the possible role of infections as a risk factor for PANS.
Conclusion:
Our data mining approach shows a very specific constellation of symptoms having strong links to laboratory and clinical variables consistent with PANS feature.
Introduction
Pediatric acute onset neuropsychiatric syndrome (PANS) is a clinically heterogeneous disorder presenting with: unusually abrupt onset of obsessive compulsive symptoms and/or severe eating restriction, with at least two concomitant cognitive, motor, behavioral, or affective symptoms such as anxiety and/or irritability/depression (Swedo et al. 2012).
The syndrome was described in 2012 as a result of the modification of the Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections (PANDAS) criteria: an acute prepubertal onset of tics or Obsessive compulsive disorder (OCD) and specific neuropsychiatric symptoms triggered by infections with group A beta-hemolytic Streptococcus (GABHS) (Swedo et al. 1998). PANS can be associated with nonstreptococcal triggers, such as Mycoplasma pneumoniae, Epstein–Barr virus, influenza, or other common viruses, usually located in the upper respiratory tract (Chang et al. 2015).
Pediatric autoimmune-mediated inflammatory brain diseases, however, may also be triggered by different environmental agents (e.g., stress, substances, virus, or bacteria), in subjects with a brain susceptibility to autoimmunity (Van Mater 2014; Graus et al. 2016). In fact, neuroinflammation has been postulated to have a pathogenic role in many psychiatric illnesses (e.g., major depression, bipolar, schizophrenia, and OCDs) (Najjar et al. 2013; Pape et al. 2019).
According to the 2013 PANS Consensus Conference (Swedo et al. 2012; Chang et al. 2015), PANS is currently conceptualized as a complex syndrome with a number of etiologies and disease mechanisms, encompassing psychiatric symptoms, arising from immune abnormalities triggered by a variety of agents (Frankovich et al. 2015; Murphy et al. 2015). The PANS diagnostic construct was proposed as a clinical entity distinct from idiopathic or familial OCD, anxiety, or Tourette disorder on the basis of clinical observations. The validity and generalizability of epidemiologic studies about PANDAS and PANS have been criticized for highly biased participant sampling and nonvalidated causes, effects, and methods (Gilbert et al. 2018).
Nevertheless, PANS may be comparable to other persistent neuroinflammatory disorders such as multiple sclerosis, Sydenham chorea (SC), Behcet's disease, and asthma, underlining that infections and other environmental triggers play a role in provoking an inflammatory brain response, which evolves into a chronic or progressive neuroimmune disorder (Frankovich et al. 2015). Despite the fact that PANS is a clinical diagnosis of exclusion without a single defined etiology or specific clinical symptoms, it could be considered a useful construct for outlining the sudden onset of severe neuropsychiatric symptoms in children with a relapsing-remitting course.
Artificial Neural Networks (ANNs) are computational adaptive systems inspired by the functioning processes of the human brain: they are considered particularly useful to solve nonlinear problems and to discover subtle trends and associations among variables. Based on their learning through an adaptive way (i.e., extracting from the available data the information needed to achieve a specific aim and to generalize the acquired knowledge), the ANNs appear to be a powerful tool for data analysis in the presence of relatively small samples (Buscema et al. 2015).
In the last decade, a fourth generation ANN called Auto-Contractive Map has been increasingly used in medicine (Street et al. 2008; Gironi et al. 2013; Buscema et al. 2015; Narzisi et al. 2015; Toscano et al. 2017; Grossi et al. 2017, 2018). Overall, literature findings suggest that this method may be a strategic approach to grasp the core of the relationship between signs and symptoms of PANS.
This study aimed to explore the associations between the different PANS features and laboratory and clinical variables in a sample of 39 children diagnosed with PANS. We used the ANN approach to exploit putative subtle simultaneous connections among the full spectrum of clinical variables and different domains of impairment.
Methods
Participants
Consecutive patients referred for obsessive compulsive or anxiety symptoms and tic disorder, between December 2017 and December 2018 to the outpatient clinics of Child & Adolescent Neuropsychiatric Unit, “G. Brotzu”Hospital Trust, Cagliari and the Child and Adolescent Psychiatry Unit, Policlinico “G. Martino,” Messina, were analyzed for possible PANS, according to PANS working criteria defined by experts convened at the National Institute of Mental Health (NIH) in July 2010 (Swedo et al. 2012), defined as follows: Abrupt dramatic onset of OCD or severely restricted food intake I) Concurrent presence of additional neuropsychiatric symptoms (with similarly severe and acute onset), from at least two of the following seven categories: Anxiety Emotional lability and/or depression Irritability, aggression, and/or severely oppositional behaviors Behavioral (developmental) regression Deterioration in school performance (related to attention deficit/hyperactivity disorder [ADHD]-like symptoms, memory deficits, and cognitive changes) Sensory or motor abnormalities Somatic signs and symptoms, including sleep disturbances, enuresis, or urinary frequency II) Symptoms are not better explained by a known neurologic or medical disorder, such as SC.
The diagnosis of PANS was confirmed by two child psychiatrists (A.G. and C.G.).
Exclusion criteria were the following: occurrence of immunologic diseases or cancer; presence of other medical or neurological/psychiatric diseases; active treatment with anti-inflammatory or corticosteroid agents; active treatment with psychoactive medications; and lack of consent form for participating in the study. Finally, patients with missing data on clinical records were excluded.
Variables
Patients were assessed according to the Consensus Statement clinical recommendations (Chang et al. 2015). An extensive physical, neurological, and psychiatric examination was performed. Parents were interviewed about family history and child medical history with a focus on the neurodevelopmental course, immune profile (autoimmune diseases, inflammatory diseases, immunodeficiency), and psychiatric conditions; family medical history included information about two generations (grandparents, parents, uncles, aunts, siblings, and cousins).
A blood sample was collected from each subject after the diagnosis and before starting any treatment. The battery of clinical laboratory test included: complete blood count, renal and liver function test, mineral panel, thyroid function indices, antithyroid antibodies (anti-thyroid peroxidase [anti-TPO], anti-thyroglobulin antibodies, TSH receptor antibodies [anti-TRAbs], and thyroid stimulating hormone receptor antibody [anti-TSH receptor]), and inflammatory blood markers (C-reactive protein [CRP], erythrocyte sedimentation rate [ESR], and procalcitonin [PCT]). Serum level of Immunoglobulin G (IgG) and Immunoglobulin M (IgM) Antibodies against Mycoplasma pneumoniae, Chlamydia pneumoniae, Haemophilus influenzae, Epstein–Barr virus, and Herpes Simplex Virus –HSV- Type 1 was also measured.
At enrollment all parents completed a checklist in Italian screening the symptoms and assessed their severity. The checklist was defined according to PANS criteria (Swedo et al. 2012).
It encompasses 10 items and systematically describes both main and additional PANS neuropsychiatric symptoms with multiple choice responses on a 4-point Likert scale (0 = absent; 1 = mild; 2 = severe; 3 = very severe). A narrative description of the meaning and implications of each item was provided to the parents (Tables 1) and a clinician helped the parents to fill out the checklist. In particular, parents were informed that the tool allows rating of how much the symptoms impact their child's life from 0 to 3, where 3 indicates the highest impact.
Mean Scores and SD at a 4-Point Likert Scale of the Main and Additional Pediatric Acute Onset Neuropsychiatric Syndrome Neuropsychiatric Symptoms and Number and Proportion of Patients Who Had Each Symptom
(Likert scale from 0 = absence to 3 = extremely severe).
PANS, pediatric acute onset neuropsychiatric syndrome.
Ethical approval
The independent Ethics Committee of Cagliari University Hospital approved the study. All the parents were given a full explanation of the study methods and purposes and gave their written consent.
Data Analysis
All patients' clinical variables (family history, child symptom severity, medical history, and clinical laboratory test results) were collected on a specific database. The complete list of the variables is shown in Tables 1–3. The proportion of patients who had a specific symptom, a positive family history and maternal disease, and abnormal laboratory test results was calculated for each variable. Furthermore, the clinical variables were analyzed in three steps: linear correlation analysis, ANN analysis, and benchmarking analysis.
Proportion of Patients Who Had Diseases and Abnormal Laboratory Test Results
Recurrent child's infections: sinusitis, chronic otitis, pharyngitis or tonsillitis, pneumonia, skin infections (i.e., staph), and/or signs of GAS infection (i.e., pharyngitis, anal or vulvar redness, skin lesions); this variable has been estimated as a dichotomic condition; a cutoff has been established on three or more respiratory infections (e.g., sinusitis, otitis, and bronchitis) in 1 year or the need for antibiotics for 2 months/year (Ballow 2008).
Frequent episodes of asthma, allergic rhinitis (AR), Immunoglobulin E (IgE)-mediated food allergies (FAs), and other immune-mediated food disorders requiring food avoidance.
Common evidence for cracked and itching skin or red and brownish-gray patches on the hands, feet, knees, wrists, upper chest, face, scalp, etc.
Standard and sleep EEG alterations.
The antistreptolysin O (ASO) patient's values in the blood plasma have been pooled in two groups (antistreptolysin titer > or < of 250 IU), based on the upper reference limit.
One or more IgG and IgM Antibodies against other germs (Anti-Mycoplasma pneumoniae, Chlamydia pneumoniae, Epstein–Barr virus, Borrelia Burgdorferi, and Herpes Simplex Virus –HSV- Type 1). Serological IgG/IgM at least fourfold rise in titer was considered positive.
One or more antithyroid antibodies (Anti-thyroid peroxidase [anti-TPO], Thyroglobulin antibodies, TSH receptor antibodies [anti-TRAbs], Thyroid Stimulating Hormone Receptor Antibody [anti-TSH receptor]) above the upper reference limit
The Antinuclear Antibody (ANA) patient's values in the blood plasma have been pooled in two groups (titers < or > of 1: 120), based on the upper reference limit.
Among the Lymphocyte subset (T, B, natural killer [NK] cells) values we considered the NK cells (CD3+/CD56+) % value, and we pooled them in two groups (NK ≥3% or NK <3%), based on the lower reference limit of 3%.
One or more inflammatory markers (erythrocyte sedimentation rate [ESR] and C-reactive protein [CRP]) above the upper reference limit.
Nasopharyngeal culture positive for Group A beta-hemolytic streptococcus (GABHS) or Staphylococcus aureus (MRSA), Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae, or other upper respiratory tract pathogenic germs
Evidences for changes in brain morphology at MRI with T-2 weighted images or contrast enhancement.
Linear correlation analysis
Spearman correlation analysis was performed on the 33 clinical and laboratory test variables expressed in binary format. A p-value <0.05 was considered to be statistically significant. Statistical analysis was performed with XLSTAT package 2018.
Benchmarking analysis
To handle a benchmarking analysis, the principal component analysis (PCA) and hierarchical agglomerative clustering (HAC) were carried out. Results of this benchmarking analysis allow to compare findings from the Auto-CM approach with findings from the traditional statistical approach.
Principal component analysis
PCA is mathematically defined as an orthogonal linear transformation of the data to a new coordinate system such that the highest variance by any projection of the data comes to lie on the first coordinate (called the first principal component), the second highest variance on the second coordinate, and so on. PCA is theoretically the optimum transform for given data in least square terms.
Hierarchical agglomerative clustering
HAC is one of the most popular clustering methods, which seeks to build a hierarchy of clusters with a “bottom-up” approach: each observation starts in its own cluster, and pairs of clusters are merged as one moves up the hierarchy. This method works from the dissimilarities between the objects to be grouped together, producing a so called “dendrogram,” which shows the progressive grouping of the data. It is then possible to gain an idea of a suitable number of classes into which the data can be grouped. PCA and AHC have been carried out with XLSTAT package 2018.
ANN analysis
General features
The Auto Contractive Map (Auto-CM) system is a fourth generation unsupervised ANNs, which has already been demonstrated to outperform several other unsupervised algorithms in a heterogeneous class of tasks (Buscema and Sacco 2017).
Auto-CM is a mapping method able to compute the multidimensional strength association of each variable with all other variables in a dataset, using a mathematical approach based on ANNs. Auto-CM is especially effective in highlighting any kind of consistent patterns, systematic relationships, hidden trends, and associations among variables. Indeed, this method is able to compute and graph a semantic connectivity map which:
preserves nonlinear associations among variables,
captures elusive connection schemes among clusters,
highlights complex similarities among variables.
The 3-layer architecture and the mathematical models of Auto-CM have been described elsewhere (Buscema and Grossi 2008). In nontechnical terms, this model has both a training phase and a learning phase. After the former, Auto-CM determines the so-called “weights” of the vector matrix, which
represent the warped landscape of the dataset and
permit a direct interpretation.
Indeed, these weights are proportional to the strength of many-to-many associations across all variables and can be easily visualized by transforming them into physical distances: variables whose connection weights are higher get relatively nearer and vice versa. By applying a mathematical filter (i.e., minimum spanning tree, MST) (Kruskal 1956; Fredman and Willard 1990) to the matrix of distances, a graph named “semantic connectivity map” is generated. This representation allows a visual mapping of the complex web of connection schemes among variables, simplifying the detection of the variables that play a key role in the graph.
The adaptive learning algorithms of inference, based on the principle of a functional estimation like ANNs, overcome the problem of dimensionality. For this reason, we did not apply Bonferroni adjustment (applied in the case of significance tests carried out with dependent variables) preferring to use an exploratory analysis looking for important associations among many independent variables.
Minimum spanning tree
The MST (Figs. 3 and 4) shows among the full spectrum of possible ways to connect the variables in a tree, the shortest combination. Based on the MST theory, the Auto-CM reveals the connections among variables providing a graph in which the distances among variables reflect their bonding strength (weights) (Buscema and Grossi 2008, 2017; Buscema et al. 2008). In practical terms, MST shows the best way to connect the variables in a tree and the shortest possible combination allowing to present the data in a simplified graph.

Semantic connectivity map (Auto-CM method) Minimum spanning tree. Strength of association across the clinical and laboratory variables: as shorter is the distance in space as higher is the links' strength values between variables. Auto-CM, auto contractive map.
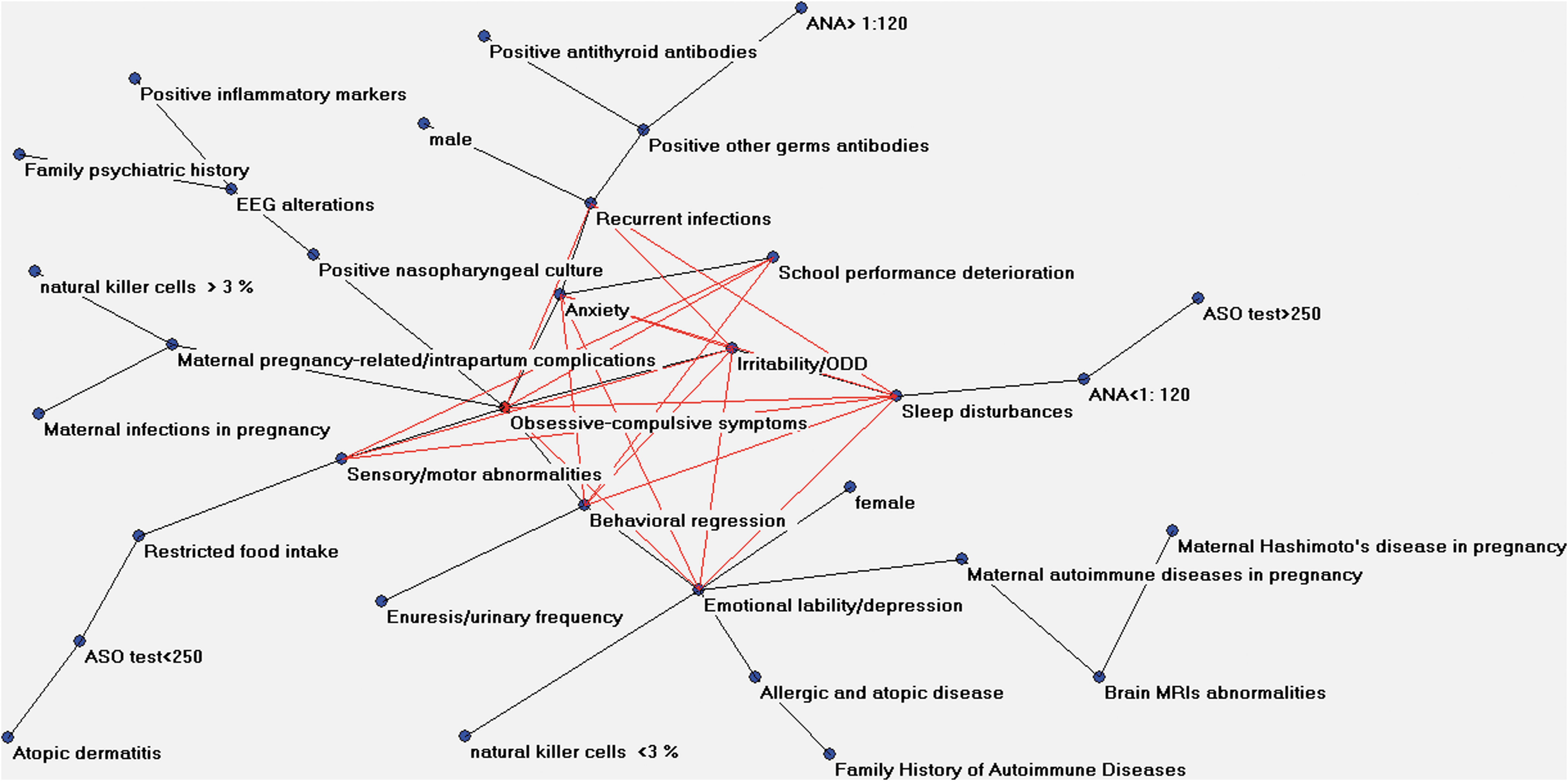
Semantic connectivity map (Auto-CM method) Minimum spanning tree and Maximal Regular Graph. It indicates the most important connections of the dataset. The resulting “diamond” expresses the complexity core of the syndrome.
In classical mechanics, Maupertuis's principle (Cheng 2012) states that the path followed by a physical system is the one of least length. It is a special case of the more generally stated principle of least action. Using the calculus of variations, it results in an integral equation formulation of the equations of motion for the system. The kinetic paths from least action principle quantify the transition processes among normal state and pathological state in biological systems. Also in case of variable interconnection, our assumption is that their system must naturally tend to minimum energy state, well described by the graph generated by MST.
This approach provides the map of relevant connections between and among variables and the principal hubs of the system. Hubs can be defined as variables with the maximum amount of connections in the map. The Auto-CM does not pose randomly the initial weights. Conversely, the Auto-CM starts with the same value. Thus, the resulting graph is reproducible along many runs. In other words, the Auto-CM visualizes in the space’ the correlation among the variables (“closeness”), and the graph identifies only the relevant associations organizing them into a coherent picture. The “central node” is the inner node that remains after bottom-up recursively pruning away the “leaves” nodes.
The MST represents what could be called the ‘nervous system’ of any dataset. In fact, summing up all of the connection strengths among all the variables, it gets the total energy of the system. The MST selects only the connections that minimize this energy, that is, only the ones that are really necessary to keep the system coherent. Consequently, all the links included in the MST are fundamental, but, on the contrary, not every “fundamental” link of the dataset needs to be in the MST. Such limit is intrinsic to the nature of MST itself: every link that gives rise to a cycle into the graph (viz., that destroys the graph's “treeness”) is eliminated, whatever its strength and meaningfulness. To fix this shortcoming and to better capture the intrinsic complexity of a dataset, it is necessary to add more links to the MST, according to two criteria:
the new links have to be relevant from a quantitative point of view;
the new links have to be able to generate new cyclic regular microstructures, from a qualitative point of view.
The additional links superimposed to MST graph generate a maximally regular graph (MRG).
Maximally regular graph
To understand how MRG works we must start remembering the nature of MST. MRG is the graph whose hubness function attains the highest value among all the graphs generated by adding back to the original MST, one by one, the connections previously skipped during the computation of the MST itself. Starting from the MST, the MRG presents the highest number of regular microstructures and highlights the most important connections of the dataset. In other words, to build the MRG the sorted list of the connections skipped during the derivation of the MST must be considered.
Each time we add a new connection to the MST basic structure, to monitor the variation of the complexity of the new graph at every step, with a specific parameter of complexity, called H Function. We call MRG the graph whose H Function attains the highest value among all the graphs generated by adding back to the original MST, one by one, the missing connections previously skipped during the computation of the MST itself. By this way, we draw a “diamond” expressing the complexity core of the system.
The frequency of a given symptom/variable influences the likelihood to become part of the central group of variables (core). Nevertheless, a high occurrence does not necessarily bring to the inclusion of a given variable in the core domain. In fact, even if the program is influenced by variable frequency, it picks up other kind of inherent information, independent from the simple frequency.
Results
Clinical variables
From a total of 312 consecutive outpatients referred for obsessive compulsive or anxiety symptoms and tic disorder, 42 were diagnosed with PANS. One child was excluded because parents refused to take part in research. Two children were excluded due to active treatment with anti-inflammatory agents.
Thus, in accordance with the inclusion and exclusion criteria of the study, 39 patients (13 females and 26 males) were enrolled into this study, corresponding to the 13% of the outpatients with obsessive compulsive or anxiety symptoms and tic disorder referred to the two units. Mean age at recruitment was 8.6 years (SD 3.1). For most of these patients (28/39 subjects; 72%), the symptom onset was close to the time of the first clinic assessment (between 1 and 12 weeks). In particular, 23/39 patients (59%) reported symptoms of infections (fever, coughing, ear pain, or diarrhea) within 4 weeks from the symptom onset. Instead, for the remaining 11/39 subjects (28%) the symptom onset lied between 3 months and 3 years before the first clinic visit, with relapsing/remitting course or with a single previous episode (spontaneously recovered) before the first observation.
Independent from their onset, all patients showed acute psychiatric symptoms at the time of the enrollment. As reported in Table 1, “anxiety” and “irritability/oppositional defiant disorder” were the most frequent, interesting the 89% of subjects. The “obsessive-compulsive symptoms” have been reported in the 87% of the sample. The percentage of subjects showing the other symptoms was never below 60%. The less frequent symptoms were “enuresis/urinary frequency” and restricted food intake (respectively, 61% and 66%).
As reported in Table 2, a positive family history of Autoimmune Diseases was the most frequent condition associated to PANS (80%). Increased rates of psychiatric disorders (72%) in the family were also reported. The pregnancy-related/intrapartum complications were reported by 64% of the mothers of the enrolled patients, active infections in 15%, active preexisting or new onset autoimmune diseases during pregnancy in 59%, and Hashimoto's disease during pregnancy in 33%.
Proportion of Patients Who Had a Family and Pregnancy-Related/Intrapartum History
Family History of Autoimmune Diseases in first-degree relatives: Sydenham chorea, Systemic lupus erythematosus (SLE), Sjögren syndrome, Kawasaki's disease, Myasthenia gravis, Asthma, Guillain–Barre’ syndrome, Multiple sclerosis, Hughes syndrome, type 1 diabetes, Celiac disease, Crohn's disease, Vitiligo, Psoriasis, Scleroderma, Familial Mediterranean fever, and Behçet's Disease.
Psychiatric history in first-degree relatives of OCD, eating disorders, emotional lability, mood disorders, ADHD, anxiety disorders, tic disorders, psychosis, disruptive disorders, autism spectrum disorder, language and communication disorders, intellectual disability, and specific learning disorders.
Pregnancy/delivery complications: high blood pressure, gestational diabetes, preeclampsia, placenta previa, preterm labor, low birth weight, fetal distress, perinatal asphyxia.
Infections in pregnancy: urinary tract infection, bacterial vaginosis, toxoplasmosis, cytomegalovirus, hepatitis B virus, influenza, Epstein–Barr virus infection. Group B Streptococcus infections.
Hashimoto's thyroiditis, or chronic lymphocytic thyroiditis in which the thyroid gland is gradually destroyed.
OCD, obsessive compulsive disorder; ADHD, attention-deficit/hyperactivity disorder.
As shown in Table 3, recurrent maternal infections were frequent (32/39; 82%); allergy and atopic diseases were reported almost in half of the sample (18/39; 46%), atopic dermatitis being the most frequent atopic disease (23/39; 59%).
Laboratory variables
Only 15 patients (39%) showed a high antistreptolysin O antibody (ASO) level (i.e., >250 IU, laboratory upper reference limit). Nasopharyngeal culture was positive in 23/39 subjects (59%) and it revealed the presence of Group A beta-hemolytic streptococcus (GABHS) in 8 out of 23 patients; other bacteria isolated by the nasopharyngeal culture were Staphylococcus aureus (11/23), Streptococcus pneumoniae (pneumococcus) (1/23), Haemophilus influenzae (2/23), and Pseudomonas aeruginosa (1/23).
In a large portion of the sample (49%) a high antibody titer against different germs was observed: the most common were antibodies against Mycoplasma and Chlamydia. We found IgG and/or IgM, depending on the length of the interval between infection and neuropsychiatric symptom onset, since the IgM normally disappears after 2–3 weeks of their production. A serological diagnosis of Epstein–Barr virus infection (IgM antibodies) was made in one case. Lyme disease was suspected for a young girl with IgG antibodies against Borrelia burgdorferi, but further laboratory tests did not confirm the diagnosis.
Antithyroid antibodies were found above the upper reference limit in the 36% of our sample, although no patients with thyroid antibodies positivity showed reduced echogenicity on thyroid sonogram, nor clinical Hashimoto's thyroiditis features, nor overt hypothyroidism. They all showed normal levels of thyroid-stimulating hormone (TSH) and free thyroxine (FT4).
The antinuclear antibodies (ANAs) were also found above the upper reference limit (titers > of 1: 120) in 13/39 subjects (33%). The lupus workup was completed for all the children with elevated ANA title: none of them resulted positive for lupus-specific antibodies. Inflammatory markers like CRP, ESR, and PCT levels above the upper reference limit were observed in only 7/39 subjects (18%).
A reduction of the Natural Killer (NK) absolute cell counts in the peripheral blood lymphocyte was observed in almost all the enrolled children. Among the Lymphocyte subsets (T, B, NK cells), the NK cell (CD3+/CD56+) % value was considered to define two groups of patients (NK ≥3% or NK <3%), based on the lower reference limit (3%). In 72% of our children the percentage of NK cells was less for the lower reference limit (5 patients had 1% or 0% of NK cells).
In 22 patients (56% of the sample) the electroencephalography (EEG) overnight recording showed intermittent or persistent focal or generalized slowing (mainly localized in temporal-frontal regions). Some patients presented also a persistent and unvarying focal or generalized slow-wave activity in the vigilant state, but none of them have had epileptic seizures.
Minor structural brain magnetic resonance imaging (MRI) abnormalities (T-2 weighted images or contrast enhancement) were observed in 8/39 subjects of the sample (21%). These abnormalities were however considered “incidental”: 2 slight ventricular asymmetries, 2 developmental venous anomalies, 1 isolated cerebellar vermis hypoplasia, 1 arachnoid cysts, 1 Arnold Chiari malformation, and 1 mild white matter hyperintensity in the periventricular area. No specific volumetric and/or inflammatory changes in the basal ganglia or cortical areas were found.
Linear correlation analysis
The Spearman linear correlation matrix of variables included in the study showed, as expected, a strong correlation between family history of autoimmune disease and maternal autoimmune disease in pregnancy and allergic and atopic disease (R = 0.38 and 0.40, respectively).
Remarkably, family history of autoimmune disease was correlated also to family psychiatric history (R = 0.39). Furthermore, family psychiatric history was related to EEG alteration and ASO positive test (R = 0.38 and 0.45, respectively).
Allergic and atopic diseases correlate to the increase of antibodies against other germs (Anti- Mycoplasma pneumoniae, Chlamydia pneumoniae, Epstein–Barr virus, Borrelia Burgdorferi, and Herpes Simplex Virus –HSV- Type 1) (R = 0.33) and against thyroid (R = 0.38).
High levels of ANA correlate with family history of autoimmune diseases (R = 0.44) and with positive other germ antibodies (R = 0.51). With regard to symptoms, ASO positive test is related to restricted food intake (R = 0.40), and the ANA positive test is related to enuresis/urinary frequency (R = 0.37). Emotional lability/depression correlates with the presence of positive other germ antibodies (R = −0.32) and with low NK cells (R = 0.33).
Benchmarking analysis
The PCA contains all possibly correlated variables distributed along vectors of different sizes (various numerical values), identifying the linearly uncorrelated variables (principal components) along which the variation in the data is maximal.
Here PCA map provided the identification of two clusters, shown in Figure 1. The first cluster is organized around the obsessive compulsive dimension and encompasses almost all PANS symptoms in the following hierarchy: enuresis/urinary frequency, school performance deterioration, sensory motor abnormalities, sleep disturbance, irritability/oppositional defiant disoder (ODD), behavioral regression, anxiety, and emotional lability/depression.
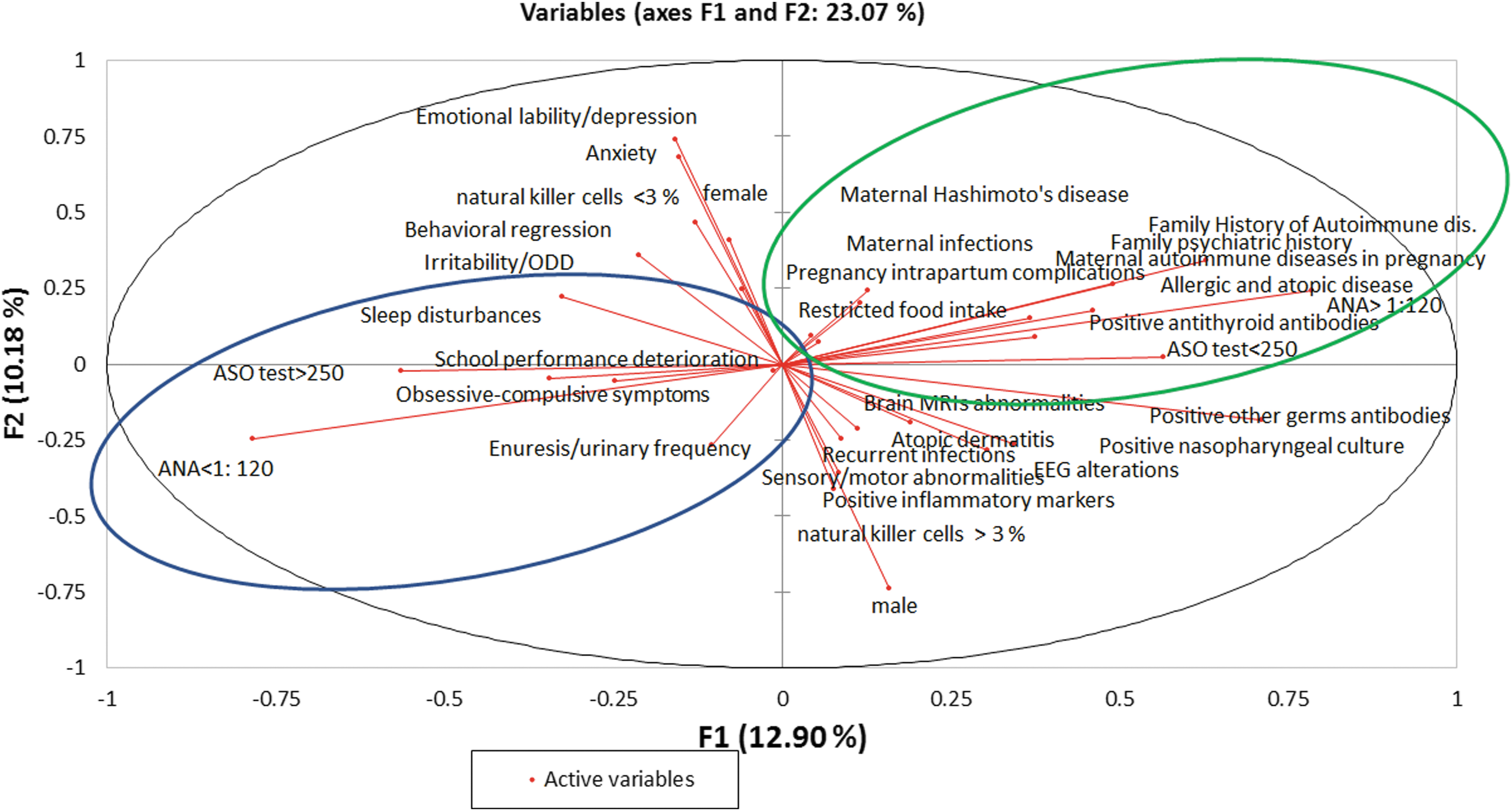
PCA (FIRST Two Components): all possibly correlated variables distributed along vectors of different numerical values, identifying the linearly uncorrelated variables (principal components) along which the variation in the data is maximal. PCA, principal component analysis.
Among the variables of this cluster we also found the variables ASO test >150 and NK <3. The opposite variables (ASO test <150 and NK ≥3) in our PCA were uncorrelated variables.
The second cluster encompasses most of the familial and personal risk factors and conditions. Among them, autoimmune diseases during pregnancy, ANA >1:110, Antithyroid antibodies, familial autoimmunity, allergic atopic disorders, and other germ (Anti-Mycoplasma pneumoniae, Chlamydia pneumoniae, Epstein–Barr virus, Borrelia Burgdorferi, and Herpes Simplex Virus –HSV- Type 1) antibodies are represented by vectors of largest size.
The agglomerative hierarchical clustering (AHC) analysis resulted in a dendrogram, which shows the progressive grouping of the variables (Fig. 2). The dendrogram shows the clustering of the variables according to a particular kind of mathematics inherent to HAC technique. As stated in the figure legend there are different clusters marked with different colors. Our dendrogram shows three clusters identified by different colors. The green cluster encompasses almost all PANS symptoms, with some variables more closely related to each other, as obsessive compulsive symptoms and school performance deterioration, enuresis/urinary frequency and behavioral regression, sleep disturbance, and irritability/ODD. Furthermore, emotional lability/depression is linked to NK <3. The red cluster shows a predictable relationship between “pregnancy/delivery complications” and “infection during pregnancy.” Noteworthy, both these conditions appear linked with “ASO test >150” and are more frequent in female children. The blue cluster encompasses all other laboratory and clinical variables.
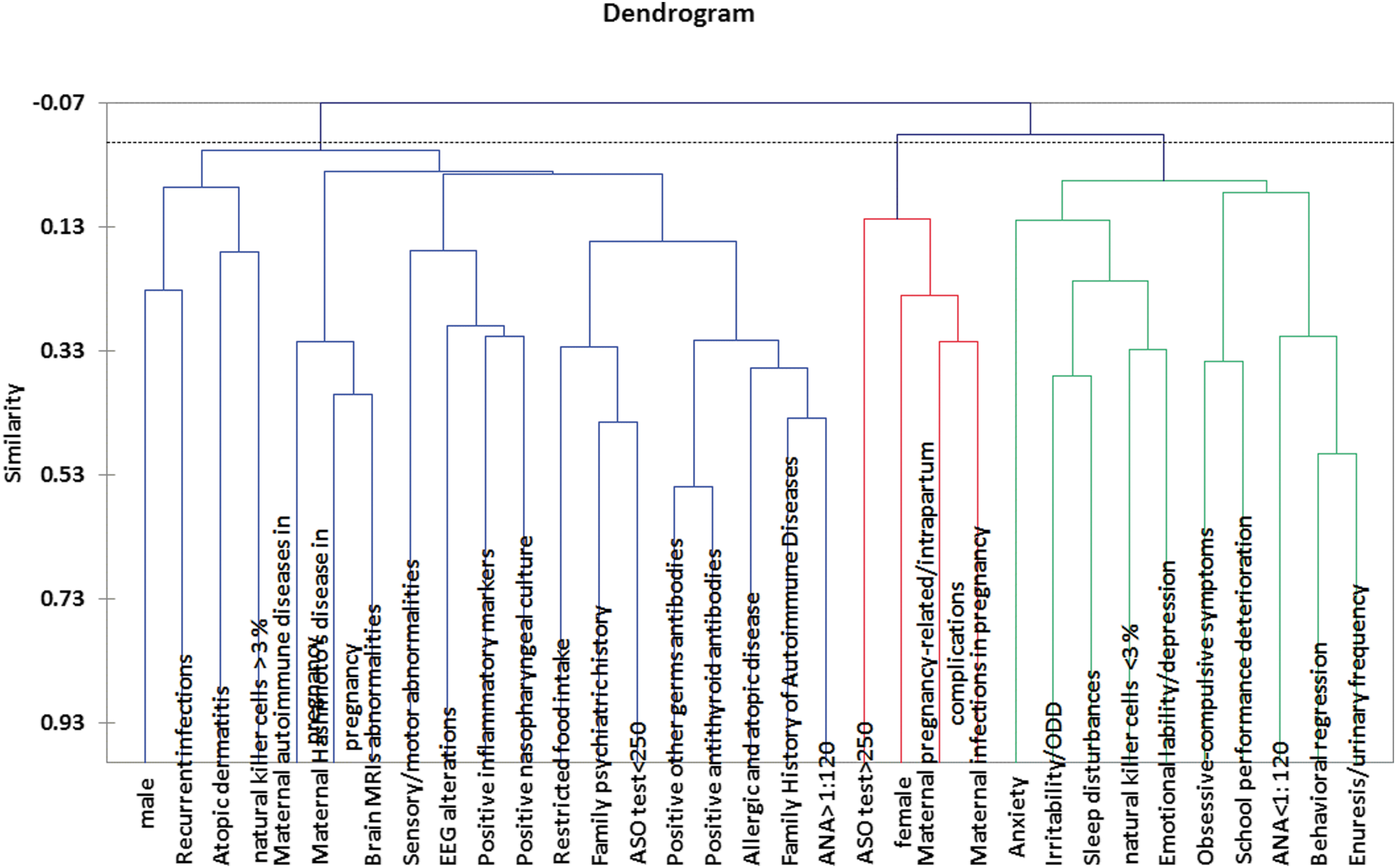
AHC shows the progressive grouping of the variables resulting in a dendrogram with three clusters identified by different colors. AHC, agglomerative hierarchical clustering.
Semantic connectivity map
The semantic connectivity map (Auto-CM method)–MST graph (Fig. 3) shows the strength of association across the clinical and laboratory variables visualized by the concept of “closeness”: the variables whose connection weights are higher get relatively nearer and vice versa. The links' strength values were all above 0.8. The connection strengths do not influence the solution of MST. They have a different meaning from the weights generated by Auto-CM and have only a descriptive function.
It is important to remember that the frequency of each variable influences the likelihood to become part of the central group of variables (core), but it does not necessarily bring to the inclusion of the variable in the core domain. For example, family history of autoimmune disease is the most frequent variable, but it is not included in the core domain.
As shown in the Figure 4, the “Maximally Regular Graph” superimposed to MST indicates the putative internal structure of the syndrome.
The map shows that PANS symptoms are strictly linked to each other in a central “diamond,” originated by the specific mathematical function called MRG (see Method section). It encompasses anxiety, irritability/ODD symptoms, obsessive compulsive symptoms, behavioral regression, sensory motor abnormalities, school performance deterioration, sleep disturbances, and emotional lability/depression. Two PANS symptoms (enuresis/urinary frequency and restricted food intake) are beyond the “diamond,” indicating a less frequent link with the other symptoms. Nevertheless, their high link strength value (≥0.8) with the other symptoms indicates a strong probability of co-occurrence with the other symptoms. In our opinion, the resulting “diamond” well expresses the complexity core of the PANS.
The robustness of Auto-CM system analyzing the stability of connections in the MST graph is described in Supplementary Data.
Discussion
Even though the data collected describe the already known characteristics of PANS, our study offers a statistic model for a specific symptoms' constellation (syndrome) clinically distinct from other neurodevelopmental disorders.
PANS described by ANN analysis
Our study is the first one to have adopted Complex network mathematics approach like Auto-CM to face the complexity of PANS phenotype. The results of the study show that PANS symptoms, as defined by the PANS Collaborative Consortium (Swedo et al. 2012; Chang et al. 2015), are strictly connected one to another, shaping a central “diamond” encompassing anxiety, irritability/ODD symptoms, obsessive compulsive symptoms, behavioral regression, sensory motor abnormalities, school performance deterioration, sleep disturbances, emotional lability/depression, and laboratory measures.
The Auto-Contractive Map method also allowed to grasp the core of the relationship between symptomatology, history, and laboratory results of our subjects with PANS. Exploiting all not obvious connections among the full spectrum of clinical variables revealed the simultaneous connections among symptoms and clinical signs, highly consistent with the PANS Collaborative Consortium's description of the syndrome (Chang et al. 2015).
Noteworthy, the classical statistical analysis (Spearman linear correlation) resulted as far less explicative of the real relationships between the variables. It failed in showing the whole symptomatic dimensions even if it displayed the relationships among them. The traditional statistical analysis approach suffered from some criticisms. Indeed, due to the heterogeneity in clinical expression of the PANS syndrome (i.e., different degrees of symptom severity along with various pathogenesis), a traditional statistical analysis approach using a “single symptom approach analysis” may not provide comprehensive information on the putative nature of the PANS.
The semantic connectivity map (Figs. 3 and 4) describes the hidden internal construct of PANS and exemplifies the consistency of the PANS working criteria, as they were defined at the NIH in July 2010 (Swedo et al. 2012). In fact, the PANS symptoms are strictly linked to one another shaping a central “diamond” encompassing anxiety, irritability/ODD symptoms, obsessive compulsive symptoms, behavioral regression, sensory motor abnormalities, school performance deterioration, sleep disturbances, and emotional lability/depression.
In the present semantic connectivity map, the variable “obsessive-compulsive symptoms” node acts as a hub (variable with three or more links) receiving convergence from the other symptom nodes (anxiety, irritability/ODD symptoms, behavioral regression, and sensory and motor abnormalities) and from clinical variables (nasopharyngeal culture and pregnancy/delivery complications). Therefore, the obsessive compulsive dimension seems to represent the core symptom of the syndrome. At the same time, it is one of the most frequent symptoms, being reported in 87% of the sample.
Enuresis/urinary frequency is located beyond the “diamond,” even though it is strictly related to the other symptoms. This symptom, reported in the 61% of patients, could be underestimated because parents may not be aware of it at the early stage.
The only other symptom located outside the “diamond” is the restricted food intake, even though it is situated along one of the branches directly arising from the main hub (obsessive compulsive symptoms). Of note, even if this symptom was very common among the subjects of the present sample (66% of the subjects), most of the children had a relatively mild food intake restriction. It is possible that cultural reasons may explain this finding, since parents (mostly living in the south of Italy) are used to strongly encourage their children to eat even when they tend to refuse the food. This peculiar approach to feeding can also explain the relatively lower frequency of food intake restriction compared to the other symptoms. However, in the semantic map, this symptom is allocated right beyond the sensory/motor abnormalities.
Interestingly, according to our clinical experience, some of the children with PANS that refused to eat also showed atypical sensory interests concerning the food (e.g., odor, consistency, or color of aliments) or compulsions and rituals related to the feeding act (e.g., crumbling the food, taking little bites, long chewing, moving the bite in the mouth, refusing to swallow, or swallowing only in specific positions, and so on). This suggests that, at least in part, the food intake restriction could be linked to the sensory and compulsive dimension of PANS clinical presentation rather than to simple loss of appetite.
The semantic map also describes the association between obsessive compulsive symptoms, school performance deterioration, and anxiety symptoms and between emotional lability/depression and behavioral regression, supporting the PANS phenotype description. Actually, the coherence of these symptoms was already evident in the benchmarking analysis. Both the PCA and the AHC provide clusters of symptoms closely and reciprocally linked.
From the PCA, the first cluster is organized around the obsessive compulsive dimension and encompasses almost all PANS symptoms in the following hierarchy: enuresis/urinary frequency, school performance deterioration, sensory motor abnormalities, sleep disturbance, irritability/ODD, behavioral regression, anxiety, and emotional lability/depression.
A second cluster encompasses the most of laboratory and clinical variables. This cluster underlines a meaningful relationship between most of the autoimmunity markers studied in our sample (“other germs antibodies,” “antithyroid antibodies,” “allergic and atopic disorder,” “familial autoimmunity,” “ANA >1:110,” “autoimmune diseases in pregnancy,” and “Hashimoto's disease in pregnancy”). It is known that most of the patients with PANS have both autoimmune/inflammatory diseases (e.g., autoimmune thyroiditis, postinfectious, enthesitis-related, psoriatic, or spondyloarthritis) and higher ANA and antithyroid antibodies than expected in the general population (Frankovich et al. 2015).
In particular, the AHC analysis resulted in a dendrogram, which shows the progressive grouping of the variables. It gains the idea of a suitable number of classes into which the variables can be grouped. One of the clusters of variables in our sample includes almost all PANS symptoms. Among them, it is possible to recognize variables closely related to each other, as obsessive compulsive symptoms and school performance deterioration, enuresis/urinary frequency and behavioral regression, sleep disturbance, and irritability/ODD.
The Auto-Contractive Map method also allowed to grasp the core of the relationship between symptomatology and family/children clinical history and laboratory results. The allocation of all the laboratory and clinical variables around the “symptoms diamond” suggests that we should consider potential biological markers of a disease with a multifactorial pathogenesis and different possible causative conditions. The semantic connectivity map shows that emotional lability/depression is a highly connected hub linked to autoimmune disease in pregnancy, allergic and atopic disorders, and low NK percentage. Also anxiety symptoms are strongly related, on our semantic connectivity map, with recurrent infectious disease remarking the possible role of infections as a risk factor for PANS. The aggregation between PANS symptoms and laboratory and clinical variables highlights the importance of testing some inflammatory markers and considering their role in the pathogenesis of PANS.
Furthermore, in our semantic map, both familial and maternal disease factors (familial autoimmunity, family history of psychiatric diseases, Hashimoto's disease in pregnancy, infections in pregnancy, and autoimmune diseases in pregnancy) and children clinical and laboratory variables (allergic and atopic disorders, atopic dermatitis, nasopharyngeal culture, EEG alterations, NK cells % value <3, inflammatory markers, ASO test, other germ antibodies, ANA, and antithyroid antibodies) are closely related to symptoms.
These suggest that it is important to take notice of the familial autoimmune/inflammatory profile and to consider the possible pathophysiologic role of immunological events during pregnancy. Even though factors having less than three links can be considered from a mathematical point of view, of relatively lower importance, they may represent the potential mechanisms, including direct influences of infections in the central nervous system (CNS), immune activation, and inflammatory mediators in PANS syndrome. Furthermore, emotional lability/depression is strongly related with NK cells % value <3.
PANS and familial, clinical, and laboratory variables
A second level of analysis with regard the familial, clinical, and laboratory data was described in our sample. As shown in Table 2, a high percentage of our patients had relatives affected by autoimmune disorders (80%) and psychiatric disorders (72%). Both conditions have been associated with PANS (Chang et al. 2015), even if most of the studies are focused on OCD and tic disorders among first-degree relatives of PANDAS probands (es. Lougee et al. 2000).
A recent survey, carried out by PANDAS network (Pohlman 2018) and based on parent's reports, described 47,34% of 1221 patients with PANS/PANDAS having autoimmune signals in the maternal and paternal lineage, 58,39% having anxiety disorders, and 27,52% having OCD in the maternal and paternal lineage. In our sample, both autoimmune and psychiatric diseases in the family members ranked higher than the survey data (around 70%). This difference may be attributed to the different method used to collect the information, because in the present study data were collected from a clinic interview by expert clinicians rather than a questionnaire. On the whole, a familiar probably genetic (Wang et al. 2015) susceptibility for both autoimmune and psychiatric disorders appears to play an important variable increasing the likelihood of developing PANS.
Results of the present study also showed a high prevalence rate of the pregnancy/delivery complications in general (64%) and active infections and autoimmune diseases during pregnancy in particular (15% and 59%, respectively) in our sample (Table 2). Prenatal exposure to infection is a risk factor for a wide range of neurodevelopmental and psychiatric disorders according to gene–environment interaction etiological model (Zhou 2012; Blomström et al. 2015). More recent studies have considered the interaction between maternal immune activation (MIA) and genetic risk factors for alterations in structural/functional neuronal network impairments leading to psychiatric conditions as autism spectrum disorder (ASD) and schizophrenia (Bergdolt and Dunaevsky 2018).
The link between maternal infection and neurodevelopmental disorders could also be regarded as a MIA potentially inducing prolonged immune alterations in the offspring's brain, independently from the infection itself (Boulanger-Bertolus et al. 2018). It is thought that the maternal activation of the innate and adaptive immune systems due to infection, stress, autoimmunity, asthma, allergies, or inflammation can lead to several neuropathologies in the progeny, particularly ASD and schizophrenia (Jiang et al. 2018). This is because MIA may influence the developing fetal CNS through the increased production of inflammatory cytokines acting as a disease primer or first “hit” and predisposing susceptible individuals for further exposures or “hits” later in life (Jiang et al. 2018; Bilbo et al. 2018). Furthermore, immune abnormalities seem to be more common in individuals and first degree relatives with ASD (e.g., Gładysz et al. 2018). For instance, fetal brain-specific antibodies have been identified in mothers of autistic children in several different studies (Keil et al. 2010; Nordahl et al. 2013; Fox-Edmiston and Van de Water 2015; Hughes et al. 2018).
In line with this hypothesis, we found that almost a third of the mothers of the enrolled patients suffered from Hashimoto's thyroiditis during pregnancy. This prevalence is almost thrice higher than the estimated prevalence (13%) of the disorder in the United States (Staii et al. 2010). Studies conducted in our geographic area found that between 5% and 20% of female and between 1% and 5% of male are affected by Hashimoto's thyroiditis in the general population (Chiovato et al. 1993). In the last decades, the disease has become even more common than it was until the early 1990s (Benvenga and Trimarchi 2008). It could be inferred that our children have been exposed to elevated levels of circulating antibodies during their intrauterine life. The association between autoimmune thyroiditis and psychiatric disorders in offspring has been poorly studied.
A family history of autoimmune disorders was described in children with “regressive” autism. Regression was significantly associated with a family history of autoimmune disorders (adjusted OR = 1.89) and particularly with autoimmune thyroid disease (adjusted OR = 2.09) (Molloy et al. 2006). A recent systematic review showed a significant association between maternal thyroid dysfunction during early pregnancy, including low and high thyroid hormone level and autoimmune thyroiditis, and several offspring behavioral and psychiatric disorders such as attention-deficit/hyperactivity disorder (ADHD), autism, pervasive developmental problems, and externalizing behavior, in addition to epilepsy and seizures (Fetene et al. 2017). In particular, the odds of autism were increased by nearly 80% among offspring of mothers who were Thyroid peroxidase antibody (TPO-Ab) positive during pregnancy (OR = 1.78), compared to mothers negative for this autoantibody (Brown et al. 2015).
Gestational immune activation and the presence of maternal autoantibodies are thought to be directly contributing to abnormal brain development mechanisms and thus involved in the pathogenesis of ASD (Hughes et al. 2018). By the analogy with ASD and other neurodevelopmental disorders, we underline the strong presence of familial autoimmunity in our PANS sample arguing that maternal infective and immunological factors may play an important role also on the PANS phenotypic expression.
In parallel, it appears interesting that among the children of our sample, anti-TPO, Thyroglobulin antibodies, TSH receptor antibodies (anti-TRAbs), and Thyroid Stimulating Hormone Receptor Antibody (anti-TSH receptor) are above the upper reference limit in the 36% of our sample, even though none of our patients had overt hypothyroidism (Table 3). This rate is much higher than the prevalence of thyroid antibodies reported in other studies where TPO-Ab positive rates ranged between 11 and 13% in different areas of the world (Hollowell et al. 2002; Amouzegar al. 2017). Longitudinal studies on general population (e.g., Li et al. 2008) demonstrated that positive thyroid antibodies were associated with an increased risk of developing hypothyroidism later in life. In particular, thyroid peroxidase antibody (TPO-Ab) measurement has been considered appropriate to identify patients at risk of developing hypothyroidism (Zelaya et al. 2010). Nevertheless, according to our data, the positive antithyroid antibodies in euthyroid children with PANS are probably an expression of a condition arising from a more general abnormal immune response.
Recurrent infections are also frequently reported in the medical history of our patients. Recurrent infections are very common in children, mostly in healthy preschool children, who can experience up to six to eight respiratory tract infections per year (Gruber et al. 2008). However, the recent findings of a population-based cohort study using Danish nationwide registers provide evidence for the involvement of infections and the immune system in the etiology of a wide range of mental disorders in children and adolescents (Köhler-Forsberg et al. 2018). The role of infectious diseases and immune dysregulation has been recently studied also in specific populations, such as individuals with fragile X syndrome (Yu et al. 2020). In PANS/PANDAS, the infection history of children is of particular interest because most PANS are suspected to be postinfectious in origin, although no single microbe, other than GABHS, has yet been consistently associated with the onset of PANS (Chang et al. 2015).
Reliably, half of our sample had different germ antibodies (IgG and/or IgM Antibodies against Mycoplasma pneumoniae, Chlamydia pneumoniae, Epstein–Barr virus, Haemophilus influenzae, and Herpes Simplex Virus –HSV- Type 1) at the clinic presentation. The most common antibodies were IgG and/or IgM against Mycoplasma and Chlamydia that are considered important causative pathogens of community-acquired infections in school-age children and adolescents. Therefore, our results are consistent with the PANS Collaborative Consortium's hypothesis that other infectious agents, particularly those with characteristically prolonged colonization, have the potential to activate PANS (Chang et al. 2015).
In addition, the nasopharyngeal culture results were often positive for different germs such as Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae (see Description in Results section). Group A beta-hemolytic streptococcus (GABHS) was found in 21% of the subjects. Therefore, the percentage of patients with an active GABHS infection as a triggering agent in our sample appears lower than that reported in previous reports (Murphy et al. 2015; Calaprice et al. 2017), although the 39% of our study subjects were positive for the antistreptolysin O antibody (ASO). However, among our 15 children with ASO >250 IU, only in 9 of them (23% of whole sample) the value exceeded the laboratory's stated upper limit of normal by twofold.
In addition to recurrent infections, allergy and atopic diseases should be considered. Atopy causes chronic inflammation of the airways that facilitate the adherence of pathogens to the respiratory epithelium and the development of respiratory infections (Mucha and Baroody 2003). In our sample, allergic and atopic diseases were described almost in one in two children (46%). However, this rate of prevalence is not far from the prevalence of any atopic diseases (40%) in general pediatric population (Christiansen et al. 2016).
Notably this high atopy prevalence is mostly due to a high prevalence of rhinoconjunctivitis (33%), with lower prevalence of asthma (13%) and atopic dermatitis (8%) (Christiansen et al. 2016). Conversely, in our sample atopic dermatitis appears as the most frequent atopic disease (59%), largely more represented than in normal pediatric population. This finding is consistent with the accumulating evidence on the association between atopic dermatitis and several children mental health disorders (es. Kandelaki et al. 2015; Catal et al. 2016). In particular, attention-deficit/hyperactivity disorder and autism (Chen et al. 2014; Lee et al. 2016; Liao et al. 2016) and anxiety and depression (Cheng et al. 2015; Becker-Haimes et al. 2017) have been associated with atopic dermatitis. In a recent Japanese study, eczema and children mental health problems (emotional symptoms, conduct problems, hyperactivity/inattention, and peer problems) were found to be significantly related, and the mean Strengths and Difficulties Questionnaire total difficulties score was significantly increased with worsening eczema status (Kuniyoshi et al. 2018).
To the best of our knowledge, there are few reports on the putative association between PANS and atopic dermatitis. A recent study (Rosa et al. 2018) described a prevalence of allergic and immune-mediated food disorders similar to the general population in a group of 69 subjects with PANS, with the exception of a higher rate of allergic rhinitis and a lower rate of atopic dermatitis than the general population. However, studies showed that different allergic diseases, not limited to atopic dermatitis, have been associated with an increased hazard of psychiatric disorders both in adults (Perugi et al. 2015; Tzeng et al. 2018) and in children (Nanda et al. 2016; Miyazaki et al. 2017).
ESR and CRP are widely used laboratory markers of systemic inflammation. A very small portion of our patients (18%) had values above the upper reference limit. However, these tests have a low index of specificity and are influenced by numerous disease factors (Bray et al. 2016). Their utility in providing valuable information in PANS has not been established yet. These inflammatory markers could have low specificity for conditions characterized by brain inflammation. Also the ANA values resulted above the upper reference limit in a relatively small part of our subjects (33%), even though the rate exceeds the estimated prevalence of positive ANAs (12–13%) in healthy pediatric population (Satoh et al. 2012).
Likewise, our data coincide with the assumption of PANS Consortium (Chang et al. 2015) that the rate of positive ANAs in patients with PANDAS and PANS is higher than the baseline.
In the present sample, a low NK cell count appears strongly associated with PANS symptoms. The recommendations from the 2013 PANS Consensus Conference (Chang et al. 2015) suggest that immune evaluation should encompass the study of lymphocyte subsets. Seventy two percent of the sample showed a percentage of NK cells below the reference limit. NK cells are a component of the innate immune system and one of the first effectors on sites of inflammation. The regulatory function of NK cells is to limit and prevent autoimmunity by killing of autologous immune cells.
Their implication in neurotoxicity and neuroprotection following CNS pathology, as well as the cross talk between NK cells and brain-resident immune cells, has been recently linked to CNS and mental disorders (Poli et al. 2013). A deranged Th17/T regulator balance and a reduced NK cell number are considered to be associated intermediate biological factors in childhood trauma, psychosis liability, and social stress reactivity in psychotic patients (Counotte et al. 2018).
A few studies have documented a decreased regulatory T cell count among children with Tourette syndrome compared with healthy controls (e.g., Kawikova et al. 2007; Bos-Veneman et al. 2011). Some studies analyzed the NK cells and white blood cell counts and activity in OCD, although with contrasting results (Denys et al. 2004; Rodriguez et al. 2017). An altered number and function of NK and T cells have been shown also in patients with schizophrenia, psychotic disorders (Karpiński et al. 2016; Vasilyeva et al. 2016), and posttraumatic stress disorder (Bersani et al. 2016). Furthermore, a consistent decrease in cytotoxic activity of NK lymphocytes (NKCA) and in lymphocyte proliferation by mitogens has frequently been reported in patients with major depressive disorder (MDD) (Ravindran et al. 1999; Zorrilla et al. 2001). A more recent research (Jeon et al. 2018) found that the NKCA was more closely related to depressive and anxiety factor scores in their 49 patients with MDD. Furthermore, the CD8-positive cell number increased and CD4/CD8 ratio decreased after 4 weeks treatment with selective serotonin reuptake inhibitors. All these findings suggest that PANS is a complex syndrome encompassing many psychiatric symptoms (anxiety, obsessive compulsive behaviors, and irritability/depression) and potentially arising from immune abnormalities, where the reduced NK cell counts could be a potential biomarker.
Finally, a large portion of our sample (56%) had overnight EEG evaluation that showed intermittent or persistent focal or generalized slow wave activity both at rest (mainly localized in temporal–frontal regions) and in vigilant state, suggesting a focal or generalized cerebral dysfunction. Notably, none of these subjects had ever suffered from epilepsy. The Consensus guideline (Chang et al. 2015) suggests that EEGs, particularly overnight evaluations, may be helpful in demonstrating focal or generalized slowing and/or epileptiform activity.
Very few reports, however, have been published on EEG evaluations of subjects with PANS/PANDAS. One study describes the results of a polysomnographic investigation of 11 children with PANDAS showing periodic limb movements and abnormalities of rapid eye movement (REM) sleep, including REM behavior disorder and nonspecific REM motor disinhibition (Gaughan et al. 2016). One more polysomnographic study on 15 subjects meeting criteria for PANS revealed that 87% of them had evidence of various forms of REM sleep motor disinhibition (excessive movement, laughing, hand stereotypes, moaning, or the continuation of periodic limb movements during sleep into REM sleep) (Gaughan et al. 2016).
No further data are yet available for results of EEG evaluations in PANS. Accordingly, improving the awareness on EEG patterns and sleep characteristics associated with PANS could be helpful to obtain a comprehensive and multidisciplinary clinical management.
The whole familial, clinical, and laboratory variables, summarized in Table 4, appear very compound and describe the PANS as a complex syndrome supported by different clinical conditions. Genetic, metabolic, infective, and environmental risk factors seem to have important implications for the assessment of such children. The lines of evidence derived from the available studies suggest to be particularly comprehensive in searching for specific laboratory biomarkers of PANS taking into account the variety of factors potentially affecting not only the mental function but also the general health of the affected children.
Summary of Pediatric Acute Onset Neuropsychiatric Syndrome Familial, Clinical, and Laboratory Variables
Limitations
The present work presents an analysis of correlation between a limited laboratory dataset of pertinent PANS signs and relevant family history conditions: a semantic connectivity map analyzing a larger set of objective parameters could be more informative about PANS construct. Another limitation of the study is the lack of a control group, as only PANS patients were included. Nevertheless, the statistic model that we have used consent to analyze a single group dataset. Comparison with patients presenting a limited association of two or more PANS criteria, but not the complete disorder may help to verify the strength of the observed associations. Finally, an enlarged sample size will be useful to confirm the present results.
Forthcoming Issues
Further studies are needed to investigate the relationships and potential diagnostic values of autoimmune/inflammatory markers. It would be meaningful to check for possible relationship between maternal autoimmune activation and PANS in offspring. In particular, a possible association between maternal thyroid autoimmune disease and PANS in offspring would be detected. Furthermore, the existence of antithyroid antibodies in clinically euthyroid PANS children could represent an indicator of a larger abnormal immune response. In particular, TPO-Ab measurement may be appropriate to help identify patients at risk of developing true autoimmune hypothyroidism.
It could be also relevant to study the possible implication of human leukocyte antigen (HLA) genes in PANS because of the increasing data on the implication of HLA genes in psychiatric and neurodevelopmental disorders (Nudel et al. 2019). To the best of our knowledge, no specific studies on NK cell counting in children with PANS are still available. Our data suggest a putative role of the NK cell counting as biomarkers in the diagnosis of PANS. EEG features are understudied in relation to their importance in lending insight into the diagnosis of localized CNS or systemic immune-mediated inflammation. Finally, the large prevalence of sleep disorders in PANS children suggests to investigate the polysomnographic features to contribute in outlining the qualitative and quantitative aspects of the sleep in this population.
Conclusion
Our study could be considered a statistical validation of the existence of the still controversial clinical entity named PANS and describes it as a clinical complex constellation of psychiatric symptoms and adventitious movements, as well as the expression of different serological variables of an autoimmune/inflammatory disease. By a data mining approach, we describe the PANS as a very specific pattern of clinical variables, each of them having a low diagnostic meaning per se, but with significant predictive values as a whole. PANS, as well as the broad spectrum of autoimmune-mediated inflammatory brain diseases, represents a rapidly developing area of medical science.
Clinical Significance
This condition challenges clinicians to find reliable biomarkers facilitating the recognition of the brain susceptibility to autoimmunity and the accurate diagnosis and treatment of children presenting with new onset neuropsychiatric symptoms. The coherence among PANS symptoms may suggest to consider the syndrome as clinical entity per se, stimulating clinicians to search for a specific combination of symptoms and signs helpful in identifying this condition. Finally, PANS should represent for clinicians a stimulus to assume a new perspective looking to the brain as an organ strictly linked with the rest of the body and potentially influenced by some general pathological conditions such as inflammatory and autoimmune diseases.
Footnotes
Acknowledgments
The authors thank all the volunteers who participated in these clinical researches, as well as the physicians and study nurses who conducted the study. The authors also acknowledge the input from Dr. Jennifer Frankovich, Dr. Margo Thienemann, and Dr. Avis Chan from the Stanford PANS/Immune Behavioral Health Clinic and Research Program at Lucile Packard Children's Hospital and Stanford University School of Medicine, California, the United States, for reviewing the article.
Disclosures
Prof. Gagliano was in the advisory boards for Eli Lilly and Shire. She is/has been involved in clinical trials conducted by Eli Lilly, Shire, Lundbeck, Janssen, and Otsuka. She has been speaker for Novartis, Eli Lilly, and Shire. Dr. Sara Carucci has collaboration within projects from the European Union (7th Framework Program) and collaboration as subinvestigator in sponsored clinical trials by Lundbeck Otsuka and Janssen Cilag. Travel support from Fidia Farmaceutici. Prof. Alessandro Zuddas served in an advisory or consultancy role for Angelini, Lundbeck, Otsuka, and EduPharma. He received conference support or speaker's fee from Angelini, Otzuka, and Takeda. He is/has been involved in clinical trials conducted by Angelini, Roche, Lundbeck, Janssen, Servier, and Otsuka. He received royalties from Oxford University Press and Giunti OS. The present work is unrelated to the above grants and relationships. Cecilia Galati, Massimo Ingrassia, Massimo Ciuffo, Maria Ausilia Alquino, Marcello G. Tanca, and Enzo Grossi have no institutional or corporate/commercial relationships to disclose.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.