
Abstract

Although the selective serotonin reuptake inhibitor (SSRI) fluoxetine is effective in youth with major depressive disorder and anxiety disorders, nearly half of these patients fail to respond. A portion of the variability in SSRI response has been attributed to pharmacogenomic factors. We retrospectively evaluated the relationship between variants in pharmacokinetic (e.g., CYP2D6) and pharmacodynamic genes (e.g., HTR2A and SLC6A4) in fluoxetine-treated youth with anxiety and depressive disorders.
Subjects were pediatric patients at the Cincinnati Children's Hospital Medical Center who underwent routine genetic testing for CYP2D6 during inpatient stay between 2013 and 2016 and returned for follow-up outpatient psychiatry care, as previously described (Poweleit et al. 2019). Patients were included if they were prescribed fluoxetine for ≥28 days and had an anxiety and/or depressive disorder. After IRB approval, charts were reviewed for demographic information, prescriptions, and measures of clinical response. Response was defined by a Clinical Global Impressions-Improvement score (CGI-I) of ≤2 within 6 months of starting treatment. Banked DNA was genotyped for HTR2A rs7997012 and rs6313, as well as SLC6A4 5-HTTLPR and rs25531, as previously described (Poweleit et al. 2019). Time to response was evaluated with the log-rank test (GraphPad Prism version 8). Response rates were examined using generalized linear models (R version 3.5.1) and findings were considered statistically significant at p = 0.05.
The cohort (N = 164, age: 14.3 ± 2.2 years) was primarily female (75.6%) and white (83%) with a diagnosis of a depressive disorder (29.9%), anxiety disorder (9.1%), or comorbid depression/anxiety (61.0%). The maximum fluoxetine dose was 30 ± 21 mg/day and treatment duration was 414 ± 609 days. Fluoxetine response rate was 47.6% at 6 months.
Patients with a HTR2A rs6313 GG genotype responded faster than those with AG/AA genotypes (p = 0.020, Fig. 1A), which is inconsistent with a previous report examining response to several SSRIs in adolescents (Brent et al. 2010). This association remained significant in a multivariable model accounting for duration of fluoxetine treatment, SLC6A4 expression level, maximum fluoxetine dose, number of concomitant psychotropic medications, and adherence (p = 0.011). Although an effect was not observed between SLC6A4 expression and faster response (p = 0.41, Fig. 1B), patients with both HTR2A rs6313 GG genotype and low SLC6A4 expression were associated with faster response at 6 months than other SLC6A4 expression and HTR2A rs6313 genotypic combinations (p = 0.021, Fig. 1C). HTR2A rs7997012 and CYP2D6 metabolizer status were not significantly associated with categorical response (p = 0.078 and p = 0.092, respectively) or time to response (p = 0.36 and p = 0.18, respectively). The lack of association between CYP2D6 phenotype and clinical response to fluoxetine is consistent with a previous study in youth, in which CYP2D6 phenotype was associated with pharmacokinetics, but not clinical improvement (Gassó et al. 2014). In addition, the Clinical Pharmacogenetics Implementation Consortium guideline for fluoxetine suggests that it may be reasonable to select an alternative SSRI not extensively metabolized by CYP2D6 due to conflicting/inconclusive data (Hicks et al. 2015). This study suggests that selecting an alternative SSRI (with potentially less efficacy in children) may not be necessary based on CYP2D6 but that variants in HTR2A may influence how fast patients respond.
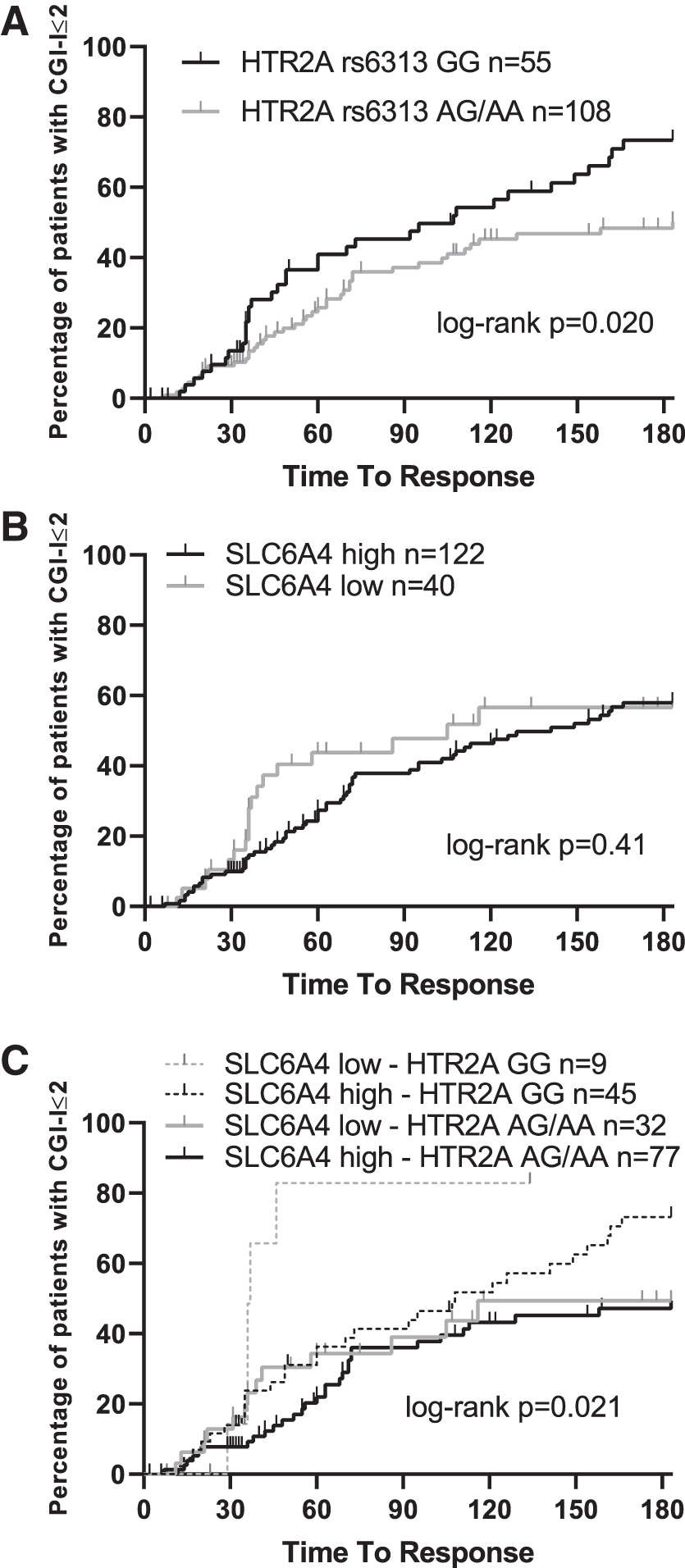
HTR2A rs6313 and SLC6A4 expression levels influence fluoxetine response.
Footnotes
Acknowledgments
Samples from the Discover Together Biobank at Cincinnati Children's Research Foundation were used in this study. We thank the Discover Together Biobank for support of this study, as well as participants and their families, whose help and participation made this study possible.
Disclosures
Dr. J.R.S. has received research support from the National Institutes of Health (NIMH/NIEHS/NICHD), the Patient-Centered Outcomes Research Institute, as well as Allergan, Otsuka, and Neuronetics. He has received material support from and provided consultation to Myriad Genetics and receives royalties from the publication of two texts (Springer). Dr. J.R.S. serves as an author for UpToDate, an associate editor for Current Psychiatry and has received honoraria from CMEology. Dr. L.B.R. has received research support from the National Institutes of Health (NICHD) and BTG, International Ltd. The remaining authors report no financial conflicts of interest.