
Abstract
Objective:
To review the use of aripiprazole in children and adolescents.
Methods:
Medline and Embase databases were systematically searched using the keywords aripiprazole and child or adolescent over the period from 2000 to 2019. The initial screen yielded 163 publications, from which 99 studies were reviewed.
Results:
Aripiprazole is one of the most widely prescribed atypical antipsychotics. Like others, its use in children and adolescents is becoming commonplace and occurs in off-label indications. Aripiprazole has proven efficacy for several indications in children and adolescents, including schizophrenia, bipolar disorder, Tourette's syndrome, and behavioral impairments associated with autism and intellectual disability. Adverse effects are more important in children and adolescents than adults, particularly weight gain, drowsiness, extrapyramidal effects, and metabolic effects, even though the latter may appear less important than with other atypical antipsychotics. Severe adverse effects often occur in multiple-prescription settings. At present, postprescription monitoring is very poor.
Conclusion:
Aripiprazole has proven efficacy for several indications in children and adolescents. However, its use requires clinical and paraclinical monitoring to assess the occurrence of adverse events that may challenge the benefit/risk ratio. In addition, off-label prescriptions should be limited, as they appear to account for a significant proportion of aripiprazole use worldwide.
Introduction
General context: antipsychotics in children and adolescents
Available evidence shows that psychiatric consultations for children resulting in prescription of an antipsychotic notably increased about eightfold between 1993 and 2009 in the United States. By 2009, use of atypical antipsychotics became a trend of concern worrying U.S. control authorities since psychiatrists prescribing an antipsychotic do so much more often in children (68%) and adolescents (71%) than in adults (50%) (Olfson et al. 2012a). This increase in the prescription of antipsychotics is also found among very young children (2–5 years). Between 2000 and 2007, a study found that the prevalence of prescriptions in minors rose from 0.78% to 1.58% in extremely varied indications, such as autism spectrum disorders or intellectual disability (28%), attention-deficit/hyperactivity disorder (ADHD; 24%), and disruptive disorders (13%) (Olfson et al. 2010). In that study, more than half of the children had not been assessed by a psychiatrist.
It appears that in the United States, the prevalence of antipsychotic prescriptions is high and often does not comply with Food and Drug Administration (FDA) recommendations. Several estimates calculated from health insurance databases have yielded high figures: 4.2% of prescriptions among children 6–17 years of age (Crystal et al. 2009) and 2.7% of prescriptions among children in the care of Child Welfare (Dosreis et al. 2011). A study by Matone et al. (2012) distinguished age groups between 3 and 18 years and found prevalences of 0.4% between 3 and 5 years, 2.1% between 6 and 11 years, and 3.7% between 12 and 18 years. Finally, a study by Olfson et al. (2012a) on changes between 1993 and 2009 showed that in 2009, the prevalence of antipsychotic prescriptions was 1.83% in children and 3.76% in adolescents compared to 6.18% in adults. The reasons for this prescription boom are summarized elsewhere (Harrison et al. 2012). The main factors identified include a trend toward greater acceptance of psychotropic drug prescriptions in children, better knowledge of these drugs combined with an awareness of the disorders and frequency of psychological suffering in children, limited access to nonpharmacological treatments, a more pressing demand for rapid and inexpensive treatment, and a very wide disparity in time available and reimbursement rates for treatment of behavioral problems (this is particularly true in vulnerable populations in which treatment options are extremely limited in terms of supply and access to care).
Data regarding non-U.S. countries are sparse. While the prevalence of antipsychotic prescriptions for children and adolescents remained low from 2004 to 2008 (<4/10,000 per year), there has been a slight increase in recent years (Clavenna et al., 2011). This trend was found in Germany, with an increase of antipsychotic prescriptions from 2.3/10,000 in 2005 to 3.2/10,000 in 2012 (Bachmann et al. 2014). The most recent large comparative study by Hálfdánarson comparing up to 16 countries showed that the increase in prescription of atypical antipsychotic drugs still continues and varies for adolescents from country to country, with Lithuania prescribing the least and Taiwan and the United States prescribing the most (Hálfdánarson et al. 2017).
The case of aripiprazole
Aripiprazole is an atypical second-generation antipsychotic drug, which is a partial agonist of dopamine D2 receptors and serotonin 5-HT1A receptors and a partial antagonist of serotonin 5-HT2A receptors. It is metabolized primarily in the liver by CYP2-D6 and CYP3-A4 enzymes. Its elimination half-life is 75 hours for rapid metabolizers and 150 hours for slow metabolizers. However, it should be noted that these data were obtained primarily in adults. While it has been prescribed in adults since the early 2000s, studies in children and adolescents and their use are more recent. Worldwide marketing authorizations available for aripiprazole in children and adolescents are summarized in Table 1; the year of first marketing authorization is usually for only one indication.
Aripiprazole in Children and Adolescents: Worldwide Agencies' Authorization (Until April 2019)
Modified from Perraudin et al. (2018).
BP, bipolar disorder; SCZ, schizophrenia.
The literature review presented in this study has endeavored to report as broadly as possible on the use of aripiprazole based on publicly available data. In terms of presentation, epidemiological studies in general or specific populations, short- and medium-term efficacy studies, and studies reporting side effects, whether in the context of efficacy or naturalistic studies, were distinguished. However, data exploited from pharmacovigilance resources and isolated case reports may enable us to identify recent trends, if any, as well as rare side effects that are sometimes only identified after prolonged use. As shown in Table 1, there is a fairly wide disparity in the years of first authorization of aripiprazole in children and adolescents since it occurred as early as 2007 in the United States, whereas for European countries and Canada, the first authorization occurred 5 years later (2012).
Methods
Medline and Embase databases were systematically searched with the keywords aripiprazole and child or adolescent from 2000 to 2019 (end of search, April 9, 2019). Titles and abstracts of selected articles were searched to ensure they were relevant to the use of aripiprazole in children and adolescents. Three subthemes were distinguished in this review: epidemiological data regarding aripiprazole, efficacy studies, and tolerance. For the latter two subthemes, a summary table was produced of the different studies selected and a corresponding flow chart was presented with the reasons each article was kept in the subtheme (list of excluded studies provided in the Supplementary Data).
Results
The results are presented distinguishing U.S. from non-U.S. epidemiological data (when available) to avoid extrapolations or shortcuts to national reality based on data that would only represent the United States. Indeed, the prescription of psychotropic drugs also depends on cultural and sociological aspects as well as access to care. Thereafter, the results detail efficacy and tolerance studies.
U.S. epidemiological data on aripiprazole
Several studies starting in 2010 have examined how prescribing physicians monitor children exposed to atypical or second-generation antipsychotic drugs, including aripiprazole. These studies also sought to distinguish which atypical antipsychotic was prescribed. They made it possible to assess the relative frequency of prescription of one drug compared to others within the same class, although rarely an estimate of prevalence (Raebel et al. 2014; Chen et al. 2018; Coughlin et al. 2018). In a large U.S. study on the monitoring of diabetic risk in 16,000 children and adolescents from 10 North American sites receiving an atypical antipsychotic, 31% were receiving aripiprazole (the first prescription being risperidone, 43%), leading to the conclusion that monitoring was very poor since only 11% of the children and adolescents had their glucose or hemoglobin A1C monitored (Raebel et al. 2014). Several U.S. states faced with a worrying increase in the prescription of atypical antipsychotic drugs in toddlers have decided to implement monitoring by prior agreement with an expert before prescription reimbursement. This control led to a moderate drop in prescriptions (by a factor of 1.31–1.75) after its implementation in the four states it was applied (Zito et al. 2018).
For aripiprazole, the most accurate data are from the FDA's pediatric focus safety review (Nevo et al. 2017). The number of patients receiving aripiprazole between June 2014 and November 2016 in the United States is presented in Table 2 according to age; more than 500,000 minors received aripiprazole during that period. According to 10th revision of the International Classification of Diseases (ICD-10) diagnostic reports, the three most frequently reported indications were infantile autism, affect psychoses, and depressive disorder in 6- to 12-year olds and affect psychoses, manic-depressive illness, and infantile autism in 13- to 17-year olds. The same report summarized adverse events reported to the FDA adverse event reporting system from May 2011 to November 2016. The raw data show 1960 reports, including 891 serious and 37 fatal events in children younger than 17 years. After analysis, the FDA identified 78 cases (46 boys, 31 girls, and 1 case not specified) of serious/severe adverse events, including 14 deaths in children and adolescents. The children who died were exposed to aripiprazole dosages of 3–30 mg. Thirteen deaths occurred in children or adolescents 5–17 years of age, including five suicides, one overdose classified as unintentional, one malignant syndrome, one hyperthermia, one cardiorespiratory arrest, one metabolic disturbance, one malignant condition, and two unlabeled causes. The fourteenth death occurred in a premature infant who had transplacental exposure to aripiprazole prescribed to his mother. The death occurred at 6 days of age in the context of Fallot's tetralogy. No specific pattern of death was retained. The 64 severe nonlethal adverse events included 20 cases of clinical worsening with changes in dosage or formulation (including 16 cases of switching from the reference dosage form of Otsuka to a generic form), 15 cases of worsening (or lack of improvement) of pathology, 5 strokes, 3 gynecomastia, 3 with hallucinations, 2 with pancreatitis, 2 nonalcoholic liver steatoses, and 2 cases of false-positive amphetamine screening. Other severe adverse events (n = 12) were reported in isolation.
Nationally Estimated Number of Patients Who Received Prescriptions for Oral Aripiprazole from U.S. Outpatient Retail Pharmacies, Stratified by Patient Age, June 2014 Through November 2016
Summing across patient age bands is not advisable because this will result in overestimates of patient counts. Patient age subtotals do not sum exactly (>100%) due to patient aging during the study period. Patients may be counted more than once in the individual age categories.
Source: Nevo et al. (2017).
Epidemiological non-U.S. data on aripiprazole
Specific aripiprazole data outside France, Germany, and Canada were not found, although the available prevalence of aripiprazole in children and adolescents was extracted from Halfdarnarson et al. and compared with the most prescribed antipsychotic in this age group (risperidone and quetiapine) by country (Fig. 1). Figure 1 shows that U.S. prescriptions are higher compared to European and Asian countries, with some exceptions, such as Taiwan (where the first prescribed antipsychotic was prochlorperazine), New Zealand, and Iceland. In most countries in 2014, aripiprazole prevalence was lower than 20/10,000.

2014 Prevalence of aripiprazole, risperidone, and quetiapine in children and adolescents (≤19 years old) from 13 countries (data extracted from Hálfdánarson et al. 2017).
In a Canadian general population study covering all of 2014, 7000 children receiving antipsychotic drugs were studied, including 4000 receiving risperidone, 2000 receiving quetiapine, and 1300 receiving aripiprazole (Chen et al. 2018). Again, indications were mostly off-label, such as ADHD, conduct disorder, and anxiety. The authors' observations were particularly worrying since the recommended monitoring of possible side effects was very limited and poorly carried out regardless of prescribed drug. Another study found the same results in terms of monitoring. In a longitudinal follow-up of 294 children and adolescents receiving an antipsychotic in a level 3 Canadian center, evaluation at 1 year showed very poor compliance with recommendations in terms of monitoring (Coughlin et al. 2018). In Germany, data from a statutory health insurance company from 2005 to 2012 yielded low rates of aripiprazole prescription. Of over 24,723 antipsychotic prescriptions for children and adolescents in 2012, only 4% related to aripiprazole (compared with 49.6% for risperidone) (Bachmann et al. 2014).
In France, two epidemiological studies explored changes in prescriptions over time. Based on health insurance data of a representative sample (at 1/97), Bénard-Laribière et al. (2019) found an increase in the use of antipsychotics in pediatric patients between 2007 and 2014 without an increase in off-label prescriptions (16% in period 1 vs. 11.1% in period 4). Nevertheless, the most frequently prescribed off-label drug was aripiprazole. This increase in antipsychotic drug use in pediatric patients was not found in adults over an almost identical period (2006–2013) (Montastruc et al. 2018). In the latter study, the increase in prescription of antipsychotics to minors was 39%. The prevalence data per drug were not described by age group, but for all ages. However, in the online supplements provided by Bénard-Laribière et al. (2019), drug-by-drug data found on off-label prescriptions in minors revealed aripiprazole was the drug most concerned, with an average off-label prescription prevalence varying from 15% to 29.4% .
Very little French data are available in a specific context (e.g., patients with autism). Nevertheless, the trends are identical. The prescription of psychotropic drugs outside legal authorization in pediatric hospitals appeared to be very frequent. In a 6-month study, including 1600 prescriptions for 472 patients, Winterfeld et al. (2009) found 68% of prescriptions were outside legal authorization, and 69% of these were for atypical antipsychotics, with risperidone being the most frequently prescribed. The most frequent off-label indications were anxiety, behavioral disorders, and pain. In addition, in a survey of parents of patients with autism (n = 393, mean age = 12 years), Cravero et al. (2017) reported that 52% received a psychotropic drug, of which 35% continued it. Atypical (23%) and typical antipsychotics (13%) were the most prescribed. The adverse effects reported by parents increased when atypical antipsychotics were prescribed, when there was polymedication, or when the prescription appeared to be off-label.
Finally, a study of French pharmacovigilance data between 1985 and 2017 found 247 reports of adverse reactions in children (2–12 years old) for atypical antipsychotics. A total of 210 patients received risperidone, 35 received aripiprazole, 1 received clozapine, and 1 received olanzapine. A total of 173 adverse reactions corresponded to off-label prescriptions, including all 35 cases reported for aripiprazole. Of the 173 off-label prescriptions, the study reported 90 nonserious and 83 severe adverse events, the majority of which were neurological (followed by endocrine and psychiatric). This study points out that the severity of adverse events inversely correlated with age (Poudroux et al. 2018). Unfortunately, few details were available as this study was only published as an abstract/poster in a congress.
Efficacy data
The flowchart corresponding to studies selected to explore and summarize efficacy data for aripiprazole is presented in Figure 2. Studies were separated according to their originality or meta-analytic nature.
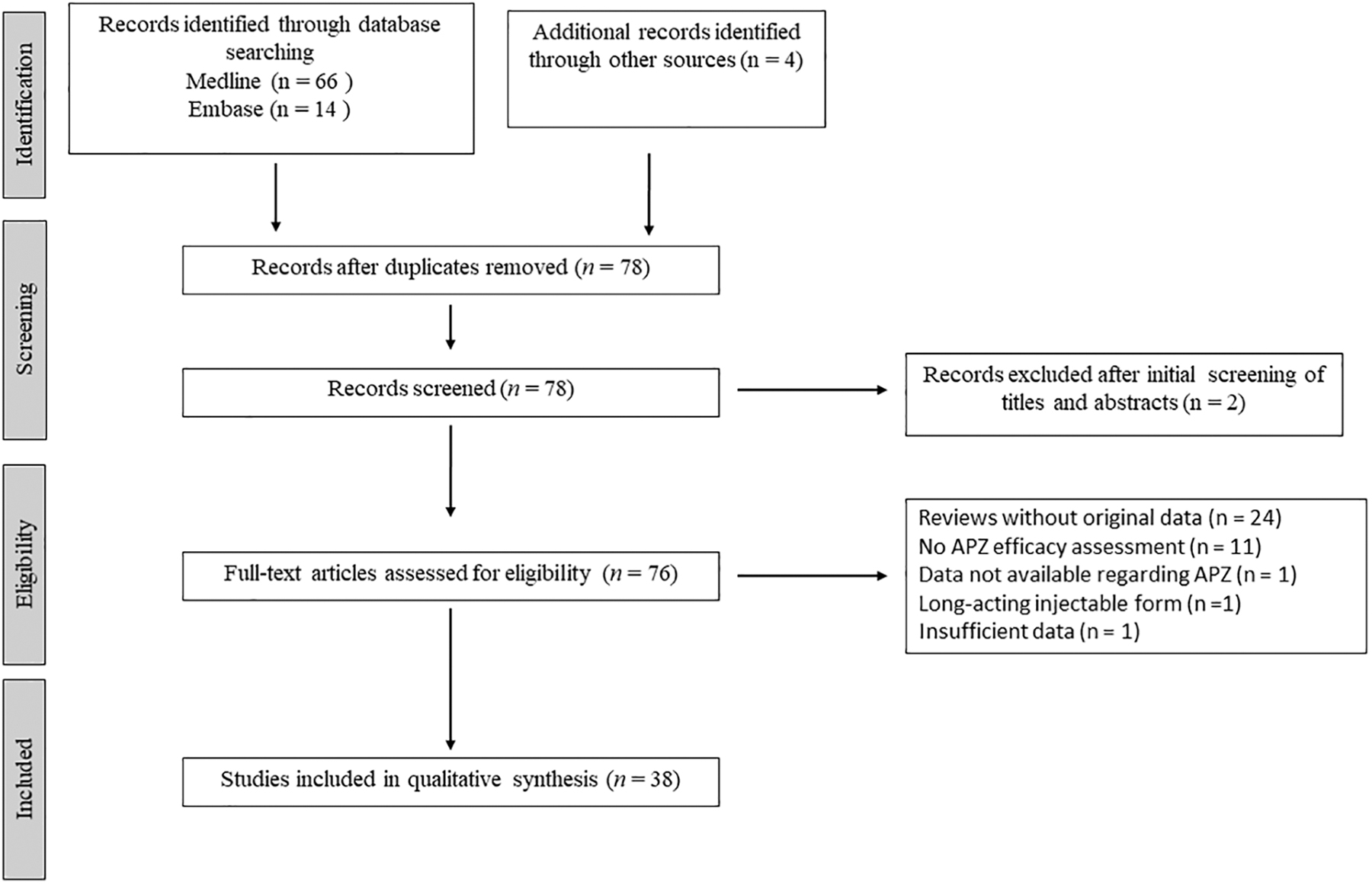
Diagram of the study selection flowchart for evaluating aripiprazole efficacy.
Table 3 summarizes all of the efficacy studies found to include at least one arm with aripiprazole in children and adolescents. The studies were separated according to the quality of the methodology by distinguishing between randomized controlled studies by primary indication and other studies (open-label, randomized, and no control group). For each of these studies, Table 3 lists the authors and year, age and primary indication of the study, number of subjects included, dosage of aripiprazole received, nature of the control group when available, duration of the study, efficacy measures used, and main results with qualitative comments.
Efficacy Studies Including One Arm with Aripiprazole in Children and Adolescents
95% CI, 95% confidence interval; ABC, Aberrant Behavior Checklist; ABC-H, ABC-Hyperactivity/noncompliance; ABC-I, ABC-Irritability; ABC-IS, ABC-Inappropriate speech; ABC-S, ABC-Stereotypic behavior; ABC-SW, ABC-Lethargy/social withdrawal; ADHD, attention-deficit/hyperactivity disorder; ADHD-RS-IV, ADHD-Rating Scale-IV; APZ, aripiprazole; ARS-IV, DSM-IV ADHD Rating Scale; ASD, autism spectrum disorder; BP (-I, NOS), bipolar disorder (type I, not otherwise specified); BYI-II, Beck Youth Inventories-second edition; CBCL, Child Behavior Checklist; CBT, Cognitive Behavioral Therapy; CCTT, Children's Color Trails Test; CD, conduct disorder; CDRS-R, Children's Depression Rating Scale-Revised; CGAS, Children's Global Assessment Scale; CGI (-S, -I), Clinical Global Impression scale (-Severity, -Improvement); CGSQ, Caregiver Strain Questionnaire; CMRS-P, Child Mania Rating Scale-Parental Version; CPRS (-H, -I): Conners' Parent Rating Scale (-Hyperactivity, -Inattention); CPT (-II), Conners' Continuous Performance Test (-version II); CY-BOCS, Child Yale–Brown Obsessive-Compulsive Scale; CYC, cyclothymic disorder; DMDD, disruptive mood dysregulation disorder; EOS, early-onset schizophrenia; GBI, Global Behavior Inventory; HR, hazard ratio; ID, intellectual disability; KADS, Kutcher Adolescent Depression Scale; MPH, methylphenidate; NR, not reported; OCD, obsessive-compulsive disorder; ODD, oppositional defiant disorder; OLT, open-label trial; PANSS, Positive And Negative Syndrome Scale; PARS, Pediatric Anxiety Rating Scale; PBO, placebo; PedsQL, Pediatric Quality of Life Inventory; PQ-LES-Q, Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire; PSI (-SF), Parenting Stress Index (-Short Form); RAAPP, Rating of Aggression Against People and Property; RSP, risperidone; SAICA, Social Adjustment Inventory for Children and Adolescents; SCWT, Stroop Color and Word Test; SCZ, schizophrenia; SNAP-IV, Swanson, Nolan, and Pelham, version IV; SSRI, selective serotonin reuptake inhibitor; T-DSM-IV, Turgay DSM-IV based child and adolescent behavior disorders screening and rating scale; TRF, Teachers Report Form; TS, Tourette's syndrome; VABS, Vineland Adaptive Behavior Scale; VFT, Verbal Fluency Test; WCST, Wisconsin Card Sorting Test; WJ-III-ACH, Woodcock-Johnson III Achievement test; YGTSS, Yale Global Tic Severity Scale; YMRS, Young Mania Rating Scale.
Four double-blind, randomized, controlled trials (RCTs) investigated aripiprazole in child and adolescent bipolar disorder and included 458 children and adolescents (Tramontina et al. 2009; Findling et al. 2012, 2013, 2017). Most studies found a significant improvement in the manic symptoms, leading to the authorizations listed in Table 1. For schizophrenia, there is only one major study involving 302 patients (Findling et al. 2008a). There, the improvement was significant and led to the approval of aripiprazole in this indication in some countries. Two RCTs that included 494 patients concerned Tourette's indication (Yoo et al. 2013; Sallee et al. 2017). Again, there was a significant improvement with aripiprazole, which has made it possible to obtain approval in some countries. Finally, four studies involving 493 patients were conducted on behavioral impairments associated with autism and/or intellectual disability (Marcus et al. 2009; Owen et al. 2009; Findling et al. 2014; Ichikawa et al. 2017). In most of the studies, aripiprazole was significantly superior to placebo, which led to its approval for this indication in some countries. The most recent RCT compared aripiprazole and risperidone for the indication of ADHD in children 3–6 years old (Razjouyan et al. 2018). While there was no significant difference between the two groups, both groups showed a substantial improvement in symptomatology at the end of the trial. No agency authorization is available to date for ADHD.
Finally, 14 studies that are less methodologically sound are also reported in Table 3: open-label studies with or without randomization (Findling et al. 2008b, 2009, 2011; Marcus et al. 2011a; Ercan et al. 2012; Ghanizadeh et al. 2014; Ghanizadeh 2016; Lamberti et al. 2016; Wang et al. 2016; Kim et al. 2018; Pan et al. 2018) and retrospective studies on files (Olfson et al. 2012b; Ercan et al. 2015; Akyol Ardic et al. 2017) in indications corresponding to FDA approval or off-label indications, such as ADHD, disruptive disorder, emotional regulation disorder, conduct disorder, and resistant obsessive-compulsive disorder. For most of these indications, a significant improvement is reported between the beginning and end of treatment, but the absence of a control group and, in particular, a placebo control group makes it very difficult to conclude that aripiprazole is useful for these nonauthorized indications.
Table 4 lists studies describing meta-analyses evaluating the efficacy of aripiprazole against placebo or possibly against another class of antipsychotic drugs, particularly risperidone. Surprisingly, only two indications were explored in the meta-analyses. First, behavioral impairments associated with autism and intellectual disabilities were explored in eight different meta-analyses (Varni et al. 2012; Cohen et al. 2013; McQuire et al. 2015; Fung et al. 2016; Hirsch and Pringsheim 2016; van Schalkwyk et al. 2017; Maneeton et al. 2018; Fallah et al. 2019). These meta-analyses reported the superiority of aripiprazole over placebo, but no difference between aripiprazole and risperidone in improving behavioral problems associated with autism and intellectual disability was found. No meta-analysis reported efficacy for autistic symptoms. The second indication explored in meta-analyses concerns tics and Tourette's syndrome. This time, four meta-analyses compared aripiprazole with placebo and another atypical (risperidone) or typical (haloperidol and tiapride) antipsychotic drug or topiramate (Yang et al. 2015; Liu et al. 2016; Zheng et al. 2016; Wang et al. 2017). Aripiprazole was found to be superior to placebo in improving tics, but not superior to other antipsychotics.
Meta-Analyses Available Assessing Aripiprazole Efficacy in Children and Adolescents by Indications
95% CI, 95% confidence interval; ABC, Aberrant Behavior Checklist; ABC-H, ABC-Hyperactivity/noncompliance; ABC-I, ABC-Irritability; ABC-IS, ABC-Inappropriate speech; ABC-S, ABC-Stereotypic behavior; ABC-SW, ABC-Lethargy/social withdrawal; ADHD, attention-deficit/hyperactivity disorder; APZ, aripiprazole; ASD, autism spectrum disorder; BP (-I), bipolar disorder (type I); CGI (-S), Clinical Global Impression scale (-Severity); HLP, haloperidol; MD, mean difference; OLT, open-label trial; OR, odds ratio; PBO, placebo; PedsQL, Pediatric Quality of Life Inventory; RBCT, randomized blinded controlled trial; RCT, randomized controlled trial; RSP, risperidone; SMD, standardized mean difference; TIA, tiapride; TOP, topiramate; TS, Tourette's syndrome; YGTSS, Yale Global Tic Severity Scale; YMRS, Young Mania Rating Scale.
Tolerance data
Figure 3 summarizes studies retained to assess aripiprazole tolerance in children and adolescents. These studies were classified according to their design, distinguishing between RCTs and open-label trials where the primary objective was to study the tolerance of aripiprazole in children and adolescents, meta-analyses, and case reports describing mainly rare side effects in children and adolescents. It was important to retain these case reports as rare side effects are usually identified in these postmarketing reports.

Diagram of the study selection flowchart for evaluating aripiprazole tolerance.
Table 5 summarizes tolerance studies, in RCT (Mankoski et al. 2013; Findling et al. 2014), open-label (Marcus et al. 2011b; Ho et al. 2012; Ichikawa et al. 2018), naturalistic (Germanò et al. 2014; Carbon et al. 2015; Al-Dhaher et al. 2016; Rafaniello et al. 2016; Pringsheim et al. 2017; Pozzi et al. 2019), or retrospective studies (Diomšina et al. 2015; Kimura et al. 2015; Rubin et al. 2015; Jakobsen et al. 2016; Yoon et al. 2016; Palanca-Maresca et al. 2017; Stassinos and Klein-Schwartz 2017). Table 5 does not include efficacy studies described in previous tables as the main objective in these studies was efficacy, especially as they generally describe tolerance, most often in the short term. These studies were in any case included in the meta-analyses.
Studies Assessing Aripiprazole Safety and Tolerability in Children and Adolescents
95% CI, 95% confidence interval; AAPCC, American Association of Poison Control Centers; ADHD, attention-deficit/hyperactivity disorder; AE, adverse effect; AIMS, Abnormal Involuntary Movement Scale; AN, AP naive; AP, antipsychotic; APZ, aripiprazole; ASD, autism spectrum disorder; BARS, Barnes Akathisia Rating Scale; BFCRS, Bush Francis Catatonia Rating Scale; BMI, body mass index; BP, bipolar disorder; CHL, cholesterol; CNS, central nervous system; ECG, electrocardiogram; EPS, extrapyramidal symptoms; ESRS, extrapyramidal Symptom Rating Scale; FAERS, Food and Drug Administration Adverse Event Reporting System; Glu, glucose; HDL-CHL, high-density lipoprotein-CHL; ID, intellectual disability; LDL-CHL, low-density lipoprotein-CHL; LOCF, last observation carried forward; NMS, neuroleptic malignant syndrome; NPDS, National Poison Data System; NR, not reported; OCD, obsessive-compulsive disorder; ODD, oppositional defiant disorder; OLP, olanzapine; OR, odds ratio; PAE, prior antipsychotic exposure; PBO, placebo; PDD, pervasive developmental disorder; PRL, prolactin; QTc, corrected QT interval, Bazett's (QTcB), United States Food and Drug Administration (FDA) Neuropharmacology Division (QTcN), and Fridericia's (QTcF) formulas; QTd, QT interval dispersion; QTP, quetiapine; RBCT, randomized blinded controlled trial; RR, relative risk; RSP, risperidone; SAS, Simpson-Angus Scale; SCZ, schizophrenia; SD, standard deviation; SGA, second-generation antipsychotic; TdP, torsade de pointes; TESS, Treatment Emergent Symptoms Scale; TG, triglycerides; TS, Tourette's syndrome.
All known side effects of other antipsychotic drugs are present in the studies listed in Table 5, particularly weight gain, which is more pronounced in children who have never been exposed to antipsychotic drugs and more common in younger subjects (Mankoski et al. 2013). Neurological and extrapyramidal effects as well as drowsiness are also quite common. A 16-month study by Findling et al. (2014) reported 25% weight gain, 15% drowsiness, 17% extrapyramidal effects, and a few cases of respiratory infections, constipation, and vomiting. However, in that long-term study, the authors did not describe any difference in metabolic parameter changes or an increase in prolactin, but rather a decrease in serum prolactin. Open or naturalistic studies of a certain duration clarify certain points: overall, the majority of side effects are mild or moderate in severity (Ichikawa et al. 2018).
For example, a 10-month study comparing patients on aripiprazole and risperidone showed that weight gain on aripiprazole may be slightly lower at the start of treatment, but higher afterward (Pringsheim et al. 2017), and discontinuation of therapy due to metabolic or extrapyramidal effects occurred in 17% and 10% of cases, respectively. A few studies have also investigated the effects on cardiac conduction and, in particular, some electrocardiogram (ECG) parameters (Germanò et al. 2014; Palanca-Maresca et al. 2017). A 20-month study of ∼50 patients on aripiprazole reported the incidence of corrected QT interval (QTc) prolongation (>450 mseconds) was 8.7%, with only one case of QTc prolongation detected after 12 months (Palanca-Maresca et al. 2017). Interestingly, most of the QTc abnormalities found were in patients taking ADHD medication, and no case of sudden death was reported. Another report involving a database of 22,000 patients revealed that those exposed to aripiprazole as the first treatment had a 1.58-fold higher risk of type II diabetes versus those taking risperidone, which is the reference in this database analysis (Rubin et al. 2015). Nevertheless, the risk of diabetes for all atypical antipsychotic drugs combined was 1.51. Two years before the FDA report on serious adverse events with aripiprazole published in 2017, an FDA database search found that 2500 cases reported had serious side effects defined as neuroleptic malignant syndrome, QT prolongation, leukopenia, and suicide attempts (Kimura et al. 2015). A significant signal was retained regarding the potential of aripiprazole to induce neuroleptic malignant syndrome and suicide attempts. Finally, a study of poison control center database reports of accidental exposure to aripiprazole in children younger than 6 years revealed that side effects were mostly minor, and only 0.8% major side effects were reported, with no deaths (Stassinos and Klein-Schwartz 2017).
Table 6 summarizes the six available meta-analyses evaluating the safety of aripiprazole in children and adolescents, generally in comparison to other antipsychotic drugs or placebo (De Hert et al. 2011; Pringsheim et al. 2011a; Robb et al. 2011; Cohen et al. 2012; Almandil et al. 2013; Jensen et al. 2015). Only two are detailed in this study, the first by Cohen et al. (2012) because it is the most important in terms of inclusion of patients on atypical antipsychotics using a Bayesian method. Their meta-analysis summarizes the side effects of each antipsychotic relative to placebo in a semiquantitative mode and shows that aripiprazole has a particular profile of side effects, including somnolence/sedation, weight gain, and relatively frequent extrapyramidal effects. In contrast, aripiprazole had no hyperprolactinemic effect and little short-term effect on metabolic parameters. The second study detailed herein was by Jensen et al. (2015) because it focused on cardiac side effects reported in 14 studies with aripiprazole arms for a total of 862 exposed patients. It appears that, on average, aripiprazole significantly decreases the QTc interval. The change in QTc correlated with the dosage received since the higher the dose, the more QTc tends to decrease.
Meta-Analyses Available Assessing the Safety and Tolerability of Aripiprazole in Children and Adolescents
95% CI, 95% confidence interval; ADHD, attention-deficit/hyperactivity disorder; AE, adverse effect; AIMS, Abnormal Involuntary Movement Scale; APZ, aripiprazole; ASD, autism spectrum disorder; BARS, Barnes Akathisia Rating Scale; BMI, body mass index; BP, bipolar disorder; CD, conduct disorder; CHL, cholesterol; ECG, electrocardiogram; EPS, extrapyramidal symptoms; Glu, glucose; HDL-CHL, high-density lipoprotein-CHL; LDL-CHL, low-density lipoprotein-CHL; LOCF, last observation carried forward; NR, not reported; OLT, open-label trial; OR, odds ratio; PBO, placebo; PRL, prolactin; QTc, corrected QT interval; RBCT, randomized blinded controlled trial; SAS, Simpson-Angus Scale; SCZ, schizophrenia; TG, triglycerides; TS, Tourette's syndrome.
Finally, Supplementary Table S1 lists all 19 case reports (corresponding to a total of 22 observations) mentioning aripiprazole tolerance problems in children and adolescents (McLaren et al. 2010; Patel et al. 2011; Star et al. 2012; Stern and Trieu 2012; Panigrahi et al. 2013; Thabet et al. 2013; Párraga and Sherman 2015; Hoşoğlu et al. 2016; Mohapatra 2016; Pinnaka et al. 2016; Binici and Güney 2017; Fatima and Mottola 2017; Gunes 2017; Han et al. 2017; Lamberti et al. 2017; LeRiger et al. 2017; Sridaran and Nesbit 2017; Boyer et al. 2018; Işik and Çam Ray 2019). Accountability is sometimes difficult to attribute since 11 of the 22 observations were in a polyprescription context and 4 adverse events occurred when a similar history was known or when an autoimmune medical comorbidity was reported. In total, eight observations report known side effects that are not detailed in this study (in particular, observations of particularly severe neurological side effects). In one case, rhabdomyolysis in the context of coprescription was observed (Star et al. 2012). Another rather complex case of a 3-year-old girl reports a history of epilepsy and encephalopathy in a context without any previous history (Thabet et al. 2013). Observation of neuroleptic malignant syndrome without fever that clinically evokes malignant catatonia was described in an 8-year-old boy after 3 days of aripiprazole initiation (Sridaran and Nesbit 2017), and one case of pseudoneutropenia was reported (Pinnaka et al. 2016). Three cases of epistaxis have also been reported, including one with gingival bleeding (Hoşoğlu et al. 2016; Binici and Güney 2017). Finally, two cases of secondary enuresis were reported (Gunes 2017), as well as one case of urinary retention in an 11-year-old boy with severe intellectual disability (Boyer et al. 2018).
Conclusion
In total, the following trends can be identified. First, aripiprazole is one of the most widely prescribed atypical antipsychotics, probably due to a well-established efficacy profile in two to four approved indications according to various countries and a safety profile that is somewhat different from other atypical antipsychotics (Cohen et al. 2012). Like other atypical antipsychotics, its use in children and adolescents is becoming commonplace and occurs in off-label indications. Second, compared with what is known about aripiprazole in adults, it appears that adverse effects are more important in children and adolescents, particularly weight gain, drowsiness, extrapyramidal effects, and metabolic effects, even though the latter may appear less important than with other atypical antipsychotics (Table 5).
Moreover, severe adverse effects often occur in polyprescription settings. Third, the fact that aripiprazole was marketed contemporaneously with the Pediatric Act has been very beneficial in terms of the number of studies available. These studies detail relatively well clinical (e.g., weight gain and extrapyramidal symptoms) and paraclinical (e.g., serum prolactin; serum cholesterol; and ECG) adverse events. This is not necessarily the case for older atypical antipsychotics, such as olanzapine. On the other hand, if the prescription of atypical antipsychotics and aripiprazole is regarded as straightforward by the physician or psychiatrist because of potentially overly positive representations, the counterpart is very poor postprescription monitoring. Consequently, even if there is no evidence of risk in this population, information to prescribers should be reinforced, particularly in terms of postprescription monitoring.
In terms of recommendations, it seems useful to limit the use of aripiprazole to the FDA-approved indications and make non-FDA prescriptions subject to specialist advice. Indeed, review of the literature highlights the need to propose aripiprazole treatment in children in certain indications where efficacy has been noted and where approval has not been obtained in some countries (e.g., Tourette's syndromeand behavioral disorders associated with autism and intellectual disability). It would also be useful to ask clinicians to reexamine polyprescriptions because it is in these contexts that the most serious adverse effects have been reported. In particular, prescribers should be informed of the need to monitor and track adverse events according to existing recommendations (Pringsheim et al. 2011b). Pharmacoepidemiology and pharmacovigilance studies should also be continued to clarify possible risks at the population level or rare side effects (e.g., suicide induction), bearing in mind that to date, there is no risk in terms of public health. Finally, given the high prevalence of off-label prescription, new evidence-based studies on these specific indications should be provided to ensure whether other indications than the FDA-approved ones are legitimate.
Clinical Significance
Aripiprazole has proven efficacy for several indications in children and adolescents, including schizophrenia, bipolar disorder, Tourette's syndrome, and behavioral impairments associated with autism and intellectual disability. However, its use requires clinical and paraclinical monitoring to assess the occurrence of adverse events that may challenge the benefit/risk ratio. In addition, off-label prescriptions should be limited as they appear to account for a significant proportion of aripiprazole use worldwide.
Footnotes
Disclosures
During the last 3 years, D.C. reported past consultation for or the receipt of honoraria from Otsuka, Shire, Lundbeck, Roche, and Janssen. N.C. and M.-L.M. have no financial relationship with any pharmaceutical company. Authors were independent in selecting the data and analyzing them, and writing the article.
Supplementary Material
Supplementary Data
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.