
Abstract
Objective:
The outcome of pediatric obsessive-compulsive disorder (OCD) is still unclear. In the present study, long-term rates and predictors of remission were used to identify potential factors influencing the outcome of pediatric OCD.
Methods:
Using meta-analysis techniques, we calculated the pooled rate of remission and performed subgroup analyses to identify potential heterogeneities, and the meta-regression analysis was used as a predictor.
Results:
A total of 18 studies including 1389 participants were identified, and the follow-up periods ranged from 1 to 16 years. The pooled remission rate of pediatric OCD was 62% (95% confidence interval: 52–72). Shorter duration of OCD at baseline (R 2 = 78.04%, p < 0.0001) predicted higher rates of remission.
Conclusions:
The outcome of pediatric OCD seems to be better than the past. Shorter duration of illness appears to be related to a better outcome. Early detection of pediatric OCD and early intervention play an important role in good prognosis. In the future, studies based on multicenter, longer follow-up studies with larger samples were needed to confirm these issues for the outcome of pediatric OCD.
Introduction
Obsessive-compulsive disorder (OCD) is a common psychiatric disorder that affects 0.25%–4% of children and adolescents (Douglass et al. 1995; Zohar 1999; Heyman et al. 2003). Although it tends to be chronic and severely disabling, the long-term outcome of pediatric-onset OCD is still unclear (Kalra and Swedo 2009). To our knowledge, only one meta-analysis study has been conducted to assess the outcome of pediatric OCD. It showed that pooled mean persistence rates were 41% for full OCD and 60% for full or subthreshold OCD at follow-up. The study also found that earlier age of OCD onset, longer OCD duration, and inpatient status predicted greater persistence (Stewart et al. 2004).
However, the studies included in the previous meta-analysis were very limited. For example, some were published in 1942 and 1960 when the diagnosis of OCD was not clear (Berman 1942; Warren 1960). Nearly half of the included studies included sample sizes of fewer than 20 patients. Moreover, the criteria of obsessive-compulsive spectrum rather than disorder were used (Berg et al. 1989). Some new studies have since challenged the conclusions of the previous meta-analysis. For instance, a longitudinal cohort study found that only 24% of children with OCD had full OCD in early adulthood (Bloch et al. 2009). It further found that later age of OCD onset was associated with persistence of OCD symptoms, in contrast to the previous meta-analysis (Bloch et al. 2009). In addition, two studies have since observed that age of onset does not contribute to persistence (Micali et al. 2010; Mancebo et al. 2014).
With the widespread use of effective, evidence-based treatments for OCD in recent years, such as selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral therapy (CBT), the outcome of pediatric OCD seems to be much improved. Recently, one research group found that the remission expected was much better than before (Melin et al. 2020), in which the outcome of pediatric OCD underwent changes during the past 15 years.
Given these changes, there is an urgent need to revisit the outcome of pediatric OCD. The aim of the present study was to identify the pooled remission rate and potential predictors of remission for the outcomes of pediatric OCD. We performed a meta-analysis to investigate the outcomes of OCD from a pool of studies, in which subgroup analysis and meta-regression analysis were used to identify the potential heterogeneity and the predictors of pediatric OCD outcomes.
Materials and Methods
Literature search
A systematic search was performed in PubMed, Elsevier, and China National Knowledge Infrastructure. The search terms were “obsessive compulsive disorder,” “prospective,” “outcome study,” “natural history,” “clinical course,” “prognosis,” “follow-up,” “remission,” and “long-term.” The references of the relevant studies were also independently crosschecked by two researchers to avoid omissions as much as possible.
Inclusion and exclusion criteria
To further identify relevant studies for our meta-analysis, the inclusion criteria were as follows: (1) English or Chinese language studies from peer-reviewed journals; (2) age of OCD at childhood (<18 years of age); (3) duration of follow-up at least 1 year; and (4) availability of data on remission. The exclusion criteria were as follows: (1) small sample size (n < 10) and (2) study reporting the same sample with shorter follow-up period. The procedures of study identification are shown in Figure 1.
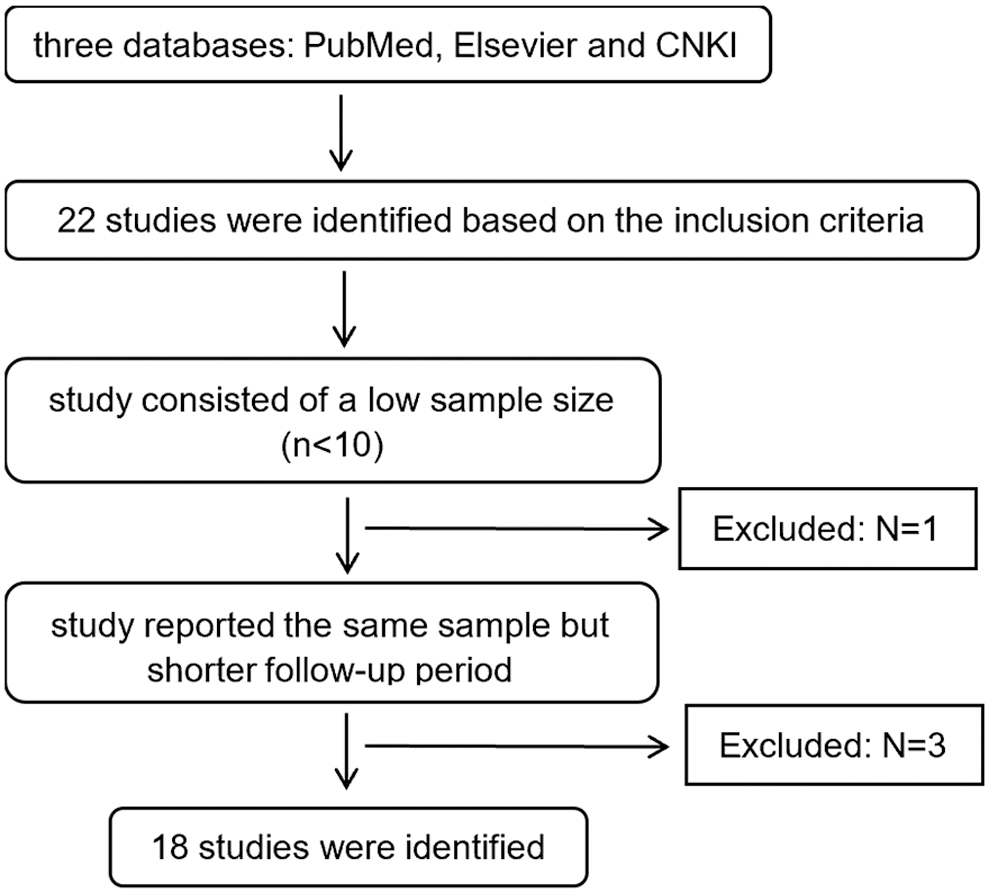
Flowchart for identification of included studies.
Data extraction
The following characteristics of each included study were coded as follows: (1) first author and publication year; (2) sample size; (3) remission rate (%); (4) proportion male (%); (5) age at illness onset; (6) age at first assessment; (7) duration of illness at baseline; (8) length of follow-up; (9) participant source (inpatient, outpatient, or both); and (10) remission criteria. Two raters independently confirmed the reliability of data extracted from the included studies.
The assessment of pediatric OCD outcomes
The rate of remission was defined as the indicator of outcome for pediatric OCD. There are 12 studies in which the remission was defined as the participant not meet the original diagnostic criteria of OCD at longest follow-up by clinical evaluation. In six other studies, the Children's Yale-Brown Obsessive Compulsive Scale or the Yale-Brown Obsessive Compulsive Scale was used and remission was defined as a score of 15 or less.
Statistical analyses
The pooled rate of remission was calculated as a sample size-weighted proportion with standard error. We used a random-effects model of DerSimonian and Laird (1986) with R software, version 3.5.3. I 2, forest plots were used to identify the heterogeneity, and the Q test was used to assess the heterogeneity with calculated p-values.
To examine predictors of remission, we performed subgroup analyses on participant source (inpatient vs. outpatient vs. mix [inpatient/outpatient combined]), remission criteria (clinical evaluation vs. scale evaluation), and year of study (before 2000 vs. after 2000) (Rapoport and Inoff-Germain 2000).
Meta-regression refers to a fixed-effects model or random-effects model that includes one or more study features as covariates, and a random-effects meta-regression model is given by the following:
(a test for the null hypothesis γ = 0 is a test to determine whether the covariate y contributes to the study heterogeneity) (Thompson and Higgins 2002). Thus, we also examined the following predictor variables by meta-regression analysis: age at onset, duration of illness, proportion male, and length of follow-up interval.
Results
Included studies
According to the inclusion criteria, we initially identified 22 English language studies for analyses. From these, one study was excluded because of a small sample size (Apter et al. 1984). Three studies reporting the same sample with a shorter follow-up period were also excluded (Bolton et al. 1983; Holmgren Melin et al. 2015; Hojgaard et al. 2017). In total, 18 studies comprising 1389 participants were included in our meta-analysis. The baseline characteristics are summarized in Table 1. No publication bias was identified (funnel plot is present in Supplementary Fig. S1).
Studies Included in the Meta-Analysis
N, number of samples; NR, not recorded; ICD, International Classification of Diseases; DSM-III, Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; DSM-III-R, Diagnostic and Statistical Mental of Mental Disorders, 3rd ed., Revision; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th ed.
The pooled rate of remission
The pooled rate of remission was 62% (95% confidence interval [CI] 52–72, as determined by a randomized-effects model (Fig. 2). The I 2 statistic was calculated and the Q statistic was used to test for heterogeneity. The I 2 was 92.4% (95% CI 89.5–94.5, p < 0.0001).
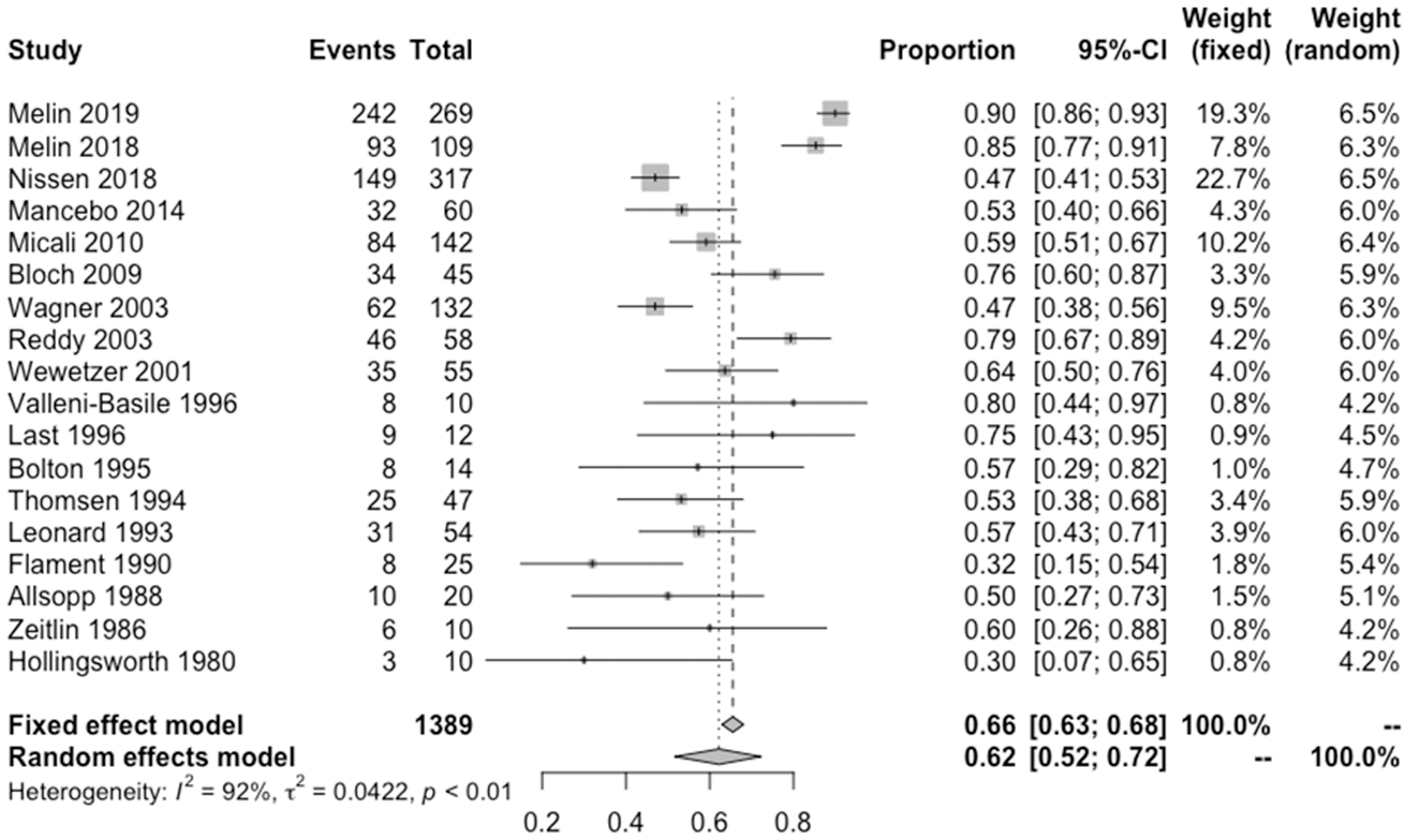
Forest plots of the rate of remission.
Subgroup analysis
One subgroup analysis was performed on the basis of participant source, which included inpatient, outpatient, and a combination of both. Figure 3 shows that the inpatient studies had a pooled rate of 49% (95% CI 31–67, I 2 = 57%), while mix studies had a rate of 59% (95% CI 51–67, I 2 = 58%) and outpatient studies showed a rate of 72% (95% CI 52–89, I 2 = 97%). However, the difference was not statistically significant (p = 0.24).

Subgroup analysis by participant source and by remission criteria.
The second subgroup analysis was examined on remission criteria. Figure 3 shows that studies using clinical criteria had a pooled rate of 56% (95% CI 50–62, I 2 = 25%), while studies that used scale criteria had a rate of 72% (95% CI 52–88, I 2 = 97%). the difference was still not statistically significant (p = 0.13).
In addition, subgroup analysis was also performed by the “Year” (before 2000 vs. after 2000) (Rapoport and Inoff-Germain 2000). There is no significant difference on the Publication Year (the year that the studies were published) and the Inception Year (the year that the cohort was initially followed) (p = 0.10, p = 0.39) (more details are seen in Supplementary Fig. S2).
Meta-regression analysis
We used meta-regression analyses to identify predictors of remission. Age at onset, duration of illness, proportion male, and length of follow-up interval were selected as the potential predictors to build our regression model (Table 2). We found that duration of illness was a significant predictor (p < 0.0001), and accounted for 78.04% of the total heterogeneity in predicting OCD outcome (R2 = 78.04%). Variables that were not significant predictors of remission included age at onset (R2 = 34.49%, p = 0.36), proportion male (R2 = 0.00%, p = 0.76), and length of follow-up interval (R2 = 0.00%, p = 0.67). Figure 4 shows that a shorter duration of OCD at baseline predicted higher rates of remission.
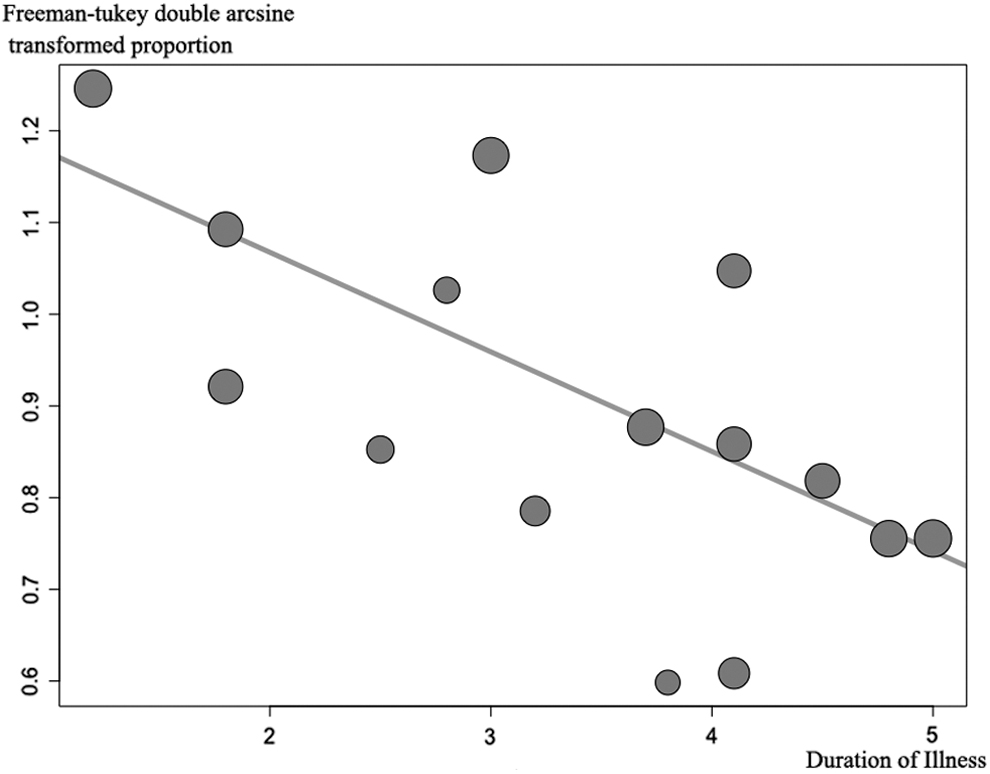
Meta-regression analysis of duration of illness at baseline for rate of remission.
Results of Meta-Regression Analysis
τ 2: the estimated amount of residual heterogeneity; I 2: the residual heterogeneity; H 2: the unaccounted variability; R 2: the amount of heterogeneity accounted for.
p < 0.0001.
OCD, obsessive-compulsive disorder.
Discussion
In this study, we aimed to identify the long-term outcomes of pediatric OCD using meta-analysis techniques. We found that the pooled rate of remission of pediatric OCD was relatively high at 62%, and that a shorter duration of OCD at baseline might predict higher rates of remission.
Although OCD is generally believed to follow a chronic waxing and waning course (Skoog and Skoog 1999; Anthony et al. 2006), our study suggests that the long-term prognosis of pediatric OCD may be better than before. For example, the pooled remission rate in our analyses was better than the previous meta-analysis from 2004, which indicated that the remission rate was 59%. Furthermore, the remission rate may be better in adults with OCD, since research has found that the long-term remission rate in adults was 53% (Sharma et al. 2014). In contrast, however, some research has also found that remission rates are improved in youth compared with adults with OCD (Mancebo et al. 2014).
We also found that duration of illness at baseline was a significant predictor of OCD outcome. This suggests that a shorter duration of OCD at baseline is associated with a higher rate of remission. The results are similar to the meta-analysis from 2004, as well as other related studies (Micali et al. 2010; Mancebo et al. 2014). For example, one group of researchers recruited a cohort of 142 adolescents with OCD and similarly found that the main predictor for persistent OCD was duration of illness at assessment (Micali et al. 2010). Similarly, Mancebo et al. (2014) tracked 60 adolescents with a primary diagnosis of OCD, and they found that treatment early in the course of illness predicted a better outcome. Therefore, the association between duration of OCD at baseline and the rate of remission seems highly likely based on past and present results, suggesting that early detection and intervention play an important role in the long-term course of pediatric OCD.
In our study, according to the subgroup analysis, both year of study publication and inception were not associated with the remission rate of pediatric OCD. Although some randomized-controlled trials have demonstrated the efficacy of CBT and SSRIs for the treatment of OCD in children in the short term (Geller and March 2012; Ost et al. 2016). It seems that more long-term follow-up studies about the outcome of pediatric OCD are needed in future studies.
Participant source, age at onset, sex, and length of follow-up interval were not found to be associated with the remission rate of pediatric OCD. This stands in contrast to previous studies that found that participant source and earlier age of OCD onset were predictive of OCD persistence. One possible reason for this difference may be due to the fact that inpatients have more severe symptoms than outpatients, and that the prognosis was likely worse without effective intervention in the earlier years of the illness. We also found that age at OCD onset accounted for 28.78% of the total remission rate heterogeneity, but it was not significant. This may be attributed to the fact that atypical symptoms are often observed in pediatric OCD, which makes diagnoses more difficult, particularly in younger children with OCD.
Our study has a few limitations. First, there are several predictors reported in previous studies, such as baseline severity (Thomsen 1995), comorbid disorders (Bloch et al. 2009; Jakubovski et al. 2013), insight (Nissen and Parner 2018), and parental accommodation (Francazio et al. 2016), that were not included in the present study due to limited data points. Moreover, the length of follow-up interval for most of the included studies was <5 years, and we may have subsequently failed to capture recurrent episodes. It also limited comparisons between studies that the definition of remission and treatments are variable. Further, the degree of heterogeneity was larger among limited number of studies. Finally, we were unable to assess other potential outcome measures, such as functional impairment and quality of life. Future studies may wish to collect more comprehensive measures of a variety of outcomes and predictors, and be expanded to multicenter sites with a greater length of follow-up interval and with larger samples.
Conclusions
In conclusion, we found the long-term outcome of pediatric OCD was relatively optimistic. More than 60% of the patients could achieve remission in the long run. The outcome of pediatric OCD seems to be better than the past. Shorter duration of illness appears to be related to a better outcome. Early detection of pediatric OCD and early intervention play an important role in good prognosis. In the future, multicenter, longer follow-up interval studies with larger samples are needed to confirm these issues for the outcome of pediatric OCD.
Clinical Significance
The present meta-analysis showed that the outcome of pediatric OCD seemed to be better than the past. Shorter duration of illness appears to be related to a better outcome. Early detection of pediatric OCD and early intervention play an important role in good prognosis.
Footnotes
Disclosures
None of the authors have any conflicts of interest to disclose.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.