
Abstract
Objective:
This study is a retrospective review of patients 5–17 years of age experiencing seclusion and/or restraint (S&R) in a pediatric psychiatric inpatient setting and an exploratory analysis of antipsychotic use on S&R duration. We examined whether administration of antipsychotics would possibly decrease the time spent in S&R.
Methods:
Reports of patients who underwent S&R in an acute care inpatient child and adolescent psychiatric unit from 2012 to 2014 were reviewed. Demographic information related to age, gender, and race as well as information on diagnosis, current medications (including antipsychotics) were obtained. Independent samples t-tests were used to determine whether there were differences in how much time patients spent in S&R based on whether they were administered antipsychotics or not. Odds ratios (ORs) of being administered antipsychotics during S&R were computed for factors such as gender, race, and diagnosis group.
Results:
Ninety-six patients (68 males, age range 5–17 years) were involved in 232 S&R events that occurred between 2012 and 2014. Results indicate that patients who were administered antipsychotics during S&R still spent significantly more time in S&R compared with those who were given medications other than antipsychotics (e.g., Benadryl) (t = 3.161; p = 0.002) and those who were not administered any medication (t = 3.54; p = 0.001). Binary logistic regression showed that female patients were at more than two times (OR(adjusted) = 2.86; 95% confidence interval = 1.234–6.655) higher risk of being administered antipsychotics while in S&R compared with their male counterparts within this particular sample.
Conclusions:
The results of our study indicate that, contrary to our hypothesis, antipsychotic administration did not appear to reduce the time spent in S&R compared with groups that were administered medications other than antipsychotics and those that were not administered any medication during S&R. We also found an increased risk of antipsychotic administration in female patients compared with male patients in S&R events, indicating the need for larger studies examining these effects in greater detail.
Introduction
In the last decade, there has been an increase in psychiatric diagnosis and treatment of children and adolescents, particularly in the United States (Altay et al. 2019; Piovani et al. 2019). Psychopharmacology has been playing an increasingly important role in treatment (Olfson et al. 2014). With this general rise in use of psychiatric medications in pediatric populations, there has been an increase in prescription of antipsychotic medications as well (Lohr et al. 2018). Antipsychotics are approved by the Food and Drug Administration in children for schizophrenia, aggression in autism, and bipolar disorder. However, they are used off label for a wide variety of diagnosis such as conduct disorder, oppositional defiant disorder (ODD), attention-deficit/hyperactivity disorder (ADHD), anxiety, and depression (Crystal et al. 2009).
This increase in prescription of antipsychotics is concerning because of the short- and long-term potential side effects associated with these medications. The two most concerning immediate reactions to antipsychotic are acute dystonia and neuroleptic malignant syndrome (NMS). Even a single dose of antipsychotic medication can cause a dystonic reaction and almost all cases are seen within 5 days of initiation or dose adjustment (Rodnitzky 2005). Dystonic reactions can cause flexion of any muscle group, but most commonly it effects the muscles of the neck and face. Children and adolescent are actually at an increased risk for having a dystonic reaction compared with older adults (Rodnitzky 2005). The prevalence of dystonic reactions is variable depending on dosage used and risk factors for the patient population from 2% to 90% (Van Harten et al. 1999). Anticholinergic medications are, therefore, often given with antipsychotics prophylactically to prevent acute dystonic reactions (Van Harten et al. 1999). NMS is a constellation of syndromes that includes diffuse rigidity, fever, diaphoresis, and hypertension. The current prevalence of NMS in the general population is ∼0.01% to 0.02%, with these lower prevalence rates potentially reflecting the shift toward using lower dose antipsychotic regimens and a greater awareness of this condition. NMS can be potentially fatal and difficult to diagnose in children owing to variability in presentation (Croarkin et al. 2008). This condition may also present differently in children than in the adult population; one example is that children are much less likely to have tremor than adults (Neuhut et al. 2009). However, there are very limited data on NMS in the pediatric population specifically (Pelonero et al. 1998; Stübner et al. 2004; Neuhut et al. 2009).
The most concerning long-term side effects of antipsychotic medications in children are Tardive dyskinesia (TD) and metabolic syndrome. TD is a movement disorder that is characterized by persistent slow writhing and sudden involuntary movements and it can affect any part of the body, but is most commonly seen in the muscles of the face and mouth (Aia et al. 2011). This diagnosis often requires years of antipsychotic exposure before symptoms become apparent, so diagnosis is rare in children. However, there have been some case reports of TD occurring in children and the duration of exposure is a known risk factor for development of TD (Garcia-Amador et al. 2015; Lamberti et al. 2017; Wei et al. 2017).
Antipsychotic use, especially second-generation antipsychotics, are associated with a variety of metabolic side effects. Exposure to second-generation antipsychotics is associated with negative outcomes such as weight gain, hypertension, dyslipidemia, hyperprolactinemia, and type 2 diabetes (Cheng-Shannon et al. 2004; Newcomer 2005; Correll et al. 2009). Some metabolic changes such as weight gain can start to occur over a very short time period (Correll et al. 2009). Certain special populations, such as autism spectrum disorder (ASD), are known to be at a higher risk (Chen et al. 2016; Tu et al. 2019) for these metabolic side effects compared with others.
The general increase in psychotropic medication use and particular antipsychotics has been shown to be affected by demographic factors such as being nonwhite and being in the foster care system (DosReis et al. 2011). This means that antipsychotics are more likely to be used in vulnerable populations and within these vulnerable populations, special populations, such as ASD, are more prone to experience the negative side effects of these medications (Mohr et al. 2003; Paterson et al. 2003; Chen et al. 2016; Tu et al. 2019). In an inpatient setting, antipsychotics may be prescribed during an seclusion and/or restraint (S&R) event wherein the patient presents a significant risk to him/herself, staff or other patients, thereby, making this subpopulation of pediatric patients especially vulnerable.
The goal of this study, therefore, was to perform a retrospective preliminary exploratory analysis examining impact of antipsychotic use on duration of S&R. Despite the retrospective nature of the study, we still think this study will provide valuable information. Our study looks at children on an inpatient unit overall who are more acutely ill and usually represent a high-risk population that can be simultaneously difficult to study through other means such as review of claims data and automated data retrieval. This makes a retrospective chart review study the most detailed way to look at hospitalization. This is also an area with very few published studies and little clinical data.
Methods
This was a preliminary exploratory retrospective study looking at a preexisting dataset that only included information on pediatric patients with S&R events during their inpatient admissions. The information was gathered from a 17-bed acute pediatric inpatient psychiatric unit at the University of Missouri Hospitals (Columbia, MO) that admits both males and females, from ages 5–17 years. The average length of stay on the unit is ∼5–7 days. All S&R events that occurred between 2012 and 2014 were included in the analysis with inclusion criteria being a physician order for S&R on the patient based on significant safety risk to self or others. The study was approved by the University of Missouri Institutional Review Board with a full waiver of consent (IRB number: #1201032). Hospital policies around S&R follow the standards that have been set by Joint Commission on Accreditation of Healthcare Organization. On the pediatric unit we follow the practice guidelines set by the American Academy of Child and Adolescent Psychiatry (Masters et al. 2001) and all employees are trained on these regulatory standards.
The Chronic Behavioral and Affective Dysregulation Syndrome (CBADS) questionnaire was used to evaluate the charts of patients who were admitted between 2012 and 2014 to the child and adolescent acute inpatient unit at the University of Missouri Psychiatric Center and experienced an S&R. The CBADS is a new questionnaire derived from a questionnaire originally developed by Beck et al. (2017) and has not been validated in the studied population. The CBADS was used in this study because a similar questionnaire has been used to look at aggression in the psychiatric population (Beck et al. 2017) and because the questionnaire covered a broad range of demographic and clinical information that we thought was particularly useful clinically for studying the S&R population (Beck et al. 2017).
Along with these variables, the type, reason, and duration of S&R (<60, 60–120, and >120 minutes), and use of medication (antipsychotic or not), if any, during S&R, were also reviewed and recorded. Axis I diagnosis as primary presentation for admission was classified into 6 groups as described hereunder for the purpose of analysis: Group 1: Mood disorders Group 2: Anxiety disorders Group 3: ASD, pervasive developmental disorder not otherwise specified and other neurodevelopmental disorders Group 4: ADHD or ODD Group 5: Posttraumatic stress disorder Group 6: Other diagnosis.
Based on clinical experience, we hypothesized that administration of antipsychotics would have an effect on time spent in S&R, possibly lowering the duration of time spent in S&R. We used independent samples t-tests (SPSS version 26; IBM Corp.) to determine whether there were differences in how much time patients spent in S&R based on whether they were administered antipsychotics or not. An exploratory analysis computing the odds ratio (adjusted) [OR(adj)] of being administered antipsychotics during S&R was computed for factors such as gender, race, and diagnosis group using a binary logistic regression model (SPSS version 26; IBM Corp.). Missing data were excluded by the statistics software on a case-by-case basis.
Results
Ninety-six patients (68 males, age range 5–17 years) were involved in 232 cases of S&R in the years 2012–2014 (Table 1). As we were interested in the effect of antipsychotics on the duration of S &R, data on duration of S &R was examined separately. Five incidents were found to be exceptionally long (outliers) (Fig. 1). Demographic data on the patients involved in these five incidents are given in Table 2.
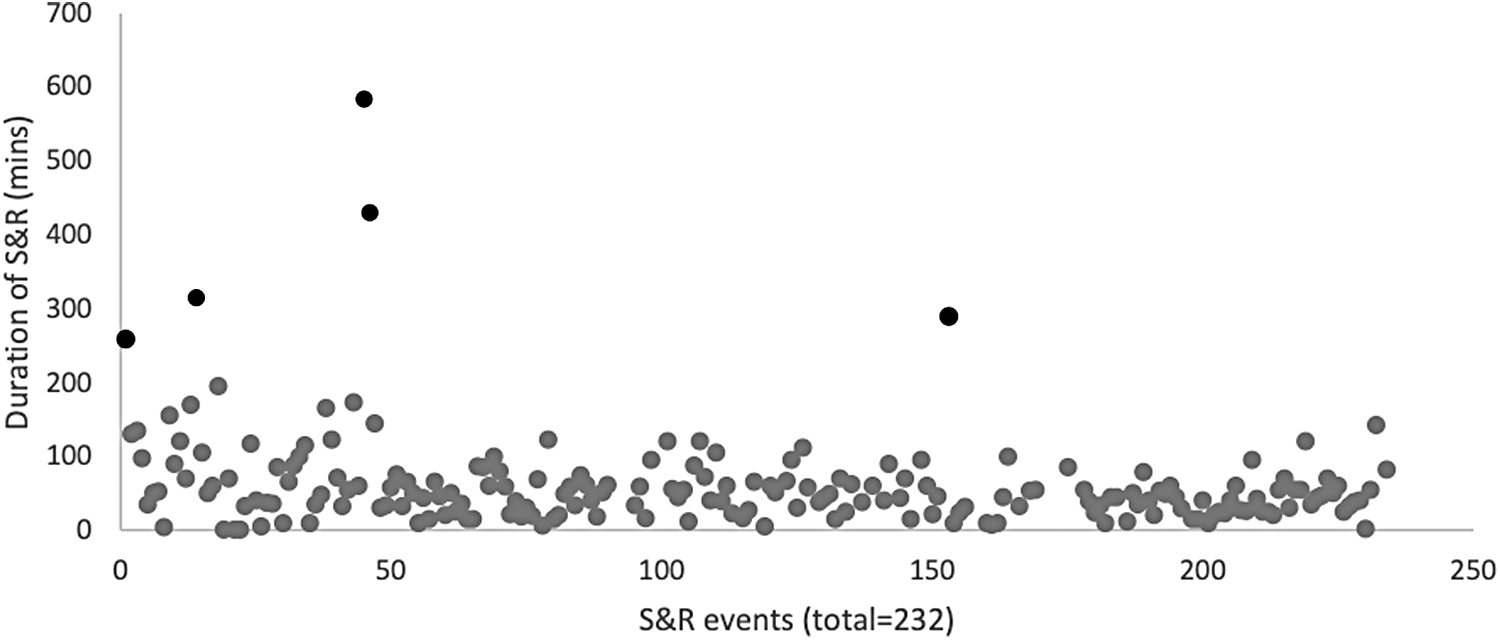
Scatter plot of S&R duration across 201* S&R events (*exact duration info missing for 31 events). Outliers indicated in red. S&R, seclusion and/or restraint.
Demographics of Participants (N = 96)
Demographics for 232 cases of S&R.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; ODD, oppositional defiant disorder; PDD, pervasive developmental disorder; PRN, as needed medications; PTSD, posttraumatic stress disorder; S&R, seclusion and/or restraint; SD, standard deviation.
Demographic Characteristics, Reason for, Type of and Duration of Seclusion and/or Restraint and as Needed Med Administration for Patients with Uncharacteristically Long Seclusion and/or Restraint Durations (>200 Minutes) (Outliers)
ASD, autism spectrum disorder; DC/DX, discharge diagnosis; IM, intramuscular; PDD-NOS, pervasive developmental disorder not otherwise specified; PO, by mouth; PRN, as needed medications; PT, patient; S&R, seclusion and/or restraint.
Results of the independent samples t-test indicate that patients who were administered antipsychotics during S&R still spent significantly more time in S&R compared with those who were given medications other than antipsychotics (e.g., Benadryl) (t = 3.161; p = 0.002) and those who were not administered any medication (t = 3.54; p = 0.001) (Fig. 2). Binary logistic regression showed that female patients were at about three times [OR(adj) = 2.86; 95% confidence interval = 1.234–6.655] higher risk of being administered antipsychotics while in S&R compared with their male counterparts within this particular sample (Table 3).

Time spent in S&R (in minutes) compared across medication administered. **Significant difference with p < 0.05. PRN, as needed medications; S&R, seclusion and/or restraint.
Odds Ratio (Adjusted) for Administration of Antipsychotics During Seclusion and/or Restraint Based on Gender, Race and Diagnosis Group
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; CI, confidence interval; ODD, oppositional defiant disorder; OR, odds ratio; PDD-NOS, pervasive developmental disorder not otherwise specified; PTSD, posttraumatic stress disorder.
Discussion
The objective of this study was to examine antipsychotic prescription practices within the especially vulnerable population of pediatric inpatient psychiatric patients who are placed in S&R. Antipsychotics are sometimes administered during an S&R with the ultimate goal of reducing the time a patient spends in S&R owing to the negative effects associated with S&R. The results of this study reveal that administration of antipsychotics did not seem to reduce the duration of S&R in this sample of inpatient pediatric psychiatric patients. In fact, patients who were administered antipsychotics spent significantly longer in S&R compared with patients who were administered psychotropic or nonpsychotropic medications other than antipsychotics or patients who were not administered any medication at all.
One possible reason for this observation could be that antipsychotic was not the first line of treatment in these patients. They were administered drugs that were not antipsychotics first, which probably were not effective enough and subsequently, administered antipsychotics. The lack of time-based data on the administration course of medications during the S&R event is a limitation of this study. However, our finding seems to be in line with previous research showing that increasing dosage of antipsychotics did not produce a favorable response in terms of reducing S&R occurrence in adolescent psychiatric patients (Miller et al. 2013). The results of this study, suggesting that the usage of antipsychotics within the S&R pediatric patient population may not be as effective as previously presumed, supports the need for future research looking at safer, effective behavioral strategies to reduce occurrence and duration of S&R (Huefner et al. 2014).
The study also found that female patients had more than twice the odds of being administered antipsychotics during S&R compared with male counterparts. This observation was despite the smaller sample size of female patients in this study. Clinical research examining gender-based differences particularly in the use of antipsychotics in S&R are too few. Our finding, although preliminary and in a relatively smaller sample size, might be important in guiding future research to examine potential antipsychotic prescription bias in this especially vulnerable population. However, a larger prospective study would be required to strongly validate these observations to identify how antipsychotics are being used in this population and if there are additional ways to decrease the need in this already high-risk and vulnerable population.
The results of this study must be interpreted with caution taking into consideration the following limitations. First, this is a retrospective chart review with a relatively small sample size consisting entirely of patients who had undergone at least one S&R event during hospitalization. We did not have a control group that did not experience any S&R event during admission to help us further conclusively isolate risk factors unique to the S&R group.
Second, we have not accounted for multiple readmissions of an individual patient that may skew some of our results. Future studies should consider using analysis of variance to reduce the probability of type I errors and include other confounding factors. We did not have data on characteristics of frontline staff (nursing, mental health technicians on the unit) regarding experience working with pediatric psychiatric patients, as they are usually the first responders to the S&R events. In addition, presence of temporary staff from different units at times, the census of the unit, and milieu of the unit may also affect S&R. The use of antipsychotics during an S&R may also be provider dependent.
Although our study does have several limitations that limit its direct clinical application, what it does provide are initial data to inform future prospective studies.
Despite these limitations, the results of the study provide preliminary evidence that antipsychotics might not be as effective in reducing time spent in S&R in pediatric psychiatric inpatients and that pediatric females might be at a higher risk of being administered antipsychotics while in S&R. Given these findings and the knowledge that these medications carry a high potential side effect burden, alternative methods including milieu management, behavioral management, early identification of high-risk patients, and working on specific behavior modification plans may warrant further exploration in a prospective study. Periodic quality checks examining efficacy of using antipsychotics during S&R, in terms of reduction in duration of S&R and reduction in frequency of S&R are required to ensure greater efficacy of interventions used during S&R. Further research is needed on the relationship of prescribing habits in these high-risk populations and what can be done to decrease risk while maintaining safety both in the inpatient and outpatient setting.
Conclusions
The increasing use of antipsychotics in the pediatric psychiatric population is a matter of growing concern, especially owing to the numerous negative short-term and long-term effects of these medications. Within the pediatric psychiatric population, specific groups may be at higher risk of being prescribed antipsychotics because of various factors (dosReis et al. 2011).
In this study, we specifically examined antipsychotic prescription practices and contributing factors in children admitted to an acute pediatric psychiatry inpatient unit who were potentially at higher risk owing to an S&R event during hospitalization. Our study found that, in our pediatric inpatient sample, administering antipsychotics did not reduce the time spent in S&R compared with groups that were administered medications other than antipsychotics and those that were not administered any medication during S&R. We also found an increased risk of antipsychotic administration in female compared with male patients, indicating the need for larger studies examining these effects in greater detail. These preliminary results point toward the need for future, larger studies examining the prescription practices and factors associated with use of antipsychotics in the S&R setting.
Clinical Significance
S&R is the highest risk intervention that occurs on any psychiatric inpatient unit and patients, their families, and staff all benefit from its reduction. Previous research S&R looks at risk factors that do not change during the course of the hospitalization. Sleep change is unique because it is a dynamic risk factor that can help identify patients that may be at a higher acute risk for S&R. Being able to identify acute risk provides a potential target for intervention and prevention. Our study provides early preliminary data that suggest there may be correlation between reduction in sleep time the 24 hours before and S&R events.
Footnotes
Disclosures
No competing financial interests exist.