
Abstract
Objective:
To determine the effect of CYP2D6 metabolizer status on aripiprazole tolerability in pediatric patients with mood disorders.
Methods:
We retrospectively reviewed electronic medical record data for 277 patients ≤18 years of age (at the time of CYP2D6 testing) with a mood disorder, receiving oral aripiprazole, and CYP2D6 genotyped as part of routine care. The maximum aripiprazole dose and concomitant medications were extracted from the medical record. The reason for aripiprazole discontinuation was determined to be from side effects (e.g., weight gain, akathisia, GI upset), nonresponse, or other reasons (e.g., financial). Associations with CYP2D6 were analyzed using multivariate linear regression models and chi-square tests.
Results:
Of the 277 patients (mean age: 14.3 ± 2.4), 57% were normal metabolizers (NMs), 37% were intermediate metabolizers (IMs), 5% were poor metabolizers (PMs), and 1.4% were ultrarapid metabolizers (UMs). A total of 72.2% of the cohort were concomitantly taking a CYP2D6 inhibitor, resulting in phenoconversion. Accounting for phenoconversion resulted in 27% phenoconverted NMs (pNMs), 24% phenoconverted IMs (pIMs), 48% phenoconverted PMs (pPMs), and <1% phenoconverted ultrarapid metabolizers. CYP2D6 pPMs discontinued treatment due to side effects more often than any other CYP2D6 group (67% for pPM, 51% pIM, 57% pNM, chi-square p = 0.024). Body mass index percentile change was associated with the CYP2D6 phenotype (p = 0.038), the time on aripiprazole (p = 0.001), and the number of concomitant CYP2D6 substrates (p = 0.044) in multivariable models.
Conclusions:
Phenoconverted CYP2D6 metabolizer status is associated with aripiprazole discontinuation. In addition, dose adjustments based on CYP2D6 metabolizer status and concomitant medications could improve aripiprazole treatment outcomes.
Introduction
Dopamine/serotonin receptor antagonists (DSRAs, formerly called antipsychotics) fail to produce an adequate response in 30%–50% of pediatric patients with mood disorders (Lee et al. 2018). As many as half of the youth treated with these medications experience metabolic, neurologic, or gastrointestinal adverse events (Lee et al. 2018). Treatment frequently relies on “trial and error” approaches to medication selection and dosing. Thus, selecting treatments that safely and effectively reduce symptoms is a major challenge in treating children and adolescents with mood disorders. Moreover, there is considerable variability in the doses at which patients experience improvement as well as side effects (Robb et al. 2011; Findling et al. 2012).
Aripiprazole, a mixed DSRA, is a partial D2 and 5-HT1A receptor agonist and an antagonist at 5-HT2A receptors. Compared with other mixed DSRAs, aripiprazole has a lower side effect liability; however, risk for discontinuation and intolerable side effects increases when aripiprazole exposure (i.e., plasma concentrations) is high (Belmonte et al. 2018; Jukic et al. 2019). As such, maintaining aripiprazole exposure high enough to achieve optimal treatment outcomes but not too high to cause side effects can be challenging.
Multiple hepatic cytochrome P450 (CYP) enzymes metabolize aripiprazole, including CYP2D6 and, to a lesser extent, CYP3A4 (CDER FDA 2014). CYP2D6, which metabolizes aripiprazole to dehydroaripiprazole, is one of the most polymorphic pharmacogenes; more than 100 alleles and suballeles are described by the PharmVar database (Nofziger et al. 2020). Variations in the CYP2D6 gene locus may enhance or diminish the enzymatic activity of CYP2D6, including single-nucleotide polymorphisms and nucleotide insertions, duplication, or deletion of the entire gene (Hicks et al. 2014). For example, CYP2D6*3, CYP2D6*4, CYP2D6*5, and CYP2D6*6 variant alleles have no function, whereas CYP2D6*9, CYP2D6*10, and CYP2D6*41 cause reduced CYP2D6 enzymatic capacity (Jukic et al. 2019). Based on the CYP2D6 genotype, patients can be classified as one of the following: poor metabolizers (PMs) who are homozygous for two no function alleles; intermediate metabolizers (IMs) who are either heterozygous for one decreased function and one no function allele or homozygous for two decreased function alleles; normal metabolizers (NMs) who are homozygous for two functional alleles; and ultrarapid metabolizers (UMs) who carry more than two functional alleles (Caudle et al. 2020). Treatment recommendations are based on the metabolizer status that is inferred from the calculated activity score (Gaedigk et al. 2018) as per the Clinical Pharmacogenetics Implementation Consortium (CPIC) (Relling and Klein 2011) and the medication labeling.
Currently, more than 350 drug/gene pairs have been identified, with 93 drug/gene pairs associated with dosage and administration recommendations based on pharmacogenetics in the FDA drug label (Federal Drug Administration 2019). Aripiprazole is among a small number of psychiatric medications for which dosage and administration recommendations based on a pharmacogenetic phenotype are included in the drug label. Clinicians are advised to decrease the aripiprazole dose for CYP2D6 PMs and/or concomitant use of CYP2D6 inhibitors (CDER FDA 2014).
However, the metabolic phenotype for CYP2D6 is also complicated by inhibitors and substrates that are commonly prescribed to pediatric patients with mood and anxiety disorders (e.g., several selective serotonin reuptake inhibitors). This concomitant administration of aripiprazole with these medications results in phenoconversion. As an example, when a patient receives an adjunctive strong/moderate CYP2D6 inhibitor, CYP2D6 activity and the phenotypic classification are reduced. Although the drug label recommends aripiprazole dose reductions with concomitant use of a strong CYP2D6 inhibitor (e.g., fluoxetine, paroxetine), it further states “…no dosage adjustment is necessary for substrates of CYP2D6 (e.g., fluoxetine, paroxetine).” Unfortunately, this inconsistency creates a barrier for both pharmacists and clinicians attempting to make effective dose adjustments. In addition, the label for fluoxetine indicates that fluoxetine may make a CYP2D6 NM resemble a PM, and that coadministration of fluoxetine with atypical antipsychotics should be approached with caution (CDER FDA 2020).
CYP2D6 metabolizer status strongly influences the metabolism of aripiprazole, leading to changes in pharmacokinetic parameters, including exposure as defined by the area under the concentration/time curve, half-life, clearance, and steady-state concentration (CDER FDA 2014; Eum et al. 2016). Accordingly, CYP2D6 PMs—even if they become PMs as a result of phenoconversion—are prone to adverse reactions (CDER FDA 2014) and require lower doses, whereas UMs may need higher doses to achieve a therapeutic response (Arranz et al. 2019).
With these considerations in mind, we retrospectively analyzed the electronic medical record (EMR) data of pediatric patients diagnosed with a mood disorder to determine the effect of CYP2D6 metabolizer status on aripiprazole tolerability. Based on pharmacogenetic studies in adults, we hypothesized that CYP2D6 PMs (through phenoconversion or genetics) would discontinue treatment due to side effects more often than any other metabolizer group and UMs would discontinue treatment due to a lack of efficacy.
Methods
Study design and participants
Data (notes, medication history, problem list, demographic data) were extracted from eligible patients' EMR at Cincinnati Children's Hospital Medical Center (CCHMC), who underwent CYP2D6 genotype testing during admission into the inpatient psychiatry service and returned for follow-up in the outpatient clinic between September 2009 and March 2017. Inclusion criteria comprised the following: CYP2D6 testing at ≤18 years old, prescription of aripiprazole, presence of a mood disorder (bipolar mania, major depressive disorder, or disruptive mood dysregulation disorder), and CYP2D6 genotyping. Patients were excluded if they failed to follow up with outpatient psychiatry services at CCHMC, had a thyroid stimulating hormone level of >5.5 mIU/L as reviewed by a board-certified physician (J.R.S.), or a diagnosis of traumatic brain injury, substance use disorder, intellectual disability, or congenital brain abnormality.
The maximum aripiprazole dose was defined as the highest dose (mg/day) prescribed during the treatment period. This study was approved by the Cincinnati Children's Hospital Medical Center Institutional Review Board, which granted a waiver of consent as it was limited to previously obtained laboratory and clinical data.
CYP2D6 genotyping
Pharmacogenetic testing is included in the standing order set for each patient during an inpatient psychiatric admission (Ramsey et al. 2019). Genomic DNA was isolated from blood or buccal swab samples using the MagNA Pure Compact System (Roche Applied Science, Indianapolis, IN). The TaqMan® Low Density Array assessed 20 CYP2D6 alleles: *2A, *3, *4, *5, *6, *7, *8, *9, *10, *11, *14, *15, *17, *18,*19, *20, *40, *41, *42, and *44. A long-range polymerase chain reaction was used for the duplication, but does not detect quantitative copy number or hybrid alleles (Løvlie et al. 1996). Genotyping was performed in the College of American Pathologists (CAP) and Clinical Laboratory Improvement Amendments-certified Molecular Genetics Laboratory at CCHMC (Cincinnati, OH). A report containing patient genotypes and metabolizer status was uploaded into the EMR that included dosing recommendations for aripiprazole based on CYP2D6 metabolizer status.
CYP2D6 activity score calculation and phenoconversion
Concomitant use of strong and moderate CYP2D6 inhibitors was extracted from the EMR. A patient's activity score was calculated by adding the activity score of each allele (Caudle et al. 2020). Each CYP2D6 allele is assigned a numerical value that represents its predicted function (i.e., 0 = no function, 0.25 or 0.5 = decreased function, 1 = normal function) (Caudle et al. 2017). The sum of the values for each allele observed in the diplotype (star allele combination, e.g., CYP2D6 *1/2) is used to assign one of the following phenotypes: patients with an activity score of 0 are PMs; 0.25–1 are IMs; 1.25–2.25 are NMs; and patients with an activity score >2.25 are UMs (Caudle et al. 2020). Phenoconverted metabolizer status was calculated for each patient by multiplying the activity score by 0 for a strong inhibitor (e.g., fluoxetine or bupropion) and 0.5 for a moderate inhibitor (e.g., duloxetine, fluvoxamine, or sertraline) (Smith et al. 2019). CYP2D6 substrates included atomoxetine, citalopram, clonidine, duloxetine, escitalopram, fluoxetine, fluvoxamine, mixed amphetamine salts, paroxetine, propranolol, venlafaxine, and risperidone (Flockhart 2020).
Outcomes
The reason for discontinuation was determined from the clinical notes and categorized as due to side effects (e.g., weight gain, akathisia), inefficacy, or other reason (e.g., insurance coverage or cost). Seventy-seven patients (27.8%) discontinued due to unknown reasons and were excluded from the discontinuation analyses. Change in body mass index (BMI) percentile was calculated from the BMI percentile nearest to the start and end of aripiprazole treatment. Patients with eating disorders in the problem list were excluded from the change in BMI percentile.
Statistical analysis
Patients were divided into four CYP2D6 genotype-defined groups: PMs, IMs, NMs, and UMs. Linear regression models were implemented using R version 3.2.2, including both genetic and clinical factors to determine contributions to the variability in outcomes. Akaike Information Criterion (AIC) minimization was used for model selection. Chi-square (χ 2) tests using Prism 7 for Windows (GraphPad, La Jolla, CA) were performed to analyze the proportion of patients discontinuing aripiprazole treatment among CYP2D6 metabolizer groups. UMs were excluded from these analyses due to the small sample size. All values are reported as the mean, and p-values <0.05 were considered statistically significant.
Results
There were 277 patients included in the study (Table 1); 57% were NMs, 37% were IMs, 5% were PMs, and 1.4% were UMs. Of the 277 patients, 72.2% (n = 200) of patients were concomitantly taking a CYP2D6 inhibitor (Table 2), which resulted in 27% phenoconverted NMs (pNMs), 24% phenoconverted IMs (pIMs), 48% phenoconverted PMs (pPMs), and <1% phenoconverted UMs (pUMs). The mean maximum aripiprazole dose (mg/day) was similar across the CYP2D6 groups before and after accounting for phenoconversion (Fig. 1). Phenoconversion occurred largely through concomitant administration of fluoxetine, bupropion, and sertraline (Table 2).

Median maximum aripiprazole dose was observed to be equivalent in all CYP2D6 groups (
Cohort Demographics
DMDD, disruptive mood dysregulation disorder; IM, intermediate metabolizer; MDD, major depressive disorder; NM, normal metabolizer; NOS, not otherwise specified; PM, poor metabolizer; pIM, phenoconverted intermediate metabolizer; pPM, phenoconverted poor metabolizer; pNM, phenoconverted normal metabolizer; pUM, phenoconverted ultrarapid metabolizer; SD, standard deviation; UM, ultrarapid metabolizer.
Patients Prescribed CYP2D6 Inhibitors
Strong inhibitor.
Moderate inhibitor.
PM, poor metabolizer; NM, normal metabolizer; UM, ultrarapid metabolizer.
CYP2D6 pPMs discontinued treatment due to side effects more often than other phenoconverted CYP2D6 groups (67% for pPM, 51% for pIM, 57% for pNM, chi-square p = 0.024; Fig. 2). CYP2D6 did not influence discontinuation due to inefficacy (chi-square p = 0.26; Fig. 2).
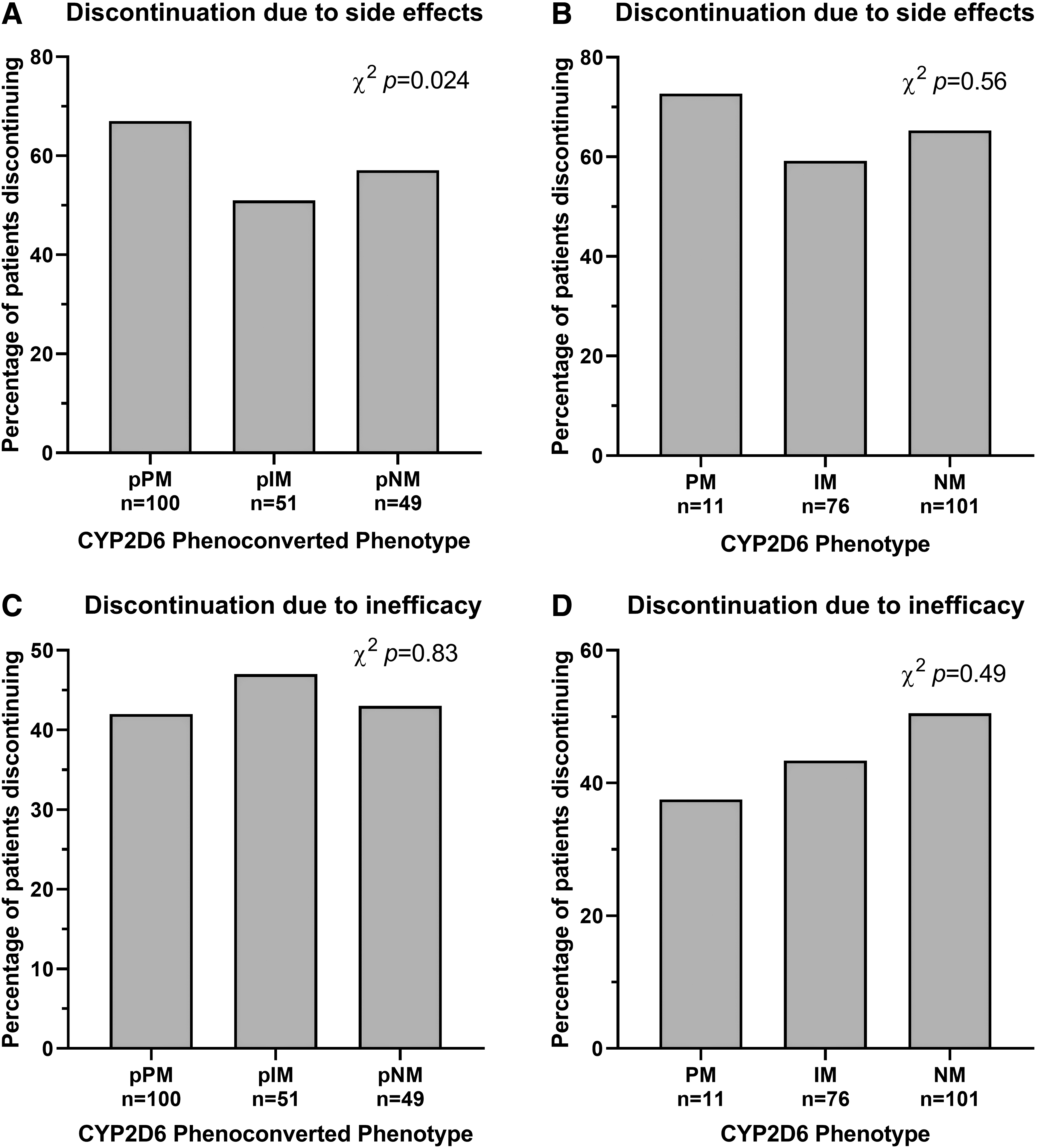
Discontinuation due to side effects was related to the CYP2D6 phenoconverted phenotype (
Weight gain is commonly experienced by patients who are on aripiprazole, however, since this cohort includes children and adolescents who are also growing, we analyzed BMI percentile change and variables likely to influence exposure to aripiprazole: CYP2D6 phenotype, number of CYP2D6 inhibitors, number of other neuropsychiatric medications, maximum aripiprazole dose (mg/day), and time on aripiprazole (days). The model fitting BMI percentile change best (lowest AIC) included the time on aripiprazole (p = 0.001), CYP2D6 phenotype (p = 0.038), and the number of concomitant CYP2D6 substrates (p = 0.044; Fig. 3). The greater the number of concomitant CYP2D6 substrates, the greater the BMI percentile increase. BMI percentile change was not associated with the phenoconverted CYP2D6 phenotype (likely due to confounding with the number of CYP2D6 substrates).

BMI percentile change is associated with the CYP2D6 phenotype (p = 0.034,
Discussion
In this retrospective analysis, we were able to quantify the effect of CYP2D6 metabolizer status on aripiprazole discontinuation and change in BMI percentile in pediatric patients diagnosed with a mood disorder. Our data supported our hypothesis that patients who were CYP2D6 pPMs discontinued treatment due to side effects more often than pNMs. Change in BMI percentile was highest in patients who are CYP2D6 PMs prescribed aripiprazole and patients prescribed multiple additional CYP2D6 inhibitors/substrates.
Our findings extend the findings of a Norwegian sample of adults who received aripiprazole (Jukic et al. 2019). This large study (N = 1334) treated with aripiprazole found that CYP2D6-poor and IMs had 40% higher plasma aripiprazole concentrations compared with NMs and that clinicians prescribed lower doses to PMs. However, there was no significant difference in switching to another antipsychotic medication among CYP2D6 metabolizer groups. Patients taking CYP2D6 inhibitors concomitantly with aripiprazole were excluded from the study. The package label indicates that CYP2D6 PMs have twice the exposure of NMs when receiving the same dose (CDER FDA 2014). Although we lack plasma concentrations in our patients, it is likely that the pPMs were more likely to discontinue treatment due to adverse effects caused by a high plasma concentration of aripiprazole. To further understand the association between aripiprazole exposure and adverse events, routine monitoring of plasma concentrations could be implemented.
Our finding that change in BMI percentile was associated with CYP2D6 phenotype and the number of concomitant CYP2D6 inhibitors is of clinical interest. Many (25%) of the patients were prescribed metformin. Adolescents are more prone to aripiprazole-related weight gain compared with adults (CDER FDA 2014). There is potential to reduce weight gain by reducing exposure to aripiprazole with dose reduction based on pharmacogenetics and concomitant CYP2D6 inhibitors, as suggested by the product insert. Pharmacogenetic clinical decision support generally does not consider phenoconversion and relies on the prescriber to consider drug–drug interactions. Approximately half of the patients who appeared genetically as CYP2D6 NM were phenoconverted to PM. These patients had similar rates of discontinuation due to side effects and BMI percentile change to the PMs as defined by genotype. This rate of phenoconversion is much higher than in an adult study of patients with depression taking venlafaxine (Preskorn et al. 2013).
Based on our study, clinicians were not following the dosing recommendations for CYP2D6 PMs found in the package insert (Table 3) nor were doses adjusted for concomitant CYP2D6 inhibitors. Clinical decision support for aripiprazole should remind the prescriber that phenoconversion is likely when concomitantly prescribing strong inhibitors of CYP2D6. Although some clinical decision support exists in our system for this gene/drug pair, it likely needs improvement in the specificity of recommendations (e.g., “This patient is a CYP2D6 PM and should be prescribed 50% of the normal aripiprazole dose” or “This patient is a CYP2D6 NM. If a strong CYP2D6 inhibitor is prescribed concomitantly, this patient would be phenoconverted to a PM and should be prescribed 50% of the normal aripiprazole dose”). Given that phenoconversion is common and pharmacogenetic testing is becoming more common in the pediatric population being treated for mood disorders, both should be accounted for and highlighted in pharmacogenetic test reports and clinical decision support.
Clinical Recommendations as per Federal Drug Administration Label
PM, poor metabolizer.
It is important to discuss limitations associated with this study that may have played a role in the overall statistical and clinical significance. First, although our study consisted of a large sample size, the number of patients who were CYP2D6 UMs was small (n = 4); therefore, more studies should be performed to provide interpretation for UMs. Second, documentation of side effects and discontinuation reasons in patient charts was inconsistent, which could potentially lead to misinterpretation of treatment outcomes. Third, follow-up, including weight measurements, was at irregular time intervals. Fourth, patients who received care at other health care facilities were not included in our study and our results may not be representative of this population. Fifth, aripiprazole doses were titrated as needed, rather than performing structured titration regimens as in clinical trials. Finally, our study did not focus on concomitant use of CYP3A4 substrates when analyzing the aripiprazole dose.
Conclusion
Antipsychotic pharmacotherapy is often challenging due to multiple factors among patients that alter the pharmacodynamic and pharmacokinetic effects of a drug. A patient's age, sex, ethnicity, disease severity, diet, tobacco/alcohol use, and concurrent medications can influence variability in both therapeutic and adverse event outcomes (Wehry et al. 2015). In addition, it is important to analyze one's genetic variability to successfully optimize aripiprazole dosing regimens. Although aripiprazole contains actionable pharmacogenetic language in its package insert, the clinical recommendations are inconsistent and difficult to clinically interpret. As a result, dose adjustments are not made and patients who are CYP2D6 PMs experience intolerable side effects and discontinue treatment. Treatment outcomes can be improved with precision dosing methods via implementation of pharmacogenetic testing in psychiatry.
Clinical Significance
Individuals who are CYP2D6 PMs or those taking CYP2D6 inhibitors are recommended to receive lower doses as per the package insert, but in our study, these recommendations were not being followed. A potential reason for this could have been the conflicting language about CYP2D6 inhibitors and substrates in the product insert. Our results suggest that adjusting doses based on the pre-emptive CYP2D6 genotype may improve aripiprazole tolerability in pediatric patients with mood disorders. The determination of metabolizer status will allow clinicians to choose a safe and effective dosing regimen that will potentially decrease the risk of side effects and discontinuation of aripiprazole.
Footnotes
Disclosures
Dr. Strawn has received research support from the National Institutes of Health (NIMH/NIEHS/NICHD), as well as Allergan, Otsuka, and Neuronetics. He has received material support from and provided consultation to Myriad Genetics and receives royalties from the publication of two texts (Springer). Dr. Strawn serves as an author for UpToDate, an Associate Editor for Current Psychiatry, and has received honoraria from CMEology and Neuroscience Educational Institute. Dr. Martin has received research support from the NIH. Dr. Ramsey has received research support from the National Institutes of Health (NICHD) and BTG, International Ltd. Dr. DelBello has received research support from Acadia, Allergen, Janssen, Johnson and Johnson, Lundbeck, Otsuka, Pfizer, Sunovion, and Supernus. Dr. DelBello has provided consultation, served on the advisory board, or received honoraria from Alkermes, Allergan, Assurex, CMEology, Janssen, Johnson and Johnson, Lundbeck, Neuronetics, Otsuka, Pfizer, Sunovion, and Supernus. The remaining authors report no financial conflicts of interest.