
Abstract
Objective:
Only few psychotropic drugs are approved to treat tic disorders. The aim was to describe use of tic-suppressing medication and other psychotropic drugs in children with tics.
Methods:
Using nationwide registries, we identified children receiving a tic diagnosis in Denmark during 2006–2017 and extracted data on tic-suppressing medication and other psychotropic drugs.
Results:
Antipsychotics were used by 12%. Use of tic-suppressing medication increased with age and varied according to sex. Over time less children with tics were medicated (from 44% to 38% in the total use of psychotropic drugs) mainly due to decreased use of antipsychotics (from 18% to 6.4%). In recent years, use of aripiprazole exceeded that of risperidone (38% vs. 35%), although risperidone was most often first choice (34%) followed by aripiprazole (22%). Most children stayed on their initial treatment. Attention-deficit/hyperactivity disorder medication (27%) was the most common additional psychotropic drug class used. Regional variations were found in the treatment of tics. Hospital specialists were mainly responsible for treatment.
Conclusions:
Most children with tics do not use tic-suppressing or other psychotropic drugs. The use of aripiprazole superseded risperidone, however risperidone remains the most common first-choice treatment. Treatment was mainly handled by specialists, which is reassuring given the lack of national guidelines, however, regional variations merit further attention as do the variation in treatment between young girls and boys.
Introduction
The pharmacological treatment of children and adolescents with tic disorders (TD), predominantly Tourette's syndrome (TS) and chronic tic disorders (CTD), is complex and focuses on reducing tics and treating comorbid disorders (Plessen 2013); most commonly attention-deficit/hyperactivity disorder (ADHD) and obsessive–compulsive disorder (OCD) (Robertson 2012). Only very limited evidence based on randomized controlled trials (RCTs) is available to guide the choice of treatment of tics (Roessner et al. 2011, 2013; Mogwitz et al. 2018), and the risk of adverse effects often outweighs the evidence of efficacy (Pringsheim et al. 2012). The treatment of tics thus mostly relies on clinical experience and the preferences of the individual prescriber (Roessner et al. 2011, 2013; Mogwitz et al. 2018). Due to their antidopaminergic properties, antipsychotics, especially the typical first-generation antipsychotics (FGA), haloperidol and pimozide, and the newer second-generation antipsychotics (SGA) risperidone and aripiprazole, is one of the few drug classes where evidence indicates a beneficial effect in tic suppression (Roessner et al. 2011, 2013). However, alpha agonists and benzamides (e.g., sulpiride and tiapride) have also been shown to have tic-suppressing effects (Roessner et al. 2011; Hollis et al. 2016; Mogwitz et al. 2018). In most European countries, including Denmark, however, only haloperidol is formally approved to treat tics (Roessner et al. 2011), while use of the other drugs to treat tics are used off-label.
Despite the off-label status of most drugs used in tic disorders, a wide range of different tic-suppressing medications are used (Roessner et al. 2011; Bachmann et al. 2015; Carulla-Roig et al. 2018; Mogwitz et al. 2018). Studies conducted before the introduction of a European clinical guideline on the treatment of tics (Roessner et al. 2011) showed variations in European prescribing practices for the treatment of tics (Rickards et al. 2012) and in the frequency of use between countries (Freeman et al. 2000). Recent studies show that the use of drugs to treat comorbid disorders in tic populations, for example, ADHD medication and antidepressants, also varies greatly between countries (Bachmann et al. 2015; Carulla-Roig et al. 2018).
In this study, we aimed to describe the use of pharmacological treatment in children and adolescents with a newly diagnosed TD in Denmark. Specifically, we described (1) children and adolescents with tics according to psychiatric comorbidities, (2) the use of tic-suppressing medication and other psychotropic drugs, changes over time, and according to type of TD, (3) use of tic-suppressing medications according to age and sex, (4) variations in the choice of first-line treatment for tics, (5) regional variations in use of tic-suppressing medication, and (6) the profile of prescribers who initiate and maintain treatment with tic-suppressing medication as well as other psychotropic drugs.
Methods
Using the nationwide Danish health registries, we identified children and adolescents 6–17 years of age with TD in Denmark. We constructed three cohorts comprising patients receiving a tic diagnosis 2006–2009, 2010–2013, and 2014–2017. For these cohorts, we extracted data on prescriptions filled during the 1st years after receiving the TD diagnosis.
Data sources
Information from the Danish National Patient Registry (Schmidt et al. 2015) [including data from the Danish Psychiatric Central Register (Mors et al. 2011)] was used to identify children and adolescents with a TD diagnosis and psychiatric comorbidities. By using the unique civil person registration number, we linked data from the Patient Registry with data from the Danish National Prescription Registry (Pottegård et al. 2016) to obtain information on dispensed prescriptions. Information on prescribers were obtained through the Danish registry of health care providers within the primary sector (Sundhedsdatastyrelsen n.d.). Information on death and migrations was obtained by using the Danish Civil Registration system (Pedersen 2011). For a detailed description of the registries used (Supplementary Data S1).
Study population
We constructed three different cohorts of children and adolescents 6–17 years old with an administrative TD diagnosis, defined as having a record of one of the following International Classification of Diseases-10 codes: F95.0 (transient tic disorder [TTD]), F95.1 [chronic motor or vocal tic disorder (CTD)], F95.2 (combined vocal and multiple motor TD/TS), and F95.8 (other TD). Children and adolescents who only had an unspecified tic diagnosis (F95.9) was not included based on clinical knowledge about diagnostic practice in Denmark, as this code is mainly used as a preliminary diagnosis before thorough assessment. The three cohorts consisted of children having an incident record of a TD diagnosis in 2006–2009, 2010–2013, and 2014–2017, respectively. A child could only be included in one cohort according to the first TD diagnosis received. Children were excluded if they migrated or died within the 1st year after inclusion. In the supplementary stratified analyses, the cohorts were grouped by sex and by three age categories: 6–9, 10–14, and 15–17 years.
Drugs of interest
In this study, we distinguished between tic-suppressing medication and psychotropic drugs presumably used to treat comorbid disorders. Tic-suppressing medication included antipsychotics (FGA and SGA), clonidine and tetrabenazine. While haloperidol is the only drug formally approved to treat tics in Denmark, however, clonidine is recommended in case of mild tics and either risperidone, aripiprazole, pimozide, or tetrabenazine in case of more severe tics (Dansk selskab for neuropaediatri 2015). Other psychotropic drugs presumably used to treat comorbid disorders included ADHD medication, antiepileptics, anxiolytics, antidepressants, hypnotics, and sedatives. Many of these drug classes are known from previous research to be commonly used in children with tics (Freeman et al. 2000; Debes et al. 2009; Olfson et al. 2011; Bachmann et al. 2015; Farag et al. 2015; Carulla-Roig et al. 2018) either to treat comorbid disorders or symptoms of tics.
Melatonin, included as a hypnotic, was not systematically captured in the Danish National Prescription Registry before 2012, and therefore use of melatonin could only be considered complete in the 2014–2017 cohort. Furthermore, lisdexamphetamine and guanfacine, included as ADHD medication, were only available in Denmark from April 2014 to September 2015, respectively.
For a detailed list of drugs included (Supplementary Table S1).
Analysis
Characteristics of the study cohorts
We described the three study cohorts according to age, sex, type of TD, and psychiatric comorbidities recorded in our data within 2 years before and up to 1 year after the date of TD diagnosis. The comorbidities were ADHD, OCD, autism spectrum disorders (ASD), mental retardation, anxiety disorders, and other psychiatric disorders. A detailed description of how we defined these comorbidities is provided in Supplementary Table S2. Baseline characteristics were presented overall, for each cohort and stratified by type of TD and sex. In a supplementary analysis, we described baseline characteristics in children with tics who did not have records of psychiatric comorbidities (“pure TD”).
One-year prevalence proportion for the use of tic-suppressing medication and other psychotropic drugs
To investigate the use and changes in the prevalence of use of tic-suppressing medication and other psychotropic drugs over time, we calculated the 1-year prevalence proportion for the use of drugs in the three cohorts. The numerator was the number of children in the cohort filling at least one prescription during the 1st year after receiving the tic diagnosis, and the denominator was the total number of children in the cohort. The 1-year prevalence was calculated in all three cohorts and stratified by type of TD. In supplementary analyses, we calculated the 2- and 5-year prevalence proportion, respectively. In these analyses, children who did not have at least 2 or 5 years follow-up time were excluded. Furthermore, as the studied drugs may be used on a trial-and-error basis, we performed a sensitivity analysis, where we required the filling of two prescriptions within 1 year to define use.
To consider the effect psychiatric comorbidities might have on the use of tic-suppressing medication and other psychotropic drugs, we repeated the analysis above only in children with tics who did not have records of psychiatric comorbidities (“pure TD”). Also, we calculated the 1-year prevalence proportions stratified by psychiatric comorbidity.
Time from tic diagnosis until treatment initiation
For children included in the 2014–2017 cohort who at some point, based on all our available prescription data (both before and after tic diagnosis), was dispensed antipsychotics, we calculated the days from filling the first prescription and until the date of diagnosis and depicted this graphically.
Use of tic-suppressing medication according to age and sex
To describe differences in use by age and sex, we described use of tic-suppressing medication by age and sex for children included in the 2014–2017 cohort.
The five most common tic-suppressing medications
To identify changes in the use of the five most common tic-suppressing medications over time, we identified the top 5 most commonly prescribed single-drug substances based on the 1-year prevalence proportion in each of the three cohorts. For each drug we then calculated the proportion of children dispensed the given drug based on the total number of children using tic-suppressing medication.
Regional differences
To describe regional differences in the treatment of tics, we repeated the analysis above for children in the 2014–2017 cohort by stratifying by region of residence by the 1st of January of the year of tic diagnosis, that is, 2014, 2015, 2016, or 2017.
The choice of tic-suppressing medication
We described the variation in the choice of tic-suppressing medication and the flow between different treatments for children included in the 2014–2017 cohort who filled at least one prescription for a tic-suppressing medication. We did this by identifying the first 5 dispensed prescriptions in each child within a 2-year period after inclusion, that is, the date of receiving the first diagnosis of tics. We categorized the prescriptions according to the top 5 drugs identified in the analysis above and included a category with other tic-suppressing medications that did not appear on the top 5 list. We depicted the flow of children in a river plot and censored children if they failed to fill a new prescription within the 2-year period. We performed two analyses; one where we included children who upon the tic diagnosis were naive to tic-suppressing medications based on a 2-year run-in period and another analysis where we included all children regardless of whether they were treated before receiving the tic diagnosis.
Prescriber profile
To describe the prescribers issuing prescriptions for tic-suppressing medication and other psychotropic drugs in children included in the 2014–2017 cohort, we calculated the distribution of tic-suppressing medication (excluding clonidine, tetrabenazine and haloperidol due to too few prescriptions) and other psychotropic drugs issued by general practitioners (GPs), hospital specialists, relevant private practicing specialists, and other private practicing specialists. Relevant private practicing specialist included specialists in child and adolescent psychiatry, neurologists, or pediatricians. We considered the prescriber profile of incident and prevalent prescriptions separately. Incident prescriptions were defined as first prescribed prescriptions (within the last 2 years from the date of tic diagnosis), whereas prevalent prescriptions excluded these.
Statistical analysis
Descriptive statistics, including medians with interquartile ranges (IQR) and frequencies were reported. We reported changes in 1-year prevalence proportions with positive values indicating increases and negative values indicating decreases. We used chi-square to test for difference between prevalence proportions in the 2010–2013 and 2014–2017 cohort.
All calculations were performed using STATA Release 15.1 (StataCorp, College Station, TX). Graphics were performed using STATA Release 15.1 (StataCorp), R version 3.5.2 (R Core Team, 2018) and the riverplot package version 0.6.
Ethics approval
In terms of data protection, the study was registered at the University of Southern Denmark's inventory (record no. 10.080). According to Danish law, purely registry-based studies does not need approval from an Ethics Committee (Thygesen et al. 2011).
Results
We identified a total of 5958 children and adolescents who received an incident TD diagnosis between 2006 and 2017. The majority was male (78%) and the median age at TD diagnosis was 10 years (IQR: 8–12). The most common comorbidities were ADHD (34%) and ASD (17%), but the prevalence of other psychiatric disorders was also high (33%) (Table 1). The frequency of comorbidities varied between boys (M) and girls (F): ADHD (M/F: 37%/23%), OCD (M/F: 5.1%/11%), anxiety (M/F: 4.3%/7.4%), and ASD (M/F: 19%/12%) (Supplementary Table S3). Except for moderate differences in the frequency of ASD and other comorbidities, there was no substantial differences in comorbidity between TD types (Supplementary Table S4). Children and adolescents with “pure TD” were slightly younger at TD diagnosis (mean 9 years) (data not shown in full).
Characteristics of Children and Adolescents with Tics Overall and by Cohort
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; CTD, chronic tic disorder; IQR, interquartile ranges; OCD, obsessive–compulsive disorder; TD, tic disorders; TS, Tourette's syndrome; TTD, transient tic disorder.
Antipsychotics were used by 12% of children and adolescents with tics while there was no or only limited use of clonidine (2.6%) and tetrabenazine (<5 users) (Table 2). ADHD medication (27%) and melatonin (9.4%) was the other two psychotropic drug classes most commonly used 1 year after diagnosis. The most marked difference in use between different TD types was noted for antipsychotics, as children with TS (14.5%) had a markedly higher use of atypical antipsychotics than children with TTD (5.2%), CTD (7.1%) or other TD (7.9%) (Supplementary Table S5).
One-Year Prevalence Proportion (%) for the Use of Psychotropic Drugs and Tic-Suppressing Medications in Children and Adolescents with Tics Overall and by Cohort
Data on melatonin not complete before 2012.
Change statistical significant.
ADHD, attention-deficit/hyperactivity disorder; SSRI, selective serotonin reuptake inhibitors; TCA, tricyclic antidepressants.
In children and adolescents with “pure TD” across all cohorts (n = 1437), 4.9% used antipsychotics (3.5% atypical antipsychotics) (Supplementary Table S6). In the 2014–2017 cohort of children with “pure TD,” 1.8% used antipsychotics, all being atypical, and the use of ADHD medication was low (1.2%) (Supplementary Table S6). ADHD medications were mainly used by children with comorbid ADHD (70%) and antidepressants mainly by children with comorbid OCD (28%) and anxiety (18%) (Supplementary Table S7). Compared with children with “pure TD,” use of antipsychotics were markedly higher in children with psychiatric comorbidities ranging from 15% (TD and ADHD) to 32% (TD and mental retardation) (Supplementary Table S7).
The number of children who were using any psychotropic drug (at least one tic-suppressing medication or other psychotropic drugs) decreased over time from 42% in the 2006–2009 cohort to 38% in the 2014–2017 cohort with the largest decrease observed for atypical antipsychotics (from 18% to 6.4%) (Table 2). The 2- and 5-year prevalence proportions for the use of any psychotropic drug were higher (48% and 57%, respectively) compared with the 1-year prevalence proportion (42%), but otherwise showed similar trends (Supplementary Tables S8 and S9). No substantial changes were observed when requiring two prescriptions to define use (data for this not shown).
There was a steep increase in the proportion of children initiating antipsychotics during the first 180 days after tic diagnosis. However, 37% of children using antipsychotics at some point in our data were already treated with antipsychotics before they received a hospital-based tic diagnosis (Fig. 1).
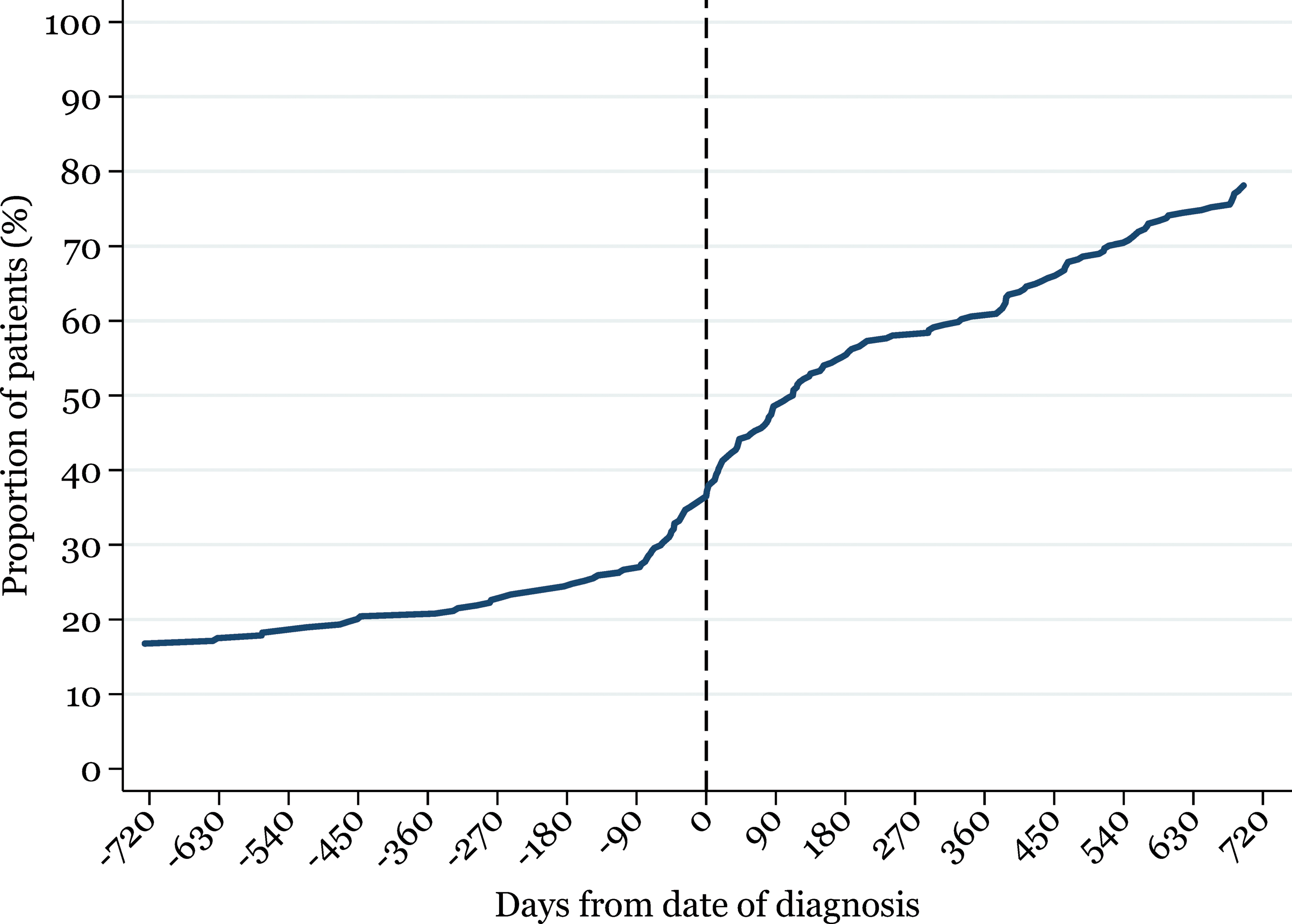
Cumulative proportion of patients receiving the first prescription antipsychotics relative to the date of tic diagnosis (2014–2017 cohort). Color images are available online.
The use of tic-suppressing medications increased with advancing age and the choice of medication varied according to sex (Fig. 2). The use of risperidone was twice as frequent in girls 6–9 years of age as in boys (2.2% vs. 1.1%), whereas the opposite was the case for aripiprazole (0.45% vs. 0.87%). Aripiprazole was the preferred drug in boys (11%) and girls 15–17 years of age (8.4%) and there was a marked difference in the use of risperidone (M/F: 7.3% vs. 2.4%) (Fig. 2).

One-year prevalence proportion for the use of tic-suppressing medication in children and adolescents with tics stratified by age and sex (2014–2017 cohort). Color images are available online.
Over time, aripiprazole was preferred over risperidone among children using tic-suppressing medication (aripiprazole increased from 22% to 38%; risperidone decreased from 57% to 35%). The use of clonidine was stable around 16%–22% (Table 3).
Number and Proportion of Children Receiving the Five Most Commonly Used Tic-Suppressing Medications among the Total Number of Children Receiving Tic-Suppressing Medication (Antipsychotics, Clonidine, Tetrabenazine) in Each Cohort (n)
There were regional variations in the choice of tic-suppressing medication and in the frequency of use. The greatest variation was observed for clonidine, where the 1-year prevalence ranged between 0.51% and 4.1%. However, variation was also noted for the use of aripiprazole (ranging between 1.3% and 5.2%) and risperidone (ranging between 1.3% and 5.0%). In all regions, except one, risperidone and aripiprazole were the preferred treatment (Supplementary Fig. S1).
In most treatment-naive children with tics, risperidone was the first prescription dispensed (32%) followed by aripiprazole (22%) and clonidine (21%) (Fig. 3). The majority of children stayed on their initial treatment for the subsequent prescriptions (Fig. 3; Supplementary Table S10). For the minority who changed treatment, the change most often occurred between the first and third prescription and mostly from risperidone to aripiprazole and vice versa. The pattern was consistent in children non-naive to treatment (Supplementary Fig. S2).
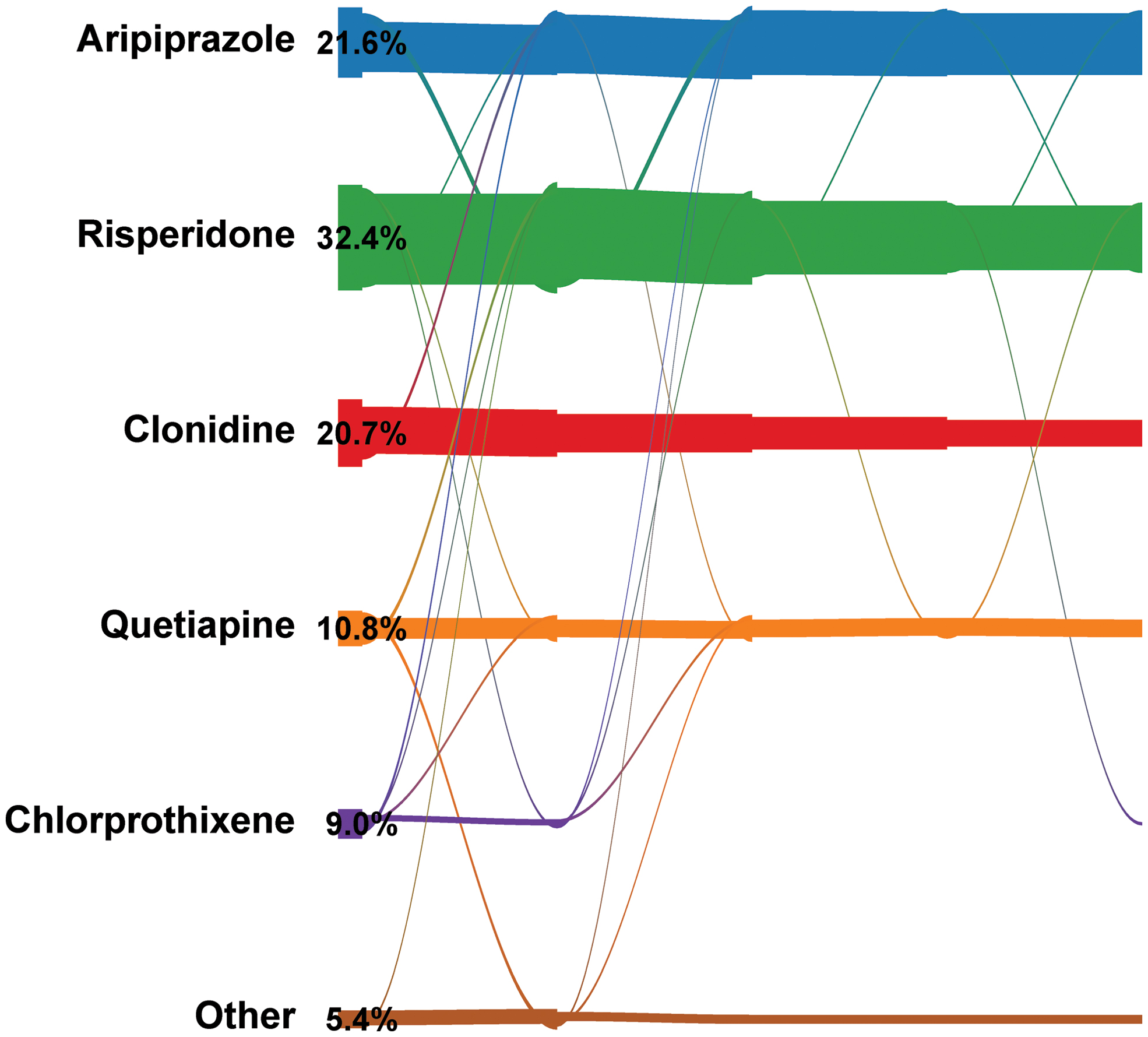
River plot illustrating variations in the choice of tic-suppressing medications in the first 5 prescriptions dispensed after receiving a tic diagnosis in children naive to treatment (2014–2017 cohort). The size of the nodes corresponds to the proportion of children within each category. The width of the links between categories reflects the extent of flow between different treatments, that is, the proportion of users of a specific drug who subsequently filled a prescription for another drug. The difference in volume between links and nodes reflects the number of children who do not fill an additional prescription. Percentages indicate the proportion of children being prescribed the given drug at the first prescription. Color images are available online.
Hospital specialists most often initiated and maintained treatment with tic-suppressing medications and other psychotropic drugs, however, GPs also played a role in the maintenance of treatment (Table 4).
The Prescriber Profile (General Practitioner, Hospital Specialists, Private Specialists) of Incident and Prevalent Prescriptions for Psychotropic Drugs and Tic-Suppressing Medications in Children and Adolescents with Tics (2014–2017 Cohort)
Private specialists in child and adolescent psychiatry, neurologists, or pediatricians.
ADHD, attention-deficit/hyperactivity disorder; FGA, first-generation antipsychotics; GP, general practitioner; NB, numbers in rows do not sum up to 100% due to missing prescriber information; SGA, second-generation antipsychotics.
Discussion
We found that only a limited proportion of children and adolescents with a hospital-based TD diagnosis use tic-suppressing medication during the 1st year after diagnosis. This corresponds well with the watchful waiting strategy that is often applied in the clinical management of TD (Roessner et al. 2011). During the 1st year, children with TD are mainly using drugs targeting psychiatric comorbidities, especially ADHD. Furthermore, use of tic-suppressing medication has decreased over time but with an increasing preference for using aripiprazole. Risperidone remains, however, the most common medication of first-line choice in tics. Hospital specialists are mainly responsible for treatment and most children stay on their initial tic-suppressing medication. There are regional variations in the treatment of TD, which raise the question of whether the pharmacological treatment of TD needs to be harmonized.
Some limitations should be acknowledged. First and foremost, our study was nested in children and adolescents who received a TD diagnosis at a hospital. This means that an unknown number of children and adolescents who receive a TD diagnosis in the primary care sector only, for example, by a child and adolescent psychiatrist or a pediatrician, are not included in our study. This potentially limits the generalizability of our study and this should be taken into consideration when interpreting the results as the patients included in our study might represent patients with more severe TD and also likely higher levels of psychiatric comorbidity. The fact that 37% of children and adolescents using antipsychotics already initiated these drugs before being diagnosed at a hospital might indicate that some of these children already had received a TD diagnosis in the primary sector first (or that they were treated for comorbidities). Second, the TD diagnoses have not been validated in the Danish National Patient Registry. However, we excluded patients only having an unspecified TD diagnosis, which should decrease the risk of having included patients who do not have a TD. Third, the Danish National Prescription Registry holds no information on indication so we can only assume that the drugs were actually used to treat TD or related comorbidity. The fact that we only looked at prescriptions prescribed after the TD diagnosis, and in one analysis also looked at treatment-naive patients, makes it more likely that the drugs were actually used to treat TD or related comorbidity. Specifically, for the use of antipsychotics, we cannot rule out that these were also used to treat other indications than TD. Finally, we used the filling of prescriptions as a proxy for consumption. The fact that our results did not vary substantially when requiring two prescriptions to define use of a drug suggest that this is not a major limitation.
Our study is strengthened by the fact that we relied on data from registries with good validity and a high completeness. Furthermore, by relying on filled prescriptions from an automated database we do not have recall bias.
Our results can be compared with findings from two recent European pharmacoepidemiological studies. Bachmann et al. (2015) described the use of tic-suppressing medication in German children with TD and found that 6.7% used antipsychotics and 2.7% used risperidone in 2011, however, with marked variations according to TD type. In children with TS, 31% used antipsychotics and 11% used risperidone (Bachmann et al. 2015). Carulla-Roig et al. (2018) described the use of tic-suppressing medication in Swedish children with TD and found that 23% used antipsychotics, 14% used risperidone, 9.6% used aripiprazole, and 3.0% used clonidine in 2013. Unlike our study, and the study by Bachmann et al. (2015), Carulla-Roig et al. (2018) did not describe use according to TD type. Based on findings from these two studies, the use of tic-suppressing medication in Danish children and adolescents with TD is seemingly markedly lower than in peers from neighboring countries. It is likely that methodological differences explain the variations in prevalence between our study and the study by Bachmann et al. (2015) and Carulla-Roig et al. (2018). As an example, unlike the two previous studies, we considered the use of medication during the 1st year after a TD diagnosis and when we extend this period, more children initiate tic-suppressing medication. In fact, when considering the use of tic-suppressing medication during the first 5 years in Danish children and adolescents with TD, the results are similar to those for Swedish peers, except that we observe no use of clonidine.
The use of antipsychotics (both FGA and SGA) in children with tics decreased over time, which is in accordance to the decreasing use of antipsychotics observed in the general pediatric population in Denmark (source:
Over time, the use of aripiprazole increased while the use of risperidone and pimozide decreased. This change is consistent with results from a survey of members of the European Society for the Study of Tourette Tourette's syndrome between 2013 and 2017 (Mogwitz et al. 2018). In 2011, a European clinical guideline on treatment of tics was published (Roessner et al. 2011). Based on available evidence at that time and clinical experience, risperidone was recommended as first-choice treatment, but with pimozide, benzamides, clonidine, and aripiprazole mentioned as well (Roessner et al. 2011). In line with the recommendations in this guideline, risperidone was the preferred drug for the treatment of tics in the earliest of our cohorts and importantly, risperidone is still the most common first-choice medication used by Danish clinicians in children and adolescents with tics. The increasing use of aripiprazole corresponds with the emerging evidence after 2012 from two placebo-controlled RCTs on the efficacy of aripiprazole to suppress tics, which consequently led to the approval of aripiprazole to treat tics by the U.S. Food and Drug Administration in 2014 (Sallee et al. 2017). Interestingly, we note that aripiprazole was used in children and adolescents with TD already before the placebo-controlled RCTs were published (Yoo et al. 2013; Sallee et al. 2017), which most likely reflects the already promising efficacy established through nonplacebo-controlled RCTs (Ghanizadeh 2012; Mogwitz et al. 2018), also in children refractory to other treatments (Mogwitz et al. 2018), and the lower risk of weight gain of aripiprazole compared with risperidone (Roessner et al. 2011; Dayabandara et al. 2017).
Aripiprazole was recently put forward currently as the most promising drug for the treatment of tics (Mogwitz et al. 2018). In line with this, aripiprazole and risperidone are the main tic-suppressing medications used in Danish children and adolescents with TD. The recommendations for specific treatment in TD vary internationally, although this must be seen in the context of new evidence that has emerged since the formulation of many guidelines. European experts recommend risperidone as first-choice treatment, whereas in Canada, alpha agonists (clonidine and guanfacine) are recommended over antipsychotics due to lower risk of side effects (Pringsheim et al. 2012). Accordingly, a recent study showed that the recommendations for the use of clonidine to treat tics in Canada has increased while it has decreased for risperidone (Cothros et al. 2019). In Germany, tiapride is recommended as first-choice treatment (Roessner et al. 2011) and accordingly, tiapride was the most prescribed tic-suppressing medication in German children with TD in 2011 (Bachmann et al. 2015). Recently, the American Academy of Neurology recommended alpha agonists over antipsychotics (Pringsheim et al. 2019). In Denmark, the Danish Society of Neuropeadiatrics has put forward recommendations for clonidine in case of mild tics and aripiprazole, risperidone, pimozide, or tetrabenazine in case of more severe tics. Despite this, use of clonidine and tetrabenazine is very limited in Danish children with TD. While clonidine is recommended in children with TD and comorbid ADHD (Roessner et al. 2011), this does not seem to be the common practice in Denmark, or at least not among those diagnosed at a hospital. The regional variations in both the specific choice of tic-suppressing medication and also in the frequency of tic-suppressing medication use may reflect a need for harmonizing the treatment of tics through development of national guidelines. However, importantly, this analysis was based on a few number of patients for some drugs, for example, clonidine with only 34 patients in the 2014–2017 cohort.
The variation in the treatment of tics between boys and girls is surprising, but it is possible that some of the variation, at least in the 15- to 17-year-olds, is explained by the use of tic-suppressing medication, especially antipsychotics, to treat comorbid disorders. Besides tics, antipsychotics may be used to treat severe aggression/irritability related to ASD, bipolar disorder, psychosis, and schizophrenia. In our study, more boys than girls had comorbid ASD, and this could explain the higher use of risperidone in adolescent boys. Our data showed that 7.4% of those using antipsychotics had ASD. However, our data did not allow us to see whether boys with ASD also had severe aggression/irritability as there is not one specific code used for this in clinical practice. Indeed, the finding of a very low use of antipsychotics in children with “pure TD” of 5% and a higher use in children with TD and comorbidities ranging from 15% to 32% indicate that these drugs are also used to treat comorbidities other than tics or that the need for antipsychotics is higher in children who have comorbid disorders, perhaps due to more severe TD. However, contrasting our results, in a clinical cohort of children with TS, the use of antipsychotics did not vary between “pure TS” and TS with comorbid ADHD or OCD (Debes et al. 2009) thus indicating the former.
The finding that the use of tic-suppressing medication increased with advancing age has also been noted in German children and adolescents with TD (Bachmann et al. 2015). This finding may seem surprising as the symptoms of tics tend to decrease in adolescence (Cohen et al. 2013) and the need for tic-suppressing medication decreases. However, this finding is most likely explained by a mixture of several factors. First, as noted above, tic-suppressing medication, may be used to treat comorbidities. Second, we described medication use in patients with newly diagnosed TD. Thus, the oldest children included in our study were included because they received a hospital-based TD diagnosis in adolescence. TD typically starts before adolescence (Plessen 2013) and therefore adolescents included in our study might be included at a time when they needed medication or they were included at the time when they were seeking treatment for psychiatric disorders other than tics, for example, ADHD. However, we provide no explanation for the fact that risperidone was used twice as much by young girls compared with young boys as differences in comorbidities in this specific age group seemingly could not explain such a discrepancy.
Farag et al. (2015) showed that many children with tics try a number of different pharmacological treatment options before a successful treatment is found. As such, only 22% of children with TS from a specialized TS clinic in United Kingdom had successive response to the first medication tried (Farag et al. 2015). Debes et al. (2009) described a clinical cohort of Danish children with TS in 2005 and found that insufficient effect and side effects were the reasons for changes in pharmacological treatment in 23%–43% of children, and only around one third of children had not changed their treatment during their medical history (Debes et al. 2009). Contrary to this, we found that most Danish children and adolescents with TD, or Danish clinicians, are loyal to the first treatment tried, in most cases risperidone and aripiprazole, at least for the first five consecutive prescriptions filled during the first 2 years.
Hospital specialists are mainly responsible for treatment in Danish children and adolescents with TDs, which is reassuring, considering the lack of a national guideline. However, this finding is not as surprising as our study was nested in patients with a hospital-based TD diagnosis. In this cohort, GPs only rarely initiate tic-suppressing medication, but they play a role in the maintenance of treatment which is most likely, and according to guidelines (Sundheds- og Ældreministeriet 2019), coordinated with specialists.
Conclusion
Tic-suppressing medication is only used in a small number of children and adolescents with TD and is limited to the use of risperidone and aripiprazole. One third of children with TD use ADHD medication, seemingly explained by the presence of comorbid ADHD. In line with the emerging evidence for aripiprazole's efficacy, the use of aripiprazole has exceeded that of risperidone, however, risperidone is still the most common first choice in line with European guidelines from 2011. Reassuringly, hospital specialists are mainly responsible for treatment and most children stay on their initial tic-suppressing medication. There are regional variations in the treatment of TD raising questions on whether the pharmacological treatment of TD needs to be harmonized. Furthermore, the difference in the use of tic-suppressing medication between the youngest girls and boys deserves attention.
Clinical Significance
This national study found that the use of tic-suppressing medication is limited in children and adolescents with TD. The use of tic-suppressing medication is dominated by atypical antipsychotics, risperidone, and aripiprazole, which is in accordance with European guidelines and current evidence. This is important considering that these medications are in many countries used off-label to treat TD and considering the lack of national guidelines on the use of tic-suppressing medication in Danish children and adolescents with TD. Other medications prescribed to patients with TD are almost exclusively driven by registered comorbidity.
Disclosures
L.R. reports grants from Jascha Fonden, during the conduct of the study; A.P. reports grants from Alcon, Almirall, Astellas, Astra-Zeneca, Boehringer-Ingelheim, Novo Nordisk, Servier, and LEO Pharma, outside the submitted work; N.B. reports grants from Tryg-foundation, Lundbeck-foundation, and Novo-Nordisk foundation, outside the submitted work. M.T.E. and J.M.T. have nothing to disclose.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.