
Abstract
Objective:
Telemental health (TMH) is not well described for mental health service delivery during crises. Most child and adolescent psychiatry training programs have not integrated TMH into their curricula and are ill equipped to respond during crises to their patients' needs. In this study, we present the implementation of a home-based TMH (HB-TMH) service during the COVID-19 pandemic.
Methods:
We describe the technological, administrative, training, and clinical implementation components involved in transitioning a comprehensive outpatient child and adolescent psychiatry program to a HB-TMH virtual clinic.
Results:
The transition was accomplished in 6 weeks. Most in-clinic services were rapidly moved off campus to the home. Owing to challenges encountered with each implementation component, phone sessions bridged the transition from in-clinic to reliable virtual appointments. Within 3 weeks (March 20, 2020) of planning for HB-TMH, 67% of all appointments were conducted at home, and within 4 weeks (March 27, 2020), 90% were conducted at home. By week 6 (April 3, 2020), reliable HB-TMH appointments were implemented.
Conclusions:
The COVID-19 pandemic crisis created the opportunity to innovate a solution to disrupted care for our established patients and to create a resource for youth who developed problems during the crisis. Our department was experienced in providing TMH services that facilitated the transition to HB-TMH, yet still had to overcome known and unanticipated challenges. Our experience provides a roadmap for establishing a HB-TMH service with focus on rapid implementation. It also demonstrates a role for TMH during (rather than after) future crises when usual community resources are not available.
Introduction
Development of the pandemic
In December 2019, a novel coronavirus (later known as SARS-CoV-2) was identified in Wuhan, in Hubei province, China (Zhu et al. 2020). The resulting disease was initially referred to as “novel coronavirus-infected pneumonia,” and was associated with potential severe complications. Infection was caused mainly by person-to-person transmission and mortality rate was estimated at 2% (Jiang et al. 2020). On January 30, 2020, the World Health Organization (WHO) declared the novel coronavirus outbreak a public health emergency of international concern (World Health Organization 2020a). On February 11, 2020, the disease caused by SARS-CoV-2 was officially named COVID-19 (World Health Organization 2020b). By March 7, 2020, the global number of confirmed cases of COVID-19 surpassed 100,000, and the number of deaths exceeded 3000 (World Health Organization 2020c).
Spread of the virus and associated infection increased rapidly. On March 11, 2020, the WHO declared COVID-19 a pandemic. By March 31, 2020, the WHO reported 750,890 cases and 36,405 deaths internationally and the Centers for Disease Control noted 186,101 cases and 3603 deaths in the United States, leading the world (Centers for Disease Control 2020b; World Health Organization 2020d).
Emergence of COVID-19 in Washington State
On January 21, 2020, the first SARS-CoV-2 infection in Washington State was reported in a man who had recently traveled from Wuhan, China (Washington State Department of Health 2020a). On Feb 28, 2020, the Washington State Department of Health announced two new presumptive cases of COVID-19, one in an individual who had recently traveled from South Korea and the other with no known travel history, suggesting community transmission (Washington State Department of Health 2020b). Then, on February 29, 2020, the first death in Washington State attributed to COVID-19 was reported (Centers for Disease Control 2020a). Following this, a series of patients with COVID-19 in multiple settings was identified, including several individuals residing at long-term care facilities. By March 31, 2020, Washington State reported 6021 cases and 228 deaths attributed to COVID-19 (Washington State Department of Health 2020c).
COVID-19 features
Genomic sequencing of the virus was completed quickly and indicated that SARS-CoV-2 had been spreading undetected in the Seattle area for several weeks (Bedford 2020). Some evidence suggested that asymptomatic or mildly symptomatic persons could shed the virus (Hoehl et al. 2020) and that the virus could remain viable on plastic and stainless steel surfaces for up to 72 hours (van Doremalen et al. 2020). Reports varied on the incubation period, but a small analysis of publicly reported cases found a median incubation period of 5.1 days, with 97.5% of patients developing symptoms within 11.5 days (Lauer et al. 2020). Most cases of COVID-19 were thought to be of mild-to-moderate severity. Testing supplies were limited, precluding the testing of mildly symptomatic individuals. All these factors delayed detection of the virus and contributed to further spread within the community.
Response of Washington State Government and community
The state and local departments of health took steps to contain transmission of the virus. They issued recommendations for appropriate hygiene and “social distancing,” particularly avoidance of large public gatherings. The University of Washington (UW) restricted travel, rescheduled presentations, canceled in-person classes and final examinations in favor of online academic activities, and eventually, halted clinical research. In early March, multiple public schools closed temporarily for decontamination when new onset cases were suspected. Several, but not all, large companies encouraged (and later mandated) employees to work remotely.
Over time, government restrictions expanded including mandates to close schools statewide for a period of 6 weeks (Washington State Office of the Governor 2020a). On March 23, 2020, the Governor issued a “Stay Home, Stay Healthy” order (Washington State Office of the Governor 2020b). Increasingly, children and parents were homebound. An overall timeline is provided in Figure 1.

Chronology of COVID-19–related events.
Seattle Children's Hospital response
Seattle Children's Hospital (the Hospital) is the tertiary pediatric medical center for a five state region that includes Washington, Wyoming, Alaska, Montana, and Idaho (WWAMI). On March 2, 2020, the Hospital intervened to protect patients and staff by decreasing person-to-person exposure, such as restricting the number of hospital entrances, screening staff and patients for symptoms or travel at hospital entry, and limiting visitors to primary caregivers. The Hospital encouraged patients to use phone consultation in lieu of clinic appointments for apparent minor illnesses and halted elective surgical procedures. Nonessential staff were encouraged to work remotely.
The Department of Psychiatry and Behavioral Medicine at Seattle Children's Hospital (the Department) comprises the Division of Child and Adolescent Psychiatry and training site for the Department of Psychiatry and Behavioral Sciences at the UW that serves the WWAMI region. On February 28, 2020, the Department started to discuss the possibility of converting the outpatient clinic to a virtual telemental health (TMH) clinic.
The first step was to transition established patients from in-clinic appointments to at-home phone appointments by clinicians who remained in the clinic. Between March 4 and 6, 2020, the Department presented a plan to transition to home-based TMH (HB-TMH) services for as many established patients as deemed appropriate and started to plan enrollment of new patients into HB-TMH. Faculty were to remain in the clinic while delivering HB-TMH. The clinic already had a small group of TMH faculty with the long-term goal to expand these services to the Hospital's satellite clinics, community sites, and the home. We fast tracked this process.
Telemental health
The Center for Medicare and Medicaid Services refers to telemedicine as the delivery of health care services through real-time interactive videoconferencing (Center for Medicare and Medicaid Services 2020). When telemedicine is used to deliver mental health services, the term telemental health is used. In this article, we use both terms. We use the term telemedicine to cover all applications of this modality for patient care and the term telemental health specifically to address mental health applications. The Department had an active TMH service for 18 years with services in Washington, Alaska, and Wyoming.
Numerous studies have demonstrated that evidence-based mental health treatments can be safely implemented through TMH with high levels of patient and provider satisfaction (Myers et al. 2007, 2008; Glueck 2013). Effectiveness has been established in multiple studies with adults (Mishkind et al. 2018) as well as youth diagnosed with a range of disorders (Storch et al. 2011; Himle et al. 2012; Reese et al. 2013; Wacker et al. 2013; Myers et al. 2015) and across treatment modalities (Reese et al. 2012; Xie et al. 2013; Myers et al. 2015; Tse et al. 2015).
Emerging evidence also indicates that evidence-based TMH therapies are safe and effective when delivered to youth outside of clinic settings such as schools (Stephan et al. 2016) and the home (Comer et al. 2014, 2017; Roth 2020), potentially offering more ecologically valid, as well as family-friendly, interventions. However, HB-TMH, using direct-to-consumer (DTC) platforms, involves concerns beyond those encountered in traditional clinic settings.
Published TMH guidelines address the safety of TMH practice generally (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017; Shore et al. 2018). Luxton et al. (2010, 2012, 2014) have further noted special considerations for HB-TMH with adults with focus on issues such as privacy, security of technology platforms, management of crises including suicidality, and disclosure of information in the case of emergency. HB-TMH for youth entails challenges in operationalizing some of these issues, particularly legal guidelines such as parental consent, disclosures, and procedures for monitoring safety (Kramer and Luxton 2016). Recently, Schoenfelder Gonzalez et al. (2019) have addressed these concerns with recommendations that facilitate the delivery of TMH to youth in the home.
Methods and Implementation
At the time of the COVID-19 crisis in Washington, the Department had 105 clinical faculty and staff, summarized by discipline in Table 1. Of these, 48 had been officially privileged by the Hospital in telemedicine practice but only 18 were providing some form of regular clinic-to-clinic services. Eight faculty members were providing HB-TMH services that included six psychologists and two psychiatrists. Thus, 57 faculty members needed to complete official basic Hospital privileging in telemedicine and 97 needed to receive additional training in delivering TMH services to the home.
Department Clinical Faculty by Discipline
Before the emergence of COVID-19, the Hospital's existing privileging protocol for telemedicine consisted of five steps: (1) complete training with the Audio-Visual Department to learn use of the legacy videoconferencing endpoint system and the online program used for clinic-to-clinic and at home services, (2) complete didactic self-administered modules and post-test on the Hospital's Learning Center, (3) read a selected article that for the Department of Psychiatry and Behavioral Medicine included a choice between the telepsychiatry guidelines published by the American Academy of Child and Adolescent Psychiatry (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017) or a book chapter on telepsychiatry practice (Myers and Roth 2017), (4) observe a 30–60-minute clinic-to-clinic TMH session with a designated privileged faculty, and (5) submit attestation of completion of these steps to the Medical Staff Office. The last step took approximately 2 months from completion of training steps to privileging.
We planned to implement this protocol with the 57 faculty who needed basic Hospital privileging and then to train all 97 who needed experience in the DTC platform to deliver HB-TMH services. We updated the Hospital's protocol based on the AACAP telepsychiatry guidelines (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017) augmented with additional recommendations for HB-TMH services generally (Luxton et al. 2012) and with youth specifically (Schoenfelder Gonzalez et al. 2019; Roth 2020).
The Department conducts, on average, 28 parent and/or child treatment or support groups per week. We had not previously conducted any group interventions by TMH. Therefore, one of the authors (T.S.) offered a 1-hour videoconference-based faculty training session to discuss translation of group treatments to HB-TMH (“TeleGroups”). The session included demonstration of features of the platform, sharing of initial acceptability data, clinical considerations, and discussion of faculty concerns and ideas.
Nine faculty members who participated in this training completed quantitative ratings of their attitudes toward providing TeleGroups. After the training, faculty reported increased comfort with TeleGroups, and moderate to high comfort with presenting information and leading discussions in a TeleGroup format to the home. The primary concerns focused on technological glitches and the potential stress of leading a group in the HB-TMH format. We decided to proceed with selected home-based TeleGroups contingent upon group leaders' determination of appropriateness to their patients and families.
Results
The feasibility of implementing a clinic-wide HB-TMH service met with administrative, technological, training, and clinical challenges to several components of Departmental functions. The relevant components are shown in Figure 2.
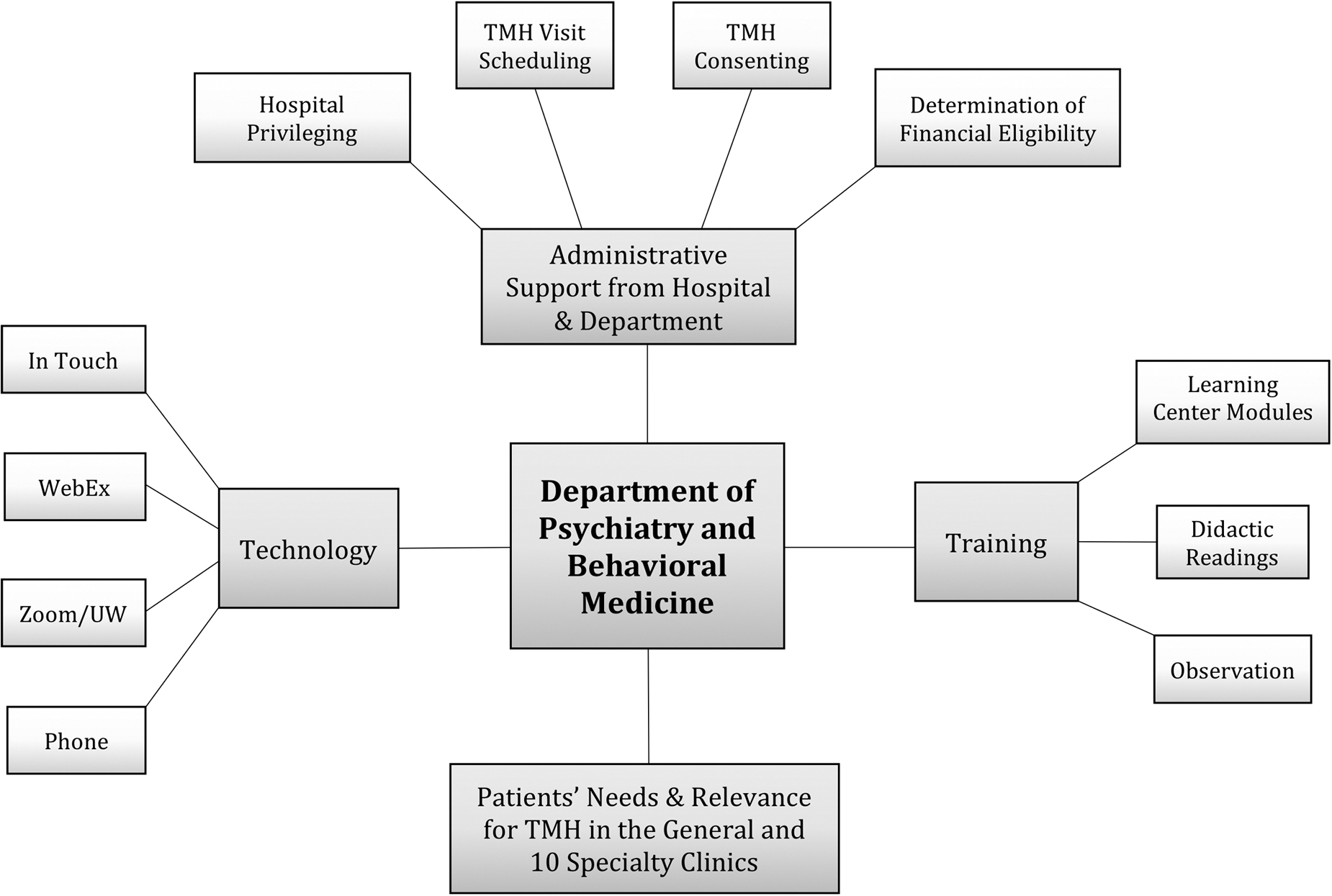
Components contributing to HB-TMH implementation. HB-TMH, home-based telemental health.
Challenges encountered and approaches to management: round 1
Administratively, and early in the pandemic, the Medical Staff Office noted that it could not rapidly process applications of faculty needing Hospital privileging for telemedicine. The Hospital's scheduling office could not manage the novel steps required for TMH scheduling in the DTC platform or remote consenting. Technologically, in January 2020, the Hospital had changed its videoconferencing platform and vendor. Therefore, most faculty members required training in use of the DTC platform that was new to even the experienced faculty.
From a training perspective, the faculty who had not obtained Hospital privileging needed an observational session with the five faculty members designated for training who also had ongoing TMH clinics. Clinically, we did not know how many families could avail themselves of private and secure clinical services at home. Alternative options such as phone appointments needed to be considered for these families to ensure clinical care could continue.
These challenges were addressed in several ways, as depicted in Figure 3. The Medical Staff Office temporarily waived the final step of Hospital privileging. Rather, faculty members completed all of the aforementioned steps and submitted their attestations to Departmental leadership that approved them to render TMH services.
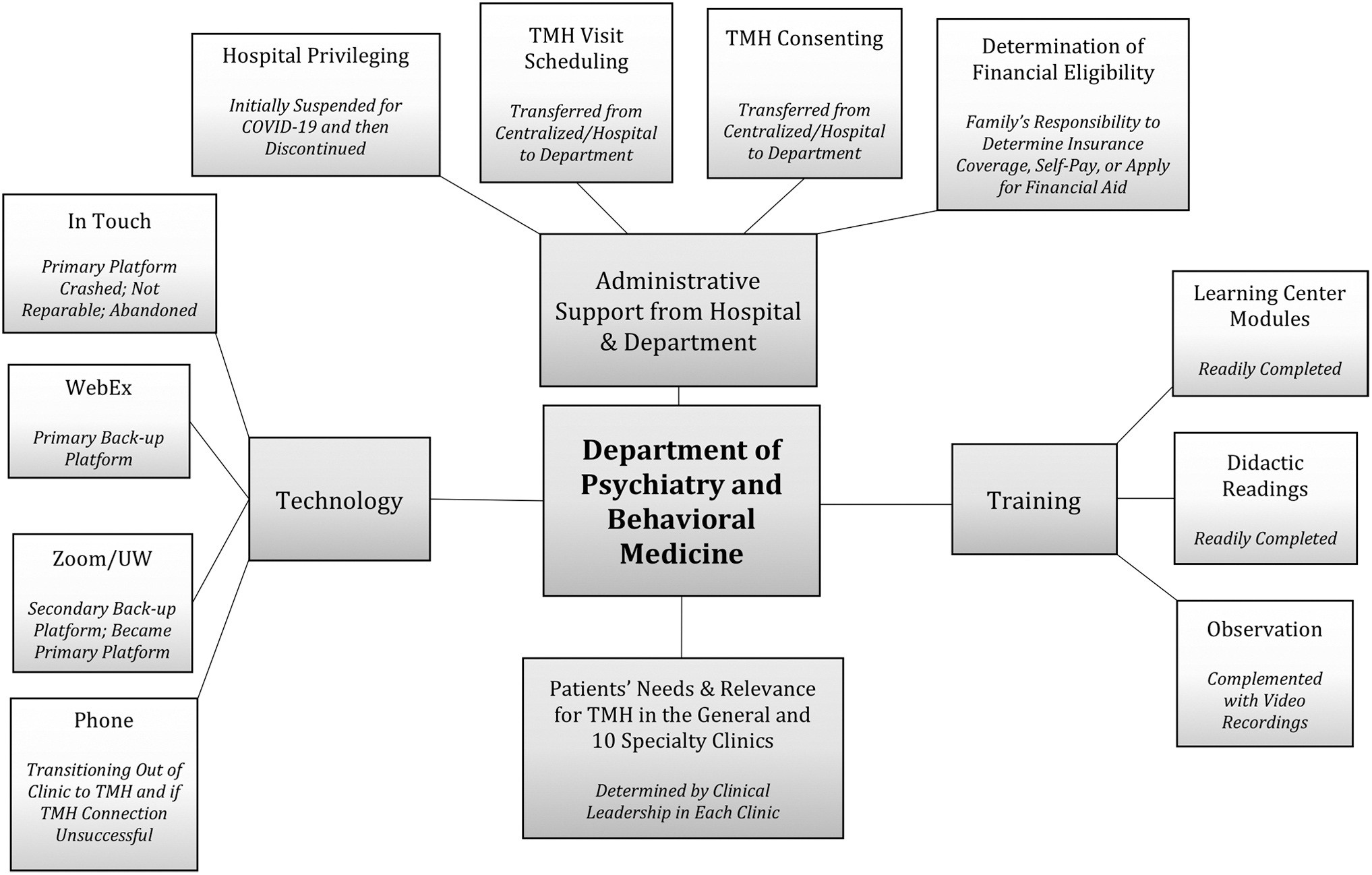
Modification of components contributing to HB-TMH implementation. HB-TMH, home-based telemental health.
We developed a protocol to convert established patients from in-clinic to HB-TMH sessions with their same clinician. The protocol included scripts for clinicians or support staff to explain the HB-TMH service and to conduct a form, the HB-TMH Pre-Screening Guidelines, focused on assessing the ability to conduct TMH sessions safely at home, including phone numbers for local contacts (e.g., police, pastor, relative, or neighbor) should urgent situations occur. The faculty or staff obtained consent for TMH, explained the potential limitations of payment by their insurance plans, and the options for financial aid from the Hospital.
We trained the Hospital's scheduling office in procedures to convert in-clinic appointments to a TELEMED HOME visit type, activate a MyChart Account, provide e-Check-in instructions, obtain the family's appropriate e-mail address, and then communicate the date and time of the HB-TMH appointment to the faculty and family sending appropriate links to each. At or before the first HB-TMH session, the clinical faculty reviewed the HB-TMH Pre-Screening Guidelines and then administered the TMH Privacy and Safety Screening Form that reviewed potential clinical risks and appropriate interventions (both forms available upon request).
To quickly and efficiently train faculty in the DTC platform and clinical aspects of HB-TMH, we remotely conducted four 45-minute group training sessions; faculty needed to attend only one of the sessions. During these four sessions, n = 24, n = 25, n = 20, and n = 32, learners attended remotely. A brief technical guide was provided to all attendees to assist in their subsequent TMH clinics. We developed a “cheat sheet” to guide families through the process of setting up their home systems and responding to the e-invite for a HB-TMH session.
To complete the requirement of an observational session with a designated privileged staff, we broadened the list of supervising faculty from five to nine. We provided a checklist of session components for the supervising faculty to note and to discuss (available upon request). Such components included topics such as room setup, camera arrangement, lighting, audio, privacy, and relatedness. During the session, the supervising faculty commented on the optimal or suboptimal status of these components to help the faculty members anticipate and manage the inconsistencies that occur during HB-TMH practice. We started contacting established patients and families.
Challenges encountered and approaches to management: round 2
On March 17, 2020, the president moved telemedicine to the forefront of health care and prevention during the COVID-19 crisis. Certain regulations specified in the Health Insurance and Portability Accountability Act (HIPAA) (United States Department of Health and Human Services 1996) were suspended temporarily. The Office for Civil Rights at the Department of Health and Human Services indicated that a health care provider could use any popular, but nonpublic facing, remote communication product to communicate with patients. Providers were encouraged to notify patients that these third-party applications potentially introduce privacy risks, and to enable all available encryption and privacy modes when using such applications. Noncompliance with HIPAA rules in connection with the good faith provision of telemedicine using such nonpublic facing products would not be penalized during the COVID-19 nationwide public health emergency (United States Department of Health and Human Services 2020).
In response, the Department encouraged staff and faculty to practice from home. Support staff worked to enroll patients in HB-TMH while obtaining administration guidance remotely. Faculty members needed additional assistance to utilize the DTC platform from home. During this time, there was a significant decrease in overall outpatient volume. While awaiting full implementation of the HB-TMH service, or awaiting completion of their training for HB-TMH, faculty members conducted phone visits for their established patients. By March 20, 2020, appointment volumes started to stabilize and ∼67% of all outpatient appointments were conducted at home. Most of these appointments were conducted by phone with some TMH sessions. By March 27, 2020, 90% of all outpatient appointments were done at home, predominantly by phone (59%) but increasingly by HB-TMH (31%). One week later (April 3, 2020), these rates were 48% versus 45%, respectively. Table 2 gives the transition from in-clinic to at-home appointments over 5 weeks from beginning discussions of a transition to virtual clinics.
Appointment Types and Volumes by Week
HB-TMH, home-based telemental health.
We started development of a protocol to enroll new patients whose scheduled in-clinic appointments had been put on hold. If families were not interested in participating in a HB-TMH visit and were not high acuity, then their visits were postponed until a later date when in-person visits can again occur. If a family was not able to participate in HB-TMH due to lacking Internet, then a phone appointment was offered to ensure equity.
Challenges encountered and approaches to management: round 3
We immediately encountered two major setbacks. First, the Hospital's primary DTC platform crashed when many faculty members across the Hospital logged on to provide home-based services. Some faculty members continued to access the primary and/or the secondary backup platform successfully, but phone sessions that require much less bandwidth continued to be the major platform for patient care while awaiting reliable availability of the DTC platform. In an attempt to provide home-based TeleGroup services, one of the authors (T.S.) conducted a pilot test with three groups of eight to nine parents each (n = 25) enrolled in the Incredible Years School-Aged parent program. The primary DTC platform again did not provide adequate connectivity. The secondary backup platform did well. A survey of parents indicated their preference for this secondary backup platform in terms of ease of use, connectivity, engagement, and overall satisfaction with their experience.
In response to the seemingly unresolvable difficulties with our primary DTC platform, the Hospital initially allowed use of a tertiary back-up DTC platform available to faculty through their appointment at the UW Hospital. When problems with the primary DTC platform were not resolvable after 3 weeks of technical consultation, the Hospital decided to contract directly with this vendor. This delayed the full implementation of HB-TMH services another 2 weeks during which the Department delivered care through a mix of phone and the three DTC platforms.
The next challenge related to the observation sessions required as part of training for those faculty who had not obtained Hospital privileges. Many clinic-to-clinic contracted TMH sites closed with intent to move to HB-TMH or phone services. Thus, the Department's designated TMH supervising faculty no longer had training clinics at which to conduct observations efficiently. Connecting from one home to another risked technical difficulties with each new connection, required more time, and infringed upon documentation efforts, all of which impeded training and service delivery. We managed this challenge in two ways. We conducted remote group observations with faculty connecting to volunteer families. We also used recordings of TMH sessions from an earlier project to demonstrate the components of a clinically appropriate TMH session.
Challenges encountered and approaches to management: round 4
Daily challenges continue. Each day the faculty analyzes and adapts to government edicts, administrative requirements, technical inconsistencies, patients' needs, and faculty's efforts at juggling work and family at home to comply with the State's mandate to “Stay Home, Stay Healthy”: analysis interminus.
“Final” implementation
By March 31, 2020, 98% of faculty completed expedited training and obtained Departmental approval for HB-TMH services during the COVID-19 crisis. Clinical leaders in each specialty clinic within the outpatient psychiatry clinic determined the criteria for who would be offered HB-TMH and who would continue to be treated in-person. For example, the autism clinic had already established HB-TMH services for their applied behavior analysis clinic, feeding clinic, and pharmacotherapy clinic, all of which they then expanded. Patients in the mood and anxiety clinic predominantly moved to TMH. Initially, the Dialectal Behavior Therapy (DBT) clinic continued individual sessions through HB-TMH while planning to include family sessions at a later date. The early childhood clinic started plans for conversion to HB-TMH. The Incredible Years and anxiety programs successfully implemented selected parent components of our TeleGroups. By April 10, 2020, we were offering HB-TMH to all established outpatients for individual visits and had started a trial process for enrolling new patients. Continued work on expanding TeleGroups occurred. Only the crisis clinic continued a regular in-clinic presence.
Next steps: trainees
On March 18, 2020, Dr. Thomas J. Nasca, MD, MACP, the president and chief executive officer of the Accreditation Council for Graduate Medical Education (ACGME), notified the members of the Graduate Medical Education Community that ACGME was accelerating implementation of telemedicine requirements originally scheduled for July 2020. ACGME announced that effective immediately, it permitted residents/fellows to participate in the use of telemedicine to care for patients affected by the COVID-19 pandemic, noting that “In no situation will a program be penalized retroactively for appropriate engagement of residents and fellows with appropriate supervision in the use of telemedicine during this crisis” (Accreditation Council for Graduate Medical Education 2020).
The Department already had four trainees able to conduct TMH sessions, and two were trained in HB-TMH. We started to train the remaining 47 fellows, general psychiatry residents, psychology residents, and psychology postdoctoral students in service delivery through HB-TMH.
Discussion
Over the past several decades, telemedicine has been used to provide direct medical services to patients or consultation to first responders and local physicians in the aftermath of disasters such as hurricanes (Vo et al. 2010) and oil spills (Kim et al. 2013) and during crises such as the treatment of refugees (Ripton 2016) or individuals in conflict areas (Medicines San Frontieres 2016). Less often telemedicine has been used to provide psychiatric services after disasters and crises, particularly to treat patients with post-traumatic stress in international populations (Jefee-Bahloul 2014; Qadir et al. 2016; Soron et al. 2019).
The mandate during the COVID-19 pandemic to use telemedicine to aid in social distancing has created a role for telepsychiatry during a crisis. Our experience may provide lessons for psychiatry training programs seeking to include telepsychiatry in their practices during the current pandemic, and during future crises that are sure to occur (Yellowlees et al. 2016; Gates 2018). Beyond such pragmatic clinical and service-related lessons, our experience demonstrates an inspiring collaboration between psychiatry and community to aid efforts to reduce the severity of a pandemic while meeting patients' needs, as well as to show the way to innovate in the future.
The Department of Psychiatry and Behavioral Medicine at Seattle Children's Hospital had an existing TMH infrastructure on which to build HB-TMH services. The good news is that it took only 6 weeks for a large training program to move from beginning considerations to actual implementation of a stable HB-TMH program. The bad news is that it took 6 weeks to do so.
The Department had several psychiatrists and psychologists already using TMH for clinical care and teaching and an administration familiar with the needed protocol modifications needed to convert the outpatient faculty to HB-TMH. All were able to mobilize quickly to teach other faculty and problem-solve needed next steps to convert to a virtual clinic. Most distressing and delaying to full HB-TMH implementation was the failure of our videoconferencing platform. There were many clues over the preceding months regarding the inadequacy of this outpatient platform, but as psychiatry was the major outpatient user—and thus the major complainer—a quick resolution was not forthcoming as efforts were focused on the more sophisticated inpatient platform used for consultation to medical units across the WWAMI region. Perhaps the failure of the platform due to excessive use during the crisis could not be anticipated.
Despite technological vulnerabilities, however, it is clear that telepsychiatry specifically, and telemedicine broadly, will be one remedy for acutely stalled health care services during the next crisis. Some modeling of technology resilience during future crises seems warranted. Back-up systems are crucial, particularly as the COVID-19 crisis has shown us that HIPAA can be waived and multiple back-up systems deployed. Smaller training programs that are now seeking to develop HB-TMH services may be able to address these technological problems more easily and redundant systems are recommended.
No less relevant than the technology challenges were the many inter-related administrative steps needed to convert services from the clinic to the home and to implement HB-TMH clinic wide. Modifications to usual procedures for consenting, scheduling, and billing required staff and patient training and written protocols. Possibly these steps could be less complex than described here. Our Department is large with faculty and support staff spread across four sites with many specialty clinics within each site, multiple trainees across disciplines, and patients across multiple counties. We needed a single reliable process for all. Community medical centers or small training programs likely could streamline some of these processes to expedite the process—but maybe not as this option has not yet been tested. The important issue is to develop a reliable process and role designations that contain anxiety for faculty, staff, and patients during an already anxiety-provoking time. Cross-training is recommended.
The financial implications are noteworthy. Our census fell dramatically as we transitioned patients from clinic to home. The interim phone appointments, while awaiting full implementation of HB-TMH services, yielded less revenue per appointment than an in-clinic or HB-TMH appointment, although required the same amount of time and almost the same level of documentation by the faculty. However, the census is increasing as technology and administrative procedures are implemented. Psychiatry may be at lower financial risk than other medical specialties. During COVID-19 crisis, many elective surgical and medical procedures were cancelled, imperiling practices. As most psychiatry does not depend on procedures, there is less risk of sustained financial loss. Furthermore, as psychiatric needs often increase during crises, planning for future crises should consider an escalation of services and consideration of revenue.
TMH has been “here to stay” for several years in response to the convergence of technological advances and public mandates to increase access to psychiatric care, improve the quality of that care, and support primary care providers in their efforts to care for their patients' mental health care needs. The current federal mandate for telemedicine will make HB-TMH “here to stay,” particularly as families strive to reconstruct their lives and minimize the inefficiencies of attending appointments at medical centers. Crises create opportunities and bring lasting societal change. Exactly what HB-TMH will look like after the COVID-19 crisis is not clear; but our faculty's relatively rapid, but complicated, development of clinic-wide HB-TMH and TeleGroups may prelude to the opportunities to come. In a future state, HB-TMH may help overcome barriers to treatment such as distance, transportation, and scheduling. Continued innovation will allow for psychiatry to be mobilized more rapidly during the next crisis.
Limitations
The experiences described here apply predominantly to training programs with some existing TMH service delivery. It is possible that the Department's size and affiliation with a major hospital both facilitated and obstructed the rollout process. It is also possible that training programs without any TMH foundation would encounter more hurdles. It is difficult to know how to get started. We are not aware of protocols that other training programs used for HB-TMH before or during the COVID-19 pandemic, and whether they conducted training, prescreening, or safety assessments similar to those described here.
Our experience does not apply to small private practices that have apparently easily contracted with videoconferencing vendors to incorporate TMH platforms into their outpatient work (personal communications with AACAP and APA Telepsychiatry Committees). How familiar these providers are with issues affecting HB-TMH practice is not known. They should refer to available guidelines to ensure safe and effective practice (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017) and resources to help families to successfully utilize HB-TMH (Roth 2020).
Conclusions
In response to the COVID-19 pandemic, we built upon an existing, but limited, TMH program to implement a HB-TMH service across a large Child and Adolescent Psychiatry Department over the course of 6 weeks. Implementation during a crisis does not mean compromising clinical and technological training. Rather, processes can be streamlined to facilitate faster implementation of the service with groups of learners. Our experience demonstrates that groups, as well as individual, treatments can be rapidly converted to a HB-TMH format. A process to assess the operational, technological, and clinical challenges that will inevitably occur will facilitate ongoing quality improvement in services that are developed during a crisis.
Clinical Significance
When a local, regional, or worldwide crisis occurs, creative solutions are necessary to address youths' existing, and to anticipate their evolving, mental health needs. During the COVID-19 pandemic, telemedicine has emerged as a safe and effective approach to meet these needs. However, delivering high-quality HB-TMH care requires planning, training, and iterative reassessment. Providers need training to anticipate unique clinical, technological, safety, and legal considerations involved in the delivery of HB-TMH services, and departments should implement protocols to operationalize such training. Our experience demonstrates the feasibility of rapidly building upon an existing telemedicine infrastructure to train a large group of multidisciplinary providers to deliver urgent HB-TMH services. However, the take-home message is that even with a well-established telemedicine infrastructure, programs must expect to encounter serious challenges during crises. Planning for the next crisis starts now.
Footnotes
Acknowledgements
The authors thank the staff of the Department of Psychiatry and Behavioral Medicine for their expert assistance, as they went above and beyond their usual activities in the midst of the COVID-19 pandemic to provide us data: Cris Fernandez for trouble-shooting the technology, providing data on clinicians training and their progress, as well as his long-standing dedication to the Telemental Health program and its vicissitudes; Marie Augustine for multiple timely data iterations; David Hall for clinic census across modalities with associated timelines; and Kathy Brewer for overall programmatic data.
Disclosures
No competing financial interests exist.