
Abstract
Objective:
This study aimed to assess the prevalence of overweight and obesity in the group of children and adolescents with attention-deficit/hyperactivity disorder (ADHD) according to three different diagnostic criteria for obesity. The effect of ADHD treatment on the risk of obesity was controlled.
Materials and Methods:
The study group consisted of 58 subjects aged from 8 to 17 years with ADHD. Control group consisted of 62 healthy age- and sex-matched children and adolescents. Overweight and obesity were assessed according to International Obesity Task-Force (IOTF), World Health Organization (WHO) and European Childhood Obesity Group (ECOG) criteria.
Results:
There was a significantly higher incidence of obesity in ADHD group according to WHO (ADHD vs. Control: 17.2% vs. 3.2%, p = 0.01) and IOTF criteria (ADHD vs. Control: 10.3% vs. 1.6%, p = 0.04), but no significant difference according to ECOG criteria. There was significantly higher occurrence of overweight (20.7% vs. 12.8%, p < 0.001), obesity (10.3% vs. 3.5%, p < 0.001), and overweight and obesity (31.0% vs. 16.3%, p < 0.001) in the ADHD group compared to the Polish population. The analysis did not show a statistically significant relationship between the amount of taken psychostimulant and the occurrence of overweight and obesity.
Conclusions:
The prevalence of overweight and obesity in the group of ADHD children and adolescents varies depending on the choice of diagnostic criteria. At the same time, it is significantly more frequent than in the general population. We suggest that future studies should give a clear rationale for the selection of cutoff points to minimize errors that could confound data analysis and interpretation.
Introduction
The comorbidity between attention-deficit/hyperactivity disorder (ADHD) and overweight/obesity has been an important research topic in recent years. The results of the previous studies show that ADHD is a risk factor of excess body weight in children and adolescents (Spencer et al. 1997, 2006; Holtkamp et al. 2004; Curtin et al. 2005; Faraone et al. 2005; Anderson et al. 2006; Hubel et al. 2006; Swanson et al. 2006; Lam and Yang 2007; Hanć and Cieślik 2008; Waring and Lapame 2008; Ptacek et al. 2009; Chen et al. 2010; Erhart et al. 2012; Hanć et al. 2012; Byrd et al. 2013; Güngör et al. 2013; Racicka 2013; Yang et al. 2013; Schwartz et al. 2014) and adults (Pagoto et al. 2009; Fuemmeler et al. 2011; Cortese et al. 2013). Nevertheless, several studies did not confirm this association (Mustillo et al. 2003; Dubnov-Raz et al. 2011).
Two of the most recent meta-analysis also gave inconsistent results. The meta-analysis by Cortese et al. (2018), which included 42 studies, has shown a significant association between ADHD and obesity in children and adolescents (odds ratio [OR] = 1.20, 95% confidence interval [CI] = 1.05–1.37) and in adults (OR = 1.55, 95% CI = 1.32–1.81). This association was also significant for overweight. The obesity prevalence was increased by about 70% in adults and by about 40% in children with ADHD compared with those without ADHD diagnosis. There was no association between pharmacological treatment and a higher risk of obesity. In turn, the results of the meta-analysis by Nigg et al. (2016) indicate a lack of statistically significant association between ADHD and the occurrence of overweight/obesity in children, but a possible relationship in adolescent girls (especially in those with a comorbid diagnosis of depressive or conduct disorders). The association between ADHD and the occurrence of overweight/obesity in adults (OR = 1.37, 95% CI = 1.19–1.58) is significantly stronger than in youth (OR = 1.13, 95% CI = 1.00–1.27).
Previous studies used heterogeneous diagnostic methods for obesity, which could contribute to incoherent findings. In studies carried out on the adult population, the World Health Organization (WHO) criteria were used. Overweight was defined as body mass index (BMI) value >85 percentile and obesity as BMI >95 percentile (Pagoto et al. 2009; de Zwaan et al. 2011; Fuemmeler et al. 2011; Cortese et al. 2013). In children, population authors used three different, the most popular criteria. Some studies used the criteria of BMI value >85 percentile (adjusted for age and sex) for overweight and BMI >95 for obesity (Curtin et al. 2005; Waring and Lapane 2008; Dubnov-Raz et al. 2011; Fliers et al. 2013; Yang et al. 2013; Bener and Kamal 2014; Kim et al. 2014; Kummer et al. 2016; Nigg et al. 2016). Other used criteria of BMI value >90 percentile for overweight and BMI >97 percentile for obesity (Holtkamp et al. 2004; Erhart et al. 2012; Türkoʇlu et al. 2015). Finally, overweight and obesity definitions might be based on International Obesity Task-Force (IOTF) cutoff points for BMI (Hanć et al. 2018; Racicka et al. 2018). Even in both mentioned meta-analyses, no coherent overweight and obesity inclusion criteria were used.
This study aimed to assess the prevalence of overweight and obesity in the group of children and adolescents with attention deficit hyperactivity disorder in comparison to control group and the population according to three different diagnostic criteria for obesity. Given the previous findings on suppressive effects of stimulant treatment on growth, its relationship to BMI, and—in consequence—overweight and obesity, the important aspect of the current research was to carefully control the effects of ADHD pharmacotherapy on the studied relationships.
Materials and Methods
Ethical and financial statements
The study has been approved by the Ethics Committee of the Warsaw Medical University and has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
This research was supported by the National Science Centre Poland Grant: 2015/17/N/HS6/03020.
Study group
The clinical group consisted of 58 patients from the outpatient psychiatry clinic, aged from 8 to 17 years, without exclusion conditions. The diagnosis was performed according to criteria of Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR; American Psychiatric Association 2000) for one of the three ADHD types: predominantly inattentive or impulsive/hyperactive or combined type as previously described (Racicka et al. 2018). For the comorbid diagnosis, supplements of Kiddie-Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime (K-SADS-PL ver.1.0) version (Kaufman et al. 1997) were administered by the child psychiatrist and the diagnosis was based on the International Statistical Classification of Diseases and Related Health Problems, 10th Revision diagnostic criteria (World Health Organization 1994). The diagnosis was performed during at least three appointments, during which children also underwent physical, neurological, and developmental examination. Exclusion criteria encompassed comorbid disorders, which could cause weight gain (e.g., diabetes, dysfunction of the thyroid gland), as well as psychiatric disorders (e.g., depressive disorder, anxiety disorders, autism spectrum disorder, intellectual disability, eating disorders, psychotic disorders) and any problems that could result in limited collaboration (e.g., defect vision, hearing loss). The duration of treatment was calculated as interval between the onset of pharmacological treatment (metylphenidate osmotic release oral system [OROS], metyphenidate sustained-release [SR]) and assessment time,. Then we estimated cumulated dose of drugs using the following equation: mg/day × days of treatment (up to the moment of assessment). The cumulated dose was calculated based on the assumption that the drugs were received 7 days/week and holiday breaks were taken into account.
Control group consisted of 62 healthy age- and sex-matched children and adolescents from primary and secondary schools between 8 and 17 years of age. Exclusion criteria were as follows: ADHD (the presence of attentional problems declared by parents), close family members (parents, siblings) with ADHD/attention deficit disorder diagnosis, neurological or psychiatric diagnosis, dyslexia, previous brain injury with the loss of consciousness, any disease that could cause weight gain (e.g., diabetes, dysfunction of the thyroid gland), and any problems that could result in limited collaboration (e.g., defect vision, hearing loss).
All participants received 150 Polish Zloty for the study.
Age calculation
The calendar age at the time of the test was calculated based on the date of examination and date of birth of the patient. Depending on needs, the age was determined in annual (standardization of growth, weight and BMI) or half-year intervals (assessment of overweight and obesity).
Anthropometric measurements
Body weight was measured with a medical scale (Radwag PUE c/31) with an accuracy of ±100 g. Height was measured using a Harpenden anthropometric instrument with an accuracy of 0.1 cm according to the standard technique (de Onis et al. 2004; Chumlea and Guo 2006) by trained medical staff. Children were weighted in their underwear. The measurements were performed between 9 a.m and 4 p.m. BMI was calculated on the basis of body weight and height. Height, weight, and BMI were later standardized according to sex and age using two sets of references developed for Polish population (Palczewska et al. 2000; Kułaga et al. 2011). Charts published by Kułaga et al. (2011) are the most up-to-date, based on data collected from 2007 to 2009. We also used charts of Palczewska et al. (2000) developed using measurements collected earlier, between 1996 and 1999, as at the time of the study, they were still in use in some clinical settings.
Overweight and obesity diagnosis
Overweight and obesity were assessed according to three different criteria IOTF (Cole et al. 2000, 2007), WHO/Center of Disease Control (CDC) (Must et al. 1991), and European Childhood Obesity Group (ECOG) (Rolland-Cachera et al. 1991). IOTF cutoffs for subsequent age categories were based on BMI data from six nationally representative surveys and corresponded approximately to the 90th percentile for overweight and the 98th percentile for obesity (Cole et al. 2007). WHO recommends using 85th and 95th and ECOG 90th and 97th percentile of BMI distributions, respectively.
Subjective socioeconomic status (SES) was assessed using Polish adaptation of MacArthur ladder, parental educational level of the subjects was compared.
Statistical methods
The Pearson correlation coefficient and regression analysis were used to assess the relationships between standardized values of z scores for height, weight, and BMI with age and cumulated dose of drugs.
Student's t-test was applied for z scores comparisons between the sample and control group and the χ 2 test was applied to assess differences in distributions of overweight, obesity, and overweight/obesity between the two groups.
Logistic regression was used to asses the effects of the cumulated dose of drugs on the risk of overweight and obesity in the study group. The quartiles of the cumulated doses of psychostimulants were used on this occasion. Results were considered statistically significant at significance level of p < 0.05.
Results
In this study, body weight of 58 patients with ADHD (age: M = 13.17 years, standard deviation [SD] = 1.98, min = 8.36, max = 16.51) was evaluated and compared with weight of 62 children and adolescent from the control group (M = 13.70 years, SD = 2.0, min = 9.44, max = 1 7.04).
Boys constituted 79.3% of the study group (46 out of 58 patients) and 83.9% of the control group (46 out of 62 persons). Forty-one patients (70.7%) from the study group (35 boys, 6 girls) had combined subtype of ADHD, 16 (27.6%) (10 boys, 6 girls) predominantly inattentive subtype, and 1 (1.7%) boy had predominantly hyperactive impulsive subtype. In 43 (74.1%) patients, at least one comorbid condition was diagnosed. The most common were oppositional defiant disorder (n = 30, 51.7%). Specific developmental disorders of scholastic skills were found in 21 patients (36.2%), tic disorder in 2 (3.4%) patients, and conduct disorders in 1 patient (1.7%). The Subjective SES measured using Polish adaptation of MacArthur ladder did not reveal any substantial differences between the Control (M = 5.95, SD = 1.39) and ADHD (M = 5.76, SD = 1.46) group, t (109.03) = 0.71, p = 0.482, d = 0.13. Across the compared groups, there were also no significant differences in the distribution of education level of both mothers and fathers of the subjects.
Most of the respondents received medication (n = 53, 91.4%, including 42 boys). The most frequently used was methylphenidate (MPH) OROS (74.1% of the sample) and SR (17.2% of the sample). The average daily dose of MPH OROS was 36.8 mg/day (min 18 mg/day, max 54 mg/day), MPH SR 27.0 mg/day (min 10 mg/day, max 50 mg/day). Adjusted for a holiday break, the duration of pharmacological treatment for OROS MPH was on average 1096.9 days (min = 73 days, max = 2777 days), MPH SR average 1188 days (min = 583 days, max = 2139 days) (Table 1).
Dosage of Metylphenidate in Attention-Deficit/Hyperactivity Disorder Patients, Adjusted Treatment Duration, and Cumulated Dose of Pharmacological Treatment
OROS, osmotic release oral system; SR, sustained-release; SD, standard deviation.
The z scores for height, body weight, and BMI
Height, weight, and BMI were standardized for age and sex based on Polish growth charts (Palczewska et al. 2000; Kułaga et al. 2011). Standardized mean values of height (zH—z score for height), weight (zW—z-scores for weight), and BMI (zBMI-z-scores for BMI) are shown in Table 2. There were no differences between the sample and the control group in these variables, independent of the type of growth charts applied. Separate analysis across sexes revealed that in case of the girls mean values of zW were statistically significantly lower in girls with ADHD according to Kułaga et al. (2011) standards (ADHD vs. Control: −0.17 vs. 0.47, p = 0.04) and according to Palczewska et al. (2000) standards (ADHD vs. Control: −0.14 vs. 0.62, p = 0.04) (Tables 3 and 4).
Standardized Mean Values of Height (zH), Weight (zW), and Body Mass Index (zBMI) in Attention-Deficit/Hyperactivity Disorder Patients and Control Group
t-Test.
ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation; BMI, body mass index.
Standardized Mean Values of Height (zH), Weight (zW), and Body Mass Index (zBMI) in Boys with Attention-Deficit/Hyperactivity Disorder and from the Control Group
ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation; BMI, body mass index.
Standardized Mean Values of Height (zH), Weight (zW), and Body Mass Index (zBMI) in Girls with Attention-Deficit/Hyperactivity Disorder and from the Control Group
Bold values indicate the significance of the result at the level of p < 0.05.
ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation; BMI, body mass index.
The relationships between standardized values and the age was assessed in both groups. Statistically significant, small negative correlation was found only between height and the age of ADHD patients according to Palczewska et al. (2000) standards. (r = −0.26, r 2 = 0.07, p = 0.04) (Table 5; Fig. 1).
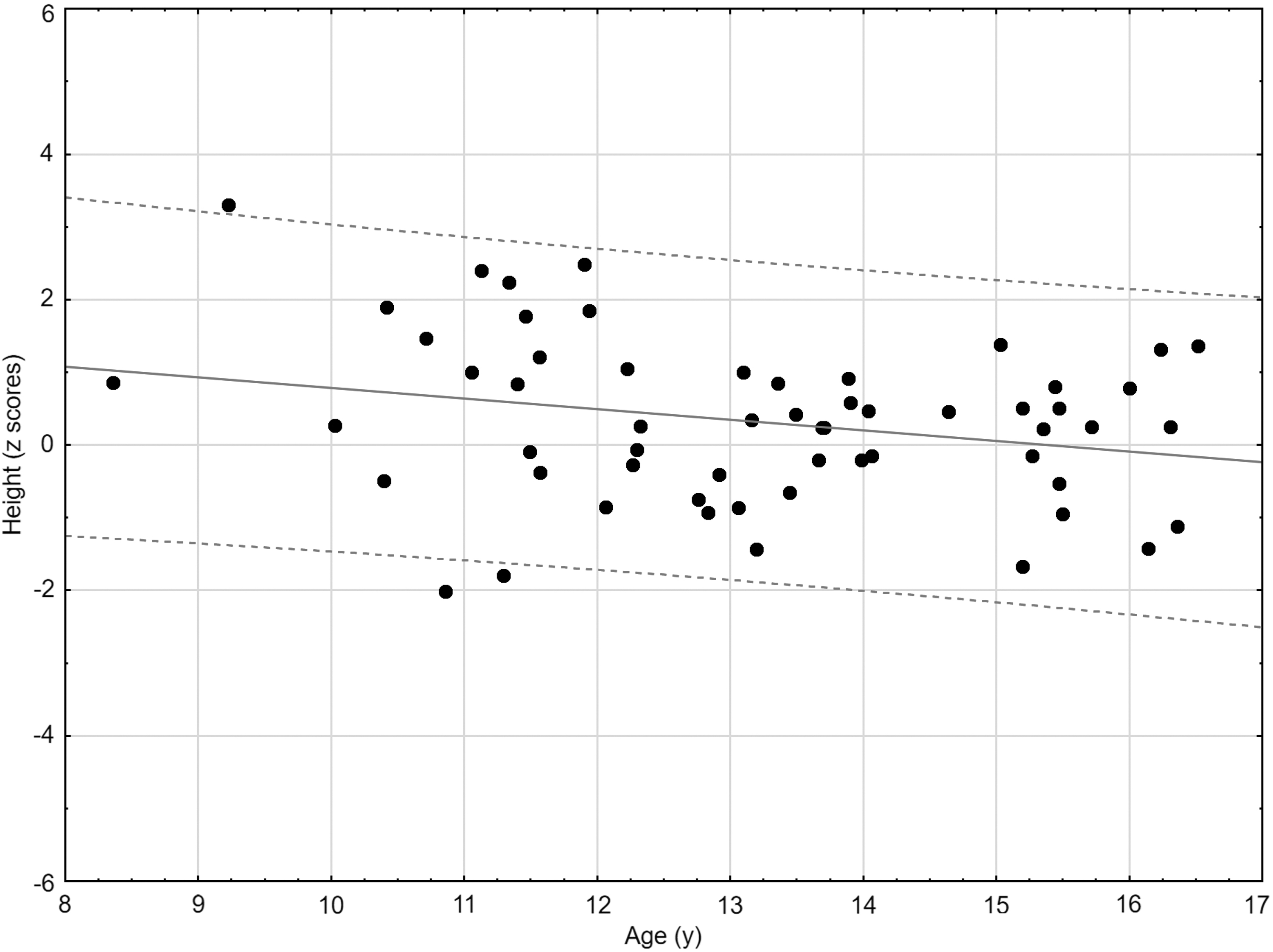
Correlation between standardized values of height and age in attention-deficit/hyperactivity disorder patients according to Palczewska et al. (2000) standards.
Bold values indicate the significance of the result at the level of p < 0.05.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index.
Occurrence of overweight and obesity
According to WHO/CDC criteria, there was a significantly higher incidence of overweight in the control group (ADHD vs. Control: 12.1% vs. 29.0%, p = 0.02). The difference remained statistically significant for the girls' subgroup (0.0% vs. 30.0%, p = 0.04). Nevertheless, there was a significantly higher incidence of obesity in the ADHD group (ADHD vs. Control: 17.2% vs. 3.2%, p = 0.01). The difference remained statistically significant for the boys' subgroup (19.6% vs. 3.9%, p = 0.01). Similarly, according to IOTF criteria, there was a significantly higher incidence of obesity in the ADHD group (ADHD vs. Control: 10.3% vs. 1.6%, p = 0.04). Again, the difference remained statistically significant for the boys' subgroup (13.0% vs. 1.9%, p = 0.01). There were no statistically significant differences in the incidence of overweight in ADHD and control group according to IOTF criteria, as well as the occurrence of overweight and obesity in ADHD and control group according to ECOG criteria (Table 6).
Occurrence of Overweight and Obesity in Attention-Deficit/Hyperactivity Disorder Patients and the Control Group (according to ECOG, WHO/CDC, and IOTF criteria)
Bold values indicate the significance of the result at the level of p < 0.05.
IOTF, International Obesity Task-Force; WHO, World Health Organization; ECOG, European Childhood Obesity Group; CDC, Center of Disease Control; ADHD, attention-deficit/hyperactivity disorder.
The occurrence of overweight and obesity in the ADHD group and the general population was compared. The analyses were carried out only using the IOTF criteria since the current assessment of overweight and obesity prevalence in the population of Polish children and adolescents was made according to these criteria (Kułaga et al. 2011). In the ADHD group, overweight (20.7% vs. 12.8%, p < 0.001), obesity (10.3% vs. 3.5%, p < 0.001), and overweight/obesity (31.0% vs. 16.3%, p < 0.001) were present significantly more often than in the general Polish population of children and adolescents. Besides, there was a significantly higher incidence of overweight (23.9% vs. 14.5%, p < 0.001), obesity (13.0% vs. 4.3% p < 0.001), and overweight/obesity (31.0% vs. 16.3%, p < 0.001) in the group of ADHD boys compared to the Polish population of children and adolescents. At the same time, there was a significantly lower incidence of overweight (8.3% vs. 11.4%, p = 0.02) and overweight/obesity (8.3% vs. 14.0%, p < 0.001) in a group of ADHD girls when compared to the population data (Table 7).
Occurrence of Overweight and Obesity According to International Obesity Task-Force Criteria: Attention-Deficit/Hyperactivity Disorder Group Versus Population
ADHD, attention-deficit/hyperactivity disorder.
An impact of stimulant treatment on growth characteristics and overweight/obesity rate
The cumulative dose of psychostimulants was assessed and its quartiles were determined as described in methods (cumulated dose: M = 39839.88, SD = 27096.01, min = 898.00, max = 106488.0, Lower quartile = 19584.00, Upper quartile = 52758.00). As we have found a negative correlation between zH and age, we also provided an estimation of correlation coefficients for age and treatment duration and cumulative dose of stimulants (r = 0.438, p = 0.001 and r = 0.482, p < 0.001, respectively).
Logistic regression was used to evaluate the impact of the cumulated dose of psychostimulants on the risk of overweight and obesity in the study group. The analysis did not show a statistically significant relationship between the amount of taken psychostimulant and the occurrence of overweight (OR = 0.951, ±95CI: 0.511–1.770, p = 0.971), obesity (OR = 0.671, ±95CI: 0.264–1.704, p = 0.389), and overweight/obesity (OR = 0.822, ±95CI: 0.470–1.437, p = 0.481) diagnosed with IOTF criteria.
Discussion
This study aimed to assess the prevalence of overweight and obesity in the group of children and adolescents with attention deficit hyperactivity disorder according to three different sets of diagnostic criteria. We hypothesized that the results will differ according to the used criteria and the prevalence of overweight and obesity in the study group will be higher than in the control group and in the general population.
Anthropometric measurements
Regardless of the standardization method used in the analyses (Palczewska et al. 2000; Kułaga et al. 2011), differences in the mean standardized values of height, body mass, and BMI between the ADHD patients and the control group were not statistically significant. This observation concerns both the whole group and the group of evaluated boys, whereas in the case of girls with ADHD subgroup, mean values of zW were significantly lower according to both Kułaga et al. (2011) and Palczewska et al. (2000) standards.
There were no statistically significant associations of body mass and BMI with the age of the respondents, which suggest that age does not significantly affect this association.
Presence of overweight and obesity in ADHD—differences related to the variability of diagnostic criteria
Previous studies on obesity has shown the discrepant estimates of obesity and overweight depending on used classification (Kain et al. 2002; Wickramasinghe et al. 2005).
To directly adress the consequences of heterogeneity of diagnostic criteria, we assessed the occurrence of overweight and obesity using criteria of IOTF, WHO/CDC, and ECOG. After applying the 90th percentile as the cutoff point for overweight and 97th percentile for obesity, no statistically significant differences were found in the occurrence of overweight and obesity between the ADHD and the control group, regardless of sex. These criteria were not previously used for the study of ADHD-diagnosed groups compared to the control group, however, they were used in population studies, with no consistent pattern of results [see: Erhart et al. (2012) and Rojo et al. (2006)]. When the WHO/CDC criteria were used to diagnose overweight, taking the 85th percentile as the cutoff point, a higher incidence of overweight was found in the control group. When sex was controlled, a significantly lower body weight was demonstrated in the group of girls [both when Palczewska et al. (2000) and Kułaga et al. (2011) standards were used]. This could be explained by the fact that 11 out of 12 girls in the study group received pharmacological treatment. Population data obtained in the the United States of America (Waring and Lapane 2008) suggest that children with ADHD receiving pharmacotherapy have ∼1.6 higher odds of being underweight. In turn, Erhart et al. (2012) report that ADHD symptoms are common not only in overweight and obesity but also in underweight.
On the contrary, the frequency of obesity diagnosed according to the WHO/CDC criteria (95 percentile value as the cutoff point) was higher in the group of patients with ADHD. When sex was controlled, the difference remained statistically significant only for the group of boys. A similar method of obesity diagnosis was used by Dubnov-Raz et al. (2011) and Güngör et al. (2016), but again the results of these studies are not consistent. In the Dubnov-Raz et al. (2011) study, based on the analysis of medical charts, the prevalence of overweight and obesity in 275 patients with ADHD was lower than in the control group. In contrast, in the study of Gungor et al. (2016), which included a group of 362 patients with ADHD, a higher incidence of overweight and obesity was demonstrated in the ADHD group.
Application of the IOTF criteria gave similar results to the WHO/CDC criteria in terms of overall pattern of results. Significant differences were found only in the obesity rate. It was more frequent in the group of patients with ADHD than in the control group. When sex was controlled, the difference again remained statistically significant only for the group of boys. Similar results were obtained in our previous study based on the same diagnostic criteria (Racicka et al. 2018).
This effect contrasts with the results reported by Hanć et al. (2015), who used the same criteria in a comparison of 219 boys with ADHD and 396 boys from the control group, showed the relationship between ADHD and higher prevalence of overweight, but not obesity.
Presence of overweight and obesity in ADHD in comparison to population
Overweight, obesity, and overweight/obesity in the examined group of patients with ADHD were significantly more frequent in comparison with the Polish population of children and adolescents. When sex was controlled, the difference remained statistically significant only for the group of boys. In turn, in the group of girls, there was a lower incidence of overweight, obesity, and overweight/obesity in the group of girls with ADHD in comparison with the population of Polish girls.
Fliers et al. (2013) compared the prevalence of overweight and obesity in a group of 372 patients with a mixed subtype of ADHD aged 5–17 years with the population. A significantly more frequent occurrence of overweight was found in particular age-subgroups of boys compared to the population, while the difference in the occurrence of obesity, although higher in the group of ADHD boys, was not statistically significant. In turn, in the group of girls, a pronounced influence of age was found—in the girls aged 10–12 years was characterized by higher standardized body weight, higher prevalence of overweight, and four-fold increase in the risk of obesity. Interestingly, when the authors of the study applied the WHO/CDC criteria, the occurrence of overweight and obesity was several-dozen times higher in ADHD, especially in the group of boys.
Previous meta-analysis showed that the strength of association between ADHD and obesity may be moderated by age (Cortese et al. 2013) with strongest effects observed in adults. Other work (Nigg et al. 2016) showed a lack of statistically significant association between ADHD and the occurrence of overweight/obesity in children, but a possible relationship in adolescent girls, suggesting specific role of sex in this association. There are also data indicating that tendency to overweight may be observed in boys in school age (children and adolescents) but not in preschoolers (Hanć et al. 2015). These results, among others, underline the necessity of controlling both age and sex of participants. Our sample included both girls and boys in wide range of age from 8.36 to 16.51 years. Nevertheless, the analysis of correlation of age- and sex-adjusted z scores weight and BMI with age of patients gave insignificant results. We have not collected data on pubertal development, therefore a detailed analysis of the differences in body size between prepubertal, pubertal, and postpubertal girls and boys was not possible.
Summarizing, our restuls are coherent with the previous publications underlining the importance of sex as a key variable moderating the relationship between ADHD diagnosis and overweight and obesity.
The impact of pharmacological treatment
Ninety-one percent of the study group was treated pharmacologically, while 8.6% did not use pharmacotherapy. The percentage of treated children and adolescents is similar to the values described in the 10-year Biederman et al. (2008) observational study (93% of patients treated pharmacologically). The most common pharmacological treatment was psychostimulant therapy, which is consistent with guidelines of the American Academy of Child and Adolescent Psychiatry (Pliszka 2007) as well as British standards of National Institute for Health and Care Excellence) (Kendall et al. 2008).
Additional analysis has shown that the age was positively correlated with the cumulative dose of psychostimulants. The relationship between age and height could be mediated by the suppressive effects of persistent stimulant treatment on growth. Such effects were reported in the most recent study from the Multimodal Treatment of ADHD Study (Greenhill et al. 2019). This rises the question about the potential effects of stimulants on BMI and overweight/obesity rates, however, such effects were not revealed in our study. We did not find a correlation between age or cumulative dose of stimulants and z scores for weight or BMI. The cumulative dose of stimulants also was not related to the decrease or increase of overweight and obesity rates. This result is consistent with Castaneda et al. (2016) study that failed to show a statistically significant relationship between the amount of drugs taken and the occurrence of overweight or obesity until early adulthood. On the contrary, current results contrast with our own observations from the previous study, in which treatment with OROS MPH was associated with a higher incidence of obesity (Racicka et al. 2018).
These disparities are most likely the result of the different inclusion criteria for the study group and differences in the treatment protocols. Our previous study based on the analysis of medical charts from 1996 to 2010 and ADHD group included patients with comorbid diagnoses potentially affecting the body weight. Moreover, previously patients received different pharmacological treatments. Less than 10% of people in the previous study received imipramine and 14.95% short-acting psychostimulants, which could affect the body weight. None of the patients in the present study received such treatment. It is possible that decreased impulsivity and improvement in executive functions, which are more substantial while using long-acting psychostimulants compared to imipramine, caused better adherence to a healthy diet. Moreover, the use of long-acting psychostimulant could also contribute to better dietary compliance due to the longer duration of their action during the day compared to short-acting psychostimulants. Better functioning during the day could also cause less stress, which may lead to emotional eating, espcecially high-calorie food (Ulrich-Lai et al. 2015).
Limitation of the study
The most important limitation of the study is related to the potential bias introduced by the fact that the ADHD group consisted only from the patients diagnosed and treated in the outpatient clinic. This aspect of the study might affect the generalizabiliy of the results. It is also important to notice that small sample size and limited number of patients with inattentive and hyperactive/impulsive ADHD subtypes narrowed the analytical possibilities and did not allow us to use multivariate statistical models that could provide, much needed, insights concerning the interplay of age, sex, and ADHD subtype on the observed effects.
Also, our study did not control and take into account other variables that may affect body weight, such as diet, eating habits, lifestyle, level of physical activity, and sleep disturbance. Further research, based on larger samples, should certainly address these issues using more complex analytical approaches.
Conclusions
The prevalence of overweight and obesity in the group of children and adolescents with ADHD varies according to used criteria for overweight and obesity. At the same time, the occurrence of obesity diagnosed according to IOTF and WHO/CDC criteria is significantly more frequent in the group of children and adolescents with ADHD, especially in the group of boys, in comparison with people from the control group matched in terms of sex and age.
It is important to understand that the IOTF reference standard and the CDC norms, as well as ECOG criteria, do not produce the same outcomes in terms of both estimating the prevalence of underweight, overweight, and obesity among children, as well as revealing more complex patterns involving participant sex. This discrepancy stems from dissimilarities in methodologies used to determine cutoff criteria, as well as the complexity of the studied relationships. It is also important to underline that diagnostic standards have been constructed based on different populations. Hence, the result for patients with the same disorder but from different populations (e.g., Poland vs. United States of America) may vary.
Thus, we suggest that future studies carried out to estimate body weight disorders among children with ADHD should give a clear rationale for the choice of cutoff points. Further research efforts in this field could significantly benefit from increasing the coherence of diagnostic and reporting standards. Lack of reporting clarity might confound data analysis and interpretation, and consequently lead to questioning of the reliability and validity of both the estimates and obtained findings.
Clinical Significance
To our knowledge, this is the first study regarding the relationship between overweight/obesity and ADHD, in which we used three different, the most popular criteria for the diagnosis of obesity. This resulted in discrepant estimates of obesity and overweight, which should be taken into consideration in future studies on this topic. Moreover, as in previous studies, obesity in children and adolescents with ADHD occurred to be more frequent than in general population, thus clinicians should focus on prevention and guidelines for treatment of this somatic comorbidity.
Footnotes
Disclosures
Dr. T.H. and Prof. T.W. have received travel support and speaker fee from MEDICE Arzneimittel Pütter GmbH and Co. KG. Dr. A.B. has received travel support from MEDICE Arzneimittel Pütter GmbH and Co. KG. Dr. E.R.-P. has received speaker fee from WCG PHARMA Sp. Z.o. and honorarium for educational materials from Qpharma Sp. z o.o. Other authors do not declare any conflicts of interests.