
Abstract
Objective:
To systematically review the impact of CYP2D6 genetic variation on antipsychotic pharmacokinetics, efficacy, and adverse drug reactions among children and youth.
Method:
The published literature was systematically searched in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations and critically evaluated using standardized tools and consensus criteria.
Results:
A total of 20 eligible studies comprising 1078 children and youth were evaluated. The included studies were of fair to moderate quality and included mostly males, individuals of European ancestry, and those treated with risperidone. CYP2D6 poor metabolizers (PMs) were consistently shown to have increased concentrations of risperidone relative to normal metabolizers (NMs). PMs were also consistently shown to have a greater propensity to experience antipsychotic (primarily risperidone) associated adverse drug reactions relative to NMs. However, robust evidence for an association between CYP2D6 and efficacy was less apparent.
Conclusion and Clinical Significance:
The current knowledge base suggests that CYP2D6 genetic variation has an appreciable impact on antipsychotic pharmacokinetics and the propensity for adverse drug reactions, particularly among children receiving risperidone treatment. However, several limitations with the current literature (e.g., sample sizes, study design, sample heterogeneity) should be addressed in future studies. Assuming that future studies support the link between CYP2D6 genetic variation and antipsychotic outcomes, we would anticipate an increase in the implementation of CYP2D6-guided antipsychotic drug selection and dose optimization in child and adolescent psychiatric services.
Introduction
Antipsychotics are used to treat psychotic symptoms (e.g., hallucinations) and disruptive behaviors (e.g., aggression) in children and youth with severe mental health and neurodevelopmental disorders (e.g., schizophrenia, autism spectrum disorders [ASDs]). The Food and Drug Administration (FDA) has approved several antipsychotics for use in children and youth. Risperidone, olanzapine, quetiapine, and aripiprazole are approved for manic or mixed bipolar I disorder (ages 10–17 years) and schizophrenia (ages 13–17 years). Risperidone (ages 5–16 years) and aripiprazole (ages 6–17 years) are also approved for the treatment of irritability and aggression in children with ASDs (Penfold et al. 2013). Paliperidone is approved for the treatment of schizophrenia in adolescents aged 12–17 years, and asenapine (10 years and older) is approved for the treatment of bipolar disorder. Pimozide is approved for treatment of Tourette's disorder in children 12 and older. However, antipsychotics are also commonly used in children and adolescents “off-label” (i.e., for indications not approved by a regulatory body or in children younger than the approved age ranges) (Harrison et al. 2012). Importantly, the on- and off-label use of antipsychotics has rapidly increased over the last 20 years (Baeza et al. 2014).
The increased use of antipsychotics in children and youth has been accompanied by reports of interindividual variation in efficacy and tolerability (Krause et al. 2018; Lee et al. 2018; Solmi et al. 2020) similar to that reported in adult populations (Leucht et al. 2013). This interindividual variation can be attributed to demographic (age, sex, ethnicity), clinical (e.g., renal function, concomitant medications), lifestyle (e.g., diet, smoking), and “omic” (e.g., genomic, microbiomic) factors. Among these many factors, the study of variation in genes that encode enzymes involved in antipsychotic metabolism has emerged as a promising avenue for understanding interindividual variability in antipsychotic treatment efficacy and tolerability (Pouget et al. 2014; Yoshida and Müller 2019).
Most antipsychotics undergo hepatic metabolism by one or more cytochrome P450 (CYP) drug-metabolizing enzymes. Among these enzymes, CYP2D6 is of particular importance given its involvement in the primary metabolism of several antipsychotics (e.g., chlorpromazine, fluphenazine, haloperidol, loxapine, perphenazine, thioridazine, zuclopenthixol, risperidone, aripiprazole, iloperidone, and paliperidone), as well as making a contribution to the metabolism of olanzapine and clozapine (Ravyn et al. 2013).
CYP2D6 is highly polymorphic and its genetic variants can be used to predict an individual's CYP2D6 enzyme activity (i.e., CYP2D6 phenotype). The most widely used CYP2D6 metabolizer phenotype classification system includes: ultrarapid metabolizers (UMs), normal metabolizers (NMs), intermediate metabolizers (IMs), and poor metabolizers (PMs) (Caudle et al. 2020). CYP2D6 metabolizer phenotypes are determined by genotyping sets (haplotypes) of genetic variants, known as star (*) alleles. Each individual has two star alleles that are collectively referred to as a diplotype or genotype (e.g., *1/*5). Each star allele is then assigned a function (i.e., no, decreased, normal, or increased) and a corresponding numerical activity level (0 = no, 0.25–0.50 = reduced, 1 = normal, 2+ = increased). The activity levels for the two alleles are then summed to derive an activity score (AS), which is translated into a metabolizer phenotype (i.e., poor = AS = 0; intermediate = 0 < AS <1.25; normal = 1.25 ≤ AS ≤2.25; ultrarapid = AS >2.25).
For example, an individual with a CYP2D6 *1/*5 genotype carries one normal (*1) and one no (*5) function allele. The *1 allele has an activity level of 1 and the *5 has an activity level of 0. Summing the levels results in an AS of 1, which translates to an IM phenotype.
To date, eight antipsychotics have FDA product labels (aripiprazole, brexpiprazole, clozapine, iloperidone, pimozide, and thioridazine) (FDA 2020) and/or prescribing guidelines (aripiprazole, haloperidol, pimozide, and zuclopenthixol) (Swen et al. 2008) that offer drug selection or dosing recommendations based on CYP2D6 genotype-predicted phenotypes. However, these product labels and guidelines are primarily based on studies conducted in adult populations, which have raised questions about the appropriateness of extrapolation to the child and youth population.
To aid efforts to address the question of appropriateness, we conducted a systematic review of the current state of knowledge regarding CYP2D6 genetic variation and antipsychotic treatment outcomes (i.e., pharmacokinetics, clinical efficacy, and adverse drug reactions) in children and youth. We are aware of one previous systematic review that specifically examined CYP2D6 and risperidone treatment in children and adolescents (Dodsworth et al. 2018). However, as stated above, CYP2D6 is involved in the metabolism of several antipsychotic drugs. As such, we reviewed the full spectrum of published literature related to CYP2D6 genetic variation and antipsychotic treatment in child and youth populations.
Method
Search strategy
The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Liberati et al. 2009) recommendations and registered with PROSPERO (CRD42020166966). Two reviewers (A.A.M. and K.S.) independently searched PubMed, MEDLINE, PsycINFO, Google Scholar, and EMBASE. All database searches were limited to published articles written in English up to January 5, 2020. The search strategy used on PubMed was: ((((adolescent OR child OR children OR pediatric OR paediatric or youth) AND (antipsycho* OR psychotropic OR neuroleptic) AND (cytochrome P450 2D6 OR CYP2D6) AND (pharmacog* OR allele OR genotype* OR metaboli*)))). Similar strategies were used for other databases.
The articles were selected through a two-phase review process. In the first phase, both reviewers independently assessed the titles and abstracts of all articles identified by the search strategies for eligibility. In the second phase, the full-text copies of articles which met the inclusion criteria in the first phase were assessed to ensure consistency with the eligibility criteria. Bibliographies of all research articles and review articles were hand-searched for additional references not identified in the primary searches. Articles for which a consensus between the two reviewers was not obtained were assessed by a third reviewer (C.B.). The articles that met the inclusion criteria were then selected for data extraction.
Study selection criteria
Inclusion criteria for data extraction were: (1) children and youth (aged <25 years as per the United Nations definition) (United Nations 2020) treated with an antipsychotic; (2) CYP2D6 genotyping was conducted, and the results relating CYP2D6 variants and treatment outcomes were reported; and (3) the article was published in a peer-reviewed, English-language journal and the full-text was available. Review articles, commentaries, books, book chapters, editorial pieces, or any published material not deemed original research was excluded. Extracted information included database ID, first author name, publication year, study title, subject characteristics, study site, study design, sample size, diagnosis studied, drugs used, the dose and duration of use, CYP2D6 variants studied, other genes studied, phenotypes investigated, how and what outcomes were measured, and main findings.
Quality assessment
An assessment of study quality was conducted independently by the two reviewers (A.A.M. and K.S.) based on a quality assessment tool adapted from the checklist developed by Jorgensen and Williamson (2008) for assessing the methodological quality of pharmacogenetic studies. The tool consisted of 26 questions covering seven issues of concern (i.e., gene/variant selection, sample size, genotyping reliability, missing data, population stratification, Hardy–Weinberg equilibrium, and choice of outcomes). For each of the questions included in the quality assessment tool, a “Yes” was recorded if the study definitively and affirmatively addressed the question, else a “No” for the question was recorded. The number of “yes” responses was summed to derive a quality score (range 0–26) for each included study, where higher scores suggest a higher quality study. To our knowledge, thresholds for classifying low-, moderate-, or high-quality studies using this tool have not been published.
Results
Study selection
The PRISMA flowchart summarizing the article selection process is provided in Figure 1. A total of 238 articles were identified through database searching. Hand searches of the bibliographies of these articles identified an additional 27 articles, resulting in a total of 263 articles after duplicates were removed. After reviewing titles and abstracts, 231 articles were excluded that did not meet the inclusion criteria for data extraction. The full text of the remaining 32 articles was reviewed and assessed for eligibility, of which 12 articles were further excluded for not meeting the inclusion criteria, resulting in a final 20 articles for data extraction and quality assessment that included 1078 children and youth.
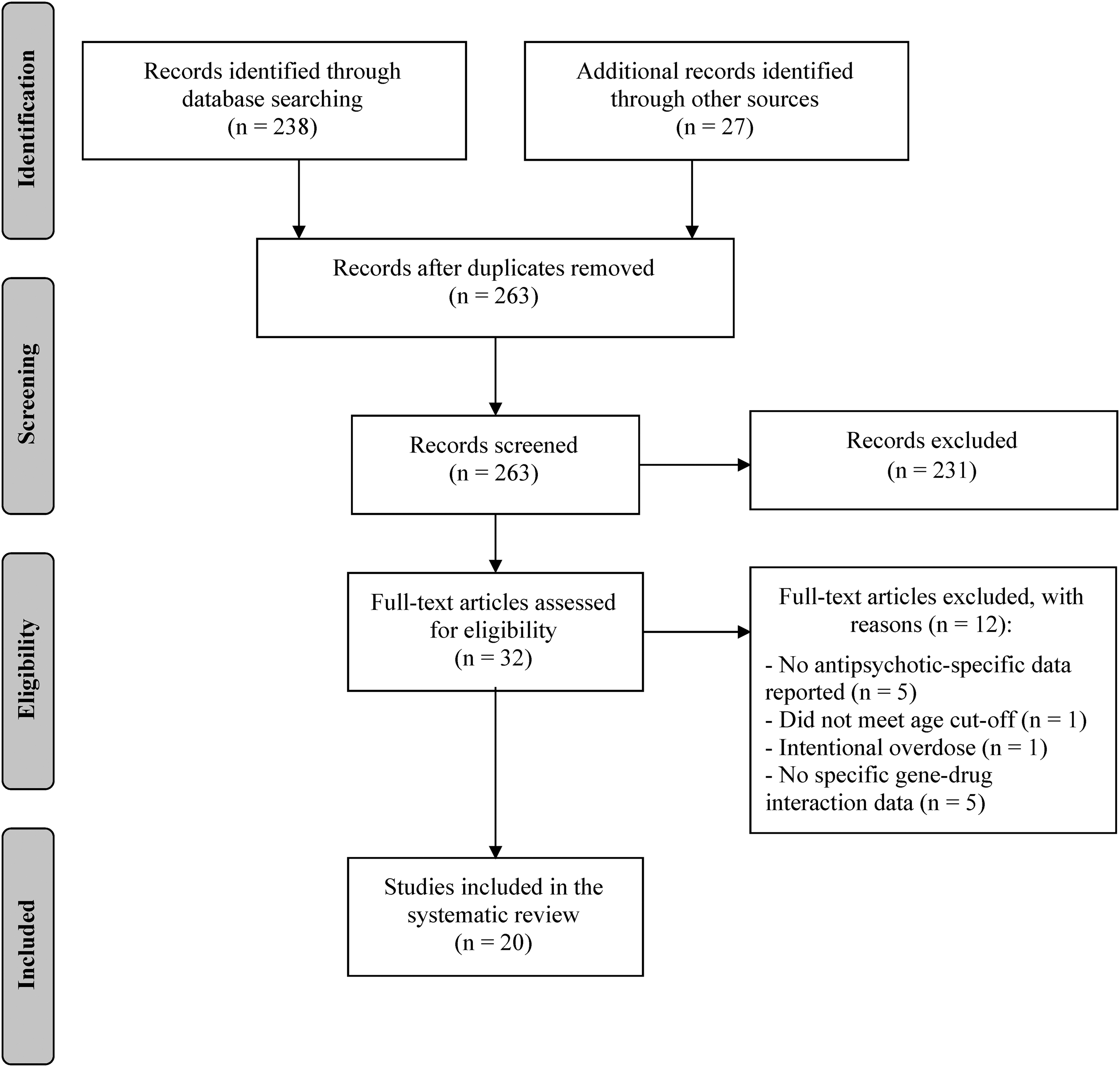
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart detailing the article selection process.
Characteristics of included studies
An overview of the characteristics of the included studies is presented in Table 1. The majority of the included studies were retrospective studies with sample sizes ranging from a single case to 257 patients. The individuals studied were primarily male (54%–100%) and of European background. The age of patients ranged from 3 to 21 years old. The most studied antipsychotic was risperidone (19 out of 20 studies) followed by aripiprazole (4 out of 20 studies), olanzapine (3 out of 20 studies), haloperidol (3 out of 20 studies), and levomepromazine (2 out of 20 studies).
Characteristics of Studies (n = 20) Included in the Systematic Review on Antipsychotic Pharmacogenetics in Children and Youth
The quality score ranges from 0 to 26 with higher scores representing higher quality. See Supplementary Table S1 for detailed information on the specific quality metrics for each study.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; BPD, borderline personality disorder; CNV, CYP2D6 copy number variations (Xn); DBD, disruptive behavior disorder; Dup, CYP2D6 duplications; ID, intellectual disability; ODD, oppositional defiant disorder; PDD-NOS, pervasive developmental disorder, not otherwise specified; PTSD, posttraumatic stress disorder; SD, standard deviation; IQR, interquartile range; PM, poor metabolizer; NM, normal metabolizer; UM, ultrarapid metabolizer; IM, intermediate metabolizer; n/a, not available.
The CYP2D6 gene variants tested varied from study to study (Fig. 2). Variants tested in 50% or more of the studies included *4 (90%), *5 (75%), gene duplications (55%), *3 (50%), *6 (50%), *10 (50%), and *41 (50%). In addition to CYP2D6, seven of the studies genotyped variants in other genes, including ABCB1 (Nuntamool et al. 2007; Corriea et al. 2010; Rafaniello et al. 2018; Sukasem et al. 2018), ABCG2 (Rafaniello et al. 2018), BDNF (Corriea et al. 2010; Sukasem et al. 2018), CYP3A4 (Rafaniello et al. 2018), CYP3A5 (Rafaniello et al. 2018), DRD2 (Nuntamool et al. 2007; Corriea et al. 2010; dos Santos Júnior et al. 2015, 2016; Sukasem et al. 2016, 2018), DRD3 (Nuntamool et al. 2007; Corriea et al. 2010), GHRL (Sukasem et al. 2018), HTR2A (Nuntamool et al. 2007; Corriea et al. 2010), HTR2C (Corriea et al. 2010; dos Santos Júnior et al. 2015, 2016), HTR6 (Corriea et al. 2010), LEP (dos Santos Júnior et al. 2015, 2016; Sukasem et al. 2018), LEPR (dos Santos Júnior et al. 2015, 2016), MC4R (dos Santos Júnior et al. 2015, 2016), and SCARB2 (dos Santos Júnior et al. 2015, 2016).

CYP2D6 alleles tested in the 20 studies reviewed. One or more studies tested for alleles with normal function (*2, *2A, *33, *35, *46); no function (*3, *4, *5, *6, *6C, *7, *8, *11, *12, *14A, *14B, *15, *18, *19, *20, *40, *42); decreased function (*3B, *9, *10, *14, *17, *29, *41); increased function (duplications); or unknown function (*52).
Notably, no study to our knowledge used CYP2D6 genotyping to guide medication selection or dosing. No studies reported sponsorship by a pharmacogenetic testing company, used a commercial pharmacogenetic testing company's panel, nor did any of the authors report relationships with such companies.
Quality assessment of included studies
Based on a quality assessment tool (Supplementary Table S1) that we adapted from Jorgensen and Williamson (2008), none of the studies met all of the quality criteria. The most common concerns were related to study design or omissions in the reporting of study methodology (Supplementary Table S1). Areas of particular concern across the reviewed studies included: missing methods to adjust for multiple testing (100% of studies), no description of how missing genotype data were handled (100%), no description on how population stratification was assessed and addressed (100%), missing sample size justification (95%), missing genotyping quality control methods (90%), and failure to report precise p-values (40%). The average quality score was 9.8 (standard deviation = 1.4, range = 7–12). Therefore, on average the studies met 38% of the 26 quality criteria.
CYP2D6 and antipsychotic pharmacokinetics
The impact of CYP2D6 genotypes or predicted metabolizer phenotypes on antipsychotic pharmacokinetic parameters was examined in 10 out of the 20 reviewed studies (Table 2). All 10 studies examined blood concentrations of risperidone, its primary metabolite 9-hydroxyrisperidone (9-OH-risperidone), active moiety (risperidone +9-OH-risperidone), and/or risperidone/9-OH-risperidone ratios. Aripiprazole and haloperidol were examined in one study each. Nine of the 10 studies reported a significant association between CYP2D6 genotypes or predicted metabolizer phenotypes and risperidone and/or 9-OH-risperidone concentrations. The single studies of CYP2D6 and aripiprazole or haloperidol concentrations were negative.
Summary of Studies Examining the Impact of CYP2D6 on Antipsychotic Pharmacokinetics in Children and Youth
Active moiety, the sum of risperidone and 9-OH-risperidone concentrations.
9-OH-resperidone, 9-hydroxyresperidone; IM, intermediate metabolizer; NM, normal metabolizer; PM, poor metabolizer; UM, ultrarapid metabolizer.
The potential link between CYP2D6 and risperidone pharmacokinetics in children/youth was first reported in a case published by Guzey et al. (2000) that described a 15-year-old male who failed to respond to risperidone and was later found to be a CYP2D6 UM (*2xN/*1) with an active moiety concentration (∼24 ng/mL) at the low end of the expected range (20–60 ng/mL) (Hiemke et al. 2018). That case was then supported by Köhnke et al. (2002), who reported risperidone-induced akathisia, parkinsonism, and drowsiness in a 17-year-old male with schizophrenia treated with risperidone. Genotyping showed that the boy was homozygous for the CYP2D6*4 allele (PM), and drug monitoring revealed an active moiety plasma concentration (60 ng/mL) at the high end of the expected range (20–60 ng/mL).
These initial published case reports were followed up by seven studies supporting the association between CYP2D6 and risperidone pharmacokinetic parameters. First, a prospective study of 25 children (including 5 PMs and 2 UMs) treated with risperidone showed that active moiety was lowest for PMs (mean = 15.8 ng/mL ±4.8 ng/mL) but both UMs had active moiety concentrations within the normal range (Troost et al. 2007). Then, in an independent prospective study of 28 children treated with risperidone, Sherwin et al. (2012) used population pharmacokinetic modeling to show that relative clearance of risperidone was higher for CYP2D6 IMs (29.2 L/h) and NMs (37.4 L/h) compared to PMs (9.38 L/h). In addition, Roke et al. (2013) examined risperidone and 9-OH-risperidone concentrations in 46 male children and showed that PMs had higher mean active moiety concentrations (36.5 ng/mL) compared to IMs (10.5 ng/mL), NMs (11.9 ng/mL), and UMs (3.5 ng/mL).
In contrast, Youngster et al. (2014) did not find a difference in active moiety concentrations between PMs, IMs/NMs, and UMs in 40 children treated with risperidone. They did, however, find significantly higher plasma risperidone concentrations (p = 0.03) and risperidone/9-OH-risperidone ratios (p = 0.02) in PMs compared to IMs/NMs. Furthermore, two cross-sectional studies conducted by Vanwong et al. (2016, 2017) examined the impact of CYP2D6 polymorphisms on plasma concentrations of risperidone and 9-OH-risperidone in Thai children and adolescents with ASD. In the first study of 84 patients (Vanwong et al. 2016), active moiety concentrations did not differ by CYP2D6 metabolizer status, although no PMs were included in this study. They did find that median plasma concentration of risperidone in IMs (1.85 ng/mL) was significantly higher than NMs (0.43 ng/mL, p < 0.0001), while the risperidone/9-OH-risperidone ratio in IMs (0.20) was found to be significantly higher than NMs (0.05, p < 0.0001) and UMs (0.00, p = 0.02). In the second study of 97 patients (Vanwong et al. 2017), there was also no association between CYP2D6 metabolizer status and active moiety concentrations, although no PMs or UMs were included in the study. However, they did report that median plasma concentrations of risperidone for individuals with *5/*10 (4.34 ng/mL, p = 0.02), *10/*41 (2.24 ng/mL, p = 0.04), or *10/*10 (1.85 ng/mL, p = 0.04) genotypes, but not the *4/*10 (0.65 ng/mL, p = 0.60) genotype, were significantly higher than *1/*1 (0.26 ng/mL) carriers.
Similarly, Nuntamool et al. (2017) showed in 82 Thai children and adolescents that active moiety concentrations did not differ by CYP2D6 genotype-predicted ASs, but they were negatively correlated with plasma risperidone concentration (p = 0.019) and risperidone/9-OH-risperidone ratios (p = 0.041). Finally, Rafaniello et al. (2018) measured plasma risperidone concentrations in 64 children of European ancestry treated with risperidone and found no association between CYP2D6 phenotypes (NM, IM, PM, UM) and risperidone plasma concentrations.
CYP2D6 and antipsychotic efficacy
Five studies examined clinical response to antipsychotics in relation to CYP2D6 genotypes or predicted metabolizer phenotypes (Table 3). All studies included risperidone and one study also included patients taking multiple antipsychotics, such as the CYP2D6 substrates haloperidol, levomepromazine, aripiprazole, quetiapine, and pimozide. Among these five studies, only one case study and a case series of nine patients suggested an association between CYP2D6 and antipsychotic clinical response. Guzey et al. (2000) showed that a 15-year-old boy who failed to respond to risperidone was identified as a CYP2D6 UM, and Thümmler et al. (2018) genotyped nine children with multiple failed trials of antipsychotics and found that five (55%) were CYP2D6 PMs or UMs. However, three other studies included in our review did not support these preliminary findings.
Summary of Studies Examining the Impact of CYP2D6 on Antipsychotic Efficacy in Children and Youth
Measured with Autism Treatment Evaluation Checklist (ATEC).
Defined as multiple failed responses to psychotropic medications and polypharmacy.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; BD, behavioral disorder; BPD, borderline personality disorder; COS, childhood onset schizophrenia; ID, intellectual disability; ODD, oppositional defiant disorder; PDD-NOS, pervasive developmental disorder-not otherwise specified; PM, poor metabolizer; IM, intermediate metabolizer; PTSD, posttraumatic stress disorder; UM, ultrarapid metabolizer.
Correia et al. (2010) measured clinical symptom improvements in 45 risperidone treated children with ASD using the Autism Treatment Evaluation Checklist, the parent version of the Nisonger Child Behavior Rating Form, and the Behavior Problems Inventory. However, no significant associations between CYP2D6 phenotypes and clinical improvements were found. Likewise, Nuntamool et al. (2017) did not find an association between CYP2D6 genotype-predicted metabolizer status and ASD patients clinically rated as stable (n = 67) or nonstable (n = 15) based on the Clinical Global Impressions-Improvement scale score.
CYP2D6 and antipsychotic associated adverse drug reactions
Among the 20 included studies, 14 examined one or more antipsychotic associated adverse drug reactions (Table 4). The results from these studies were divided into four categories: (1) general side effect burden (n = 4); (2) hyperprolactinemia (n = 6); (3) metabolic syndrome (n = 4, e.g., weight gain, hypertension, dyslipidemia, insulin resistance); and (4) neurological (n = 2, e.g., extrapyramidal symptoms). Although dosing information was provided for the majority of the studies, only one study (Youngster et al. 2014) reported dosing by CYP2D6 metabolizer phenotypes and showed that PMs were given a lower median dose (0.65 mg/day) relative to NM/IMs (1 mg/day) and UMs (1.25 mg/day).
Summary of Studies Examining the Impact of CYP2D6 on Antipsychotic Associated Adverse Drug Reactions in Children and Youth
ADR, adverse drug reaction; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; IM, intermediate metabolizer; HOMA-IR, homeostatic model assessment of insulin resistance; NM, normal metabolizer; PM, poor metabolizer; UM, ultrarapid metabolizer.
General side effect burden
In a retrospective cohort study of 257 children and adolescents, Oshikoya et al. (2019) reported that PMs and IMs had a 2.4 (95% confidence interval 1.1–5.1, p = 0.03) greater odds of experiencing risperidone associated side effects compared to NMs and UMs after adjustment for age, sex, race, and the initial risperidone dose. In a case series, Thümmler et al. (2018) reported that only children with UM and PM genotype-predicted phenotypes experienced side effects (e.g., extrapyramidal syndrome, weight gain) following use of a CYP2D6 substrate (e.g., risperidone, aripiprazole). In contrast, Nuntamool et al. (2017) found no association between CYP2D6 metabolizer phenotypes and the development of any side effects in 82 Thai children being treated by risperidone. Similarly, Rafaniello et al. (2018) found no association between CYP2D6 metabolizer status and side effects in 90 patients treated with either aripiprazole or risperidone.
Hyperprolactinemia
One of the most common adverse effects of antipsychotic therapy is hyperprolactinemia (i.e., elevated prolactin levels) leading to gynecomastia in boys which has resulted in a class action against the manufacturer of risperidone (ClassAction 2017).
In a prospective study of 25 children treated with risperidone, Troost et al. (2007) reported that the number of CYP2D6 functional alleles positively correlated (p = 0.03) with prolactin levels, which was further corroborated by a strong positive correlation (r = 0.66, p = 0.001) between 9-OH-risperidone (but not risperidone) concentration and prolactin after 8 weeks of treatment, a finding previously reported in young adults (Knegtering et al. 2005). More recently, Grădinaru et al. (2019) investigated the impact of the CYP2D6 genotype-predicted phenotypes on prolactin levels over 18 months in 81 pediatric patients treated with risperidone, aripiprazole, or olanzapine. PMs and IMs showed significant increases in prolactin over the study period, while levels in the NMs remained stable.
In contrast, several other studies have failed to support an association between CYP2D6 metabolizer status and prolactin levels. A cross-sectional study by dos Santos Júnior et al. (2015), did not find a difference in CYP2D6 genotype-predicted phenotype frequencies among risperidone treated patients with (n = 79) and without (n = 41) hyperprolactinemia. Similarly, Roke et al. (2013), Sukasem et al. (2016), and Youngster et al. (2014) found no statistically significant association between CYP2D6 genotype-predicted phenotypes and prolactin concentrations in children and adolescents treated with risperidone. These results concur with a recent meta-analysis of seven studies (combined children and adult studies) that showed no association between CYP2D6 metabolizer status and hyperprolactinemia (Calafato et al. 2020).
Metabolic syndrome
Evidence suggests that higher concentrations of antipsychotics may trigger a cluster of conditions (e.g., weight gain, obesity, cardiovascular effects) commonly referred to as metabolic syndrome (Puangpetch et al. 2016). Aligned with this notion, Correia et al. (2010) reported that CYP2D6 UMs treated with risperidone had a lower propensity for increases in body mass index (BMI) and waist circumference compared to NMs. Furthermore, Nussbaum et al. (2014) reported that IMs (*1/*4) treated with aripiprazole, olanzapine, or risperidone had significantly greater increases in BMI and insulin levels over 18 months of treatment relative to their NM counterparts. In addition, dos Santos Júnior et al. (2016) reported in a cross-sectional study of 120 children and adolescents treated with risperidone that IMs (*10/*10) were heavier and were more likely to have hypertension relative to NMs (*1/*10 or *1/*1). They also reported that IMs (*10/*10) had higher homeostatic model assessment of insulin resistance and alanine transaminase levels relative to NMs (*1/*1). However, in a cross-sectional study of 89 risperidone treated Thai children, Suskasem et al. (2018) did not detect an association between CYP2D6 genotype-predicted phenotypes or ASs and insulin resistance.
Neurological and movement disorders
Two case studies have reported a tentative association between CYP2D6 and antipsychotic-induced neurological or movement disorders. The first reported by Köhnke et al. (2002) was a 17-year male and CYP2D6 PM (*4/*4) treated with risperidone who developed severe extrapyramidal symptoms that only subsided after risperidone discontinuation. Similarly, Butwicka et al. (2014) reported that a 16-year-old adolescent and CYP2D6 PM (*4/*4) treated with haloperidol, lorazepam, levomepromazine, and olanzapine developed neuroleptic malignant syndrome. The authors suggested that this event was likely due to haloperidol, given urine toxicology after 6 weeks of the last administration of neuroleptics revealed the presence of haloperidol, but not olanzapine (levomepromazine was not measured).
Discussion
Our systematic review of the current knowledge base suggests that CYP2D6 genotype-predicted phenotypes may have an impact on antipsychotic pharmacokinetics and adverse drug reactions but not efficacy in children and youth. Importantly however, many of the reported associations have not yet been independently replicated in children and youth, and most studies were underpowered to detect associations between CYP2D6 and antipsychotic treatment outcomes, particularly among PMs and UMs. Nevertheless, the reported associations in the pediatric literature echo findings reported in the adult literature, which has been presented elsewhere (Pouget et al. 2014; Puangpetch et al. 2016; Jukic et al. 2019; Yoshida and Müller 2019; van Westrhenen et al. 2020).
The concordance between the pediatric and adult literature is perhaps not surprising, given that the expression of CYP2D6 reaches adult levels soon after birth (Upreti and Wahlstrom 2016). However, we are not suggesting that CYP2D6 studies in adults should be simply extrapolated to pediatric patients. Children and adolescents do have unique characteristics that should be considered, such as age-dependent differences in the body liquid composition (including hepatic capacity), distribution of serum proteins, and factors affecting blood–brain barrier permeability, as well as lifestyle and hormonal differences. As such, further pharmacogenetic studies are warranted in children and adolescents, particularly studies that address the limitations highlighted in this review.
All of the studies were limited by one or more of the following factors: (1) retrospective or cross-sectional study designs, which make it difficult to establish causal relationships; (2) small sample sizes resulting in limited representation of the full spectrum of CYP2D6 metabolizer phenotypes, particularly PMs and UMs; (3) poor coverage of CYP2D6 genetic variation; (4) heterogeneous patient groups with regard to age, ethnicity, diagnoses, illness severity, drugs and doses used, and treatment duration; (5) lack of standardized outcome measures; and (6) minimal consideration for concomitant drug impacts on CYP2D6 genotype-predicted phenotypes. As such, several recommendations for future studies can be made.
First, the current knowledge base covers a large age range (3–21 years). Given the potential developmental, physiological, and hormonal changes that may affect a drug's pharmacodynamic and pharmacokinetic profiles within this age range, the field would benefit from future prospective studies confined to particular age groups or with sufficient sample size to examine age-specific effects. Doing so would assist in the establishment of therapeutic concentration windows for risperidone and 9-OH-risperidone that currently are not available but have been suggested to exist (Kloosterboer et al. 2020).
Second, researchers should utilize assays with adequate coverage of CYP2D6 genetic variation, including structural variation (i.e., gene duplications and hybrids). Likewise, strategically designed studies that enrich for patients with CYP2D6 UM and PM phenotypes would be desirable, as these phenotypes were associated with the greatest variations in antipsychotic treatment outcomes among the studies we reviewed.
Third, additional studies in populations from non-European backgrounds are needed, particularly as these populations carry variants that are relatively less frequent in Europeans (Huddart et al. 2018).
Fourth, studies of CYP2D6 substrates beyond risperidone are required. Although risperidone is an important first-line antipsychotic in child and adolescent psychiatry, other commonly used antipsychotics (e.g., aripiprazole) in children would benefit from further study.
Fifth, strong and moderate CYP2D6 inhibitors can impact on the interpretation of CYP2D6 genotype-predicted enzyme function. Many of these inhibitors (e.g., fluoxetine) are commonly used in combination with antipsychotics and, when present, can result in discordance between an individual's genotype-predicted metabolizer status and their clinical observed metabolizer phenotype, a phenomenon known as phenocopying or phenoconversion. For example, a CYP2D6 genotype-predicted NM taking paroxetine, a strong CYP2D6 inhibitor, would phenotypically resemble a PM until paroxetine was discontinued. Likewise, inhibitors of other enzymes involved in antipsychotic drug metabolism could also result in a PM phenocopy that could be further exacerbated if CYP2D6 metabolism is also impaired. For example, the CYP3A4 inhibitor ketoconazole has been shown to increase risperidone concentrations (Mahatthanatrakul et al. 2012). Although most of the studies reviewed herein included children and youth on monotherapy, in real-world practice, polypharmacy is a reality and as such phenocopying/phenoconversion requires attention. Future pragmatic studies should account for concomitant drugs when determining an individual's genotype-predicted metabolizer status and report the prevalence or incidence of phenocopying/phenoconversion within their study sample.
Although our systematic review rigorously followed PRIMSA guidelines, there are notable caveats. First, our inclusion criteria encompassed studies that examined CYP2D6 and antipsychotic outcomes in participants up to the age of 25 years. This decision was made in an effort to increase the number of studies for inclusion in the review and also aligns with the notion that the age of 18 is not necessarily an appropriate threshold when investigating questions that can be affected by developmental processes. Second, our search strategy did not yield the number of studies required to conduct a meta-analysis of the current knowledge, and as such, only qualitative interpretations were permitted. Furthermore, our search yielded five studies (Sukasem et al. 2016, 2018; Vanwong et al. 2016, 2017; Nuntamool et al. 2017) from the same research group that appeared to use overlapping cohorts. Despite the presumed participant overlap, these studies were retained as each study examined an independent outcome associated with CYP2D6. Finally, we interpreted the CYP2D6 metabolizer phenotypes as published by the authors of the included studies. Although standardization of the CYP2D6 genotype to phenotype translation process has recently been established (Caudle et al. 2020), all the studies included in this review predated this standardization. As such, variation in the genotype to phenotype translation process across the included studies could produce differing results that should be considered when interpreting the findings of this review.
Conclusion
The current child and youth knowledge base suggests that CYP2D6 genetic variation has an appreciable impact on antipsychotic pharmacokinetics and the propensity for adverse drug reactions, particularly metabolic adverse reactions among those receiving risperidone treatment. However, the evidence is still emerging, and a number of CYP2D6 investigations among children and youth treated with antipsychotics are expected in the future.
Clinical Significance
Future studies will be essential to the development of guidelines and decision-making related to the implementation of CYP2D6-guided antipsychotic drug selection and dose optimization in child and adolescent psychiatric services. Assuming these future studies support the link between CYP2D6 genetic variation and antipsychotic outcomes, we would anticipate an increase in the implementation of CYP2D6-guided antipsychotic drug selection and dose optimization in child and adolescent psychiatric services.
Footnotes
Acknowledgments
C.A.B. is supported by the Cumming School of Medicine and Alberta Children's Hospital Foundation. P.D.A. is supported by the Alberta Innovates Translational Health Chair in Child and Youth Mental Health.
Disclosures
A.A.M., D.J.M., and C.B. are members of the Clinical Pharmacogenomics Implementation Consortium. K.J.A. has acted in a consulting capacity for companies, including Roche Diagnostics, Bristol-Myers Squibb and Otsuka Pharmaceuticals Ltd., Otsuka Canada Pharmaceuticals, Inc., Lundbeck, and HLS Therapeutics. She has also received research support from companies, including Bristol-Myers Squibb and Otsuka Pharmaceuticals, Johnson and Johnson Research and Development, Jannsen, Inc., Canada, and Roche Molecular Systems. D.J.M. is co-investigator in two pharmacogenetic studies where genetic test kits were provided as in-kind contribution by Assurex Health (Myriad Neuroscience) to evaluate feasibility of pharmacogenetic testing in clinical practice and potential benefits of pharmacogenetic testing compared to treatment as usual. D.J.M. has not received any payments or received any equity, stocks, or options from this company or any other pharmacogenetic companies. D.J.M. is co-investigator in two filed genetic patents assessing risk for antipsychotic-induced weight gain. C.B. has received material support from Assurex Health (Myriad Neuroscience), CNSDose, Genomind, and AB-Biotics for research purposes but does not have equity, stocks, or options in these companies or any other pharmacogenetic companies. C.B., D.J.M., and K.J.A. are members of the Genetic Testing Committee of the International Society of Psychiatric Genetics. K.S. and P.D.A. declare no conflicts.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.