
Abstract
Objective:
The effects of selective serotonin reuptake inhibitor (SSRI) on deficits in attention and executive function in adolescents with major depressive disorder (MDD) are relatively unknown. We aimed to investigate changes in symptom measures of attention in adolescents with MDD treated with escitalopram.
Methods:
The study included 82 MDD adolescents and 54 healthy controls aged from 12 to 17 years. Symptom measures of attention were assessed using the Attention-Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) and Child Behavior Checklist attention problems scale at baseline and during week 8. Adolescents who showed at least 40% improvement in the Children's Depression Rating Scale-Revised (CDRS-R) scores from baseline to week 8 were referred to as “responders.”
Results:
No baseline differences were found between the responders (n = 47) and nonresponders (n = 35) in their age, sex, intelligence quotient, CDRS-R score, and attention measures. Linear mixed models showed significant group-by-time interaction effect in the ADHD-RS inattention subscale score, but not in the other attention measures.
Conclusion:
Our results suggest that treating depressive symptoms with SSRI may lead to improvements in attention in MDD adolescents. Monitoring changes in symptom measures of attention can be useful when treating adolescents with MDD.
Introduction
Major depressive disorder (MDD) is commonly associated with cognitive impairment (Rock et al. 2014). The diagnostic criteria for MDD in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5; American Psychiatric Association 2013) include impairment in cognition (i.e., diminished ability to think or concentrate or indecisiveness). There is increasing evidence that neurocognitive impairment is common in adults with MDD (Hammar and Årdal 2009; Wagner et al. 2012). A recent meta-analysis showed that executive neuropsychological impairment was associated with adult MDD and depressive symptom severity (Snyder 2013). However, this association is less clear in depressed children and adolescents (Vilgis et al. 2015).
Cognitive impairment in depression is an important feature associated with poor general functioning (Baune et al. 2010). As cognitive impairment was suggested to be a major mediator of functional impairment in adult MDD (McIntyre et al. 2013), much attention is being given to the role of cognitive function in depression treatment (Bortolato et al. 2014). Considering that childhood and adolescence are critical periods of cognitive development and academic achievement, it is important to investigate this domain in the pediatric population.
Longitudinal effects of antidepressants on cognitive function in children and adolescents with MDD are relatively unknown. In a systemic review and meta-analysis in adults (Rosenblat et al. 2015), the authors found that antidepressants have beneficial effects on cognitive function, especially on psychomotor speed and delayed recall in adult MDD. In one study in adolescents (Shehab et al. 2016), patients with depression showed persistent deficits in visual memory and sustained attention compared with healthy controls after treatment with fluoxetine. However, no study has examined the longitudinal effects of escitalopram on cognitive functions in depressed children and adolescents.
In Korea, many adolescents and their parents complain about attentional problems. As education and academic achievement are excessively emphasized in Korea, attention problems during schoolwork are distressing. In one study (Lee 1994), the attention states of Korean adolescents were reported to be more negative than those of American adolescents, and the attention states of individuals during schoolwork activities were associated with depression in Korean adolescents. Therefore, attention problems are sometimes perceived earlier and more often than depressed mood by Korean adolescents or their parents. Considering the importance of attentional problems in Korean adolescents, we used symptom measures of attention to assess cognitive function in this study.
The aim of this study was to investigate the changes in symptom measures of attention in adolescents with MDD treated using escitalopram. We expected that adolescents with MDD would have lower scores on symptom measures of attention than healthy controls at baseline. In addition, we hypothesized that adolescents with MDD would show improvements in symptom measures of attention during the course of treatment. Specifically, participants who respond to treatment would show better outcomes with respect to symptom measures of attention compared with those who do not respond. To the best of our knowledge, this is the first study to investigate the changes in symptom measures of attention during escitalopram treatment in pediatric depression.
Methods
Participants
A total of 95 adolescents aged from 12 to 17 years with primary diagnosis of MDD were recruited from the child and adolescent psychiatric outpatient clinic of Seoul National University Hospital between August 2015 and June 2018. MDD diagnoses were made using the Kiddie-Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997, 2016; Kim et al. 2004b) according to the DSM-5 criteria. Participants were included in the study if they had MDD symptoms lasting for at least 4 weeks or more without psychotic features, a score of 40 or higher on the Children's Depression Rating Scale-Revised (CDRS-R) (Poznanski and Mokros 1996), and a score of 4 or higher on the Clinical Global Impressions-Severity (CGI-S) (Guy 1976) at baseline. Participants were excluded from the study if they had a full-scale intelligence quotient (IQ) lower than 70; had a history of alcohol or substance abuse within the past 6 months; had a history of schizophrenia, bipolar disorder, eating disorder, or autism; had chronic medical conditions (e.g., asthma, inflammatory bowel disease, and diabetes); had first-degree relatives with a history of bipolar I disorder; and took any concurrent medication with psychotropic effects other than stimulants for attention-deficit/hyperactivity disorder (ADHD).
A total of 57 healthy controls were recruited from local communities through school flyers. All healthy controls were screened using the K-SADS-PL and only those with a full-scale IQ of at least 70 or more, without any history of psychiatric disorders, without first-degree relatives who had a history of any psychiatric disorders, and not taking any medication with psychotropic effects were included in this study.
The present study included 82 depressed adolescents and 54 healthy controls, who had analyzable data for symptom measures of attention at baseline and during week 8. This study was approved by the Institutional Review Board (IRB) for Human Subjects at the Seoul National University Hospital (IRB No. 1504-1113-668). Detailed information about the study was provided to the adolescents and parents, and written informed consent was obtained before the study began.
Procedures
All MDD subjects were treated with escitalopram in an 8-week open-label trial. Escitalopram treatment was initiated at 5 mg/day for the first week and increased to 10 mg/day during week 2. From week 3, the dose of escitalopram was flexibly titrated to a maximum dose of 30 mg/day if there was no satisfactory clinical improvement. The use of psychotropic medication simultaneously was not permitted except the use of stable doses of stimulants for ADHD. Individual psychotherapy or cognitive behavior therapy for depression was not allowed during the study.
Symptom measures
All participants completed several questionnaires, including the CDRS-R, CGI-S, Attention-Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS), and Child Behavior Checklist (CBCL) at baseline and during week 8. In MDD subjects, clinical severity and treatment response were assessed during weeks 1, 2, 4, 6, and 8 using the CDRS-R and CGI-S. The primary measure of effectiveness was the change in the score on the CDRS-R from baseline to week 8. During week 8, MDD subjects who had at least a 40% decrease in the adjusted CDRS-R total score (CDRS-R total minus 17, the minimum possible total score) were referred to as responders, and those who did not meet this criterion were referred to as nonresponders. In healthy controls, the CDRS-R and CGI-S were done at baseline and during weeks 2 and 8, while the ADHD-RS and CBCL were done at baseline and during week 8.
Children's Depression Rating Scale-Revised
The CDRS-R is an interviewer rating scale, which is widely used to assess the severity of depression and response to treatment. It comprises 17 items for the evaluation of mood, somatic, subjective, and behavioral symptoms. Total scores on the CDRS-R range from 17 to 113, with 14 items being rated on a scale of 1–7 and the remaining three items being rated on a scale of 1–5. These three items are rated based on the interviewer's observation only. In this study, we used the Korean version of the CDRS-R, which showed high internal consistency (α = 0.91) and strong criterion and discriminant validity (Kim et al. 2017). A total score of 40 or higher on the Korean version of the CDRS-R indicates the presence of depressive disorder.
Attention-Deficit/Hyperactivity Disorder Rating Scale-IV
The ADHD-RS was developed to evaluate the severity of ADHD symptoms in children and adolescents (DuPaul et al. 1998). It is a four-point Likert, 18-item scale according to the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association 1994). It is a scale for assessing the frequency of symptoms over 1-week period, provided by parents or teachers. It consists of two subscales, which are namely the inattention and hyperactivity–impulsivity. The even-numbered items in the ADHD-RS are symptoms on the hyperactivity–impulsivity subscales, whereas the odd-numbered items are those on the inattention subscales. The Korean version of the ADHD-RS was developed and standardized (So et al. 2002; Kim et al. 2003). In this study, we used the parent rating version of the ADHD-RS administered by trained psychologists (Kim et al. 2004a).
Child Behavior Checklist
The CBCL is a parent rating questionnaire for the assessment of behavioral problems and social competencies of children during the previous 6 months (Achenbach 1991). It has three-point Likert scale (0 = “not true,” 1 = “somewhat or sometimes true,” and 2 = “very true or often true”), and raw scores can be transformed to norm-referenced T-scores. The CBCL consists of two main scales, namely the behavior problem and social competence scales. The behavior problem scale has eight syndrome scales: anxious/depressed, withdrawn, somatic complaints, delinquent behavior, aggressive behavior, social problems, thought problems, and attention problems. Among these syndrome scales, we are more interested in the attention problems scale. It assesses both inattention and hyperactivity–impulsivity symptoms. The Korean version of the CBCL was standardized and shown to be both valid and reliable (Oh and Lee 1990). A T-score of 60 on the attention problems scale showed diagnostic discrimination for ADHD in both in the United States and Korea (Biederman et al. 1993; Kim et al. 2005). In this study, we shortened the time frame of the CBCL to 1 week to reflect symptoms only during the study.
Statistical analyses
Demographic and clinical characteristics at baseline were compared between the MDD subjects and healthy controls or the responders and nonresponders using Student's t-tests for continuous variables and the Chi-square test for categorical variables. Relationships between variables were examined using Pearson correlation analysis. We performed a linear mixed model to examine changes in symptom measures of attention over time (baseline vs. week 8) in groups (responders vs. nonresponders). Time, group, and time × group interaction were included in the model as fixed effects, while intercept was as a random effect. All analyses were performed using IBM SPSS Statistics version 25 (SPSS, Inc., Chicago, IL), and statistical significance was set at a p-value <0.05.
Results
Demographic and clinical characteristics
There were no significant differences between the MDD subjects and healthy controls in age and sex (Table 1). However, the two groups showed significant differences in IQ (p = 0.039), the CDRS-R score, ADHD-RS total score, ADHD-RS inattention subscale score, ADHD-RS hyperactivity–impulsivity subscale score, and CBCL attention problems scale score at baseline (p s ≤ 0.002).
Baseline Demographic and Clinical Characteristics of Patients with Major Depressive Disorder and Healthy Controls
Healthy controls (n = 53).
MDD patients (n = 79); Healthy controls (n = 51).
ADHD-RS, Attention-Deficit/Hyperactivity Disorder Rating Scale; CBCL, Child Behavior Checklist; CDRS-R, Children's Depression Rating Scale-Revised; IQ, intelligence quotient; SD, standard deviation; MDD, major depressive disorder.
Forty-seven (57.3%) of the 82 adolescents with MDD were classified as responders. Between the responders and nonresponders, there were no significant differences in age, sex, IQ, number of subjects with comorbid ADHD, and proportion of subjects in their first depressive episode (Table 2). In addition, the severity of depression on the CDRS-R and symptom measures of attention did not differ significantly between these two groups at baseline.
Baseline Demographic and Clinical Characteristics of Responders and Nonresponders to Treatment with Escitalopram
Responders (n = 45); Nonresponders (n = 34).
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, Attention-Deficit/Hyperactivity Disorder Rating Scale; CBCL, Child Behavior Checklist; CDRS-R, Children's Depression Rating Scale-Revised; IQ, intelligence quotient; SD, standard deviation.
Relationships between symptom measures of attention and depression at baseline
Within the MDD group, all symptom measures of attention were positively correlated with each other (Table 3). However, no correlations were observed between all symptom measures of attention and severity of depression, assessed using the CDRS-R in the MDD subjects.
Correlations Between Clinical Measures of Attention and Severity of Depression in Patients with Major Depressive Disorder at Baseline (n = 82)
MDD patients (n = 79).
ADHD-RS, Attention-Deficit/Hyperactivity Disorder Rating Scale; CBCL, Child Behavior Checklist; CDRS-R, Children's Depression Rating Scale-Revised.
Effects of treatment on attention
As no significant differences in age, sex, and IQ were found between the responders and nonresponders at baseline, we did not include any adjustments for these variables in the linear mixed model. Estimated marginal mean scores for symptom measures of attention at baseline and week 8 are presented in Table 4. There was a significant effect of time × group interaction (F = 4.3, p = 0.04) in the ADHD-RS inattention subscale score (Fig. 1). However, there were no significant time × group interactions in the ADHD-RS total score, ADHD-RS hyperactivity–impulsivity subscale score, or CBCL attention problems scale score.
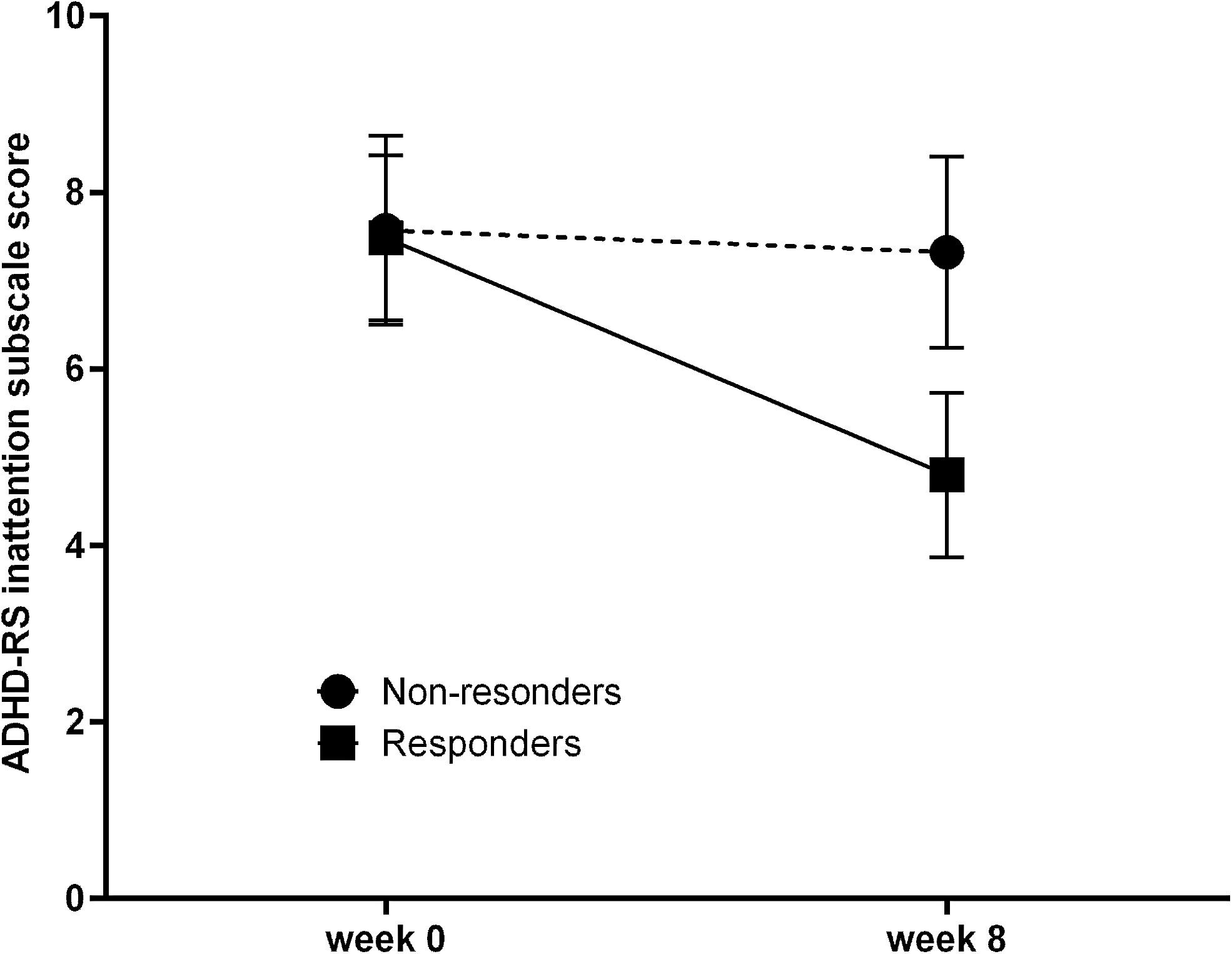
Changes in scores on ADHD-RS inattention subscale during 8-weeks intervention. ADHD-RS, Attention-Deficit/Hyperactivity Disorder Rating Scale.
Changes in Scores on Clinical Measures of Attention During Eight Weeks Intervention
Responders (n = 45); nonresponders (n = 34).
Responders (n = 47); nonresponders (n = 35).
Estimated marginal means (standard error).
Time × group effect of linear mixed model.
ADHD-RS, Attention-Deficit/Hyperactivity Disorder Rating Scale; CBCL, Child Behavior Checklist.
Discussion
In this study, we examined the changes in symptom measures of attention during escitalopram treatment in adolescents with MDD. Our result showed that adolescents with MDD had more attentional problems than healthy controls at baseline. However, there was no difference in symptom measures of attention at baseline between responders and nonresponders. With respect to the effect of escitalopram, only the ADHD-RS inattention subscale score changed significantly between responders and nonresponders during 8 weeks of treatment.
Surprisingly, little is known about symptom measures of attention in children and adolescents with MDD. In adults, depression is associated with symptom measures of cognitive function. For instance, both seasonal and nonseasonal depression groups filed more cognitive complaints compared with the control group. The cognitive complaints were evaluated using the Cognitive Failures Questionnaire, which measures self-reported failures in simple daily tasks (Sullivan and Payne 2007). In another study (Farrin et al. 2003), the depressed group filed more cognitive complaints, but in much greater proportion to neuropsychological errors, as a form of catastrophic reaction to mistakes. Consistent with previous adult studies, we found that among adolescents, the MDD group had more attentional problems than the control group.
However, there were no correlations between the symptom measures of attention and severity of depression at baseline in this study. In several adult studies, on the contrary, correlations between depression severity and symptom measures of attention have been reported (Lawrence et al. 2013; Benedict et al. 2014). The difference between pediatric and adult MDD may explain this discrepancy. In a systemic review of executive function and attention in children and adolescents (Vilgis et al. 2015), the authors suggested that the duration and chronicity of depression play important roles in maintaining cognitive deficits. Adults with MDD may have longer periods of unnoticed illness and more recurrences than children and adolescents, which could partly explain the absence of correlations between symptom measures of attention and severity of depression in this study.
With regard to the effects of selective serotonin reuptake inhibitors on symptom measures of attention in children and adolescents, to the best of our knowledge, no study has been conducted in individuals with depression only. In children with ADHD and comorbid nonbipolar mood disorder, fluoxetine monotherapy improved not only the severity of depressive symptoms but also caregiver-rated measures of attention/overactivity (Quintana et al. 2007). Similarly, in an open study of bupropion, an antidepressant with dopaminergic- and noradrenergic-agonist effects, bupropion sustained release improved both depressive and parent-reported ADHD symptoms in adolescents with comorbid ADHD and depression (Daviss et al. 2001). In the current study, we found that the score on the ADHD-RS inattention subscale, but not on the hyperactivity–impulsivity subscale, changed differently during the 8-week treatment period among the responders and nonresponders. This finding suggests that inattention is more specific than hyperactivity in monitoring changes in cognitive function during treatment for depression in adolescents. In other words, this could reflect the importance of evaluating symptom measures of attention, specifically the ADHD-RS inattention subscale, as a proxy for treatment response in adolescents with MDD.
There were some limitations in this study. First, our results are based on an open-label study. This limits evaluation of improvement because of the effect of knowledge of treatment. Furthermore, since we assessed attentional function in adolescents based on parent reports, not objective neuropsychological tests, the severity of the attentional problems could have been under- or overestimated. Considering that complaints of concentration and memory are experienced by adolescent patients themselves, parents might have difficulty rating problems associated with concentration and memory experienced by adolescents. It is also possible that the reports of parents concerning their children's attention symptoms were influenced by parental characteristics or anxiety. Thus, future placebo-controlled studies with a cognitive assessment of attention are needed to confirm our preliminary findings. However, since the scores assigned by parents on the Korean version of the ADHD-RS distinguish between children and adolescents with ADHD and those without (Kim et al. 2003), parent report-based symptom measures of attention provide useful information about attentional function in depressed children and adolescents. Furthermore, the fact that there was no clear association between the results obtained from objective neuropsychological tests and depression in children and adolescents (Vilgis et al. 2015) suggests that subjective symptom measures may be better proxies for evaluating the effects of treatment on attention in depressed children and adolescents than neuropsychological measures.
Conclusions
In summary, this study highlights the importance of using the results from symptom measures of attention as proxies for neurocognitive changes during the treatment of adolescents with MDD. The pattern of change in the scores from the ADHD-RS inattention subscale during escitalopram treatment differs between responders and nonresponders. These findings suggest that symptom measures of attention can provide clinicians with useful information for predicting responses to antidepressants during MDD. Furthermore, cognitive impairment may be an important target for the treatment of depression in children and adolescents.
Clinical Significance
In adolescents with depression, the effects of antidepressant on deficits in attention are relatively unknown. There were no differences in symptom measures of attention between responders and nonresponders at baseline. ADHD-RS inattention subscale score showed a significant effect of time × group interaction during antidepressant treatment. Treating depressive symptoms with antidepressant may lead to improvement in attention in adolescents with depression.
Footnotes
Disclosures
No competing financial interests exist.