
Abstract
Objectives:
Majority of youth with autism are taking two or more medications (psychotropic or nonpsychotropic) simultaneously, also known as polypharmacy. Yet the efficacy and the potential outcomes of polypharmacy in this population are widely unknown. This systematic literature review described the trends of polypharmacy among autistic youth, and identified factors associated with polypharmacy.
Methods:
Sixteen studies were included, encompassing over 300,000 youth with autism.
Results:
Rates of polypharmacy varied quite substantially across studies, ranging from 6.8% to 87% of autistic youth. Having psychiatric comorbidities, self-injurious behaviors, and physical aggression, as well as being male and older, were associated with higher rates of polypharmacy.
Conclusion:
Findings emphasize the importance of further research to determine appropriate practices related to the monitoring of adverse side effects, and the long-term impact of polypharmacy among autistic youth.
Introduction
Autism spectrum disorder is a neurodevelopmental disorder characterized by impairments in social communication, and the presence of restricted, repetitive interests and activities (American Psychiatric Association 2013). Children and youth i with autism ii frequently experience co-occurring mental and physical health issues, including psychiatric disorders, seizures, epilepsy, sleeping problems, and gastrointestinal disorders (Woolfenden et al. 2012; Isaksen et al. 2013; Mazefsky and Herrington 2014; Salazar et al. 2015; Gordon-Lipkin et al. 2018; Lai et al. 2019). Psychopharmacology is often associated with a reduction in mental health symptoms and severity, along with other co-occurring symptoms among individuals with autism (Vohra et al. 2016). Currently, there are no pharmacological treatments approved by the U.S. Food and Drug Administration (FDA) that address the core symptoms of autism (e.g., social communication difficulties and repetitive/rigid behaviors and interests).
Despite this, previous research highlights that a large number of individuals with autism are prescribed and use psychotropic medications in an attempt to address both primary and secondary autism symptoms, including aggression, irritability, and self-injury (Wink et al. 2018). While high rates of pharmacotherapy are commonly attributed to the management and treatment of co-occurring physical and mental health problems (Hollander et al. 2005), Houghton et al. (2017) found that ∼1/3 of autistic people between the ages of 3 and 65 years are prescribed a psychotropic medication without the presence of a co-occurring psychiatric disorder.
The U.S. FDA has approved only two psychotropic drugs (risperidone and aripiprazole), both atypical antipsychotics, for autistic youth between 5 and 17 years to address irritability (a common secondary symptom of autism; Squibb 2015; Food and Drug Administration 2006). Yet, individuals with autism are often prescribed several other classes of medication, including antidepressants, stimulants, anxiolytics, and anticonvulsants (Aman et al. 2005; Lake et al. 2012, 2014; Hirsch et al. 2017; Wink et al. 2018). For example, most (97.1%) autistic youth (mean age = 12.9 years; SD = 3.3 years) admitted to psychiatric facilities were treated with various combinations and doses of antipsychotics (e.g., risperidone, quetiapine, aripiprazole, paliperidone, ziprasidone, olanzapine, loxapine, thioridazine, asenapine, clozapine, haloperidol, pimozide, trifluoperazine, and chlorpromazine; Wink et al. 2018). Furthermore, psychotropic polypharmacy (defined by authors as use of more than one concomitant psychotropic medication at once) was present in over half of the participants (Wink et al. 2018).
In recent decades, there has been a 4- to 18-fold increase in the rates of prescribing and use of second-generation antipsychotics (Elbe et al. 2015). In both clinical and research contexts, there has also been a growing concern regarding pharmacological treatments related to dosage-type drug toxicity when multiple medications are used concurrently, and especially in the absence of adequate monitoring for youth (Spencer et al. 2013; Jobski et al. 2017; Wink et al. 2018).
Taking multiple psychotropic medications at the same time (a practice termed polypharmacy) appears to occur frequently in autistic youth despite little evidence to support this practice. While varying definitions of polypharmacy exist in the literature (Masnoon et al. 2017), in psychiatry, polypharmacy has been defined by the National Association of State Mental Health Program Disorders as the use of two or more psychiatric medications in the same patient (Flaum et al. 2001). In addition to the limited evidence for the practice of polypharmacy, there are a number of known side effects that youth with autism currently experience when using psychotropic medications, including adverse drug reactions such as marked weight gain, sedation, and the risk of extrapyramidal symptoms (e.g., tremors, dystonia, paranoia; Aman et al. 2005; McDougle et al. 2005; McPheeters et al. 2011). Other reported side effects include neurological symptoms, gastrointestinal distress, lower quality of life, and metabolic issues (e.g., type 2 diabetes mellitus, dyslipidemia, obesity, hypertension, metabolic syndromes; Ceylan et al. 2016; Hirsch et al. 2017; Iversen et al. 2018).
Autistic youth are not the only clinical group who are taking multiple medications concurrently. For example, 40%–50% of autistic adults are on more than one medication at the same time, with lower levels of social competence, poorer adaptive behavior, older age, restrictive housing, and severity of autism symptomatology found to contribute to the prescribing of one or more medications (Aman et al. 2003, 2005; Lake et al. 2014; Poling et al. 2017). A multitude of long-term adverse consequences of polypharmacy, including health care costs, (Santibáñez-Beltrán et al. 2013; Maher et al. 2014), increased risk for poor clinical outcomes (e.g., depression), cognitive and functional decline, delirium, (Frazier 2005; Onder et al. 2012; Hein et al. 2014), and mortality (Bemben 2016), have been found in elderly populations without autism. Similarly, adults with an intellectual disability (ID) are frequently prescribed psychotropic medications, with ∼22% on multiple medications at the same time (Lunsky and Modi 2017). Among adults with ID, those more likely to receive psychotropic polypharmacy were women, those living in supervised residential settings, and those with a psychiatric diagnosis in two or more diagnostic categories (Lunsky and Modi 2017).
Polypharmacy is present in other pediatric populations, including children in foster or residential care, and children with other neurodevelopmental disorders. For instance, Medicaid claims of children in foster or residential care suggest that rates of psychotropic medication use range from 21% to 52% (dosReis et al. 2001; Ferguson et al. 2006; Zito et al. 2008; Government Accountability Office 2011). This is significantly higher than the rate of 4% in the general pediatric population (Olfson et al. 2002). Zito et al. (2008) found that ∼41% of children in foster or residential care were taking multiple psychotropic medications simultaneously. In addition, polypharmacy in individuals with fetal alcohol spectrum disorder is overwhelmingly common. In particular, families and caregivers frequently seek out medications to treat behavioral and attention difficulties (Ipsiroglu et al. 2015), despite some medications, (e.g., stimulant medication) being only partially effective in this population (Coles 2001; Rasmussen et al. 2008).
Many characteristics inherent with a diagnosis of autism make prescribing appropriate medications for autistic youth challenging, such as lack of verbal communication and awareness of body and emotions. These deficits can result in inappropriate drug prescribing and can potentially lead to side effects and decreased effectiveness in the absence of a medical follow-up. While many of these psychotropic medications have shown to be effective in managing some symptoms associated with autism independently, little is known about the trends, effectiveness, and long-term impact of psychotropic polypharmacy on the development of autistic people. The current systematic review aimed to fill this gap in the existing literature by the following: (1) describing the rates of psychotropic polypharmacy use among youth with autism (aged 5–25 years); and (2) identifying factors associated with psychotropic polypharmacy. It was expected that autistic youth would have high rates of polypharmacy overall. In particular, we hypothesized that youth experiencing aggression and self-injury would have higher rates of psychotropic polypharmacy than autistic youth with depression and anxiety, or other internalizing issues.
Methods
Literature search
A systematic literature search was conducted using five different electronic databases: PsycINFO, Medline, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, and Cochrane. Each database was searched from inception until March of 2020 using relevant controlled vocabulary terms and key terms related to autism (e.g., autism spectrum disorder, autistic disorder [AD]), age (e.g., child, youth, young adults), psychotropic medication type (e.g., antipsychotic, antidepressant, antiepileptic), and polypharmacy (e.g., polypharmacy, multi-drug, simultaneous). See Table 1 for the full search strategy.
Search Terms Used to Identify Relevant Articles
The electronic search was conducted independently by two authors (C.R., K.H.) and supplemented by a manual review of reference lists from eligible publications and relevant reviews. The review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al. 2009), as seen in Figure 1.
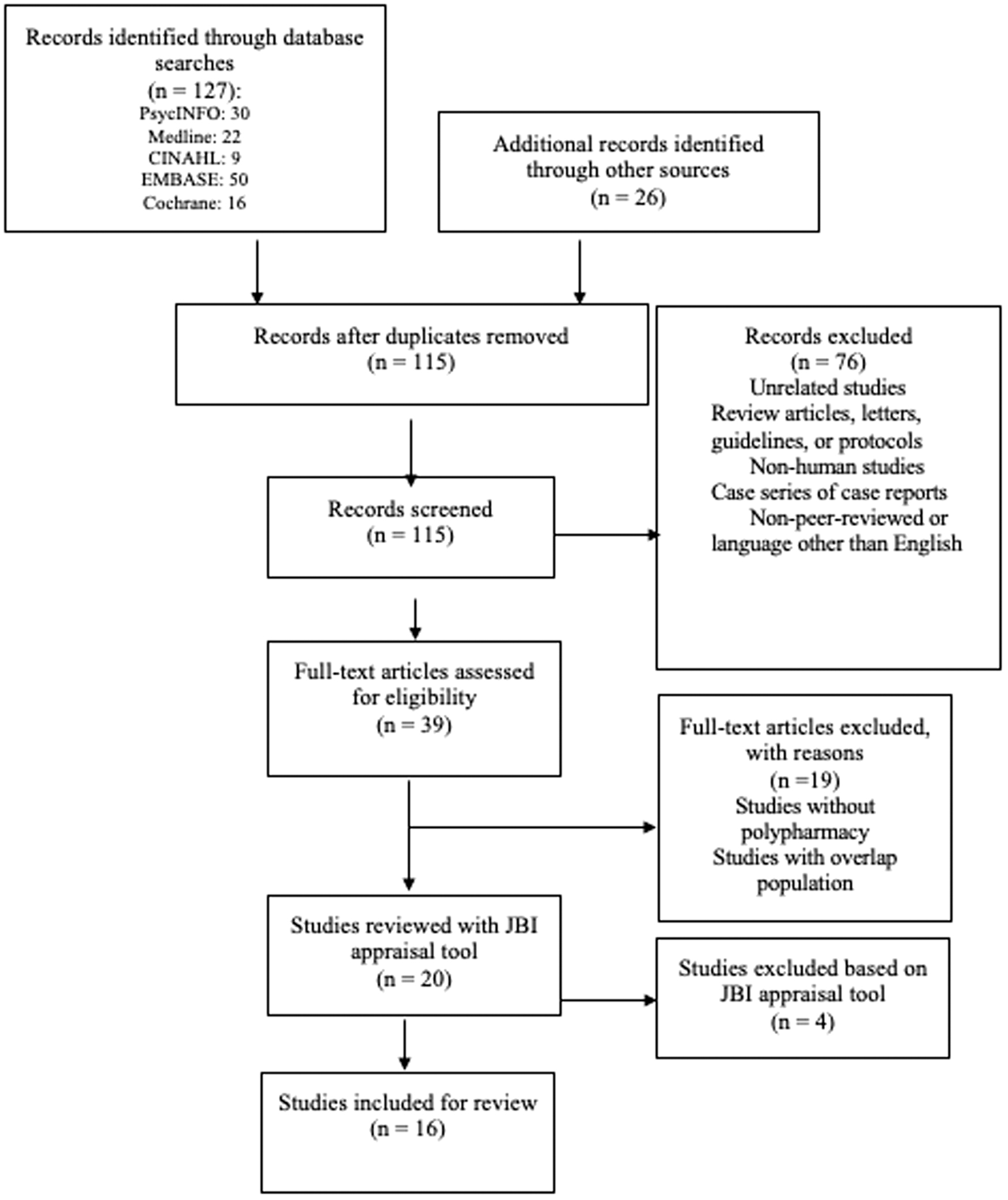
PRISMA diagram for systematic review of polypharmacy in children and youth with autism.
Inclusion and exclusion criteria
Across all databases, the search was restricted to studies written in English and published in peer-reviewed journals. Studies that reported quantitative estimates related to the use of psychotropic polypharmacy in youth (≤25 years of age) with a diagnosis of autism were included. If studies included participants who were older than 25 years and results were stratified by age group, the study was included, and data were extracted from the appropriate age group. Case studies were excluded, and eligible studies had to include youth with a primary diagnosis of autism, or acceptable diagnosis equivalent to autism (e.g., pervasive developmental disorder [PDD] or Asperger syndrome [AS]) consistent with previous versions of the Diagnostic and Statistical Manual of Mental Disorders (such as the DSM-IV-TR) or International Classification of Diseases and Related Health Problems (ICD-9 or ICD-10). Medications of interest were psychotropic medications. Due to variability in the terminology of specific drug classes, eligible studies had to explicitly state the drug class and prevalence rate of the medications studied. Based on previous literature and existing clinical guidelines, the present study operationalized polypharmacy as at least one episode of two or more medications used concurrently.
Data extraction
Two authors (C.R. and K.H.) independently extracted data using the following categories: patients, database and data source, total number of participants, definition of polypharmacy, and medication classes. Any inconsistencies were resolved by consensus and discussion with the third author (C.A.M.).
Critical appraisal
The Joanna Briggs Institute (JBI) Prevalence Critical Appraisal Checklist (Joanna Briggs Institute 2014) was applied to the selected articles to evaluate their scientific strength. The JBI Prevalence Critical Appraisal Checklist is a common approach used in systematic reviews to appraise the quality of available research evidence (Joanna Briggs Institute 2014). Nine checklist items were used from the JBI Prevalence Critical Appraisal Checklist: sample representativeness, sampling source, sample size appropriateness, description of study subjects and setting, data analysis with regard to the identified sample, validity of methods, standard and reliable measurement of participants, statistical analysis, and response rate. For each of the nine checklist items, studies were rated as fully meeting the criteria (“Y”), being unclear as to whether the criteria were met (“U”), or not fully meeting the criteria (“N”). Where disagreements among the reviewers occurred, ratings were discussed until a consensus was reached. See Table 2 for the completed JBI Prevalence Critical Appraisal Checklist on the included studies.
Joanna Briggs Institute (2014) Appraisal Tool
Rating questions: (1) Was the sample frame appropriate to address the target population? (2) Were study participants sampled in an appropriate way? (3) Was the sample size adequate? (4) Were the study subjects and the setting described in detail? (5) Was the data analysis conducted with sufficient coverage of the identified sample? (6) Were valid methods used for the identification of the condition? (7) Was the condition measured in a standard reliable way for all participants? (8) Was there appropriate statistical analysis? (9) Was the response rate adequate, and if not, was the low response rate managed appropriately?
N, criterion not met; U, unclear whether criterion met; Y, criterion fully met.
Results
Study selection and characteristics
The complete search strategy yielded 127 studies. Searching the reference lists of critical studies yielded an additional 26 studies. After removing duplicates, a total of 115 studies were identified. Titles and abstracts were subsequently screened for eligibility based on the predetermined inclusion and exclusion criteria (outlined above), resulting in the exclusion of 76 studies. Of the remaining 39 studies, full-text screening excluded 20 additional studies because samples included a primary diagnosis other than autism, or studies did not specifically state the prevalence of polypharmacy. The remaining 20 studies were then assessed using the JBI Prevalence Critical Appraisal Checklist (Joanna Briggs Institute 2014; Table 2). Four more studies were excluded through critical appraisal, resulting in a final total of 16 studies for analysis (see Fig. 1 for PRISMA diagram).
Study characteristics are summarized in Table 3. Of the 16 studies included, 12 studies were conducted in North America. Years of publication ranged from 1999 (Martin et al. 1999) to 2018 (Houghton et al. 2018), with the majority (N = 15) published in the last 10 years (2010 or later). Data sources included electronic health care databases, referral centers, and online surveys, as well as data obtained from autism societies or related organizations. The majority of results were obtained from claims data via physicians, pharmacies, hospitals, and other health care providers.
Design and Population Characteristics of Studies Reporting Quantitative Data in Children and Youth with Autism Taking Polypharmacy
ASD, autism spectrum disorder; CR, cross-sectional; CS, cohort study; IAN, Interactive Autism Network; NR, not reported; SSC, Simons Simplex Collection.
Studies differed with respect to how they operationalized polypharmacy (described in detail below) and psychotropic drug classes. Terms such as antipsychotics, neuroleptics, or tranquilizers were used most often to refer to “atypical antipsychotics” (or second-generation antipsychotics) such as aripiprazole, olanzapine, risperidone, or ziprasidone. In some studies, “antipsychotics” also included older drugs such as haloperidol, loxitane, or thioridazine. Antidepressants included selective serotonin reuptake inhibitors, serotonin and noradrenaline reuptake inhibitors, or tricyclic antidepressants. Classes and/or specific medications were noted when extracting the results.
Participant characteristics
Over 315,000 (N = 317,039) individuals were included in the studies reviewed, with sample sizes ranging from 61 (Wink et al. 2017) to 93,639 (Houghton et al. 2017). All studies included more males (M = 82.46%; Table 3) than females. Confirmation of autism diagnosis varied across studies and depended on the methodology used in each study. In particular, autism diagnostic codes from ICD-9 or ICD-10 or DSM-5 were used in studies using health administrative/claims databases, whereas in survey studies, autism diagnoses were reported by parents/caregivers or confirmed through diagnostic reports by a health provider. The majority of studies classified autism as AD, AS, or PDD—not otherwise specified. In one study (Martin et al. 1999), autism was defined by severity, through which only participants deemed to have “higher functioning” (IQ ≥70) PDDs were included for analysis of psychotropic medication use.
Majority of the studies (N = 10) included participants 18 years or younger. Specifically, two studies examined polypharmacy in youth between 7 and 14 years of age (Memari et al. 2012; Mire et al. 2014); one study examined children between 7 and 8 years of age (Logan et al. 2015); one study examined children and youth up to 16 years of age (Martin et al.,1999); four studies examined individuals up to 17 years of age (Rosenberg et al. 2010; Schubart et al. 2014; House et al. 2016; Madden et al. 2017); and one examined children 2–18 years of age (Coury et al. 2012). Others examined youth up to 21 years of age (Mandell et al. 2008; Spencer et al. 2013); one did not specify an age range (Wink et al. 2017); two studies compared polypharmacy in youth up to 25 years of age (Croteau 2017; Murray et al. 2014); and two others included adults (Houghton et al. 2017, 2018). Although the latter three studies included participants above the age exclusion criteria for the present study, these studies were included, as the majority of individuals fell within the appropriate age range. That is, given that authors stratified by age, only data from those studies concerning children and youth up to 25 years of age were utilized in the results and conclusions for this systematic review.
Frequencies and trends of polypharmacy among children and youth with autism
The definition of psychotropic polypharmacy varied across studies; however, the occurrence of at least one episode of two or more medications used concurrently (polypharmacy) ranged from 6.8% to 87% across all 16 studies (M = 31.31%, median = 30%). Definitions varied from “concurrent use of greater than one medication” (Coury et al. 2012), “two major classes” (Madden et al. 2017), “two or more drugs” (Murray et al. 2014), to “one or more psychotropic medication classes” (Mire et al. 2014), as seen in Table 4.
Definitions and Rates of Polypharmacy Among Children and Youth with Autism as per Medication Class
ADHD, attention-deficit/hyperactivity disorder; NR, not reported; SSRI, selective serotonin reuptake inhibitor.
Factors associated with increased risk of polypharmacy
Consistent with our hypothesis, the majority of studies revealed a higher prevalence of psychotropic polypharmacy as children age (Martin et al. 1999; Mandell et al. 2008; Rosenberg et al. 2010; Memari et al. 2012; Mire et al. 2014; Croteau et al. 2017; Houghton et al. 2017; Madden et al. 2017). Although the percentage of those receiving medication was similar among males and females, medication type differed by biological sex. For example, males were more often prescribed stimulants (Memari et al. 2012; Murray et al. 2014; Madden et al. 2017), while females were more likely to be taking antidepressants (i.e., fluoxetine) or mood stabilizers, such as valproic acid (Memari et al. 2012; Murray et al. 2014; Madden et al. 2017). Higher rates of polypharmacy were also found in children and adolescents of older ages (Mandell et al. 2008; Rosenberg et al. 2010; Coury et al. 2012; Spencer et al. 2013; Schubart et al. 2014; Logan et al. 2015).
Caucasian children and adolescents were found to have higher rates of psychotropic polypharmacy compared with other ethnic groups (including Latino and African American). Of note, four studies did not report the race and/or ethnicity of participants. Mandell et al. (2008) found lower rates of polypharmacy and medication use overall in children and youth with a diagnosis of AD residing in areas of the United States that have a lower percentage of Caucasian residents or greater urban density. In addition, the insurance plan type influenced prevalence of polypharmacy, such that higher rates among those individuals using private insurance were demonstrated in six studies (Rosenberg et al. 2010; Coury et al. 2012; Logan et al. 2015; House et al. 2016; Houghton et al. 2017; Madden et al. 2017).
Rates of psychotropic drug prescriptions and polypharmacy differed between countries. For example, 26% of autistic youth aged 0–21 years received psychotropic drug prescriptions in U.K's primary health care (Murray et al. 2014), whereas 56% of Medicaid-enrolled youth (aged 0–21 years) with autism received psychotropic drug prescriptions in the United States (Mandell et al. 2008). Murray et al. (2014) attributed this substantial difference to the more conservative practices of U.K. practitioners overall, and further stated that no psychotropic drugs are approved for individuals with autism in the United Kingdom (Murray et al. 2014). Similarly, Houghton et al. (2017) found that rates of psychotropic medication use in the United Kingdom were distinctly lower than in North America (specifically, the United States). There were significant differences between these two countries' polypharmacy rates as well, with 33.8% of youth with autism in the United Kingdom reportedly taking two or more psychotropic medications concurrently (Murray et al. 2014), and 20% of autistic youth in the United States using three or more medications concurrently (Mandell et al. 2008). This difference may be credited to distinct operationalizations of what constitutes polypharmacy and insurance-type.
As expected, the presence of physical and mental health symptoms/diagnoses was significantly associated with polypharmacy (Martin et al. 1999; Rosenberg et al. 2010; Coury et al. 2012; Spencer et al. 2013; Murray et al. 2014; Logan et al. 2015; House et al. 2016; Croteau et al. 2017; Houghton et al. 2017; Madden et al. 2017). Co-occurring mental health problems, including externalizing disorders (i.e., conduct disorder, oppositional defiant disorder; Coury et al. 2012), repetitive, restrictive behaviors (Mire et al. 2014), and attention-deficit/hyperactivity disorder (Martin et al. 1999; Mandell et al. 2008; Rosenberg et al. 2010; Memari et al. 2012; Mire et al. 2014; Schubart et al. 2014; Logan et al. 2015; Croteau et al. 2017; Madden et al. 2017), were found to be highly associated with polypharmacy. In addition, physical health problems such as gastrointestinal distress or sleep problems (Coury et al. 2012; House et al. 2016), and epilepsy (Memari et al. 2012; Mire et al. 2014; Schubart et al. 2014; Croteau et al. 2017; Houghton et al. 2017; Madden et al. 2017) were found to be associated with polypharmacy.
Functioning level/IQ of the participants or the presence of an ID was only described in six of the included studies, with the findings being mixed. Of these studies, the majority found that having an ID did not increase the likelihood of polypharmacy (Martin et al. 1999; Coury et al. 2012; Lake et al. 2014; Houghton et al. 2017); however, two studies (Mire et al. 2014; Croteau et al. 2017) reported that the presence of an ID was a predictor of medication use. For example, Mire et al. (2014) found that individuals with a higher IQ were less likely to be treated with psychotropic medications.
The most commonly observed drug classes were stimulant medications, followed by antipsychotics and anticonvulsants/mood stabilizers. Aggressive behavior was associated with higher rates of psychotropic polypharmacy in a number of cases (Coury et al. 2012; Logan et al. 2015; Wink et al. 2017). In addition, two studies (Mandell et al. 2008; Houghton et al. 2017) found that autistic youth in foster care were significantly more likely to be prescribed multiple medications at the same time.
Prescribing patterns
Prescribing patterns also varied across studies. Only two studies (Lake et al. 2014; Schubart et al. 2014) examined whether polypharmacy was interclass (between different medication classes) or intraclass (within the same medication class). Schubart et al. (2014) found a significant increase in both inter- and intraclass polypharmacy from 2000 to 2003, where interclass increased by 4% and intraclass increased by 2.5%.
Discussion
This systematic review described rates of polypharmacy among youth with autism and outlined specific factors that were associated with polypharmacy use. Among the studies reviewed, a markedly wide range of children and youth with autism were receiving psychotropic polypharmacy despite limited knowledge about the potential adverse side effects and long-term safety of polypharmacy use in autistic youth. It appears as though polypharmacy was often used to manage behavioral difficulties, as predictors of polypharmacy included psychiatric comorbidities, self-injurious behavior, and physical aggression across studies.
Use of psychotropic polypharmacy ranged from 9% to 87%, a range that may be of limited value in clinical practice with autistic youth. This large range in rates may be due to a more liberal definition of “polypharmacy” utilized in this review. This definition was chosen to: (1) be consistent with existing literature and guidelines; and (2) encapsulate the majority of instances of psychotropic polypharmacy among autistic youth. However, a major limitation in this field and our study is the large variability in the definitions of polypharmacy, and a lack of a clear universal definition in existing literature (Masnoon et al. 2017). Whereas some studies classified polypharmacy as “more than one medication,” other studies were more stringent in their definition and required three or more medications. In addition, polypharmacy definitions varied in terms of the time frame in which individuals were required to be on multiple medications from no requirement to 30, 60 (Schubart et al. 2014), or 90 days of continuous use (Croteau et al. 2017).
In the general population, little is known about the impact of polypharmacy on development, mental and physical health, and overall quality of life of youth with autism, as the majority of studies to date have focused on polypharmacy in adult or elderly populations. Similar to the elderly population, autistic youth may experience both co-occurring mental and physical health problems, and consequently, there is substantial prescribing of medications to manage these conditions. Physicians may prescribe nonindicated medications on a “trial” basis to help manage behavioral issues such as aggression, irritability, self-injury, and psychiatric comorbidities (Warren et al. 2011). Larger, longitudinal studies investigating the trends of polypharmacy are required, particularly since using multiple medications has the potential to compound autism symptomatology and may exacerbate the risk of self-injury, suicidal ideation, and other mental health issues.
Determining the etiological reasons for behavioral symptoms can be complex in autistic people as it is often difficult to distinguish symptoms related to autism versus those related to medical or psychiatric comorbidities (McGonigle et al. 2014). For example, there is emerging evidence suggesting that behavioral symptoms such as aggression and self-injury may be reactions to visceral pain or discomfort (Penmetsa et al. 2019; Cohen and Tsiouris 2020). In addition, medication is often a “first line” of treatment, rather than psychotherapy or other nonpharmacological interventions, when severe aggression is the primary presenting problem. This is especially the case in older male patients who are growing in physical size, in which the safety of their carers is often a high priority. Difficulties in distinguishing autism-related symptoms from secondary issues highlight the importance of monitoring when prescribing, and not treating behaviors with psychotropic medications when a possible medical reason may exist. There is also great need for systematic approaches or clinical guidelines to rule out medical comorbidities in this population before prescribing medication, which is particularly important among individuals who are nonverbal.
Overall, a focus on the efficacy and safety of concomitant medication use in autism (Spencer et al. 2013; Wink et al. 2017), and ultimately the development of pharmacological management guidelines for this population, needs to be considered. The “Stopping Overuse of Medication in People with ID” (STOMP) guidelines (Branford et al. 2019) highlight the excessive use of psychotropic medication among people with intellectual and developmental disabilities (IDD; including autism; NHS England 2018). The STOMP guidelines were developed in response to high rates of psychotropic medication use in adults with IDD and are among the few guidelines that propose standards for improving clinical practice in this population. These guidelines reference the prescribing of any psychotropic medication and outline a framework for clinicians to guide their prescribing practices. Furthermore, the STOMP guidelines highlight that reducing medication is beneficial for individuals with IDD, and most important, feasible. To date, no guidelines analogous to the U.K. STOMP guidelines have been created for use in North America for youth with IDD, including those with autism.
The impacts of combining medication and nonpharmacological interventions are also largely unknown (such as the combination of pharmacotherapy with behavior-analytic treatment), and measures of desired outcomes and side effects are often weak (Poling et al. 2017). Furthermore, the U.S. FDA-approved medications for autism (risperidone and aripiprazole) seem to only display moderate effectiveness and have been associated with substantial side effects such as sedation, obesity, dizziness, drooling, and tardive dyskinesia (McCracken et al. 2002; Warren et al. 2011; Dove et al. 2012). Little is known about the trends, effectiveness, long-term impact, and appropriate monitoring processes, or the methods in which the effectiveness and adverse side effects are continually checked, for youth with autism on multiple medications. However, this does not necessarily mean physicians are not monitoring their prescribing patterns in their clinical practice. It is possible that frequent monitoring following prescribing psychotropic medications is a practice that physicians are engaging in, although more knowledge and guidelines regarding these practices are crucial to ensure the effectiveness and safety of medication in this population.
Of the literature reviewed, only one study (Wink et al. 2017) included information regarding medication monitoring, or any mention of follow-up after medication was prescribed. Using a retrospective chart review, Wink et al. (2017) examined the effectiveness and safety of the use of multiple antipsychotic medications in autism through their longitudinal medication management database (between July 2004 and April 2012). Follow-up required caregivers to complete the Aberrant Behavior Checklist for symptoms at the start of medication treatment and at each 5-month follow-up period. This study specifically investigated the use of multiple antipsychotic medications in a sample of mostly Caucasian males diagnosed with autism and a co-occurring ID, in which the mean duration of treatment with multiple antipsychotics was 509 days (minimum 35 days and maximum 2659 days). The use of multiple antipsychotics was reportedly well tolerated in their sample, with few reported side effects and improvement with combination treatment compared with single-drug therapy. However, 11 of the 61 patients (18%) reported one or more adverse events from polypharmacy at their final visit. Adverse side effects in this sample included weight gain, sedation/tiredness, tics, drooling, self-injury, speech problems, repetitive tongue/mouth movements, and withdrawal dyskinesia. While this is the only study that explicitly describes medication monitoring, information concerning follow-ups for physical health and side effects from other included studies included may have not been discussed or examined explicitly or were not available in the clinical records. Thus, the extent of such monitoring in the other studies included may be underestimated in the current review.
As demonstrated in our review, the most commonly prescribed medication class among autistic youth was stimulant medication, followed by antipsychotics, anticonvulsants or mood stabilizers, and antidepressants. Medications including antidepressants and mood stabilizers are frequently prescribed to youth with autism, despite no significant improvements in autism symptoms, and in some cases pose an additional risk for the development of secondary symptoms (Williams et al. 2011), including hyperactivity, agitation, and aggression (West et al. 2009).
Across studies, males were more often prescribed antipsychotics and stimulants, while females were more often prescribed antidepressants or mood stabilizers. This is consistent with the sex differences found in the use of medications to address mood disorders in the general population. Specifically, females are diagnosed with depression at a 2:1 ratio (female:male), and subsequently treated with antidepressants at a higher rate (Sundbom et al. 2017). As autism affects males four times more often than females (Fombonne 2009; Werling 2016), studies in our review appear to be consistent with this ratio, with ∼82% of males across all 16 studies. However, autistic females may go undiagnosed possibly due to distinct or subtler symptom presentation (Howe et al. 2015). The expression of autism between males and females is also often qualitatively different (Mandy et al. 2012; Lai et al. 2017), with autistic females having fewer externalizing and more internalizing behaviors (Mandy et al. 2012), less restricted interests (Hiller et al. 2014), and fewer repetitive behaviors (van Wijngaarden-Cremers et al. 2014). It has also been suggested that females require more severe symptoms or different symptoms than males to meet the diagnostic criteria for autism (Bargiela et al. 2016). Subsequently, sex differences in the autism phenotype may contribute to biases in the assessment and diagnosis of autism (Kreiser and White 2014). Therefore, the differential prescribing patterns found in our review may be based on sex differences in autism, an emerging area in the literature.
Limitations and future directions
Our results highlight the high prevalence of youth with autism prescribed multiple medications simultaneously, and the substantial gap in the literature outlining appropriate and effective monitoring practices within this population. However, a limitation of this review is the methodological variability of studies, including inconsistent definitions of psychotropic polypharmacy in the existing literature. Although our definition of polypharmacy was determined based on existing literature and guidelines aimed at encompassing all instances and definitions of multiple medication prescribing, our wide range of prevalence of psychotropic polypharmacy is potentially a result of the varying definitions in the field. Second, while the National Association of State Mental Health Program Directors describes types of polypharmacy (e.g., same-class polypharmacy, multiclass polypharmacy, and total polypharmacy), due to limitations in the data of the included studies, we were unable to analyze data as they pertain to these types of polypharmacy. Third, autistic youth are frequently prescribed and utilize nonpsychotropic medications to address common secondary issues (e.g., sleep issues and constipation). While we did not include nonpsychotropic medications in our search terms, many of the studies failed to inquire/outline the degree to which polypharmacy was happening between psychotropic and nonpsychotropic medications—identifying a new area of further research.
Moving forward, longitudinal studies are needed to monitor psychotropic polypharmacy in youth with autism, where researchers examine the types of polypharmacy and onset of medication use, including dosage and the onset of other “side effects” (physiological symptoms) to better understand the relationship between the two. In addition, further investigation into the interaction of psychotropic medications with each other, and the interaction of psychotropic and nonpsychotropic medications between classes should be examined. Lastly, to date, there are no long-term studies demonstrating monitoring of medication use (either mono- or polypharmacy) for autistic children and youth. Where possible, prescribing clinicians should frequently be monitoring if there is a reduction in symptoms using standardized questionnaires or tools, as well as the presence of any adverse side effects determined using a multimethod, multi-informant process (e.g., blood work and interviews with patients and caregivers). Timing and frequency of monitoring will differ based on the client, history of medication and adverse side effects, and prescribing drug. This apparent gap in the literature concerning monitoring practices and follow-up of drug effects for children and youth with autism requires further research.
Conclusion
Autistic youth are a vulnerable and a highly medicated population, and evidence describing effective monitoring practices utilized with psychotropic polypharmacy is limited. To date, there is little empirical evidence supporting the practice of polypharmacy as a means to improve the behavior of children and youth with autism (Li et al. 2017). Consequently, there is a critical need for high-quality research examining the short- and long-term therapeutic, physiological, and behavioral effects of polypharmacy (Li et al. 2017). Importantly, a lack of regulatory body approval (e.g., U.S. FDA approval) does not imply that there is no evidence for the use of specific medications; however, combinations of psychotropic medications to date have not been investigated extensively. Ultimately, these findings highlight the need for prescribing clinicians to take a thoughtful, cautious, and active role in prescribing and monitoring medication use in autistic children and youth.
Clinical Significance
Autistic children and youth are frequently prescribed psychotropic medications to manage both their primary and secondary symptoms. Rates of polypharmacy among children and youth with autism are generally quite high, with only one study documenting effective monitoring practices. Being male and older, as well as presenting with psychiatric co-morbidities, self-injurious behaviours and physical aggression are factors that appear to put someone at heightened risk for being prescribed multiple medications simultaneously. Very little is known about the short and long-term impact of multiple medication use in autistic people, and consequently clinicians should use caution when prescribing psychotropic medications to autistic people.
Footnotes
Acknowledgment
We thank Dr. Johanna Lake for her content expertise and thoughtful feedback in the development of this article.
Disclosures
We wish to confirm that there are no known conflicts of interest associated with this publication, and that there has been no significant financial support for this work that could have influenced its outcome. We are not affiliated to or have any relationships with pharmaceutical companies. This study was not supported by any pharmaceutical company. We confirm that the article has been read and approved by all the named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the article has been approved by all of us. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication, including the timing of publication, with respect to intellectual property. In so doing, we confirm that we have followed the regulations of our institutions concerning intellectual property. We further confirm that any aspect of the work covered in this article that has involved human patients has been conducted with the ethical approval of all the relevant bodies and that such approvals are acknowledged within the article. We understand that the corresponding author (C. McMorris) is the sole contact for the editorial process. She is responsible for communication with the other authors about the progress, submissions of revisions, and the final approval of proofs. We confirm that we have provided a current, correct e-mail address that is accessible by the corresponding author and which has been configured to accept e-mail from.