
Abstract
Objective:
Antipsychotic use among youth is common and is associated with metabolic side effects such as weight gain. Guidelines recommend periodic screening of metabolic measures in youth prescribed antipsychotics; however, a guideline-to-practice gap exists. We systematically reviewed the literature to synthesize the knowledge from interventions that aim to improve antipsychotic metabolic screening. We described the interventions' effect on screening rates, the strategies used for improvement, and study quality.
Methods:
We conducted a systematic review of studies that attempted to improve antipsychotic metabolic risk screening practices among pediatric populations published between 2004 and August 2019. We included studies with an improvement intervention that compared screening rates before and after the intervention. We extracted data about study characteristics, screening rates in pre- and postintervention groups, strategies used to influence screening practices, and assessed studies' risk of bias. This review was prospectively registered with PROSPERO #CRD42018088241.
Results:
We identified six studies that demonstrated modest improvements in median metabolic screening rates for waist circumference (0%–16%), glucose (9%–39%), and lipids (11%–37%). Median postintervention screening rates were higher for weight and blood pressure (84% and 72.5%) compared with glucose and lipids (39% and 37%). Interventions used a variety of improvement strategies to address patient-, provider-, and organization-level barriers for screening, including increasing patient and provider knowledge regarding antipsychotic side effects, fostering social clinical environments that promote screening, and organizational commitment for screening antipsychotic-treated youth. All interventions were deemed at high risk of bias due to uncontrolled design and lack of adjustment for confounders.
Conclusions:
Included studies reported partial success in improving antipsychotic screening rates but were of poor methodological quality. Common improvement strategies may affect provider behavior to conduct metabolic screening, but these need to be tailored to local resources and organization structure. Future studies need to use rigorous methodology and theory-informed improvement strategies aligned with organizational actions to prioritize safe and judicious practice of antipsychotics among pediatric populations.
Introduction
In the 21
Of particular concern are their metabolic side effects, mainly the atypical (i.e., second-generation) class, which can cause obesity, hyperglycemia, and hyperlipidemia (Almandil et al. 2013; Pillay et al. 2018). Relative to adults, youth are more susceptible to metabolic side effects due their ongoing growth and development (De Hert et al. 2011) and as many as 50% will become overweight or obese within 1 year of antipsychotic initiation (Ronsley et al. 2015). To address these concerns, there have been concerted efforts over the past decade to improve the quality of antipsychotic prescribing among youth. Health authorities promoted judicious antipsychotic use by implementing the need for prior authorization (Thackeray et al. 2018), mandatory drug reviews (Barclay et al. 2017), and low barrier access to psychiatric consultations (Crystal et al. 2016; Mackie et al. 2020). To complement these efforts, regulators put in place guidelines that call for metabolic risk screening among youth in receipt of antipsychotics (Findling et al. 2011; Pringsheim et al. 2011). Antipsychotic monitoring guidelines generally follow the consensus statement issued in 2004 by the American Diabetes Association and the American Psychiatric Association (American Diabetes Association et al. 2004) calling for regular screening of anthropometric measurements such as weight, height, waist circumference, and blood pressure (BP) together with glucose and lipid testing. In addition, monitoring for abnormalities in hormonal and extrapyramidal systems is indicated (Pringsheim et al. 2011).
Despite clear recommendations, the clinical uptake of these guidelines is lacking. For example, among Medicaid-insured youth and commercially insured youth, metabolic risk screening rates for glucose and lipids before initiation of antipsychotic treatment were 31% and 13% and 12% and 10%, respectively (Morrato et al. 2010; Delate et al. 2014).
To address the guideline-to-practice gap of antipsychotic metabolic risk screening in youth, researchers delivered interventions that improve the uptake of antipsychotic screening guidelines into clinical practice, however, to date, the literature on this topic has not been systematically reviewed. We aimed to conduct a knowledge synthesis of interventions that aim to improve antipsychotic metabolic risk screening in youth. We identified intervention effects on screening rates, characterized improvement strategies used by the interventions using a theoretical framework, and assessed their methodological rigor. This review aims to summarize existing literature to inform the development of future programs to improve antipsychotic metabolic risk screening among youth.
Methods
Overview
We conducted a systematic review of interventions targeting metabolic screening of youth (age 18 years or younger) taking antipsychotic medications, with the objective of improving screening rates to the level recommended by clinical guidelines. We aimed to describe the various improvement strategies used by the interventions and to assess interventions' effectiveness in increasing metabolic screening rates. This review was written in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al. 2009). As this study is a systematic review of published literature, it did not require an approval of an ethics review board.
Search strategy
Articles published in print or online from January 1, 2004, to August 2, 2019, were identified through systematic searches in MEDLINE (including Epub ahead of print, in-process, and other nonindexed citations), Embase, APA PsycINFO, the Cumulative Index to Nursing and Allied Health Literature, ProQuest Dissertations and Theses Global, and the Cochrane Library using database-specific subject headings and keywords in natural language. The search strategy was developed in collaboration with a research librarian (T.R.) who also executed the searches.
Search terms for the antipsychotics included the MeSH heading “Antipsychotic Agents,” as well as text words “neuroleptic” and specific drug names. Search terms for metabolic monitoring included “metabolic,” “lipids,” “blood glucose” combined with terms such as “monitor,” “screen,” “track.” The practice concept included MeSH headings “Practice Patterns” and “Guideline Adherence,” and text words for monitoring rates, screening practices, and best practice implementation. Search terms and concepts were combined using Boolean logic and operators including proximity searching. These results were then limited to articles where “child” and “adolescent” terms and their synonyms appear in selected fields. Year limits applied were “2004 to present,” and no language limits were applied. The Medline search strategy can be found in Supplementary Appendix SA1. Reference lists of chosen articles and documents were also hand searched to identify any relevant resources not captured by the systematic searches.
Title and abstract screening was conducted independently by two reviewers (O.C.M., L.R.L.) and was followed by a full-text screen against a priori inclusion criteria as registered in PROSPERO, systematic review registry, CRD42018088241. Disagreements between reviewers were brought to discussion in face-to-face meetings. References in question were then reassessed by the two reviewers and each reviewer provided feedback into the decision. Following a careful review of the references and discussion, the reviewers would then reach a consensus regarding the reference in question.
Criteria for study selection
Inclusion criteria
We included interventions aiming to improve metabolic risk screening of youth (age 18 years or younger) taking antipsychotic medication. Eligible interventions targeted screening practices of at least one of four metabolic measures: (1) obesity—weight, body mass index (BMI), or waist circumference, (2) glucose —blood glucose or glycated hemoglobin (HbA1c), (3) lipids—total cholesterol, low-density lipoprotein (LDL)-cholesterol, high-density lipoprotein (HDL)-cholesterol, or triglycerides, and (4) BP. Studies were neither restricted to a minimum duration of intervention nor to a specific psychiatric diagnosis or type of antipsychotic medication used. We included all available study designs in any setting to identify the full breadth of available literature. When studies reported metabolic screening rates at multiple time points postintervention, we considered the latest time point available.
Exclusion criteria
We excluded studies describing interventions for adults only, as well as studies addressing metabolic screening of psychiatric medications other than antipsychotics (e.g., mood stabilizers, antidepressants).
Data extraction and classification
Two authors (O.C.M. and L.R.L.) independently extracted data following criteria outlined in the “Cochrane Handbook for Systematic Reviews of Interventions” (Higgins and Green 2011). The following data were extracted: description of study populations, study setting, study design, and rates of metabolic screening before and after the intervention. Strategies used by the intervention to improve metabolic risk screening (i.e., improvement strategies) at the levels of the patient, provider, and system were extracted as these have been found to influence the uptake of clinical guidelines (Kennedy et al. 2007).
Outcome measures
Primary outcome measures included metabolic screening rates for: (1) obesity—weight, BMI, or waist circumference, (2) blood glucose—blood glucose or HbA1c, (3) blood lipid measure—total cholesterol, LDL-cholesterol, HDL-cholesterol, or triglycerides, and (4) BP in the pre- and postintervention groups. Secondary outcome measures included the type of improvement strategies used in each intervention to influence monitoring rates at the provider, patient, and system levels.
Quality assessment
To appraise studies' internal validity, we assessed their risk of bias using the Effective Public Health Practice Tool (EPHPP) (Thomas et al. 2004). The EPHPP includes the following six domains: (1) sample selection, (2) study design, (3) identification and treatment of confounders, (4) blinding of outcome assessors and participants, (5) reliability and validity of data collection methods, and (6) withdrawals and dropouts. Each domain is rated according to a standardized guide and given a rating of 1-strong, 2-moderate, or 3-weak. Once all domains have been assessed, the study is rated according to the number of domains with a weak rating: strong (no weak ratings), moderate (1 weak rating), or weak (2 or more weak ratings). Two authors (L.R.L., B.G.O.) conducted the quality assessment with discrepancies resolved by discussion.
Data analysis
Study characteristics and quality assessments are summarized in the tables. Quantitative data were summarized regarding screening rates of four metabolic indices (1-obesity measures, 2-glucose measures, 3-lipid measures, and 4-BP measures). Median screening rates before and after the intervention were calculated using Microsoft Excel. Qualitative data regarding the strategies used by the intervention to improve screening rates (i.e., improvement strategies) were organized into three categories according to their level of action at the patient, provider, and system level and anchored within the Theoretical Domains Framework, which is commonly used to describe theoretical constructs associated with change in provider behavior (Atkins et al. 2017). Improvement strategies at the provider level included increasing knowledge and skills required to perform metabolic screening and also facilitating memory and attention processes that enable providers to embed screening into their routine. Improvement strategies at the system/organization level included the following: (1) social influences, which are interpersonal processes that shape one's feelings, thoughts, and behavior, (2) professional role, which is defined as social norms or group identity influenced by organization values and leadership, and (3) environmental resources, which point to circumstances in one's environment that encourage or discourage the development of skills and abilities for monitoring (Supplementary Appendix SA2) (Atkins et al. 2017). Two authors (O.C.M., L.R.L.) initially identified the improvement strategies and in an iterative process, the research team met several times to analyze and identify these strategies in the studies using a consensus model (Creswell and Miller 2000).
Results
Characteristics of included studies
Our initial search resulted in 747 citations, of which 21 were selected for full-text review (see Fig. 1 for additional details). Seven articles met the inclusion criteria. We considered the articles by Cotes et al. (2015, 2017) one as the latter is a long-term follow-up of the former. Figure 1 contains a flowchart of the search process and study selection according to the PRISMA guidelines (Moher et al. 2009). The characteristics of the six included studies are summarized in Table 1. All included studies were conducted in mental health care systems. Two were conducted in inpatient settings (Pasha et al. 2015; Washington 2017) and four in outpatient settings (Ronsley et al. 2012; Cotes et al. 2015; Carpenter 2018; Featherston et al. 2018). Four studies originated in the United States (Cotes et al. 2015; Washington 2017; Carpenter 2018; Featherston et al. 2018), one in Canada (Ronsley et al. 2012), and one in the United Kingdom (Pasha et al. 2015). All included studies were designed as clinical audit cycles with comparison between pre- and postintervention screening rates. All six studies were published between 2012 and 2018, four of which were reported between 2017 and 2018 (Cotes et al. 2017; Washington 2017; Carpenter 2018; Featherston et al. 2018). Four were published as peer-reviewed articles (Ronsley et al. 2012; Cotes et al. 2015; Pasha et al. 2015; Featherston et al. 2018) and two were dissertations (Washington 2017; Carpenter 2018).
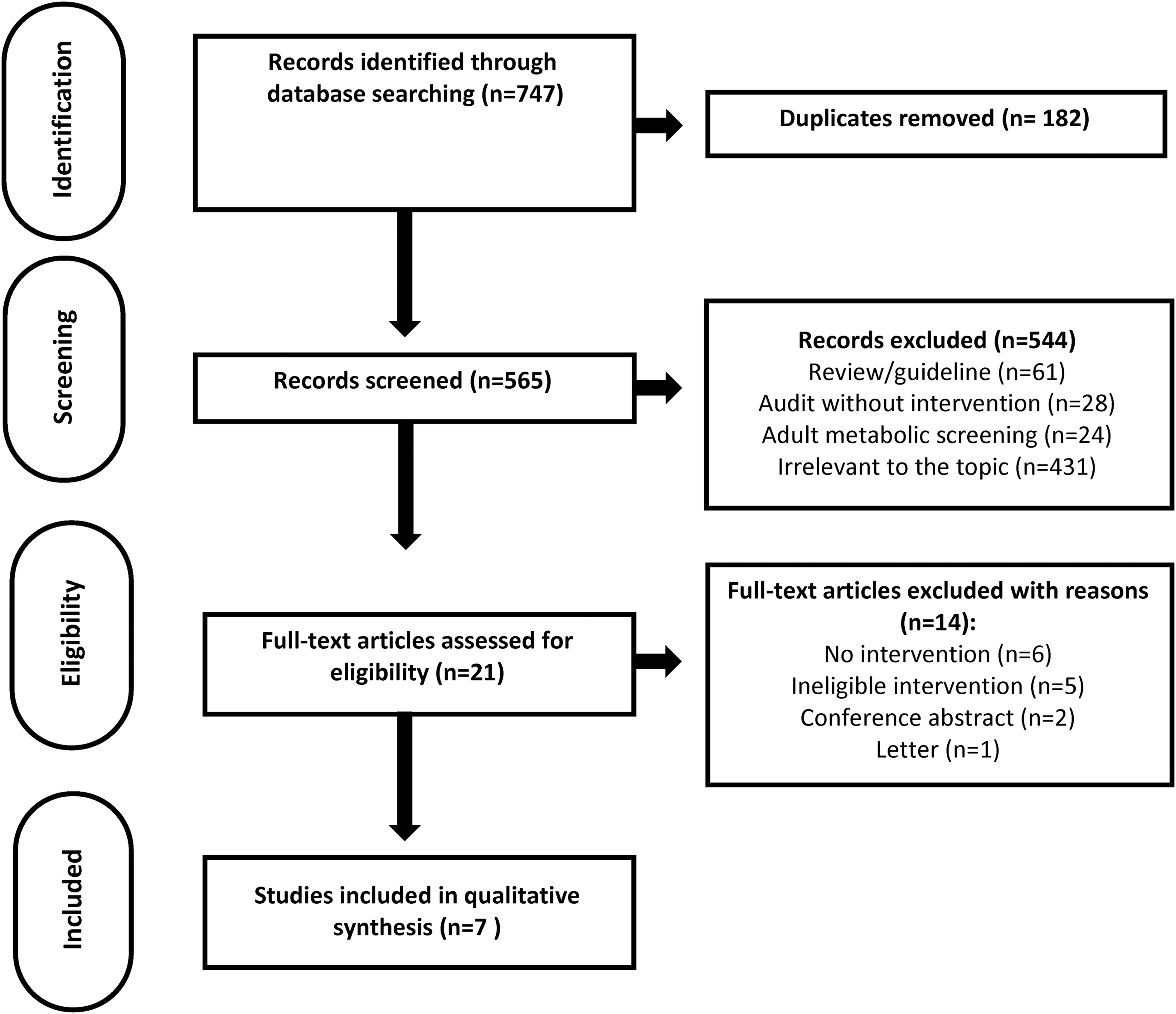
Flowchart of the search process and study selection according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Characteristics of Studies Aimed to Improve Metabolic Risk Screening Among Youth Prescribed Antipsychotics
The Cotes et al. (2015, 2017) articles were considered one study as the latter is a long-term follow-up of the former.
AAP, atypical antipsychotic; ADHD, attention-deficit/hyperactivity disorder; AP, antipsychotic; BMI, body mass index; BP, blood pressure; MH, mental health; MMTP, Metabolic Monitoring Training Program; PCP, primary care providers; PDD, pervasive developmental disorders; QIP, quality improvement program; WC, waist circumference.
Intervention effects on metabolic risk screening
Four studies targeted all of the recommended metabolic measures, including obesity, glucose, lipids, and BP (Ronsley et al. 2012; Cotes et al. 2015; Carpenter 2018; Featherston et al. 2018), while two studies lacked measurement of BP (Pasha et al. 2015; Washington 2017). All studies saw improvements, some of which were statistically significant, in the rates of the targeted metabolic measures (Table 2). Waist circumference was the measure with the lowest postintervention screening rate (16%).
Pre- and Postintervention Screening Rates for Metabolic Indices in the Included Studies
Studies that reported a significant change in screening rates between pre- and postintervention groups.
BMI, body mass index; BP, blood pressure; WC, waist circumference.
Categorization and description of improvement strategies
Studies used different improvement strategies to influence metabolic risk screening practices at the patient, provider, and system levels (Table 3). Studies provided patients and families with education regarding metabolic side effects of antipsychotic medication and called for scheduled monitoring both in oral (Cotes et al. 2015) and written (Carpenter 2018) forms. All six studies provided education to providers on antipsychotic risk screening, while delivery format, content, and intensity varied. Both in-person and written educational activities were used. One study used electronic newsletters (Cotes et al. 2015) and another provided a physician handbook (Ronsley et al. 2012). Intensity of educational sessions ranged from single (Pasha et al. 2015) to multiple sessions (Ronsley et al. 2012) and some were embedded into routine weekly staff meetings (Featherston et al. 2018). A number of studies included skill training for providers in the measurement of metabolic parameters in children (Ronsley et al. 2012; Carpenter 2018; Featherston et al. 2018). Most studies added a paper template to the charts of patients prescribed an antipsychotic medication to remind providers to conduct metabolic screening and to record which screening has been done to date (Ronsley et al. 2012; Pasha et al. 2015; Carpenter 2018; Featherston et al. 2018). Two of the studies reported on mental health organizations' commitment to perform metabolic risk screening by using dedicated quality improvement teams (Ronsley et al. 2012; Featherston et al. 2018), which oversaw the implementation of screening into practice. One study reported on quality improvement teams that specifically educated leaders in both the health system and managers in mental health organizations (Cotes et al. 2015). All studies used social influences to shift providers' practice, however, these varied between the interventions. Examples included: designating a “clinician champion” for screening (Washington 2017), letters sent by leaders in the organization to encourage screening (Cotes et al. 2015), creating a task log in which each clinician had a designated role in the screening practice (Ronsley et al. 2012; Carpenter 2018), and meetings with influential colleagues who advocate for screening (Ronsley et al. 2012). Lastly, four of the studies assessed barriers to screening practices (Pasha et al. 2015; Washington 2017; Carpenter 2018; Featherston et al. 2018), and two studies conducted rapid improvement cycles of plan-study-do-act (Pasha et al. 2015; Carpenter 2018), allowing recurrent assessment of barriers and rapid iteration of procedures to overcome identified barriers.
Improvement Strategies Used by Interventions to Influence Metabolic Risk Screening at the Levels of Patient, Provider, and System
Professional role is defined as social norms or group identity influenced by organization values and leadership. Social influences are interpersonal processes that shape one's feelings, thoughts, and behavior. Environmental resources which point to circumstances in one's environment that encourage or discourage the development of skills and abilities for monitoring (Atkins et al. 2017).
Quality assessment of included studies
We rated all included studies as “weak” quality. All were designed as uncontrolled audit cycles in which a comparison between preintervention and postintervention screening rates occurred. No studies reported adjustments for confounders known to influence monitoring rates such as age or mental health diagnosis (Morrato et al. 2010; Edelsohn et al. 2015). A summary of the EPHPP quality assessment tool results is provided in Table 4.
Quality Assessment of the Included Studies
Each of the six domains (selection, design, cofounders, blinding, data collection, withdrawal) is rated according to a standardized guide as 1-strong, 2-moderate, or 3-weak.
Each study is given a global rating according to the number of domains with a weak rating. Studies without any weak domains are rated strong, studies with 1 weak domain are rated moderate, and studies with 2 or more weak domains are rated as weak.
NA, not applicable.
Discussion
Summary of main findings
This review identified six studies reporting on interventions to improve antipsychotic metabolic risk screening among youth. Interventions increased median screening rates for metabolic measures, including glucose, lipids, weight, and BP and to a lesser extent waist circumference. Nevertheless, median screening rates remained below 40% for lipids, glucose, and waist circumference. High risk of bias due to uncontrolled pre/post design and lack of adjustment for confounders limit our ability to draw firm conclusions regarding the effect of the interventions. All studies educated providers about metabolic risk screening and also used social influences to shift providers' practice. Organizational commitment evidenced by the use of quality improvement teams holds promise to provide adequate support for narrowing the guideline-to-practice gap, however, additional rigorous studies on the topic are needed.
Interpretation of main findings in the context of available literature
Guidelines call for periodic screening of metabolic measures in youth prescribed antipsychotic medications, including weight, height, waist circumference, BP, blood glucose, and lipids (Findling et al. 2011; Pringsheim et al. 2011). Preintervention screening rates in the studies reviewed here were consistent with the low rates reported in the literature, and hence, the impetus to conduct improvement interventions. For example, screening for lipids among the six included studies had a median rate of 14%, which is comparable with 13% and 10% found in previous samples (Morrato et al. 2010; Delate et al. 2014). The interventions reported improvements in screening rates (Table 2), however, postintervention median screening rates remained suboptimal for glucose, lipids, and waist circumference (39%, 37%, 16%, respectively). Interventions had more success in increasing screening of anthropometric measures with postintervention median rates of 84% for weight and 72.5% for BP. This could be explained by the relative ease of obtaining “in-house” anthropometric measures (no need to visit a laboratory) and their acceptability by both providers and patients. Conversely, glucose and lipid screening, which necessitates venous puncture in a fasted state, may have been less feasible for patients and families; this has also been reported by others (Walter et al. 2008; McLaren et al. 2017). Of note, waist circumference demonstrated the lowest postintervention median screening rate (16%). This is of concern as waist circumference is the most sensitive anthropometric measure correlating with degree of metabolic risk (Panagiotopoulos et al. 2012). Given the partial success of interventions in increasing metabolic risk screening, additional studies are needed to further narrow the guideline-to-practice gap, particularly those that address patient-level barriers and barriers for waist circumference measurements.
Previous reports have described several barriers for metabolic risk screening among youth, such as limited knowledge on how to conduct physical measurements (Rodday et al. 2015), particularly among providers in nonacademic settings and those who have long been out of medical training (McLaren et al. 2017). Fragmentation of mental health and primary care services is also a concern, where providers are reluctant to screen in the absence of resources for the management of metabolic abnormalities (Ronsley et al. 2011). Nonadherence of youth and their families with recommended blood testing due to fear and inconvenience of fasting samples poses an additional challenge (Walter et al. 2008; McLaren et al. 2017). Using a theoretical framework for behavior change (Atkins et al. 2017), we identified improvement strategies used by each study to address known barriers at the levels of the patient, provider, and system (Table 3). All studies increased provider knowledge with educational activities and some improved skills by providing “hands on” training on how to conduct anthropometric measurements (Ronsley et al. 2012; Carpenter 2018; Featherston et al. 2018). Some addressed patient and family concerns by providing education and written materials (Cotes et al. 2015; Carpenter 2018), supporting families' health literacy and informing better decision-making relating to the use of antipsychotics (Xu et al. 2012). Studies also targeted providers' memory and attention processes by including paper monitoring tools in patients' charts, which allows for quick recall of recommended monitoring and to assess the need for testing at any given time. Similarly, electronic “pop-up” prompts for monitoring, which appear at the time of antipsychotic prescribing, have been successful in improving monitoring among adults (Melamed et al. 2019). Studies used organization- and system-level approaches to shift provider behavior. One of these included social influences by organization leaders, who sent electronic newsletters to providers to encourage screening (Cotes et al. 2015) as well as appointing clinician “champions” for monitoring in clinical teams (Washington 2017). The dedication of internal staff and the seeking of an external consultant to support screening practices speak to a shift in the professional role and to an organizational commitment to prioritize metabolic health among antipsychotic-treated youth (Ronsley et al. 2012; Cotes et al. 2015; Featherston et al. 2018). To address providers' concerns that metabolic abnormalities identified by screening will be left untreated, interventions linked screened youth with local resources to treat these abnormalities. For example, one study collaborated with colocated primary care services (Featherston et al. 2018), and another provided “in-house” health coaching for physical activity and healthy diets (Washington 2017). We recommend that future metabolic risk screening programs use sound theoretical frameworks to address known barriers for monitoring and include sufficient resources to advise families on healthy active living, as well as primary or specialist care for prompt pharmacological management of metabolic abnormalities.
The paucity of published studies and their low methodological rigor point to the emerging nature of this topic in the literature. We found six studies, all of which used an uncontrolled design where preintervention and postintervention screening rates were compared. Studies did not adjust for potential confounders such as age despite evidence suggesting younger children are less likely to be screened compared with older ones (Edelsohn et al. 2015). These factors contribute to the high risk of bias, which prevents us from reliably assessing the true effect of the interventions on metabolic screening rates and hinders our ability to point to the superiority of one improvement approach over another. Quality improvement studies are rarely performed in traditional “rigorous” designs such as randomized-controlled trials, however, recent advancements in their methodology allow researchers to increase their credibility (Poots et al. 2017). For example, the use of interrupted time series analyses, cluster randomized trials, and explanatory models grounded in theoretical frameworks (Ralston et al. 2019) could address the methodological shortcomings seen in the studies reviewed here, including pre/post design, and short-term duration (<12 weeks). The use of interrupted time series analyses, for example, could be especially beneficial to assess the uptake of interventions over the long term. Indeed, one study that assessed the effect of the intervention over time found that its effect waned as time from the intervention elapsed (Ronsley et al. 2012). Future studies, using improved methods, are needed to enhance the available knowledge base of effective interventions targeting the practice of antipsychotic metabolic risk screening.
While antipsychotics are associated with a myriad of metabolic abnormalities, not all youth are affected in a similar manner. Evidence suggests that prepubertal children are more susceptible to weight gain compared with adolescents (Martinez-Ortega et al. 2013). Genetic differences in histaminergic (H1) and serotonergic (5-HT2) neurotransmission also account for differential weight gain (Roerig et al. 2011). In addition, social disadvantage is linked with unhealthy behaviors and obesity even before initiation of antipsychotic medication (Greves Grow et al. 2010). Hence, future metabolic risk screening programs should provide greater attention to screening, prevention, and management of metabolic risk among disadvantaged youth, who are overrepresented among antipsychotic-treated youth, by using evidence-based interventions (Nicol et al. 2016). Additional research is needed to improve our understanding of the interplay between biological, social, and environmental factors influencing metabolic risk in youth prescribed antipsychotics. This new knowledge will facilitate a reduction of screening requirements for youth deemed at low risk for metabolic complications and conversely increase surveillance and preemptive measures for those at high risk.
Metabolic risk screening is one of a number of antipsychotic “quality concepts” recently described in the literature (Kealey et al. 2014). Other concepts include the following: (1) use in children younger than the age of 6 years, (2) antipsychotic polypharmacy, (3) high doses of antipsychotics, (4) off-label use, and (5) first-line psychosocial interventions. The past few years have seen a proliferation of studies aiming to improve the quality of antipsychotic prescribing in pediatric populations and limit unnecessary use. For example, a statewide initiative granted community providers with low-barrier telephone access to consultations with child and adolescent psychiatrists before antipsychotic prescribing (Barclay et al. 2017). In another study, prescription of antipsychotics among young children or at higher than recommended doses triggered a medication review (Mackie et al. 2020). Similarly, a Medicaid quality improvement collaborative used a multistrategy approach to promote safe and effective prescribing of antipsychotics and improve access to nonpharmacological behavioral health services, which yielded a 25% reduction in antipsychotic prescribing (Thackeray et al. 2018). These efforts have been conducive to the judicious practice of antipsychotic prescribing in which a reduction in prescribing for behavioral conditions was seen without a concomitant decrease in prescribing for psychotic disorders. Some of the aforementioned approaches led to improvements in metabolic risk screening, and on average, a third of all youth were screened for glucose and lipids (Olin et al. 2019; Mackie et al. 2020) similar to the postintervention rates found in this review. To increase metabolic risk screening, there is an urgent need to integrate interventions such as those reviewed here into larger systemic efforts that promote high-quality use of antipsychotics in pediatric populations. It would be advantageous to anchor these actions within local health policies. Of note, these systemic efforts are in line with health authorities and insurers' interest of cost-containment as ∼30% of pediatric pharmaceutical expenditure is attributed to antipsychotic medications (Cohen et al. 2017) as well as excess health care utilization among antipsychotic-treated youth (Sikirica et al. 2012).
Limitations
As in any review, it is possible relevant studies were missed. We attempted to mitigate this through a broad literature search carried out in multiple databases by a specialist librarian. As our preliminary database search yielded a small number of studies, we decided to include dissertations in this review (two out of the six studies). Evidence from nonpeer-reviewed studies is deemed to be of lower quality compared with peer-reviewed studies, further limiting our ability to draw firm conclusions regarding the interventions' effect. The analysis of improvement strategies through qualitative inquiry has inherent limitations of researchers' bias. To address this, we followed recommended advice to guide the analysis process (Cypress 2017).
Clinical Significance
Antipsychotic use among children and adolescents is common and may lead to metabolic abnormalities, such as weight gain. However, only a minority of youth are screened for metabolic side effects of antipsychotics, as recommended by clinical guidelines (Findling et al. 2011), thus missing out on opportunities to mitigate or reverse them. Metabolic abnormalities in youth are a precursor for cardiovascular disease and place youth at risk for premature morbidity and mortality in adulthood (Tirosh et al. 2011). The knowledge synthesized in this review of interventions aiming to improve antipsychotic metabolic risk screening among youth provides a mixed-method inquiry, which describes the effect of the intervention on screening rates and characterizes the improvement strategies used by the interventions to influence screening practices at the levels of the patient, provider, and system. For example, strategies included the use of patient and provider education, social influences within providers' work environment to encourage screening, and the use of tools to capture providers' attention to monitoring. This knowledge could inform the development and implementation of future antipsychotic metabolic risk screening programs into clinical care. In particular, an organizational commitment for monitoring of antipsychotic side effects and a shift in organization “culture” to prioritize screening have been shown to influence screening practices in adult mental health services (Melamed et al. 2019). Lastly, it is important to keep in mind that screening for metabolic side effects of antipsychotics is only one aspect of high-quality antipsychotic prescribing (Kealey et al. 2014), which ideally should be incorporated into larger systemic efforts, including health policies, that promote judicious use of these agents in pediatric populations.
Conclusions
The literature describing interventions aimed to increase antipsychotic metabolic risk screening among youth is scarce and of low quality. The studies reviewed here point to modest improvements in screening rates for glucose, lipids, and waist circumference with suboptimal screening postintervention. Included studies lacked scientific rigor, highlighting the importance of subsequent studies to use sound methodology to provide reliable and replicable evidence on how to improve antipsychotic screening. While provider education and clinical tools aiding in monitoring may be helpful, significant improvements in antipsychotic metabolic screening are likely to be seen when health organizations are committed to deliver high-quality and judicious practice of antipsychotic prescribing alongside a commitment to conduct metabolic screening among antipsychotic-treated youth.
Footnotes
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Appendix S1
Supplementary Appendix S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.