
Abstract
Objectives:
Numerous studies have examined determinants contributing to methylphenidate adherence and persistence, but these were mainly conducted in adults. These determinants are likely to be different in children as they usually rely on their parents to provide them with the care they need. The objective was to study child and family characteristics as determinants of methylphenidate adherence and persistence in children.
Methods:
The study population consists of 307 children from the Generation R Study in the Netherlands, who had at least one dispensing record of methylphenidate until the age of 16 years. Adherence was defined as a medication possession ratio ≥0.80 up to 2 years after treatment initiation. Persistence was defined as the duration of treatment until a discontinuation period of ≥6 months. Family and child characteristics were tested as determinants of adherence with multivariable logistic regression analysis. Persistence was evaluated using a Kaplan–Meier analysis.
Results:
Children of mothers with one child (adjusted odds ratio [OR]: 2.31, 95% confidence interval [CI]: 1.17–4.54) or of mothers with an average household income (compared to high) were more likely to be adherent (adjusted OR: 3.45, 95% CI: 1.43–8.31). Children who started treatment at the age of 12–16 years (compared to <12 years) (adjusted hazard ratio [HR]: 3.55, 95% CI: 2.54–4.98) and girls (adjusted HR: 1.44, 95% CI: 1.07–1.95) were more often nonpersistent.
Conclusion:
Both child and family characteristics may play a role in methylphenidate treatment adherence. Furthermore, gender and the start age of treatment were found to be associated with nonpersistence. These findings may be important for health care professionals when initiating methylphenidate treatment in children.
Introduction
Methylphenidate is the first-line pharmacological treatment option for attention-deficit/hyperactivity disorder (ADHD) as it is considered to have the best balance between safety and effectiveness in children (Cortese et al. 2018). However, for medication to be effective, compliance to treatment is crucial. Two important aspects of compliance are reflected by adherence and persistence. Adherence refers to the extent to which patients take medications as prescribed and persistence refers to continuing treatment for the prescribed duration. Various studies have shown that both adherence and persistence to stimulant medication in children and adolescents are only 40%–50% (Adler and Nierenberg 2010; Barner et al. 2011).
Many studies investigating factors that influence adherence and persistence were performed in adolescents and adults, whereas limited information is available in children (Semerci et al. 2016; Skoglund et al. 2016). These studies showed that adults with a high education, a family history of ADHD, and higher doses of methylphenidate were more likely to be adherent. Furthermore, another previous study in adults examined different sociodemographic factors that may contribute to adherence and persistence of methylphenidate treatment and showed that male gender and a lower educational level were associated with discontinuation (Sobanski et al. 2014).
To investigate treatment adherence and persistence in children, it is important to also consider parental involvement as there are many parental factors that may contribute, such as socioeconomic status and ethnicity (Nagae et al. 2015).
A previous study that included 27 parents of children with ADHD, who were given a stimulant treatment recommendation, showed that parents described deeply ambivalent feelings about medication. Parental fear for side effects, inadequate family support for the decision to start medication, and parental guilt fueled by social pressure were described as factors that may influence parent decisions to follow ADHD treatment recommendations (Coletti et al. 2012). Consequently, this may influence child adherence and persistence of methylphenidate as parents are supposed to encourage children to continue to take their medication. However, the number of patients included in that study was small and family or patient characteristics influencing treatment acceptance were not investigated. For example, the age at treatment initiation may play a role as adolescents usually manage their own medication intake and could be more likely to forget or abstain from medication (Hugtenburg et al. 2006).
For school-aged children, parents usually make treatment decisions and have a greater influence on adherence and persistence of medication. Studies also showed that medication adherence was greater when both children and parents felt that symptoms improved with treatment (Gau et al. 2006; Nagae et al. 2015; Skoglund et al. 2016). The adherence and persistence may also be dependent on the dosage and the number of pills they have to take on a daily basis (Gau et al. 2006; Nagae et al. 2015; Skoglund et al. 2016).
Finally, many studies have assessed adherence and persistence separately (Miller et al. 2004; Hugtenburg et al. 2006; Gajria et al. 2014; Wang et al. 2016). It is important to assess adherence together with persistence, as they both are important aspects of adequate pharmacotherapy. For this reason, the objective of our study was to determine adherence to and persistence of methylphenidate treatment in children and to study potential determinants that were associated with these outcomes.
Methods
Study population
This study was conducted within the Generation R Study, a large population-based cohort study investigating children's health from fetal life onward in Rotterdam, the Netherlands (Kooijman et al. 2016). All pregnant women from Rotterdam with a delivery date between April 2002 and January 2006 were asked to participate in the study. Detailed and extensive data have been collected over the years, which included interviews, questionnaires, and behavioral observations of children and their parents (Kooijman et al. 2016). In addition, pharmacy records of the children from community pharmacies from Rotterdam were retrieved.
In this study, all children (n = 7986) and their parents were invited to participate in the follow-up study. Children were excluded if parents withdrew from the study (n = 74), if no consent by parents was provided to retrieve the pharmacy records (n = 1084) or if the pharmacy did not consent to retrieve the pharmacy records (as they had to provide us access to their system), or because no pharmacy records were available in the pharmacy database (which may include nonusers) (n = 1742). For 5068 individuals in The Generation R Study, all prescriptions that were filled at their pharmacy during the entire study period were gathered. Of these, 6% (n = 307) of children received at least one methylphenidate prescription and formed the study population (Fig. 1 for flowchart).
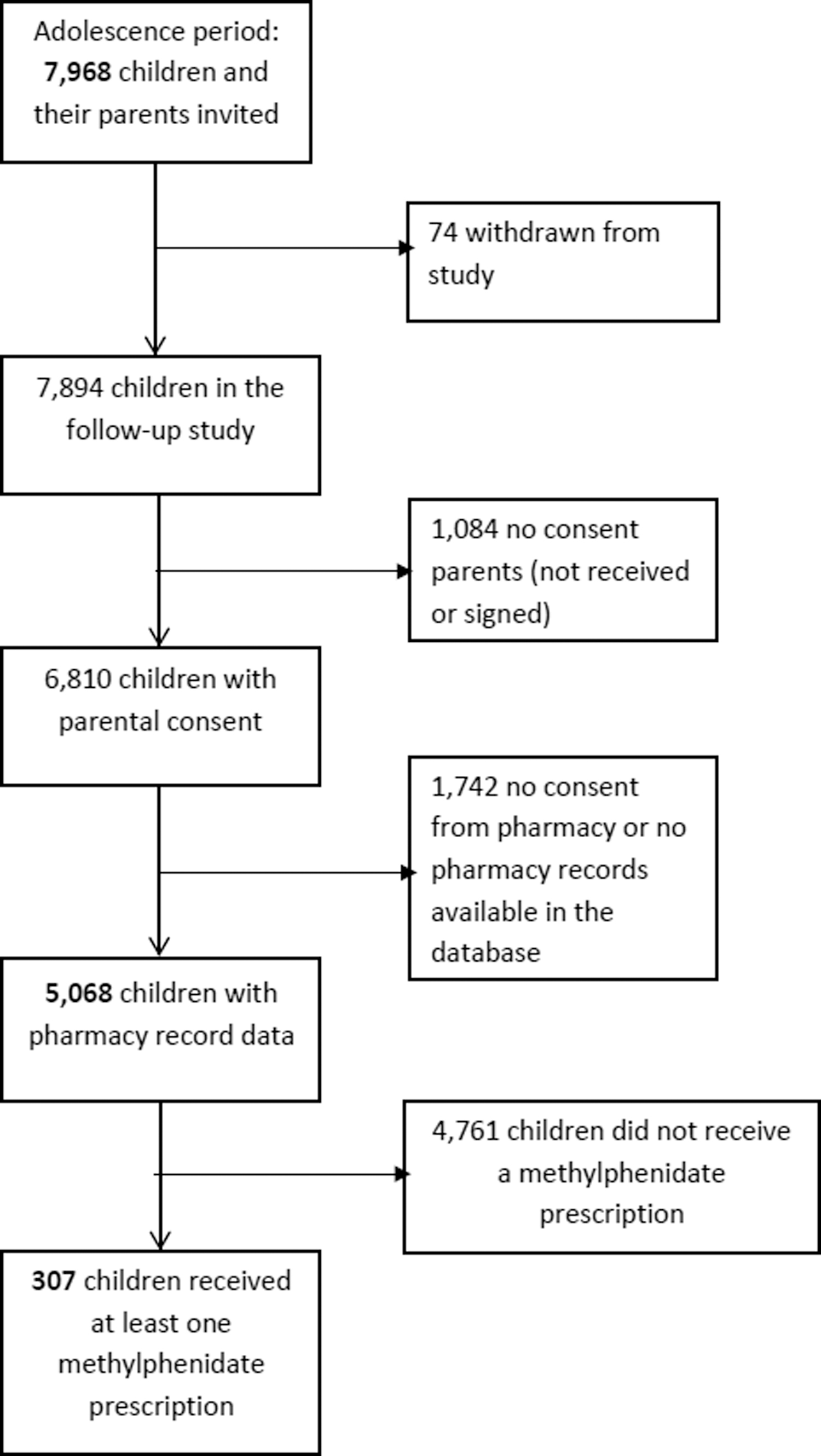
Selection of the study population.
We only focused on methylphenidate use in children, because it is by far the most frequently prescribed ADHD medication and the number of other ADHD medications was low (n = 4). All methylphenidate-using individuals were followed as of their first prescription until (i) the end of the study period at October 30, 2018, (ii) loss to follow-up, or (iii) end date of the last methylphenidate prescription, whichever came first.
Pharmacy records
Linkage between pharmacy records and Generation R participants was done at the community pharmacies in Rotterdam, but the information on methylphenidate use was extracted from automated pharmacy records, which was provided by the Dutch Foundation for Pharmaceutical Statistics (2019). For each dispensation, we collected the product name, Anatomical Therapeutic Chemical (ATC) code (WHO Collaborating Center for Drug Statistics Methodology 2016), date of filling, number of delivered tablets/capsules, and prescribed daily number. A methylphenidate dispensation was selected based on the ATC code N06BA04.
Methylphenidate use
Adherence was measured by the medication possession ratio (MPR), which measures the percentage of time a patient has access to medication. The MPR was only calculated when children received at least two prescriptions of methylphenidate. The MPR is the sum of days' supply of methylphenidate during the follow-up period divided by the number of days in the time period, that is, between the first prescription and the end of the last prescription. According to international literature, a good adherence is set at an MPR of 0.80 or higher (Adler and Nierenberg 2010; Rolnick et al. 2013).
Persistence of methylphenidate was calculated for all children who received at least one prescription of methylphenidate. Currently, there is no clear definition of nonpersistence of methylphenidate treatment. In general, a gap period of 15–180 days is used as nonpersistence as shown in previous studies (Miller et al. 2004; Wang et al. 2016). Prescriptions for methylphenidate in the Netherlands are generally filled for 3 months. To ensure that no methylphenidate was dispensed after that, a gap period of 6 months (without prescription) was chosen as nonpersistence. Nonpersistence was calculated starting from the calculated end date of the last prescription.
In addition, we collected information on the type of methylphenidate prescriber (medical specialist [pediatrician or child psychiatrist], general practitioner), as well as prescriptions of other psychotropic medication before the first methylphenidate dispensation, including antiepileptics (ATC code N03A), antipsychotics (N05A), anxiolytics (N05B), hypnotics and sedatives (N05C), antidepressants (N06A), or other ADHD medications (N06BA, such as dexamphetamine and atomoxetine). We included the number of times the prescription was switched from short-acting methylphenidate to long-acting methylphenidate or vice versa and the number of prescriptions of short- or long-acting methylphenidate (number of long-acting prescriptions greater than short acting or number of short-acting prescriptions greater than long acting).
Child characteristics and other determinants
Child characteristics that were considered determinants of adherence include age at first methylphenidate prescription (5–11 and 12–16 years), gender, ethnicity (Dutch/other Western included European, American Western, Asian Western, and Oceanian and non-Western included Turkish, Moroccan, Surinamese, Antillean, Cape Verdean, African, Asian, South American, and Central American) (Migrants in the Netherlands [Allochtonen in Nederland] 2004), and the presence of ADHD symptoms or other emotional and behavioral problems as reported by mothers using the Child Behavior Checklist (CBCL) (Chen et al. 1994; Achenbach and Dumenci 2001). The CBCL (CBCL/1.5–5 and CBCL/6–18) was used to obtain information about behavioral and emotional problems in children (Chen et al. 1994). The CBCL questionnaire has been filled out by the mother when the child was 3, 5, and 9 years old. The CBCL/6–18 was only used at the 9 years of age assessment.
For the analyses, we used the most recently completed questionnaire before the first methylphenidate prescription. The CBCL contains items on the child's behavioral and emotional problems, which are scored on a three-point scale (0 = not true, 1 = somewhat or sometimes true, and 2 = very or often true) during the preceding 2 months. There are five Diagnostic and Statistical Manual of Mental Disorders (DSM)-oriented scales: affective problems, anxiety problems, pervasive developmental problems, ADHD, and oppositional defiant problems. It has been reported that these DSM-oriented scales provide accurate and supplementary information on clinical diagnosis with good reliability and validity for the CBCL (Kim et al. 2005; Alegria et al. 2008).
We also measured the level of ADHD symptoms using the revised Conner's' Parent Rating Scales (CPRS-R), which was filled out by the primary caregiver at the age of 7–8 years. The CPRS-R consisted of 27 items that yielded several subscales: ADHD combined, ADHD Inattentive, ADHD Hyperactive-impulsive, and Oppositional Defiant Disorder (ODD) Scale (Conners et al. 1998). The score ranges from 0 to 18 for the ADHD inattentive, hyperactive-impulsive, and ODD subscales and a possible score between 0 and 36 for the ADHD combined scale. Higher scores indicate more problems.
Autistic traits were assessed using the Social Responsiveness Scale (SRS) short form (Constantino and Todd 2000; Roman et al. 2013). Each item is rated from 0 to 3 (never true to almost always true), covering social, language, and repetitive behaviors. We used a cutoff defined as the upper 15% for the presence of autistic traits.
Family characteristics
We considered several family characteristics as potential determinants for adherence in children: parity (1, >1), marital status (married, living together, no partner), maternal education (no or primary education, secondary education, and high education), and household income (low: less than or equal to €2000; high: greater than €4000; and moderate: €2100–4000). The demographic data were obtained using self-reports.
Analysis
Characteristics of the study population were presented for all methylphenidate users with regular summary statistics.
First, determinants for adherence (MPR ≥0.80) to methylphenidate up to 2 years of follow-up (after receiving their first prescription) were assessed using logistic regression analyses to calculate odds ratios (ORs) and their 95% confidence interval (CI). For all determinants, we tested their independent association with adherence. Then, a multivariable logistic regression model was performed with all relevant determinants and confounders based on the literature (age, gender, ethnicity, type of prescriber, other psychotropic medication, number of short-acting and long-acting methylphenidate, number of switches between short- and long-acting formulations, parity, marital status, maternal education, and household income) (Miller et al. 2004; Gau et al. 2006; Safavi et al. 2019) to assess the association with adherence up to 2 years.
Second, to evaluate the extent of medication nonpersistence between a low (<0.50), moderate (0.50–0.79), and high MPR (≥0.80), we used unadjusted Kaplan–Meier curves. Statistically significant differences in methylphenidate persistence among children with an MPR <0.50, an MPR 0.50–0.80, and an MPR ≥0.80 were identified using Wilcoxon tests. An extended Cox proportional hazards model was used to assess the risk of nonpersistence adjusting for determinants.
Missing data of the determinants (ethnicity, type of prescriber, parity, marital status, and household income) were imputed using multiple imputation (n = 5) (van Buuren 2018). Missing data were only imputed if <30% of the specific variable was missing. Data of the child's behavioral characteristics (CBCL, SRS, and CPRS-R) were not imputed. These characteristics were assessed as determinants in the univariable analysis, but they were not included in the multivariable analyses. Results were considered statistically significant at p < 0.05. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY).
Results
Characteristics of study population
The characteristics of the study population and information about the dispensed medications are shown in Table 1. The mean age on the date of first methylphenidate prescription was 9.7 years and the majority of children receiving methylphenidate were boys (74.6%). Children were more often Dutch or had a Western ethnic background (73.6%) compared to non-Western and the majority of our children received their first methylphenidate prescription from a medical specialist (89.3%). Around 10.1% of the children received other psychotropic medications before their first methylphenidate prescription. Finally, 18.9% of the children had autistic traits above the cutoff score.
Child and Family Characteristics of Children Who Have Received a Methylphenidate Prescription (n = 307)
Values are given in numbers (%), unless stated otherwise.
Antiepileptics, antidepressants, antipsychotics, anxiolytics, hypnotics and sedatives, and melatonin.
CBCL indicates Child Behaviour Checklist (CBCL/1.5–5 and CBCL/6–18).
SRS indicates Social Responsiveness Scale short form.
Number of missing values is not shown.
CPRS, Conner's Parent Rating Scale; MPH, methylphenidate; SD, standard deviation.
Determinants of adherence
Table 2 shows determinants that were associated with adherence (MPR ≥0.80) to methylphenidate treatment. Of the 264 children with more than one prescription, 63 were adherent within 2 years after treatment initiation. In the univariable analyses, we found children more likely to be adherent when they mainly received long-acting methylphenidate during the follow-up period (OR: 2.50, 95% CI: 1.37–4.54). However, this association did not remain present in the multivariable analysis (adjusted OR: 2.01, 95% CI: 0.99–4.11). Children who switched their medication multiple times from short acting to long acting (and vice versa) were more likely to be adherent than those who did not switch (adjusted OR: 2.35, 95% CI: 1.08–5.09).
Determinants Associated with Adherence (MPR ≥0.80) to Methylphenidate Treatment Up to Two Years After Treatment Initiation (n = 264)
The bold values are considered ‘statistically significant’.
The MPR was only calculated when more than two prescriptions was received.
Values are given in numbers (%), unless stated otherwise.
Anticonvulsants, antidepressants, antipsychotics, anxiolytics, hypnotics and sedatives, and melatonin.
CBCL indicates Child Behaviour Checklist (CBCL/1.5–5 and CBCL6–18). We corrected for the time between the date the questionnaire was completed and the date of first prescription.
SRS indicates Social Responsiveness Scale short form.
Number of missing values is not shown.
The multivariable model included all variables, except for the behavioral characteristics. Determinants were selected based on the literature.
CI, confidence interval; CPRS, Conner's Parent Rating Scale; MPH, methylphenidate; MPR, medication possession ratio; OR, odds ratio; SD, standard deviation.
Furthermore, children of mothers with one child only (adjusted OR: 2.31, 95% CI: 1.17–4.54) were more likely to be adherent. Compared to those with a high household income, we observed an association between a moderate household income and methylphenidate treatment adherence (adjusted OR: 3.45, 95% CI: 1.43–8.31). For the remaining determinants, including age of first treatment, gender, type of prescriber of first prescription, dispensation of other medications before the first methylphenidate prescription, maternal education, and behavioral characteristics, no significant associations were found in the univariable or multivariable analysis.
Persistence
In total, 264 children were included in the survival analyses as they received more than one prescription for which the MPR could be calculated (43 children only received one prescription). In the study population, 67 children had an MPR below 0.50 (25.4%), 125 children had an MPR between 0.50 and 0.79 (47.3%), and 74 children had an MPR of 0.80 or above (28.0%). The overall mean treatment duration until discontinuation was 2.7 years (standard error [SE]: 0.14). In patients with an MPR <0.50, the mean treatment duration was 2.6 years (SE: 0.24), the mean treatment duration in patients with an MPR between 0.50 and 0.79 was 5.6 years (SE: 0.17), and the mean treatment duration in patients with good adherence (MPR ≥0.80) was 3.1 years (SE: 0.33).
Figure 2 shows the survival curves of persistence in children with a low, (MPR <0.50), intermediate (MPR 0.50–0.70), and high adherence (MPR ≥0.80). We found that children with a low or intermediate MPR had a higher persistence in the first 2.7 years of methylphenidate treatment (p < 0.001). After 2.7 years, persistence was higher in children with good adherence (p < 0.001). Differences in survival curves between the three MPR groups were observed (p = 0.03).
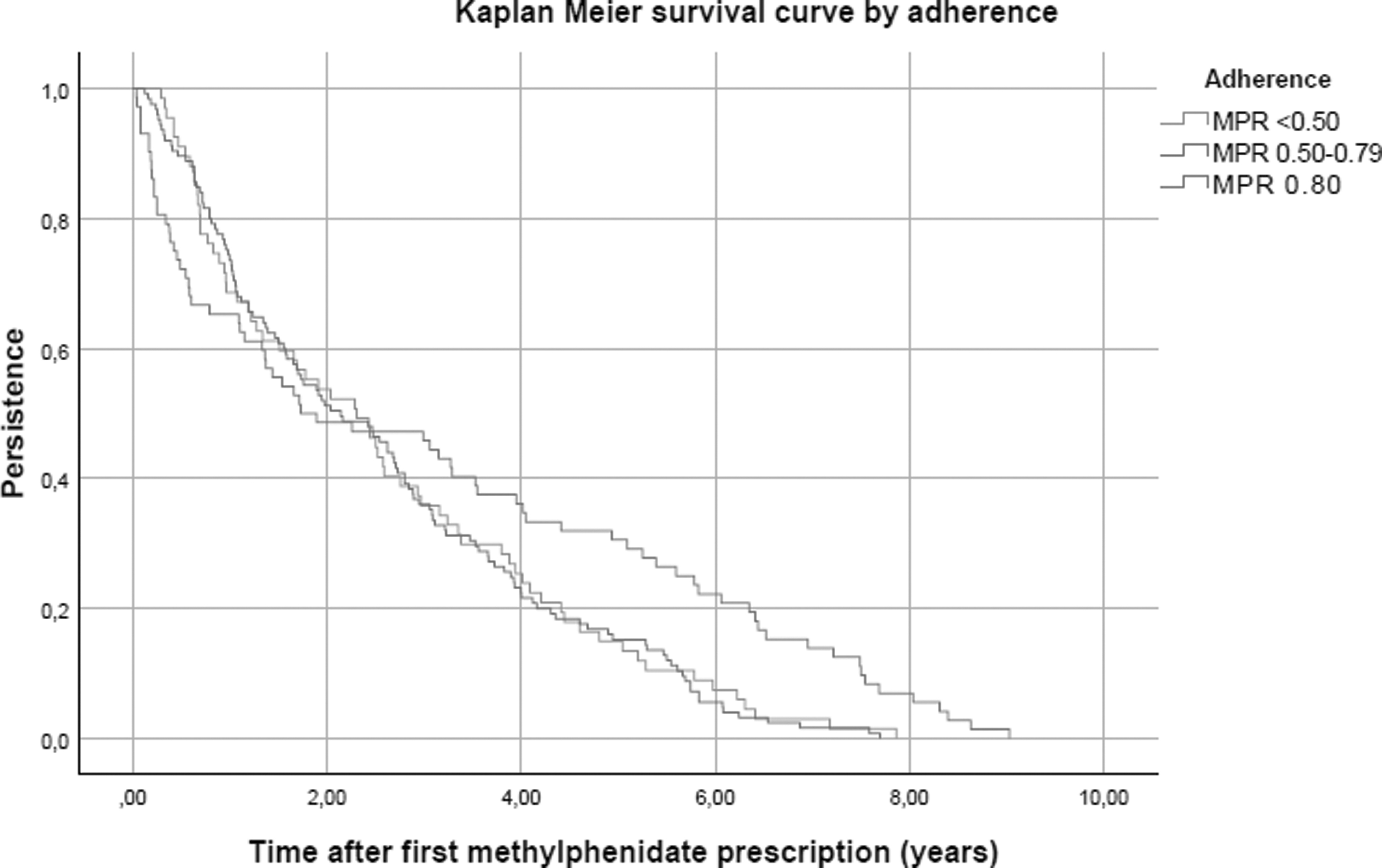
Kaplan–Meier curve for persistence by adherence (n = 264). The Kaplan–Meier curve was presented for persistence where children were censored when having a gap period without prescriptions for 6 months or more (nonpersistence). This curve shows the probability of persistence of methylphenidate treatment in three adherence groups (low, intermediate, and high) over a time interval with a maximum of 9 years after the first methylphenidate prescription. MPR, medication possession ratio; n, number.
Table 3 shows the risk of nonpersistence in children who started methylphenidate treatment. Only four children (1.3%) were persistent during the entire follow-up period. Girls were more likely to be nonpersistent than boys (adjusted hazard ratio [HR]: 1.44, 95% CI: 1.07–1.95). The risk of nonpersistence increased with age (adjusted HR: 3.55, 95% CI: 2.54–4.98). Children who were more often prescribed short-acting methylphenidate than long-acting methylphenidate were more likely to be nonpersistent (number of short acting higher than long acting, adjusted HR: 1.49, 95% CI: 1.13–1.96).
Risk Factors for Nonpersistence of Methylphenidate Treatment (n = 307)
The bold values are considered ‘statistically significant’.
Adjusted for MPR, gender, age of first prescription, ethnicity, type of prescriber, other medications before the first MPH prescription, number of short-acting and long-acting methylphenidate, and the number of switches between long acting and short acting.
Anticonvulsants, antidepressants, antipsychotics, anxiolytics, hypnotics and sedatives, and melatonin.
CI, confidence interval; HR, hazard ratio; MPH, methylphenidate; MPR, medication possession ratio; SD, standard deviation.
Discussion
Main findings
This study aimed to investigate the adherence and persistence of methylphenidate treatment and their associated determinants. These findings show that children who switched their medication multiple times from short acting to long acting (and vice versa) were more likely to be adherent than those who did not switch. Also, a number of family characteristics played a role in the treatment adherence of children. We found that children whose mother had given birth to more than one child had a lower adherence than those who had given birth to one child only. Children from families with a moderate household income were more adherent than those with a high household income.
We found that girls were more likely to be nonpersistent than boys and the risk of nonpersistence increases with age. Furthermore, we found that children who were mainly using long-acting methylphenidate (compared to short-acting methylphenidate), were less likely to be nonpersistent.
Explanation of these findings
First of all, it is important to emphasize that adherence in children is, unlike adolescents and adults, not only based on child determinants but also on parental factors. Parents play an important role in the medication adherence of children as they usually depend on them. We found that children whose mother gave birth to more than one child were less likely to be adherent. As these children are mostly reliant on their parents, it is possible that mothers who have more than one child may find it difficult to make sure that their child follows the prescribed treatment regimen due to an overload of responsibilities and tasks (as they have to take care of more than one child) (Gayer and Ganong 2006).
Furthermore, we found that children from families with an average household income were more likely to have good adherence than those from families with a higher household income. Whether this is due to a higher household income where both parents are working and therefore have less time to monitor medication use in children could not be studied. Further research is needed to investigate this observation. It is also possible that parents with a higher household income are more ambivalent toward this type of pharmacotherapy (Coletti et al. 2012).
Second, we observed that patients with high adherence in the first 2.7 years of treatment were less persistent. A possible explanation for this finding is that these children are adherent, but found out earlier that the treatment does not work, or they stop due to adverse effects. Children may stop using their medication due to adverse effects (e.g., problems with sleep or loss of appetite) or contraindications, or they may only take it when needed, resulting in discontinuity of treatment and thus a lower adherence (Frank et al. 2015). Children who do not take their medication as prescribed (nonadherence) may eventually discontinue treatment as shown previously (Gajria et al. 2014). However, the question of whether patients are nonpersistent or nonadherent may also be influenced by the fact that children are advised to have a medication break (of 1–2 weeks) at least once a year.
The Dutch Guidelines for General Practitioners describes that these breaks should be initiated to determine whether or not the pharmacological treatment is effective and should be continued, preferably during a representative period of 1–2 months. Furthermore, patients may also have a break during weekends or vacations as part of the regular treatment with methylphenidate (NHG-Standaard ADHD bij kinderen 2018). These breaks may not always be reflected in the number of prescriptions and may show a lower adherence in these patients. Therefore, it is possible that patients in our study, who show a low adherence and high persistence, may be in fact patients with a higher adherence. More research is needed to further elaborate these findings.
Third, the results of our study show that girls were more likely to be nonpersistent than boys, which was previously reported (Miller et al. 2004). One of the possible reasons is that the effectiveness of methylphenidate is better to observe in boys in terms of symptoms improvement than girls, because boys more often show hyperactivity, while girls more often have concentration problems. When these symptoms improve, parents will probably encourage their children to take their medication according to prescribed treatment regimen (Novik et al. 2006; Mowlem et al. 2019). It is important to conduct further research to investigate the differences in nonpersistence to methylphenidate treatment among boys and girls. In addition, the reason for nonpersistence could be further investigated.
Finally, we found that children who started methylphenidate treatment at an older age were more likely to be nonpersistent than those who started at a young age. This is in line with a previously published study where a younger age (0–8 years vs. 10–19 years) was associated with greater persistence (Miller et al. 2004). A possible explanation is that they are less dependent on their parents and may stop or continue treatment when they want. They also may have used methylphenidate (often short term) for other reasons than treating ADHD symptoms, such as increasing school performance, and are therefore less persistent (Setlik et al. 2009). Another possible reason is that methylphenidate was prescribed for other indications such as ODD, where methylphenidate may be less effective.
When considering long- and short-acting methylphenidate, our finding shows a greater persistence in children who mainly received long-acting methylphenidate, which is in line with a previous study (Palli et al. 2012). Patients who receive the long-acting methylphenidate are less likely to forget to take their medication as they have to take less pills a day compared to the short-acting methylphenidate. This may result in a higher adherence. Also, children who switched medication multiple times from long acting to short acting and vice versa were more likely to be adherent than those who did not switch at all. It may be possible that they switch based on the severity of the disorder and symptom improvement, and adverse events may have played a role. This group may be more willing to try and find the best possible treatment and therefore are more likely to be adherent to treatment (Punja et al. 2013).
Strengths and limitations
One of the strengths of this study is the population-based cohort of young children with up to 16 years of follow-up and the multiethnic nature of this population. This long follow-up duration enabled us to investigate potential factors associated with adherence up to 2 years (rather than 6 months as in previous studies) (Gau et al. 2006; Hugtenburg et al. 2006). Pediatric patients who started with methylphenidate may stop and restart again. Therefore, it is important to consider a long treatment duration to examine adherence. Also, extensive information about the children and parents was collected prospectively since birth, which made it possible to assess numerous factors that are associated with good treatment adherence. Furthermore, adherence and persistence were calculated based on dispensing records, which is more accurate in terms of dispensation dates than information on prescription records as these medications may have been prescribed, but not collected from pharmacies.
However, our study also has several limitations. We did not have information on clinical diagnoses and relied on maternal reported questionnaire data on emotional or behavioral problems in the child. Furthermore, we did not have information about other treatments such as behavioral therapy, which may have also influenced the persistence and adherence to methylphenidate. Also, the number of children in the older age groups is lower as for most children in our study, they were followed until the age of 16 years. Therefore, the follow-up after treatment initiation in the older children was shorter. However, persistence was only calculated in children when at least 7 months of follow-up was available after starting treatment to ensure a gap period of 6 months (which is needed to measure nonpersistence). Furthermore, characteristics of the father or partner were not included because the number of questionnaires completed by them was too low to be included in the analyses. We did not have sufficient power to assess the association between several determinants, such as child ethnicity and marital status, with adherence as the numbers were too low.
Further research in a larger population is needed to assess if and how ethnicity or marital status would affect adherence to methylphenidate in children. Finally, we did not have the pharmacy records of 1742 children, which may have included methylphenidate users.
Conclusion
In conclusion, the results of our study showed that both child and family characteristics may play a role in treatment adherence. Furthermore, child's gender and age at the start of treatment were found to be associated with persistence. Considering these findings, it is important for health care professionals to take these into account when initiating methylphenidate treatment.
Footnotes
Clinical Significance
Treatment adherence and persistence in children may be difficult to measure as parents also play an important role in the medication use of children. The findings from this study showed that not only child characteristics but also family characteristics may influence methylphenidate treatment adherence and persistence in children.
Disclosures
No competing financial interests exist.