
Abstract
Objective:
This study evaluated the predictors for delayed initiation and continuation of ADHD medication use in children and adolescents with ADHD in Taiwan.
Methods:
This longitudinal cohort study enrolled 188,061 children and adolescents with ADHD between 2001 and 2011. Delayed initiation of ADHD medications was defined as the interval >365 days between diagnosis and first prescription, and continuation of ADHD medications was defined as ≥365 defined daily doses of ADHD medications.
Results:
Of the included patients, 39.2% were never treated with ADHD medications. Delayed initiation and continuation of ADHD medication use were found in 11.9% and 19.9% of the ever-treated patients, respectively. Younger age at ADHD diagnosis, male sex, older mother's age at child's ADHD diagnosis, and higher family income were associated with more delayed initiation but were also associated with more continuation of ADHD medication use.
Conclusions:
The initiation and continuation of ADHD medication use might be underlined by different mechanisms and warrant different strategies.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is the most common neurodevelopmental disorder in children. A systematic review, including more than one million children aged ≤18 years, reported that the overall pooled estimate of prevalence was 7.2% worldwide (Thomas et al. 2015). According to clinical practice guidelines by the American Academy of Pediatrics, pharmacological treatment (i.e., stimulants and nonstimulants) is one of the standard treatments for ADHD. The first-line treatment for children aged 6–11 years and adolescents aged 12–18 years is medications (Grade A recommendation) (Wolraich et al. 2019). Regarding children aged <6 years, stimulants are recommended for those with moderate-to-severe continued disturbance or those with no significant improvement after behavioral therapy (Wolraich et al. 2019).
Although pharmacological treatment is a cornerstone of ADHD treatment, poor adherence to ADHD medication use remains an unresolved issue (Perwien et al. 2004; Marcus et al. 2005; Froehlich et al. 2007; Garbe et al. 2012). According to the National Health and Nutrition Examination Survey in the United States, among 8- to 15-year-old patients meeting the ADHD criteria as per the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association 1994), only 32.0% were treated consistently with ADHD medication use in the past year (Froehlich et al. 2007). A similar situation was noted in Germany, where only 52.0% of 3- to 17-year-old ADHD patients received ADHD medications (Garbe et al. 2012).
As untreated ADHD in childhood and adolescence negatively affects long-term functioning—such as poor academic performance, presence of antisocial or addictive behaviors, and poor social function (Shaw et al. 2012; Hechtman et al. 2016)—identifying patients who may be potentially untreated, late-treated, or quit medication use early is crucial. This study evaluated the predictors for delayed initiation and continuation of ADHD medication use in children and adolescents with ADHD.
Methods
Data source
This longitudinal cohort study is based on a nationwide claims database, the National Health Insurance Research Database (NHIRD). The Taiwan National Health Insurance program, a compulsory and universal health insurance program, was implemented in 1995 and offered comprehensive medical care coverage to all residents of Taiwan. The NHIRD is a database of insurance claims consisting of health care data from >99% of the population of Taiwan and was administered and organized by the National Health Research Institutes (NHRI). The NHIRD was audited by the NHRI and was released for academic research. To protect the privacy of insured subjects, when individual medical records are extracted from the NHIRD, the information is deidentified and patient anonymity is guaranteed. The database contains comprehensive data on insured subjects, including their demographic characteristics, clinic visit dates, disease diagnoses, and medical interventions. The codes of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) are used for disease diagnosis. In this study, using each resident's unique personal identification number, all of the demographic information was linked. Subsequently, following the method by Chen et al. (2019) and Cheng et al. (2018), the parent–child relationships in the NHIRD were identified. Numerous Taiwanese epidemiological studies have used the NHIRD (Chen et al. 2016, 2019; Cheng et al. 2018; Huang et al. 2020). This study was initiated after approval from the Institutional Review Board of Taipei Veterans General Hospital.
Study subjects and measures
Children aged 3–11 years and adolescents aged 12–19 years who received the diagnosis of ADHD (ICD-9-CM code: 314) from board-certified psychiatrists between January 1, 2001, and December 31, 2011, were enrolled in the current study. ADHD medications were identified according to the Anatomical Therapeutic Chemical (ATC) Classification System. In Taiwan, only three medications were approved and available for ADHD treatment: immediate-release methylphenidate (ATC code: N06BA04), extended-release methylphenidate (ATC code: N06BA04), and atomoxetine (ATC code: N06BA09). The initiation of ADHD medications was defined as the date of first prescription of these ADHD medications. The interval between the date of ADHD diagnosis and the date of first prescription of ADHD medications was calculated. Delayed initiation of ADHD medications was defined as an interval >365 days. Continuation of ADHD medications was defined based on the amount of ADHD medications used from the date of ADHD diagnosis to December 31, 2011, or to death and was divided into three groups: rare users (cumulative defined daily doses [cDDD] <30), short-term users (cDDD = 30–364), and long-term users (cDDD ≥365). The psychiatric comorbidities, including developmental delay/intelligence disability, autism spectrum disorder (ASD), disruptive behavior disorders, anxiety disorders, depressive disorders, and alcohol and substance use disorders, with ADHD at baseline (before or at the ADHD diagnosis date) were assessed. The parental ages at the time of children's ADHD diagnoses were calculated and the parental monthly incomes were also identified. In the current study, 101,010 (53.7%) patients with ADHD were linked with both fathers and mothers, 47,579 (25.3%) were only linked with fathers, 39,267 (20.9%) were solely linked with mothers, and 205 (0.1%) patients could not be linked with any parent. The monthly insured amount was assessed to define and classify the state of family income (low: <19,100, middle: 19,100–42,000, and high: >42000 New Taiwan Dollars) because the monthly insured amount was determined by family income. We determined the family income state by the higher income state of the father or mother. For example, the high family income state was assigned if the father was in the middle-income state and mother was in the high-income state. Finally, we assessed the level of urbanization (level 1 [most urbanized] to level 5 [least urbanized]) as a variable in this study (Liu et al. 2006).
Statistical analyses
For between-group comparisons (ADHD ever treated with medications vs. ADHD never treated with medications), the F test was used for continuous variables and Pearson's χ 2 test for nominal variables, where appropriate. Stratified by age group (children aged 3–11 years and adolescents aged 12–19 years), logistic regression analysis was performed to investigate the predictors for ever use of ADHD medications with potential variables of age at ADHD diagnosis, sex, psychiatric comorbidities, father's age at child's ADHD diagnosis, mother's age at child's ADHD diagnosis, family income, and level of urbanization. For patients who were ever treated with ADHD medications, logistic regression analyses were also used to evaluate the predictors for delayed initiation of ADHD medications (>365 days vs. ≤365 days) and continuation of ADHD medications (long-term use vs. short-term/rare use), respectively, with the same potential variables in the above regression model. In Taiwan, ADHD medications were only approved for patients aged ≥6 years. Therefore, these two analyses were limited to and stratified for children aged 6–11 years and adolescents aged 12–19 years. A two-tailed p-value of <0.05 was considered statistically significant. All data processing and statistical analyses were performed with Statistical Package for the Social Sciences (SPSS), version 17, software (SPSS, Inc.) and Statistical Analysis Software (SAS), version 9.1 (SAS Institute, Cary, NC).
Results
In all, 188,061 children and adolescents with ADHD were enrolled in our study: 114,298 (60.8%) ever treated with ADHD medications and 73,763 (39.2%) never treated with ADHD medications (Table 1). Patients ever treated with medications were predominantly male, had greater prevalence of baseline psychiatric comorbidities (developmental delay/intelligence disability, disruptive behavior disorders, anxiety disorders, and depressive disorders), and were in the lower family income state compared with those never treated with medications (Table 1). The paternal age and maternal age at children's ADHD diagnosis were higher in patients ever treated than in those never treated (Table 1).
Demographic Data of Children and Adolescents with Attention-Deficit/Hyperactivity Disorder
ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation; cDDD, cumulative defined daily doses; ASD, autism spectrum disorder; NTD, New Taiwan Dollars.
Logistic regression analyses showed that predictors for ever use of ADHD medications included older age at ADHD diagnosis, male sex, older age of father at child's ADHD diagnosis, younger age of mother at child's ADHD diagnosis, psychiatric comorbidities of developmental delay/intelligence disability, disruptive behavior disorders and anxiety disorders, less urbanization, and lower family income in children with ADHD. In adolescents with ADHD, younger age at ADHD diagnosis, absence of developmental delay/intelligence disability and alcohol and substance use disorders, presence of anxiety disorders, and less urbanization significantly predicted ever use of ADHD medications (Table 2).
Likelihood of Use of Attention-Deficit/Hyperactivity Disorder Medications Among Children and Adolescents with Attention-Deficit/Hyperactivity Disorder (Aged 3–19 Years)
Bold type indicates statistical significance.
ADHD, attention-deficit/hyperactivity disorder; OR, odds ratio; CI, confidence interval; ASD, autism spectrum disorder; NTD, New Taiwan Dollars.
Delayed initiation of ADHD medications
Among the 114,298 patients ever treated with ADHD medications, 13,629 (11.9%) patients had delayed initiation of ADHD medications. The average delayed interval between diagnosis and medications is shown in Figure 1. The interval dramatically reduced after the age of 6 years. In children ever treated with ADHD medications, younger age at ADHD diagnosis, male sex, older age of mother at child's ADHD diagnosis, absence of disruptive behavior disorders and anxiety disorders, less urbanization, and high family income significantly predicted delayed initiation of ADHD medications. In adolescents, only male sex and the presence of developmental delay/intelligence disability were significant predictors for delayed initiation of ADHD medications (Table 3).
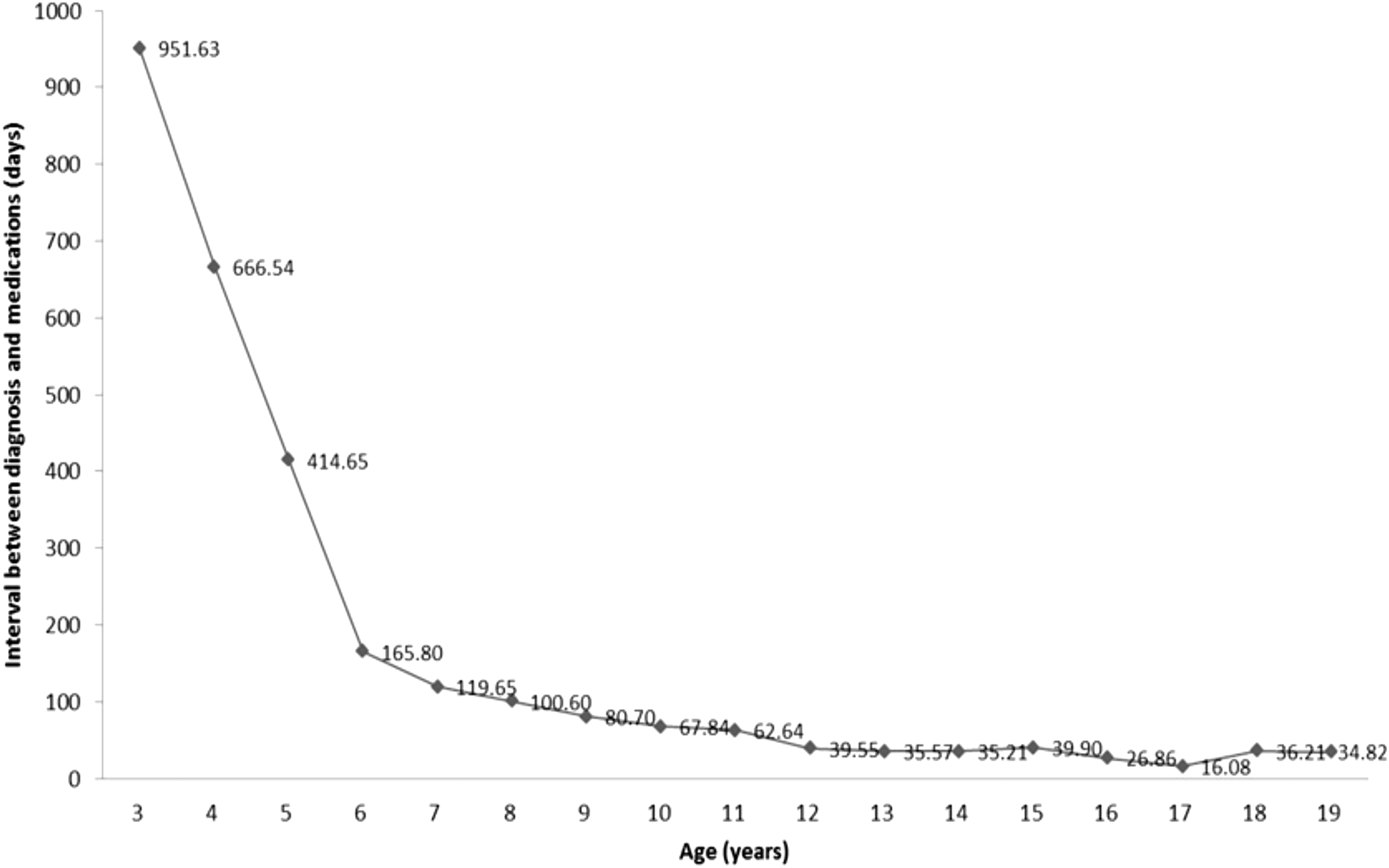
Interval between ADHD diagnosis and ADHD medications among children and adolescents with ADHD receiving ADHD medications (aged 3–19 years). ADHD, attention-deficit/hyperactivity disorder.
Likelihood of Delayed Medication Treatment (>365 Days) Among Children and Adolescents with Attention-Deficit/Hyperactivity Disorder Receiving Attention-Deficit/Hyperactivity Disorder Medications (Aged 6–19 Years)
Bold type indicates statistical significance.
ADHD, attention-deficit/hyperactivity disorder; OR, odds ratio; CI, confidence interval; ASD, autism spectrum disorder; NTD, New Taiwan Dollars.
Continuation of ADHD medications
Among the 114,298 patients ever treated with ADHD medications, only 22,733 (19.9%) patients were long-term users of ADHD medications, and short-term users and rare users accounted for 53,155 (46.5%) patients and 38,410 (33.6%) patients, respectively. In children ever treated with ADHD medications, younger age at ADHD diagnosis, male sex, older age of mother at child's ADHD diagnosis, presence of developmental delay/intelligence disability and anxiety disorders, and high family income were significantly associated with the long-term use of ADHD medications. In adolescents, younger age at ADHD diagnosis, older age of mother at child's ADHD diagnosis, presence of ASD and disruptive behavior disorders, absence of anxiety and depressive disorders, and high family income significantly predicted the long-term use of ADHD medications (Table 4).
Likelihood of Long-Term Use of Attention-Deficit/Hyperactivity Disorder Medications Among Children and Adolescents with Attention-Deficit/Hyperactivity Disorder Receiving Attention-Deficit/Hyperactivity Disorder Medications (Aged 6–19 Years)
Bold type indicates statistical significance.
ADHD, attention-deficit/hyperactivity disorder; OR, odds ratio; CI, confidence interval; ASD, autism spectrum disorder; NTD, New Taiwan Dollars.
Interestingly, a U-shaped association between urbanization (most urbanized and most rural regions) and long-term use of ADHD medications was noted both in children and adolescents ever treated with medications (Table 4).
Discussion
In Taiwan, ∼40% of children and adolescents with ADHD were never treated with ADHD medications. Among those who received medications, ∼12% had delayed initiation and only ∼20% were long-term ADHD medication users, which was compatible with findings from the multimodal treatment study of ADHD where only approximately one-third of adolescents with ADHD were medicated for over 50% of days in the past year at the 8-year follow-up (Molina et al. 2013). In addition, our study identified several predictors for delayed initiation and continuation of ADHD medication use, including age at ADHD diagnosis, sex, mother's age at child's diagnosis, psychiatric comorbidities, family income, and urbanization.
We found different predictors for delayed initiation and continuation of ADHD medication use, with some of them even being counterintuitive, particularly in children. For instance, younger age at ADHD diagnosis, male sex, older age of mother at child's ADHD diagnosis, and higher family income were not only associated with more delayed initiation but also with more continuation of ADHD medication use. These findings suggest that different mechanisms might underlie the initiation and continuation of ADHD medication use. Concern for adverse effects is one of the main reasons for limiting ADHD medication use, and adverse events and ineffective treatment are the main reasons for discontinuing ADHD medication use (Brinkman et al. 2018). Sex, parental age at child's ADHD diagnosis, and family income may differently affect these two important treatment issues. Our results provided insight into these issues and also indicated that mental health professionals must design different strategies for these two issues.
The role of urbanization was another notable finding in our study. Less urbanization was related to a higher likelihood of ever use of ADHD medications. However, for predicting delayed initiation and continuation of ADHD medications, a U-shaped relationship was noted, particularly in children. Evidence of the role of urbanization in ADHD medication use is mixed, with some studies reporting no relationship between the two (Chen et al. 2011; Bhang et al. 2017; Danielson et al. 2018; Kamimura-Nishimura et al. 2019), but others demonstrating a geographic variation in ADHD medication use (Cox et al. 2003; Centers for Disease Control and Prevention 2005; Leslie et al. 2005; McDonald and Jalbert 2013). Cox et al. (2003) reported that children (aged 5–14 years) in mostly rural areas and mostly urban areas had a higher likelihood of receiving at least one stimulant treatment than those in 100% rural areas and that children in 100% urban areas had a similar prevalence of stimulant treatment to those in 100% rural areas. Moreover, the possible reasons for the U-shaped relationship of urbanization with ADHD medication use require further investigation because geographic variation can also confound numerous other factors, such as access to mental health services (Ahmed et al. 2013), socioeconomic conditions of the families (Anderson et al. 2013), educational level of patients (Anderson et al. 2013), and clinician practice patterns (McElligott et al. 2014).
Our results also revealed that children with ADHD having psychiatric comorbidities at baseline tended to have a lower prevalence of delayed initiation and a higher prevalence of continuation of ADHD medication use. However, the results for adolescents were different from those for children. For instance, adolescents with comorbid developmental delay and intelligence disability were more likely to have delayed initiation of ADHD medication use. Adolescents with anxiety or depressive disorders were less likely to be long-term users, in contrast to those with ASD or disruptive behavior disorders. Most studies have recognized psychiatric comorbidities as crucial predictors for initiation (Garbe et al. 2012; Wang et al. 2016) and discontinuation (Toomey et al. 2012; Wang et al. 2016; Bhang et al. 2017) of ADHD medication use. However, some have reported no significant results (Leslie et al. 2005; Kamimura-Nishimura et al. 2019; Safavi et al. 2019). These aforementioned variations among adolescents may be due to adolescents being more involved in decision-making than children during the treatment process and due to each study considering different confounding factors.
Family income and parental age may affect ADHD medication use, but the relevant evidence is mixed (Stevens et al. 2005; Gau et al. 2006; Toomey et al. 2012; Ahmed et al. 2013; McDonald and Jalbert 2013; Heins et al. 2016; Danielson et al. 2018; Kamimura-Nishimura et al. 2019; Safavi et al. 2019). Family income and parental age are highly related to some factors that might be more powerful than income and age themselves, such as educational level, job, marital status, psychological history of parents, and parent–child relationship. Because parental knowledge, attitude, and stigma toward ADHD obviously affect ADHD medication use (Toomey et al. 2012; Ahmed et al. 2013; Brinkman et al. 2018; Boudreau and Mah 2020), we could draw any specific conclusion from our results without adjustments for some potentially confounding factors. In addition, this study found that boys had a higher likelihood of receiving medications and continuation, similar to previous studies (Firestone 1982; Leslie et al. 2005; Froehlich et al. 2007; Chen et al. 2011; Garbe et al. 2012; Wang et al. 2016; Kamimura-Nishimura et al. 2019). However, we also observed that boys were more likely to have delayed initiation, contrary to previous reports (Chen et al. 2011; Garbe et al. 2012; Wang et al. 2016). Some studies have even described the negative relationship of sex with adherence to medications (Chen et al. 2011; Toomey et al. 2012; Hong et al. 2013; Bhang et al. 2017; Safavi et al. 2019; Efron et al. 2020). These inconsistent results are likely due to different confounding factors considered in each study.
Our results revealed that older age was associated with less delayed initiation, and the interval between ADHD diagnosis and medication initiation considerably reduced after the age of 6 years. The results were comparable with reports from the United States (Danielson et al. 2018) and Germany (Garbe et al. 2012). The analysis involved individuals aged 6–19 years ever treated with ADHD medications, and current recommendations are for patients aged ≥6 years, and not those aged <6 years; thus, our findings might just reflect the clinicians' adherence to guidelines (Chen et al. 2011; Garbe et al. 2012; Wang et al. 2016; Wolraich et al. 2019). The present study also noted that older patients were less likely to be long-term ADHD medication users. Parents make decisions for younger children, but the influence of parents decreases with time, and older children are more likely to refuse medications (Thiruchelvam et al. 2001; Gau et al. 2006; Chen et al. 2011; Wang et al. 2016).
Several study limitations need to be addressed. First, this was a secondary analysis of data from a claims database. Although the database provided comprehensive patient information, data of several potential confounding factors were not included, such as characteristics of parents, family history, medical history, environmental factors, ADHD severity, and complementary and alternative treatments. Second, this study focused only on ADHD medication use and did not consider behavioral therapy and the combination of medications with behavioral therapy. Third, treatment outcomes (e.g., academic outcomes and presence of antisocial behaviors) and adverse events may also affect ADHD medication use and were not evaluated in this study. Fourth, whether our findings can be generalized to other ethnicities, especially non-Asian people, would need further investigation because of the diverse help-seeking behaviors between ethnicities and differences in the medical service system. Fifth, psychosocial services may affect time to pharmacological treatment among patients with ADHD. However, the NHIRD only included the codes given by physicians, but not by other specialties, such as psychologists and social workers. Without this information, we cannot assess its impact.
Conclusions
Several predictors for delayed initiation and continuation of ADHD medication use were identified, including age at ADHD diagnosis, sex, mother's age at child's diagnosis, psychiatric comorbidities, family income, and urbanization, but their predictive roles varied between the initiation and continuation of ADHD medication use. The results suggest that initiation and continuation of ADHD medication use might be underlined by different mechanisms and warrant different strategies.
Clinical Significance
About 40% of Taiwanese children and adolescents with ADHD were never treated with ADHD medications. Among those who received medications, approximately 12% had delayed initiation and only approximately 20% were long-term ADHD medication users, which may be related to age at ADHD diagnosis, sex, mother's age at child's diagnosis, psychiatric comorbidities, and family income. The bio-psycho-social dimensions of ADHD should be comprehensively evaluated for the improvement of ADHD care and treatment.
Footnotes
Acknowledgment
We thank Mr I-Fan Hu, M.A. (Courtauld Institute of Art, University of London; National Taiwan University) for his friendship and support in English editing.
Disclosures
All authors have no financial relationships relevant to this article to disclose.