
Abstract
Objectives:
While hospitalization is an essential aspect of the therapeutic strategy for adolescents with severe or treatment-refractory mood disorders, little is known about the outcome predictors during inpatient treatment.
Methods:
A retrospective chart review was conducted in a university tertiary referral hospital to determine the factors associated with the length of stay, symptom improvement (based on the Clinical Global Impression-Improvement [CGI-I] scale), and the change in the overall level of functioning during the stay (based on the Children-Global Assessment Scale [CGAS]). Over 2 years, 106 adolescents were diagnosed with mood disorders (mean age = 15.0 ± 0.16; 43% girls), with a particular high rate of associated adverse psychosocial factors, and an average length of stay longer than most psychiatric hospital settings (mean = 100.7 ± 9.57 days).
Results:
Multivariate analysis concluded that longer duration of current episode and worse functioning at admission (CGAS score) were independent predictors for length of stay. Greater functional improvement (CGAS score change from admission to discharge) was best predicted by the diagnosis of bipolar disorder, lower functioning, and greater illness severity on admission. Symptom improvement (CGI-I) did not have any independent predictors.
Conclusion:
This finding supports the value of measuring symptoms duration in predicting the hospitalization outcomes of adolescents with severe or treatment-refractory mood disorders, in view of addressing maintenance factors at an early stage. Bipolar symptoms should be sought not only at admission but also regularly during the stay.
Introduction
Mood disorders are the most common causes of admissions in adolescent inpatient units (Hayes et al. 2018) and the main causes of global burden for psychiatric reasons at this age (Thapar et al. 2012; Malhi and Mann 2018). While the indications for hospitalization are generally consensual, when the patient should be discharged is often a matter of controversy. The debate on the optimal length of stay of adolescents in inpatient psychiatric units raises many questions concerning the expected clinical benefits, the possible side-effects of a full-time stay, the cost of services, and ethical issues (Terr and Sarles 1993; Swadi and Bobier 2005; Zambrowicz et al. 2019). These questions have surprisingly received little scrutiny, while hospitalization is an essential aspect of treatment-refractory mood disorders (Consoli et al. 2007; Thapar et al. 2012).
Several studies examined the predictors of length of stay in adolescent psychiatric inpatients, regardless of diagnostic categories (Livingston et al. 1990; Borchardt and Garfinkel 1991; Gold et al. 1993; Pottick et al. 2000; Sourander et al. 2002; Swadi and Bobier 2005; Stellwagen and Kerig 2010; Reddy et al. 2017; Zeshan et al. 2018). These studies are useful for informing psychiatrists on the patients' and families' needs that should be addressed during the hospitalization to facilitate recovery. The most robust predictors of length of stay based on these studies are gender (being a boy), a young age, ethnic minority, clinical severity, and a lower level of functioning at admission (Borchardt and Garfinkel 1991; Gold et al. 1993; Pottick et al. 2000; Sourander et al. 2002; Swadi and Bobier 2005; Stellwagen and Kerig 2010; Reddy et al. 2017; Zeshan et al. 2018). It is important to keep in mind that the length of stay cannot be viewed as a proxy for treatment outcome as it is not only influenced by patient's individual characteristics but also by many external factors such as the type of facility, social characteristics (e.g., the stability of the home environment, the availability of outside placements), or the type of health care system (e.g., access, cost) (Tulloch et al. 2011). To determine which patients with mood disorders are the most likely to benefit from hospitalization, markers of symptom and functional improvement are worth measuring alongside (Lyons and Schaefer 2000; Green et al. 2001; Mathai and Bourne 2009; Setoya et al. 2011; Haggerty et al. 2014; Serim Demirgoren et al. 2017).
In most inpatient services, the clinical attention during the stay of an adolescent with mood disorder is more focused on stabilizing symptoms rather than obtaining a full recovery (Sadock et al. 2015). This seems rather reasonable considering that the average length of hospitalization does not exceed 2 weeks in most countries (Borchardt and Garfinkel 1991; Gold et al. 1993; Bobier et al. 2009; Burgess et al. 2009; Reddy et al. 2017; Zeshan et al. 2018). A decrease in the length of stay in adolescent psychiatric inpatient facilities observed in almost all countries over the last decades has coincided with greater emphasis on community-based services, a more systematic use of residential care for patients requiring longer term treatment and the development of short-stay crisis centers (Swadi and Bobier 2005; Lahey and Kupfer 2013). However, during a 2-week hospitalization it may be very difficult to differentiate a true symptom improvement of the mood problems from the containment effect of inpatient admission itself due to the removal from stressful environments or the effect of group milieu. Concerns have been also raised that 2-week hospitalizations are in many cases too short to estimate the response to most medications used in mood disorders (i.e., antidepressant, mood stabilizer) (Terr and Sarles 1993). Finally, longer period of observation in an inpatient facility may be an opportunity to gain detailed information on the reasons why some of these patients do not respond to front-line treatments (Garno et al. 2005; Emslie et al. 2010). This is particularly true for adolescent with depressive disorders, wherein repeated adverse life events in different domains (i.e., school, family, peers) may fuel negative mood and perpetuate depressive state (Olliac et al. 2018; Malhi et al. 2020).
We aimed to address these main gaps in the literature by determining the factors associated with several outcomes of the hospitalization of adolescents with mood disorders: the length of stay (aim 1), the change in symptom severity and in the level of functioning (aim 2). In this retrospective chart-review study, we used data from one of the few remaining university-affiliated psychiatric units for adolescents with the possibility of long-duration stay if needed, explaining why this sample is particularly enriched in patients with severe and treatment-refractory mood disorders.
First, we expected to confirm that a higher level of symptom severity and a lower level of functioning at admission predicted a longer length of stay among inpatients with mood disorders, in line with previous findings (Gold et al. 1993; Stellwagen and Kerig 2010; Reddy et al. 2017). We also examined the effect of a series of factors previously reported in the literature as etiological and/or maintenance factors (Consoli et al. 2007; Emslie et al. 2011) and/or predictors of treatment response (Asarnow et al. 2009; Nilsen et al. 2013) for mood disorders: duration of symptoms, suicidal ideation, nonsuicidal self-injury, aggressive behaviors, number of comorbid psychiatric disorders, association with chronic medical condition, learning disabilities or language disorders, history of maltreatment, parent–child conflict or poor parenting skills, fostered children.
Second, we hypothesized that the predictors of therapeutic outcomes will be, at least partly, distinct from those which influence the length of stay. This finding will confirm the assumption that length of hospital stay cannot be regarded as a proxy for the therapeutic outcomes (Green et al. 2001). In addition, full-time stay hospitalization may result in specific side-effects influencing hospitalization outcomes, for example due to the disconnection from family and community supports, social stigma, or the effect of deviant peer influences (Terr and Sarles 1993; Swadi and Bobier 2005; Lahey and Kupfer 2013). It is important to take into account the factors associated with a longer inpatient stay and a lower symptom/functional improvement prior admission to guarantee the correct assessment of the risk–benefit ratio of the hospitalization. In contrast, factors associated with a longer length of stay and a higher symptom/functional improvement should be cautiously screened at admission as they represent potential areas of improvement. In line with previous studies, we will also examine how therapeutic outcomes are affected by the length of stay (Mathai and Bourne 2009; Setoya et al. 2011; Serim Demirgoren et al. 2017).
If confirmed, these findings will enable to identify the individual and social characteristics of inpatient adolescents with mood disorders who had required longer stay hospitalizations. In addition to guiding medical decision, this information may be useful to discuss with family of patients with severe or resistant mood disorders, or health care payers in countries with no free access to inpatient services.
Methods
Setting and study design
Data from the medical record of all patients hospitalized in two adolescent units of a university hospital between January 2017 and December 2018 had been previously extracted for a research on substance use in inpatient adolescents. The research was funded by competent national authority (MILDECA project IReSP-15-Prevention-11) and received the approval of the ethics committee of the hospital. A waiver of written consent applies due to the retrospective design of the study, patient deidentification, and the use of routine questionnaires. Two researchers extracted information for all consecutive patients based on the available clinical and paramedical charts using a 66-item computerized questionnaire. The data collected encompassed (i) sociodemographic characteristics (3 items); (ii) clinical characteristics, including the discharge psychiatric diagnoses among a list of the 16 most frequently used categories (27 items); (iii) symptom severity, level of functioning, and treatment response (9 items); (iv) developmental history and associated medical conditions (18 items); and (v) school functioning and psychosocial factors (9 items). Each patient's information was crosschecked by clinicians who directly cared for the participant, and discrepancies were resolved by discussion in conjunction with the senior authors. The assessment of the inter-rater reliability was based on the analysis of ten randomly selected files (kappa = 0.87). The data extracted have been anonymized before statistical analysis, in line with the ethical general recommendation regarding chart review (Gearing et al. 2006). Only variables in line with the scope of the study are presented here.
Participants
For this study, we extracted information from patients with a discharge psychiatric diagnosis of mood disorder. The psychiatric diagnoses had been defined according to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria and categories (American Psychiatric Association 2013); that is, a major depressive disorder, a persistent depressive disorder, a disruptive mood dysregulation disorder, and a bipolar disorder. The routine diagnostic work-up was based on comprehensive and repeated patient assessment and family interviews. No exclusion criteria were used. During the study period, 106 adolescents ranging from 12- to 18-year old were admitted to hospital with a diagnosis of mood disorder for a total of 191 consecutive new admissions. Table 1 details the main sociodemographic and clinical characteristic of this sample. The adolescent inpatients facilities encompass one unit for 12- to 15-year-old (Esquirol unit) and another for 15- to 18-year-old inpatients (Seguin unit) with 15 beds each. An integrative approach for adolescent mental health problems is fostered with different types of interventions, including pharmacological treatment (detailed in Table 2), individual counseling, supportive groups, occupational therapy, recreational and sporting activities. The indications of providing more structured interventions during the stay are discussed case to case (e.g., cognitive behavioral therapy, bodily mediation, psychodrama). Strong attention is paid to family system with family sessions conducted weekly for providing psychoeducation, and structured family sessions conducted for some of them. In addition to the assessment of the adolescent's school functioning, the progressive inclusion of inpatient in the hospital school center plays an important role in the elaboration of patient's clinical project. A step-down approach through the orientation to ambulatory daily care facility is possible for the most chronically impaired patients.
Description of the Sociodemographic and Clinical Characteristics of the Adolescents with Mood Disorders
CGAS, Children-Global Assessment Scale; CGI-S, Clinical Global Impression-Severity; SD, standard deviation.
Symptom and Functional Improvement During the Stay and Psychopharmacological Treatments at Discharge
CGAS, Children-Global Assessment Scale; CGI-I, Clinical Global Impression-Improvement; ECT, electroconvulsive therapy; FGA, first-generation antipsychotic; SD, standard deviation; SGA, second-generation antipsychotic; SSRIs, selective serotonin reuptake inhibitors.
Assessments
The length of stay was the number of days between admission and discharge. For patients with repeated admissions only the longest hospitalization was selected. The mean length of stay was 100.66 days, standard error [SE] = 9.57, standard deviation [SD] = 97.102 days (min = 1, max = 600, median = 79, 95% confidence interval [CI 81.7–119.6]). The normality assumption for the variable “length of stay” was excluded with 95% confidence based on the Shapiro–Francia test (z = 6.57, p < 0.001) and the Shapiro–Wilk test (z = 7.10, p < 0.001). Kernel density analysis estimates the distribution of data as possibly bi- or trimodal (Supplementary Fig. S1).
The level of functioning was assessed using the Children-Global Assessment Scale (CGAS) (Jones et al. 1995). The CGAS was systematically measured the first and the last week of stay by a senior psychiatrist (respectively, “CGAS admission” and “CGAS discharge”). We used the difference between the CGAS score at discharge and at admission, also labeled Δ-CGAS to track change in the level of functioning during the hospitalization. In this study, the mean difference between the CGAS score at discharge and at admission was 24.19, SE = 1.25, SD = 12.67 (min = −19, max = 53, median = 25, 95% CI [22.3–27.3]). The normality assumption for the variable “Δ-CGAS” was not excluded with 95% confidence based on the Shapiro–Francia test (z = 1.13, p = 0.129) and the Shapiro–Wilk test (z = 1.28, p = 0.100).
Clinical improvement during the hospitalization was measured with the Clinical Global Impression-Improvement (CGI-I) scale (Busner and Targum 2007), completed by a senior psychiatrist during the last week of the hospitalization. In this study, the CGI-I assessed the patient's overall symptom improvement during the hospitalization compared with his/her baseline state at admission, irrespective of the treatments provided (e.g., medication, structured psychotherapy, group interventions). In our sample, 7 patients were “Very much improved” (CGI-I = 1), 56 patients were “Much improved” (CGI-I = 2), 33 patients were “Minimally improved” (CGI-I = 3), 7 patients had “No change” (CGI-I = 4), and 1 patient was “Very much worse” (CGI-I = 6). The mean CGI-I score was 2.43, SE = 0.08, SD = 0.85, and median = 2. The normality assumption was excluded with 95% confidence based on the Shapiro–Francia test (z = 3.98, p < 0.001) and the Shapiro–Wilk test (z = 4.35, p < 0.001).
The severity of clinical symptoms was measured with the Clinical Global Impression-Severity (CGI-S) scale (Busner and Targum 2007). The variable “Duration of current symptoms” refers to a clinician-rated measure of the time interval since the psychiatric symptoms became significantly impairing for the patient and/or caused substantial functional impairment. For example, an adolescent with depressive symptoms occurring 3 months ago who first experienced a depressive episode at age 8 but was relatively symptom free for several years, had a duration of current symptoms estimated at 3 months. This variable was not specifically referring to mood symptoms; for patients with associated chronic nonmood disorder (e.g., attention-deficit disorder), this time interval started when a sudden worsening and/or the onset of new symptoms was observed. The presence of aggressive behavior was defined as the use of physical restraints and/or intramuscular pro re nata medications and/or admission through intensive psychiatric care unit. Parent–child conflict or poor parenting skill was endorsed when home educative assistance and/or prior report to child-protection agencies was reported. Table 2 presents the clinical improvement, level of functioning, and psychopharmacological treatments in inpatients with mood disorders at discharge.
Statistical analysis
The effect of each predictor variable on the length of stay was tested for significance using nonparametric tests: the Spearman correlation for continuous variables and the Wilcoxon signed-rank test for categorical variables. Only, the variables statistically associated with the length of stay in bivariate analyses were included as predictor variables in a multiple regression model using the length of stay as the outcome.
The same analyses were performed to identify the predictors of Δ-CGAS and the CGI-I, except parametric tests were used for the CGI-I (Pearson's correlation for continuous variables and Student's t-test for categorical variable). All analyses were rerun after the transformation of the CGI-S as a categorical variable (i.e., a positive answer was endorsed if the CGI-I score was 1 or 2, and a negative answer in the other cases). To explore the relation between therapeutic outcomes and the length of stay, a three-level ordinal variable was created by splitting the variable length of stay at the upper quarter and the lower quarter, in line with recommendations for analyses of non-normally distributed variable (Gelman and Park 2009): category 1 “short-stay hospitalization” (<42 days); category 2 “intermediate duration” (≥42 days and <120 days); and category 3 “long-stay hospitalization” (≥120 days). Analysis of variance (ANOVA) tests were performed to determine whether the Δ-CGAS and the CG-I scores were statistically different across the three categories. Post hoc Scheffé tests were used for the comparisons between groups when ANOVA yielded a significant F-statistic. Correlations between the length of stay, as a continuous variable, and the Δ-CGAS and the CG-I scores were also performed (respectively, Supplementary Figs. S1 and S2).
Data on medication were not collected initially, and no a priori hypothesis was formulated. Considering the risk of multicollinearity between patients' clinical features and medication, the effects of pharmacological treatments on the length of stay and therapeutic outcomes were analyzed separately. As the observation of clinical features preceded in time and influences the choice of medication, only the formers were kept in the multivariate models presented in Tables 3 and 4.
Variables Predicting Length of Stay in Multivariate Analysis
The results of the regression indicated the predictors explained 37% of the variance [R 2 = 0.37, F (5, 97) = 11.27, p < 0.001].
β represents the standardized regression weights. LL and UL indicate the lower and upper limits of a CI, respectively.
p < 0.05; ** p < 0.01; *** p < 0.001.
CGAS, Children-Global Assessment Scale; CGI-S, Clinical Global Impression-Severity; CI, confidence interval; SE, standard error.
Variables Predicting Therapeutic Outcomes in Multivariate Analysis
β represents the standardized regression weights. LL and UL indicate the lower and upper limits of a CI, respectively.
p < 0.05; ** p < 0.01; *** p < 0.001.
BD, bipolar disorder; CGAS, Children-Global Assessment Scale; CGI-I, Clinical Global Impression-Improvement; CGI-S, Clinical Global Impression-Severity; CI, confidence interval; SE, standard error.
No mathematical correction was made for multiple comparisons. List-wise deletion was used for missing value. The robustness of the analytical method was checked by confirming the main findings after the exclusion of outliners; that is, the six patients who had a length of stay above the 95th percentile ( = 256 days) (data available on demand). Data were analyzed using Stata-12 (StataCorp 2009).
Results
Aim 1: factors predicting the length of stay
The length of stay was significantly associated with longer duration of current episode [rs (106) = 0.28, p = 0.004], worse functioning at admission (CGAS score) [rs (106) = −0.31, p = 0.002], greater illness severity (CGI-S score) [rs (106) = 0.28, p = 0.004], aggressive behavior (respectively, median = 113.5 vs. median = 70.0, z = −2.34, p = 0.019), and parent–child conflict or poor parenting skills (respectively, median = 104.0 vs. median = 65.5, z = −3.21, p = 0.001). The association between the length of stay and other sociodemographic and clinical variables examined was not significant. Multivariate analysis concluded that duration of current episode and functioning (CGAS score) on admission were the bottom-line length of stay predictors (Table 3).
Aim 2: factors predicting the therapeutic outcomes
Greater functional improvement (based on CGAS score change from admission to discharge) was associated with lower functioning (CGAS score at admission, r = −0.52, p < 0.001) and greater illness severity on admission (CGI-S score, r = 0.24, p = 0.016), psychotic feature [respectively, M = 30.70, SD = 12.50 vs. M = 22.68, SD = 12.12, t(106) = −2.93, p < 0.001], bipolar disorder [respectively, M = 36.69, SD = 9.72 vs. M = 23.07, SD = 12.14, t(106) = −3.87, p < 0.001], and being admitted through the emergency room [respectively, M = 27.96, SD = 12.67 versus M = 21.79, SD = 12.02, t(106) = −2.54, p = 0.013].
Less functional improvement was associated with speech delay [respectively, M = 20.19, SD = 13.29 vs. M = 26.96, SD = 11.91, t(106) = 2.55, p = 0.012] and disruptive behavior disorder [respectively, M = 20.75, SD = 10.60 vs. M = 26.29, SD = 13.10, t(106) = 2.01, p = 0.048]. The association between the CGAS score change from admission to discharge and other variables examined was not significant. In multivariate analysis, degree of functional improvement was best predicted by level of function (CGAS score), illness severity at admission (CGI-S), and the diagnosis of bipolar disorder (Table 4).
Greater symptom improvement (based on CGI-I score) was associated with bipolar disorder (z = 2.47, p = 0.013, the number of comorbidities [rs (106) = 0.26, p = 0.001] and with a lower CGAS score on admission [rs (106) = 0.25, p = 0.001]. The association between the CGI-I score and other variables examined was not significant. In multivariate analysis, symptom improvement (CGI-I) did not have any independent predictors (Table 4).
ANOVA test showed that the mean change in the CGAS score during the hospitalization was statistically different across the three categories: “short-stay hospitalization,” “intermediate duration,” and “long-stay hospitalization”; overall ANOVA: F: 5.32, df = 2, p = 0.006. Post hoc tests revealed that the group with short-stay hospitalization had significantly lower change in the CGAS score between admission and discharge (M = 18.67, SD = 10.81) than the group with long-stay hospitalization (M = 29.78, SD = 13.25, Scheffé test p = 0.006) (Fig. 1). The mean change in the CGAS score in the group with intermediate duration (M = 25.47, SD = 12.15) was not statistically different across the groups with short- and long-stay hospitalizations (respectively, Scheffé tests p = 0.112 and p = 0.261).
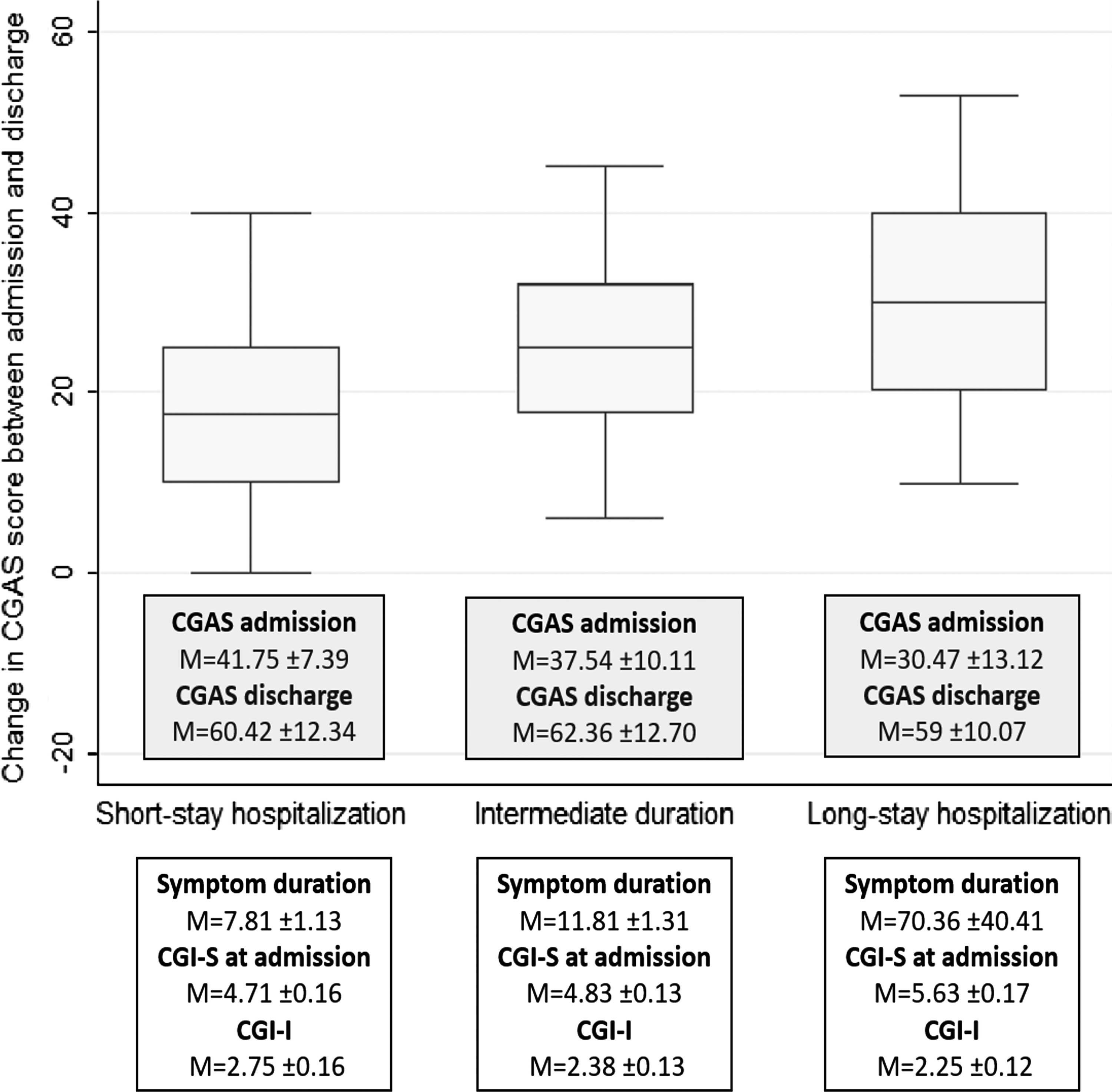
Change in Children-Global Assessment Scale score between admission and discharge in subjects with different durations of stay.
The proportion of inpatients considered as much or very much improved during their stay was 46% in the category “short-stay hospitalization,” 65% in the category “intermediate duration,” and 60% in the category “long-stay hospitalization.” In these three groups, the proportions of inpatients rated as minimally improved were, respectively, 33%, 29%, and 33%. The proportions of inpatients rated as not improved or worse were, respectively, 21%, 6%, and 7%. ANOVA test showed that the mean CGI-I score was not statistically different across the three categories; overall ANOVA: F: 2.50, df = 2, p = 0.087.
Additional analyses: effect of medication on length and therapeutic outcomes
Among adolescent inpatients with mood disorders, those receiving a non-selective serotonin reuptake inhibitors (non-SSRI) antidepressant or lithium at discharge had a longer length of stay compared with other inpatients. In addition, patients treated with electroconvulsive therapy (ECT) had a longer duration of stay. As shown in Table 5, a prescription of lithium was negatively associated with the CGI-I score and positively with Δ-CGAS.
Effects of Pharmacological Treatment on Length of Stay and Therapeutic Outcomes
Estimates with a level of statistical significance below 0.05 were noted in bold.
CGAS, Children-Global Assessment Scale; CGI-I, Clinical Global Impression-Improvement; ECT, electroconvulsive therapy; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor.
In multivariate analysis, when adding antidepressant, lithium, ECT as covariates in the multiple linear regression model predicting the length of stay (Table 4), the effect of the duration of current symptom, but not the effect of CGAS score at admission, remained significant. This likely reflects the strong association between the variable CGAS score at admission and non-SSRI antidepressant (β = −8.53, p = 0.040), lithium (β = 15.02, p < 0.001), or ECT (β = −21.79, p = 0.001).
When adding lithium as a covariate in the multiple linear regression model predicting functional improvement during the stay, the effects of the CGAS score at admission and the CGI-S score remained significant, while the effect of a bipolar diagnosis was not significant anymore. This likely reflects the strong association between the variable bipolar disorder and lithium (β = 0.82, p < 0.001). Finally, when adding lithium and first antipsychotic (anxiolytic dose) as covariates in the multiple linear regression predicting symptom improvement, the initial predictors remained nonsignificant.
Discussion
Length of stay
Only two variables significantly and independently predicted the length of stay in this sample of inpatient adolescents with mood disorders: the duration of the current symptoms and the CGAS score at admission. In our study, one-unit decline in the CGAS score at admission increased the length of stay by 2.3 days on average. The association between the overall level of functioning at admission and the length of stay was in line with findings from studies conducted in children and adolescent inpatients, regardless of the diagnostic categories (Gold et al. 1993; Stellwagen and Kerig 2010).
While the duration of current symptoms was positively associated with the length of stay, this variable did not predict symptom or functional improvement during the hospitalization. This is therefore likely that adolescents with a chronic course of mood symptoms require longer period of time before improving and finally being discharged than patients with more acute emotional disorder. The assumption that adolescents with chronic form of depressive disorder take longer time to improve is also consistent with the literature on staging model for mood disorders, which states that duration of untreated symptoms is a key factor to understand the progression of the natural course and the rate of resistant form of mood disorders (Malhi et al. 2014; Benarous et al. 2016).
Parent–child conflict or poor parenting skills predict the length of stay in univariate but not in multivariate analysis. This was consistent with the assumption that psychosocial factors are no longer associated with the length of stay when taking into account clinical factors (Borchardt and Garfinkel 1991; Stellwagen and Kerig 2010; Reddy et al. 2017), even though other studies contradicted this finding (Gold et al. 1993; Zeshan et al. 2018). Psychosocial factors may lead to poor prognosis through changes in clinical presentation. Our data support this view as post hoc analysis found a positive association between the duration of current symptoms and the presence of family conflict (z = −2.61, p = 0.001). However, psychosocial factors can also affect the patients' prognosis through the effect of nonspecific factors such as difficulties in accessing health care, understanding information about the disorder, or following treatment recommendations (Garno et al. 2005; Benarous et al. 2017). It is possible that the negative effect of these moderator factors on therapeutic outcome be less relevant in a context of full-time hospitalization rather than ambulatory care. This would explain why in our sample psychosocial factors did not predict symptom or functional improvement, unlike findings from secondary analysis of randomized controlled trial (Asarnow et al. 2009; Nilsen et al. 2013). This also illustrates how external factors influencing the length of stay are still subject to being mediated by the internal characteristics of hospitalized youth (Livingston et al. 1990).
Our findings also confirm the association between the length of stay and greater severity of psychopathology (Gold et al. 1993; Stellwagen and Kerig 2010) and aggression in hospital ward (Borchardt and Garfinkel 1991; Zeshan et al. 2018). However, the predictive values of these factors were relatively low and became nonsignificant when other factors were taken into account.
Therapeutic outcomes
Table 6 summarizes the main findings of our study. A low score of global functioning at admission was associated with greater functional and symptom improvement during the stay. A high level of clinical severity at admission predicted higher functional improvement in bivariate analysis, but lower functional improvement when other covariates were taken into account. Besides, a high level of clinical severity at admission had no effect on the level of symptom improvement during the stay.
Main Findings of the Study
In each case, the first symbol refers to univariate analysis, and the second symbol refers to multivariate analysis.
CGAS, Children-Global Assessment Scale; CGI-I, Clinical Global Impression-Improvement; CGI-I, Clinical Global Impression-Severity; ns, nonsignificant.
These findings contradicted results from randomized controlled trials, showing that a high level of functional impairment at baseline was associated with lower response rate to antidepressants (Emslie et al. 2011) or structured psychotherapies (Nilsen et al. 2013). It is worth reminding that these studies have rarely a follow-up period >12 weeks and frequently exclude patients with severe, comorbid, or treatment-refractory presentations.
Otherwise, this apparent paradoxical finding was also noted in observational studies conducted in adolescents hospitalized in long-stay inpatient units (i.e., several months on average) (Lyons and Schaefer 2000; Setoya et al. 2011; Serim Demirgoren et al. 2017) or those referred for severe psychiatric disorders, such as catatonia or bipolar disorder type-I (Benarous et al. 2017). This suggests that the change in the patient's level of functioning observed during the stay is likely to be affected by many factors not directly related to clinical severity but likewise positively influenced by the interventions provided during the stay.
The fact that in this study clinical and functional improvements were assessed at discharge and not after a fixed period of time (e.g., 12 weeks after the admission) is key to interpreting these findings. As shown in Figure 1, the patients were usually discharged when their CGAS scores reached ∼60. While a gradual decrease in CGI-I score was observed between patients with short stay, intermediate and long duration of stay, differences were not statistically significant (p = 0.087, Fig. 1). Based on these figures, patients within these three categories had comparable response rates with inpatient care. Most probably, inpatients with higher levels of functioning on admission (e.g., CGAS 40) took less time to get to a CGAS of 60 than those admitted with lower CGAS scores (e.g., CGAS 30). However, it cannot be said from these data whether some of these patients would benefit for longer duration of stay, or if they have already reached maximum hospital benefit. Interestingly, the visual inspection of the spline analysis of the correlation between change in CGAS score and length of stay showed a nonlinear relation (Supplementary Fig. S2), supporting heterogeneity in the individual response patterns to inpatient care. Person-centered analysis of longitudinal data collected regularly during the hospitalization could help determine the different trajectories of clinical and functional recovery during the stay, and then determine for which classes of inpatients prolonging stay could be useful.
While functioning often lags behind symptom change, it is interesting that here functioning change was more impressive than symptom change. This is likely because functional change in mood disorder takes longer to effect; it is therefore the benefit of a longer term hospitalization. Besides, adolescents whose mood symptom had decreased in the protective environment of the hospital may require longer stay to enable the consolidation and preclude a rapid surge of symptoms after discharge and readmission. In our experience, long-stay hospitalizations are often clinical situations associating vulnerabilities at multiple levels for which there are often associated family adversity and medicolegal issues (among the patients with long-stay hospitalization 47% reported at least one type of maltreatment, 27% have been exposed to sexual abuse, detailed report in Supplementary Table S1).
Although not significant, the relationship between the length of stay and the presence of speech delay and/or speech therapist intervention seems worth exploring in further studies. A link between language ability and youth's emotion regulation competence, a key developmental risk factor for mood disorders (Malhi et al. 2017), has been reported by several lines of research; that is, longitudinal community-based study, clinical study, or interventional study measuring the effect of speech therapy (Cole et al. 2010). As the content of many therapeutic interventions for adolescents with mood disorders is delivered orally (e.g., structured psychotherapies, group interventions, psychoeducation, family-focused interventions), language disorder constitutes an important prognostic factor to identify to provide more appropriate therapeutic options for the patients with the two conditions.
A diagnosis of bipolar disorder was associated with greater symptom and functional improvement compared with adolescents with depressive disorders. To better understand this finding, we subsequently reviewed the clinical chart of the 13 patients finally diagnosed with bipolar disorder. Of note six subjects were misdiagnosed at admission, and were finally diagnosed after several weeks of observation in different contexts and under several pharmacological treatments (e.g., after a mood switch induced by a SSRI prescription, or during the treatment of so-called acute psychotic episode psychotic or borderline personality disorder). In the total sample (N = 191), we found in post hoc analysis that the longer the hospitalization, the more likely an adolescent with chronic mood disturbances has to receive a diagnosis of bipolar disorder (BD) at discharge (12% in inpatients discharged before 8 weeks and 33% in those discharged after 32 weeks).
Analysis of the impact of medication prescribed at discharge on therapeutic outcomes was roughly consistent with the relation previously observed. First, the relations between lithium and greater clinical and functional improvement during the stay are likely to be mediated by the diagnosis of BD. Second, a longer duration of depressive symptom could account for the relation between the prescription of non-SSRI agents at discharge and longer duration of stay. Indeed, in line with general recommendation, non-SSRI medication was only prescribed to patients who did not respond to ∼8 weeks of SSRI (Dwyer et al. 2020).
Limitations
First, the specific characteristics of our hospital should be taken into account when discussing the generalizability of our results. Our hospital mostly serves patients with severe treatment-refractory illness, with an average length of stay longer than most psychiatric hospital settings. A substantial proportion of youth was addressed from another hospital in a context of treatment-refractory psychiatric disorders, as the department became an expert center for catatonic syndrome, bipolar disorder, and rare neurodevelopmental diseases with psychiatric manifestations (Consoli et al. 2014; Guinchat et al. 2015; Raffin et al. 2015). According to the CGAS score, most of the participants had a major impairment of functioning in several areas at admission, and participants were rated on average as “markedly ill” at the CGI-S, more than half had been previously hospitalized and 32% at least twice. This specificity of clinical practice (severe clinical profile, longer stay) may also be regarded as an opportunity, as managed care system, which results in inpatient stays of 2 weeks, rendered virtually impossible to study predictors of improvement in youth with severe and treatment-refractory mood disorders. It should be noted that our sample is likely to be free of sampling bias due to economic or patients' insurance characteristics as medical care is free of charge in France.
Second, the naturalistic design of the study would not allow one to collect information that may be pertinent to research purpose (e.g., patient's perceived alliance with the clinician, borderline personality traits) or to assess treatment efficacy under blind conditions. To limit the potential biases due to the assessment of psychosocial factors retrospectively, we used administrative data from child-protection agencies that were systematically sought during hospitalization in line with previous studies in inpatients with mood disorders (Marchand et al. 2005; Breton et al. 2012; Benarous et al. 2017).
Third, as noted above, a lack of statistical power due to a large number of variables and relatively small sample size made it difficult to interpret nonsignificant results.
Conclusion
This finding supports the value of measuring symptoms duration in predicting the hospitalization outcomes of adolescents with severe or treatment-refractory mood disorders, in view of addressing maintenance factors at an early stage. Future studies using repeated measures of therapeutic outcomes during the stay, adolescent's perceptions and follow-up information could help us gain knowledge on the optimal timing to start and stop inpatient treatment for adolescents with severe and treatment-refractory mood disorders.
Clinical Significance and Research Implications
Our research supports the value of measuring symptoms duration and functional impairment alongside symptoms severity in adolescents with mood disorders during treatment. This finding confirms the utility of the CGAS score at admission in predicting hospitalization outcomes (Green et al. 2001; Haggerty et al. 2014; Hayes et al. 2018). It is thus worth reminding that our average patient here was a boy from a reasonable socioeconomic background, with chronic depression associated with suicidal behavior. How these findings applied to population of adolescents with mood disorder is not well established.
Clinical features associated with severe presentation of mood episodes (i.e., psychosis feature, bipolarity, admission through emergency, high symptom severity, and low functioning) were associated with greater functional improvement. However, the association between speech delay and disruptive behavioral disorder decreased the likelihood of these patients to gain functional remission. More attention should be paid such that the modalities of therapeutic interventions for mood disorders provided during inpatient care be well adapted for patients with these associated problems.
As around half of the patients with bipolar disorder were misdiagnosed at admission, much remains to be done to better identify early-onset bipolar disorder and prevent the course of the disorder. Our findings support the importance to search for bipolar symptoms in adolescents with atypical mood disturbances (e.g., mood shifts with irritability, resistant depression, psychotic symptoms with elated mood) not only at admission but also repeatedly during the inpatient treatment. Among this sample of adolescent inpatients particularly enriched in chronic and refractory forms of mood disorders, a diagnosis of BD and prescription of appropriate medication (e.g., lithium) represented a therapeutic opportunity to gain better clinical and functional improvement during their stay.
While long-stay hospitalization has become the exception rather than the rule in adolescent psychiatry over the last decades, it is important to not fall into the opposite extreme, and to make room for some adolescents with severe and treatment-refractory mood disorders. From our data, it can be said that the proportion of good responders to inpatient care in terms of clinical and functional improvement were globally comparable, irrespective of the duration of stay (<6 weeks, between 6 and 30 weeks, and >30 weeks). While the most functionally impaired patients needed more time in hospitalization to improve significantly in terms of symptom severity and overall functioning, they finally did so if hospitalization last long enough.
It is also worth reminding that sometime long-stay hospitalization seems a better choice than a series of relapses and readmissions that can cause more disruption to patients' lives (Lifland et al. 2018). Therefore, long hospitalizations should not regard as “failed” because they are not fitted the usual 2 weeks standard of inpatient care. In some situations, such long stays provide an opportunity to address various maintenance factors that could not be otherwise treated. Further studies using longitudinal data with repeated measures of therapeutic outcomes during the stay, adolescent's perceptions, and longitudinal information on relapse risk could help us gain knowledge on the optimal timing to start and stop inpatient treatment for adolescents with severe and treatment-refractory mood disorders.
Footnotes
Acknowledgments
We thank Dr. Cosmin Iancu for his help in collecting data and the medical secretaries for their expert technical assistance.
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.