
Abstract
Objective:
This study aimed to investigate the serum levels of inflammatory markers in adolescents with major depressive disorder (MDD) using selective serotonin reuptake inhibitors.
Methods:
This was an 8-month observational study, involving 30 adolescents with and 38 without (control) MDD diagnosis. Demographic (age and gender) and anthropometric data (weight, height, and calculated body mass index [BMI] z score) were collected. Body composition was assessed with whole-body DXA scan. Depressive and anxiety symptoms were assessed using the Beck Depression and Anxiety Inventories (BDI-II and BAI), respectively. Serum levels of interleukin (IL)-6, IL-8, IL-1β, tumor necrosis factor, monocyte chemoattractant protein-1 (MCP-1), leptin, resistin, and adiponectin were measured using Bio-Plex Multiplex Immunoassays at baseline and after 8 months.
Results:
At baseline, patients with MDD and controls did not differ in age, gender, BMI z score, and fat mass index (FMI) z score. At follow-up, 58.3% (21/36) of patients with MDD were in full remission. Patients with MDD had higher levels of resistin at baseline (26274.16 pg/mL [16162.68–54252.72]) than controls (21678.53 pg/mL [11221.17–37343.27]; p < 0.01). This difference remained statistically significant after adjustment for sex, age, and FMI z score. No differences in other inflammatory markers were observed between the groups. By follow up, depressive and anxiety symptom severity had decreased significantly in patients with MDD in parallel with a decrease in the serum levels of TNF (p = 0.02), IL-8 (p < 0.01) and MCP-1 (p = 0.04). Among these markers, BDI-II score was positively correlated with serum levels of MCP-1.
Conclusion:
These results corroborate the view of involvement of peripheral inflammatory mechanisms in the pathophysiology of MDD in adolescents.
This trial is registered at
Introduction
Major depressive disorder (MDD) is estimated to affect >264 million people worldwide (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators 2018). The number of years lived with MDD increased by ∼15% between 2007 and 2017, in all age groups (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators 2018). It is estimated that half of major psychiatric disorders start before 15 years of age (Kessler et al. 2005). Among adolescents, MDD is associated with increased risk for suicide and illicit drug use as well as impaired academic performance (Avenevoli et al. 2015; Mendelson and Tandon 2016).
Peripheral inflammation has been consistently associated with depressive symptoms (Moulton et al. 2015; Hickie et al. 2018; Martins et al. 2019). In adults, elevated circulating levels of inflammatory markers, such as tumor necrosis factor (TNF), interleukin (IL)-6, and C-reactive protein (CRP) are associated with MDD (Howren et al. 2009; Dowlati et al. 2010; Strawbridge et al. 2015), and antidepressant treatment decreases their levels (Strawbridge et al. 2015). Furthermore, the use of anti-inflammatory interventions for MDD has shown promising results (Kohler-Forsberg et al. 2019).
Although the evidence supporting a role for proinflammatory mechanisms in adults with MDD is robust, there is a dearth of studies in youth. A recent meta-analysis showed the potential bidirectional association between MDD and proinflammatory markers (i.e., CRP and IL-6) in children and adolescents (Colasanto et al. 2020). However, the authors highlighted the small number of studies, preventing an adequate control of confounding factors that could have influenced this association (Colasanto et al. 2020). Since immune activity, including production of cytokines, may differ by age (Mitchell and Goldstein 2014), findings in adults cannot be readily extrapolated to younger age groups. Moreover, the pathways involved in the pathogenesis of MDD in adolescents and young adults are less influenced by confounding factors, such as chronic diseases (e.g., cardiovascular and metabolic diseases), which influence immune function (Hickie et al. 2018).
Given that the association between immune/inflammatory markers and MDD in adolescents requires further examination (Mills et al. 2013; Kim et al. 2014; Mitchell and Goldstein 2014), the current longitudinal study sought to investigate possible alterations in serum inflammatory markers in adolescents with MDD treated with selective serotonin reuptake inhibitors (SSRIs).
Methods
Data were obtained from participants enrolled in an observational study investigating the long-term effect of SSRIs on bone mass in adolescents (NCT02147184). The University of Iowa Institutional Review Board approved the study. Methods and main results of this study have been described elsewhere (Calarge et al. 2017).
In brief, male and female individuals, aged between 15 and 20 years, within a month of starting SSRI treatment or unmedicated were enrolled. Exclusion criteria included (1) treatment with psychotropic agents other than SSRIs during the 2 years before study entry, (2) presence of eating disorders, (3) substance use disorder, (4) severe medical conditions, and (5) pregnancy. All participants underwent an initial interview comprising the National Institute of Mental Health (NIMH) Diagnostic Interview Schedule for Children (DISC-IV) (Shaffer et al. 2000) as well as a clinical assessment by a child psychiatrist. At every visit, consensus diagnoses were generated following the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) (American Psychiatric Association 2000) based on all available information, including clinician- and self-completed symptom rating scales. Full remission of a depressive episode was defined as the resolution of all reported depressive symptoms. Participants were divided into control and MDD groups, with the baseline and 8-month assessments used.
Demographic (age and sex) and anthropometric data (weight and height) were collected. Body composition was assessed using whole-body DXA scan (Hologic QDR DELPHI-4500A unit or a Hologic Discovery A unit; Hologic, Inc., Bedford, MA). The two DXA units were cross-calibrated (Calarge et al. 2014). Age- and gender-specific z scores were generated for body mass index (BMI; calculated by the formula: weight/height2) and fat mass index (FMI; calculated by the formula: fat mass/height2) (Ogden et al. 2002; Weber et al. 2013).
Depressive and anxiety symptoms were assessed using the Beck Depression and Anxiety Inventories (BDI-II and BAI), respectively (Beck et al. 1961, 1988).
A fasting blood sample was collected. Serum levels of IL-6, IL-8, IL-1β, TNF, monocyte chemoattractant protein-1 (MCP-1), leptin, resistin, and adiponectin were measured using Bio-Plex Multiplex Immunoassays following the manufacturer's instructions (Bio-Rad Laboratories, Inc., Hercules), as routinely performed in our laboratory (Rocha et al. 2019).
Statistical analyses were performed using SPSS, version 26.0 (IBM Corp., Armonk, NY) and GraphPad Prism 5.0 (GraphPad Software, Inc., La Jolla, CA, EUA). The Kolmogorov–Smirnov test was used to test normality. The chi square test was used to compare categorical variables between those with and without MDD, and independent samples t-test and Mann–Whitney U test for continuous variables. Logistic regression was used to adjust comparison of the markers between the groups for age, sex, and FMI z score. To evaluate differences between visits, Wilcoxon test was used. MDD group was dichotomized into those who remitted from depression (full remission) and those who remained depressed (full episode) on follow-up. Pearson's and Spearman's correlation analyses were used to assess the potential association between inflammatory markers and psychiatric symptom severity of normally and non-normally distributed variables, respectively. Multivariable regression models examined the association between the inflammatory markers and the clinical parameters (BDI, BAI, FMI z score, SSRI use, and equivalent dose), using stepwise forward regression modeling. SSRI equivalent dose was defined as one SSRI unit as equivalent to 10 mg of escitalopram; 20 mg of fluoxetine, citalopram, or paroxetine; or 50 mg of sertraline (Deumic et al. 2016). Univariate analysis was performed to select clinical parameters associated with dependent variables when p < 0.20. Statistical significance was set at p < 0.05. Our sample size provides a statistical power >80% to detect an effect size of 0.70 in resistin level.
Results
Sixty-eight individuals were included in this study, of which 38 were diagnosed with MDD. Data on two participants with MDD were available at baseline but not at the 8-month follow-up. Patients and controls did not differ in age, gender, BMI z score, or FMI z score. As expected, the MDD group had higher baseline BDI-II and BAI scores (Table 1).
Demographic and Clinical Parameters of Depressive Patients and Controls at the Baseline
Mann–Whitney.
Chi-square.
Independent samples t-test.
BMI, body mass index; BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory-II; FMI, fat mass index; MDD, major depressive disorder.
At baseline, 28 participants with MDD were taking SSRI (fluoxetine, n = 10; sertraline, n = 7; citalopram, n = 8, escitalopram, n = 2, and paroxetine, n = 1). Five patients (13.2%) were using medications other than SSRIs (omeprazole, n = 3; propranolol, n = 1, and cetirizine, n = 1). At the 8-month follow-up, 58.3% (21/36) of patients with MDD had fully remitted and the rate of SSRI use dropped from 73.7% (28/38) to 41.7% (15/36) (Table 2).
Major Depressive Disorders Status and Selective Serotonin Reuptake Inhibitors Use at the Baseline and 8-Month Follow-Up Visit
MDDs, major depressive disorders; SSRIs, selective serotonin reuptake inhibitors.
Figure 1 shows serum levels of inflammatory markers in both groups, at baseline and follow-up. Patients with MDD had higher levels of resistin at baseline (Fig. 1G). This difference remained statistically significant after adjustment for potential confounders (sex, age, and FMI z score). No significant differences in the other inflammatory markers were observed.

Serum levels of
Depressive and anxiety symptom severity decreased significantly in patients with MDD on follow-up (from 20.8 [3–46] to 8.7 [0–29] in the BDI-II and from 12.7 [0–31] to 6.1 [0–22] in the BAI score; p < 0.01), in parallel with a decrease in the serum levels of TNF (p = 0.02), IL-8 (p < 0.01) and MCP-1 (p = 0.04) (Fig. 1A, C, E). Among these markers, BDI-II score positively correlated with serum levels of MCP-1 only at follow-up (Fig. 2). In a multivariate analysis, serum MCP-1 levels (adjusted R square = 0.328) were associated with BDI-II scores (β = 11.58, p < 0.01) and SSRI use (β = −144.2, p = 0.01) in participants with MDD. No other association between any of the other inflammatory markers, on the one hand, and the BDI-II and BAI scores or the use of SSRI, on the other, was observed.
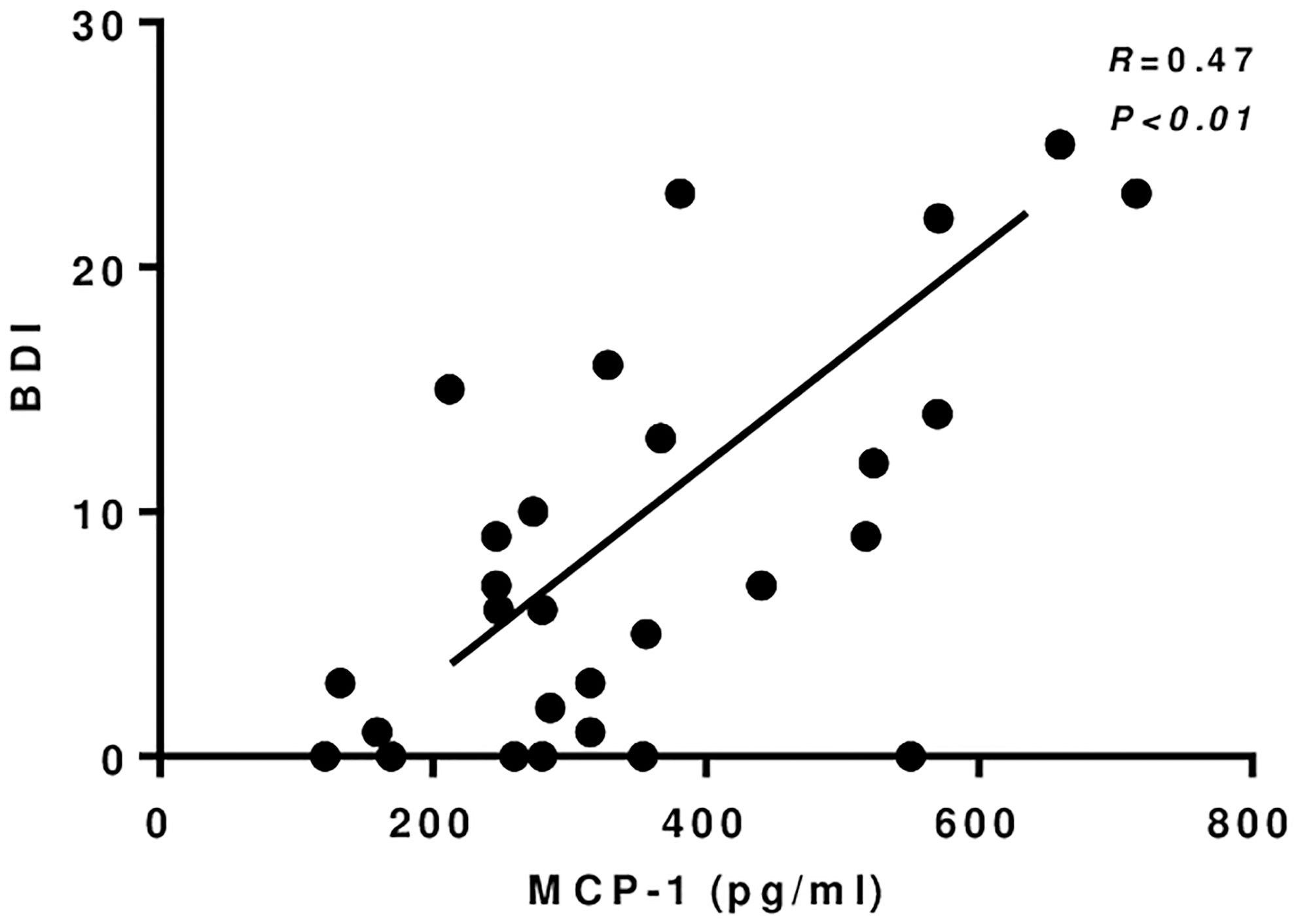
Correlation between MCP-1 and BDI-II at follow-up. BDI-II, Beck Depression Inventory Score-II; MCP-1, monocyte chemoattractant protein-1.
Discussion
The number and quality of studies examining inflammatory markers in adolescents with MDD are still limited, with less robust evidence implicating immune/inflammatory mechanisms as compared with the adult population (Mills et al. 2013; Kim et al. 2014). The main findings of this study include: (1) adolescents with MDD have higher serum levels of resistin than controls; (2) despite the improvement of depressive and anxiety symptoms occurring in parallel with the decrease of the serum levels of inflammatory markers (TNF, IL-8, and MCP-1), there was no clear association between them.
Resistin is an adipokine associated with the regulation of both central and peripheral insulin sensitivity (Benomar et al. 2013). The circulating level of resistin has been associated with insulin resistance in metabolic diseases, such as obesity and diabetes mellitus type 2 (DM2) (Su et al. 2019). Given that individuals with obesity and DM2 are more likely to develop MDD, this suggests that these conditions may share common pathophysiological mechanisms, such as inflammation, oxidative stress, and dysregulation of the hypothalamic–pituitary–adrenal axis (Moulton et al. 2015; Martins et al. 2019). In addition, recent studies have shown that childhood trauma might increase the circulating levels of resistin (Veru-Lesmes et al. 2021). The association between childhood trauma and depression in adolescents is well established (Gardner et al. 2019). Although history of trauma was not evaluated in this analysis, it is tempting to hypothesize that it might have contributed to the higher levels of resistin in depressed subjects. Only a few studies have evaluated circulating levels of resistin in MDD, with conflicting findings. Aliyazicioglu et al. (2011) observed lower serum resistin levels in adults with MDD compared with controls, whereas Papakostas et al. (2013) did not find any difference. Similarly, Pan et al. (2008) found no association between depressive symptom severity and plasma resistin level in middle-aged and older adults. In contrast, Lehto et al. (2010) found a positive correlation between serum resistin levels and depressive symptoms in adults. With regard to antidepressant treatment, Weber-Hamann et al. (2007) showed that plasma levels of resistin decreased in adult patients with MDD who remitted from depression after treatment with amitriptyline or paroxetine. To our knowledge, no study has examined circulating resistin concentration in adolescents with MDD. We found that resistin levels are increased in adolescents with MDD, but they were neither correlated with symptom severity nor with treatment response. Further studies are needed to fully characterize the association between resistin and MDD, especially in younger age groups.
Over the 8-month follow-up period, depressive and anxiety symptoms improved in parallel with changes in serum levels of inflammatory markers. The severity of depressive symptoms and use of SSRI were correlated with MCP-1 serum levels at follow-up. MCP-1 (also called chemokine (C-C motif) ligand 2; CCL2) is involved in immune responses through regulation of monocytes/macrophages migration to and infiltration of various organs, including the brain (Deshmane et al. 2009; Barnes et al. 2017). Recent meta-analyses have shown that circulating levels of MCP-1 are higher in adult patients with MDD (Eyre et al. 2016; Leighton et al. 2018) and bipolar disorder during depressive episodes (Misiak et al. 2020) compared with controls, suggesting that MCP-1 is likely to play a pathophysiological role in depression. In this study, correlation between MCP-1 and depressive symptoms occurred only at follow-up, highlighting the need for additional investigations.
Although we found a decrease in the serum levels of other markers at follow-up, they did not associate with change in depressive and anxiety symptom severity or with SSRI use. Previous studies have also failed to find a consistent longitudinal association between inflammatory markers and depressive symptoms. For instance, in a 6-year study, no association was observed between depressive symptoms as assessed by the BDI-II and serum IL-6 or CRP concentrations (Stewart et al. 2009). Similarly, Duivis et al. (2011) found that the association between depressive symptoms, as evaluated using the 9-item Patient Health Questionnaire, and inflammatory markers (IL-6, CRP, and fibrinogen) in patients with established coronary artery disease followed for 5 years was no longer significant after accounting for health behaviors (i.e., physical activity, current smoking, and BMI) (Duivis et al. 2011). Morris et al. (2011) also observed that the association between CRP and depressive symptom severity in women was no longer significant after controlling for metabolic risk factors (smoking, waist circumference, and systolic blood pressure by waist circumference) (Morris et al. 2011).
The limitations of this study include its open-label (or naturalistic) approach and the relatively small sample size. In addition, we did not control for some potential confounding factors (e.g., physical activity). It is worth mentioning that other potential confounders (medical comorbidities, polypharmacy, etc.) are much less prevalent in adolescents than in adults.
Conclusion
In sum, this was the first study to show alteration in serum resistin levels in adolescent patients with MDD and the putative association between MCP-1 and depressive symptom and SSRI use in these patients. These results corroborate the view of involvement of peripheral inflammatory mechanisms in the pathophysiology of MDD in adolescents. Future longitudinal studies involving larger samples are necessary to confirm these findings.
Clinical Significance
Although the evidence supporting a role for proinflammatory mechanisms in adults with MDD is robust, there is a dearth of studies in youth. A better understanding of the mechanisms involved in the pathophysiology of MDD in adolescents can contribute to the development of more efficient treatment strategies.
Footnotes
Acknowledgment
The Neuropsychiatry Program/Immuno-Psychiatry Lab is supported by the UT Health Department of Psychiatry and Behavioral Sciences.
Disclosures
No competing financial interests exist.