
Abstract
Objectives:
Children's Depression Inventory (CDI) is a self-report tool for measuring depression in children and adolescents. In this study, the psychometric properties of the Persian version of CDI were investigated in an Iranian adolescent population.
Methods:
This study was conducted on a sample of 480 adolescent boys and girls in the age range of 12–18 years. The results showed that 23.6% of the study population were 11–13 years old, 62.1% were 14–16 years old, and 14.3% were 17–18 years old. Also, 48.5% of the sample were girls, and 51.5% were boys. To investigate the convergent and divergent validity, Beck's Depression Inventory-Second Edition (BDI-II) and Teenage Inventory of Social Skills were used, respectively.
Results:
The reliability coefficient of CDI, based on Cronbach's alpha, indicated the relatively high internal consistency of the items (0.907). The results of the exploratory factor analysis showed that CDI has a saturated factor, explaining 50.11% of the variance in the data. Also, goodness-of-fit indices of confirmatory factor analysis showed that the model is well suited for explaining depression. The present results also showed a negative correlation between children's depression and the social skills subscale and a positive correlation between children's depression and BDI-II score.
Conclusions:
The construct validity of the questionnaire was confirmed. It can be concluded that the Persian version of CDI has adequate reliability and validity. Therefore, it can be used as a useful tool for early screening of depression in adolescents due to its easy use and specific design for children and adolescents.
Introduction
Depression is a mood disorder associated with emotional, vegetative, cognitive, and suicidal symptoms (Kaplan et al. 2014). Although there are similar diagnostic criteria for depression in children and adolescents based on the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5) (American Psychiatric Association 2013), a study of adolescents' depression showed that they expressed their depression in five ways: (1) misery and frustration; (2) anger and violence toward themselves and others; (3) a negative perspective toward life; (4) social isolation, and (5) low educational attainment (Midgley et al. 2015).
Depression has always been a major concern because of its high prevalence and long-term adverse effects on the individual's functioning. If this problem occurs in childhood, it can have long-term adverse consequences in adulthood (Giannakopoulos et al. 2009; Luby et al. 2014). The onset of this disorder at a younger age is one of the predictors of poor prognosis and is associated with a higher severity and longer duration of disorder (Kovacs and Lopez-Duran 2010). The high prevalence of depression in childhood and adolescence, besides its harmful effects on the individual's performance, such as poor school performance, interpersonal problems, drug abuse, and suicidal attempts, has made this disorder a global concern (Garber and Rao 2014; Wang et al. 2015).
According to epidemiological studies, the prevalence of depression is estimated at 0.4% in children, 0.4%–8.3% in adolescents (Costello et al. 2003), and 13.05% in Iranian Pupils (Mohamadi et al. 2017). Also, the mean age at onset of major depressive disorder and persistent depressive disorder was reported to be 10.98 and 8.71 years, respectively (Kovacs et al. 1997). The adverse effects of this disorder, in addition to its high prevalence and low average age at onset, have led the World Health Organization to address the incidence of depressive symptoms in children and adolescents as a serious mental health concern (Marcus et al. 2012).
Adolescence, as an important stage in a person's development, is accompanied by physical, psychological, and social changes, which can be a major source of stress for adolescents (Choudhury et al. 2006; Blakemore 2008). Therefore, these developmental changes, in addition to the associated stress, can influence the adolescents' vulnerability to depression. It is known that depression has significant effects on one's performance and quality of life (Garber and Rao 2014). Considering the adolescents' vulnerability to depression (Blakemore 2008), the relationship between age at onset and prognosis (Giannakopoulos et al. 2009), and the high prevalence of this disorder (Luby et al. 2014), early diagnosis, and timely interventions are of great significance (Saluja et al. 2004).
There are various tools and methods to examine depression. One of these methods is to use self-report questionnaires. These questionnaires are useful tools for initial screening, given the ease of implementation and the high speed of data acquisition. Numerous self-report questionnaires are used to measure depressive symptoms in adolescents. However, many of these questionnaires, because of their low construct validity and specificity, are only used as screening tools and are not applicable for estimating the diagnostic criteria (Myers and Winters 2002). One of the most commonly used scales is the Beck's Depression Inventory (BDI), which is a 21-item self-report questionnaire for measuring depression in adults, as well as adolescents (Beck 1987).
Another tool for assessing depression is the Center for Epidemiologic Studies-Depression scale, which is a 20-item self-report tool for screening depression in adults, in addition to adolescent populations (Roberts et al. 1990). The Reynolds Adolescent Depression Scale is another tool for measuring the severity of depressive symptoms in adolescents. This scale, with 30 items, was first developed by Reynolds in 1987, and its second edition was published in 2002. This scale contains four subscales of depression, including dysphoric mood, negative self-evaluation, anhedonia/negative affect, and somatic complaints (Reynolds 1987).
The Children's Depression Inventory (CDI), developed by Kovacs, is an extension of BDI for measuring depression in children and adolescents. It consists of 27 items and is applicable to pediatric populations, aged 7–17 years. Each item is rated on a three-point scale. The respondent is asked to select the item that best describes him/her in the last 2 weeks. Each item is scored from 0 to 2, with the total score ranging from 0 to 54. The final score indicates the severity of depressive symptoms, but cannot confirm a psychiatric diagnosis independently (Kovacs 1992).
The factor analysis of CDI yielded six factors, that is, depressive moods, social problems, externalizing, self-blame, school problems, and biological dysregulation (Craighead et al. 1998), representing the tool's potential to measure depressive symptoms in various domains. The main strength of CDI is its exclusive design for measuring depressive symptoms in children and adolescents. It also includes six domains of depressive symptoms assessment, making it a distinctive instrument.
Various studies have investigated the psychometric properties of CDI. The Arabic version of this scale was administered to Egyptian children and adolescents, aged 7–16 years. Its internal consistency and convergent and divergent validity have been validated by measuring test/retest reliability (Ghareeb and Beshai 1989). Also, in a study of internal consistency and factor analysis, the results indicated the high internal consistency of the scale and extracted four factors. Moreover, the relationship between demographic characteristics and depression scores was investigated.
The results showed that regardless of gender and race, age had a significant relationship with the final depression score, with older children showing more symptoms. Also, the relationship between depression and social skills was investigated in this study. The results showed that childhood depression was negatively correlated with strong social skills. In addition, excessive impulsivity was positively correlated with guilt/irritability (Helsel and Matson 1984).
Another study, comparing the factor structure of CDI in two groups of children and adolescents, examined the differences in the factor structure of this questionnaire. The results indicated that the first five factors were common in both groups, and the difference was attributed to the combination of these two factors (Weiss et al. 1991). In another study, to investigate the functional structure of CDI in children and adolescents with chronic pain, five factors were identified by two-stage exploratory and confirmatory factor analysis methods. The results indicated the effectiveness of this tool for measuring depression symptoms in this population (Logan et al. 2013).
As mentioned earlier, different factor models have been proposed for the CDI structure in different studies and populations. Kovacs, in the original model, proposed a five-factor and a single second-order factor model (Kovacs 1992). One of the objectives of the present study was to determine the factor structure of this inventory in an Iranian adolescent population.
Moreover, in a study using the Dutch version of CDI, the standardization and screening of this tool were evaluated in children and adolescents of both clinical and nonclinical populations. For this purpose, the relationship between CDI and DSM-based self-report instruments for anxiety and depression was assessed. The results showed that the CDI score had a significant correlation with depressive symptoms and a moderate correlation with anxiety symptoms. CDI was introduced as a useful tool for screening depression, as well as anxiety, to a lesser degree. A cutoff score of 16 for identifying the symptoms showed relative sensitivity and specificity, whereas a cutoff score of 21 showed higher sensitivity and specificity for identifying the symptoms in some subtypes (Roelofs et al. 2010).
The high prevalence of depression during adolescence, besides the significance of early diagnosis, highlights the need for early screening tools.
The literature search indicated the validity of CDI as a suitable tool for identifying depressive symptoms in children and adolescents (Nurcombe et al. 1989; Chan 1997), while the validity of BDI for evaluating depressive symptoms in adolescents (Ambrosini et al. 1991) and symptom screening was controversial (Beck and Steer 1993). Therefore, access to more reliable tools, specifically designed and approved for screening depressive symptoms in children and adolescents, is essential.
To facilitate the use of CDI in the Iranian population, the psychometric properties of its Persian version need to be confirmed. Therefore, this study aimed to investigate the psychometric properties of this scale, including factor structure, convergent validity, and divergent validity, in an Iranian adolescent population due to the lack of similar research in the adolescent population.
Besides, since the CDI assesses the universal symptoms of depression in children and adolescents, translation and evaluation of the Persian version of this questionnaire in an Iranian adolescent population can be helpful in evaluating and increasing its validity if approved.
Methods
In terms of data collection and methodology, it is considered a search study with a descriptive design. Correlational analysis, goodness of fit, factor analysis, and reliability analysis were performed to determine the correlations of variables in the questionnaire and to study the theoretical framework and standardization of the scale. In addition to the factor analysis method, convergent validity and divergent validity were also examined. Based on our review of the literature and the theoretical framework of most previous studies on depression and social skills, these variables were found to be associated with CDI. Therefore, we decided to use BDI-Second Edition (BDI-II) and Teenage Inventory of Social Skills (TISS) to assess the convergent and divergent validity of the scale.
Participants
Since the present study aimed to validate CDI via factor analysis, the minimum desirable sample size was considered to be 405 people. Considering the possible sample attrition, 500 people were finally selected as the sample size via multistage cluster sampling. The participants were selected among all male and female students studying at high schools in 22 districts of Tehran in the first half of the academic year 2018/2019. The cluster sampling method consisted of several steps, and the participants were selected in three stages. In the first stage, out of 22 districts of Tehran (Iran), 8 were randomly selected. In the second stage, from each district, 2 schools were chosen randomly (a total of 16 schools, 8 girls' schools and 8 boys' schools).
Finally, in the third stage, one class was randomly selected from the sample. An average of 31 students were recruited from each class. A total of 500 students completed the questionnaires; however, 20 questionnaires were excluded due to incomplete responses.
Measures
CDI: This scale is a self-report instrument, designed by Maria Kovacs, for assessing depressive symptoms in children and adolescents, aged 7–17 years. It includes 27 items on discomfort, self-blame, loss of appetite, insomnia, interpersonal relationships, and school adjustment. Each item includes three statements, describing the symptoms at three levels of intensity. Children are asked to choose the option that best describes them. The score of each item ranges from 0 to 2, with 2 indicating the greatest degree of depression. The total CDI score is the sum of scores of all items (Kovacs 1985).
BDI-II: BDI first was designed by Beck (1987) to measure all components of depression, based on Beck's theory of depression. The BDI-II contains 21 items, each rated on a Likert scale of 0 to 3; a higher score indicates more depressive symptoms. The minimum score of this questionnaire is 0, and the maximum score is 63; in samples of adolescent Psychiatric inpatients Osman et al. (2004), study showed that the reliability estimates of the BDI-II total and scale scores were good (range = 0.72 to 0.91). Toosi et al. (2017) confirmed the validity and reliability of this scale in a study of the psychometric properties of the Persian version of BDI-II in a population of high-school students.
TISS: This scale, which was developed by Inderbitzen and Foster, contains 39 five-choice questions. The respondent is asked to expresses his/her response to each question in a continuum of “It does not apply to me at all” to “it always applies to me.” The original version of this scale contained 40 items; however, one of them was omitted due to incongruence with the Iranian culture. The TISS items are grouped into two scales of positive and negative behaviors; the negative items are reverse-scored (Inderbitzen and Foster 1992).
If a person's TISS score is above average, he/she has high social skills, whereas if it is below average, he/she has low social skills. A score of 98 was considered to be average, according to the test standard. The reliability coefficients of this scale, reported by Inderbitzen and Foster (1992), were 0.9 and 0.72 for positive and negative items, respectively, and the internal consistency coefficient was 0.88. Also, the reliability of this scale was confirmed by Amini et al. (2013) in Tehran for female students in the second year of high school (0.71 and 0.68 for positive and negative items, respectively).
Translation
First, CDI was translated from English into Persian by two Iranian translators (with master and PhD degrees in clinical psychology, respectively), who were fluent in English. The two versions were then compared by an examiner (with a PhD degree in clinical psychology). After editing and revising the translated article, a PhD student, fluent in Persian and English, was asked to back-translate the Persian version into English. The back-translated article was then compared with the original version. There was no significant difference between the back-translated version and the original version.
Statistical analyses
In this study, our hypothesis was “Children's Depression Inventory (CDI) has good validity and reliability in Iranian adolescents.”
BDI-II and TISS were used to assess the convergent and divergent validity of the scale. Given the number of CDI items, which is 27 items and the minimum number of 15 samples for each item in factor analysis (Meyers et al. 2016), the minimum desirable sample size was considered to be 405 people. Considering the possible sample attrition, 500 people were finally selected as the sample size via multistage cluster sampling.
To investigate the construct validity of CDI, exploratory and confirmatory factor analysis methods were applied. The Kaiser–Meyer–Olkin (KMO) test and Bartlett's test of sphericity were used for sampling adequacy in factor analysis. Convergent and divergent validity was analyzed with the Pearson correlation coefficient test, and differential validity was analyzed with the independent t-test. Finally, Cronbach's alpha was performed to evaluate the reliability of the questionnaire.
All statistical analyses were performed with SPSS-22 and AMOS.24 version for Windows. The level of significance for all tests was set at a level of 0.01 (one tailed).
Results
Demographics and clinical characteristics
The analysis of demographic data showed that 23.6% of the study sample were 11–13 years old, 62.1% were 14–16 years old, and 14.3% were 17–18 years old. Also, 48.5% of the study sample were girls, and 51.5% were boys.
Sampling adequacy and extracted factors
First, the KMO test was performed for factor analysis of the 27-item CDI, which indicated a satisfactory coefficient (KMO = 0.89). Also, the result of Bartlett's test of sphericity was significant p < 0.0001 (χ 2 = 2035.72). Table 1 presents the information of extracted factors.
The Eigenvalues and Percentages of Variance Explained by the Extracted Factors of Children's Depression Inventory
The present study identified one general factor, which explained 50.11% of the variance in children's depression. The factor loadings of 27 items on one general factor (or more) are presented in Table 2.
Principal Component Analysis and Factor Loadings of 27 Items of Children's Depression Inventory
CDI, Children's Depression Inventory.
Considering the correlation coefficient of 0.30 as the minimum acceptable factor loading of each item on the extracted factor, the factor loadings of 27 items on one factor are presented in Table 2. Item 9 had negative factor loadings below 0.3 and was excluded from the questionnaire. As seen in Figure 1 in order to investigate the construct validity of the questionnaire, the first-order confirmatory factor analysis was performed. AMOS software was used to perform a confirmatory factor analysis.
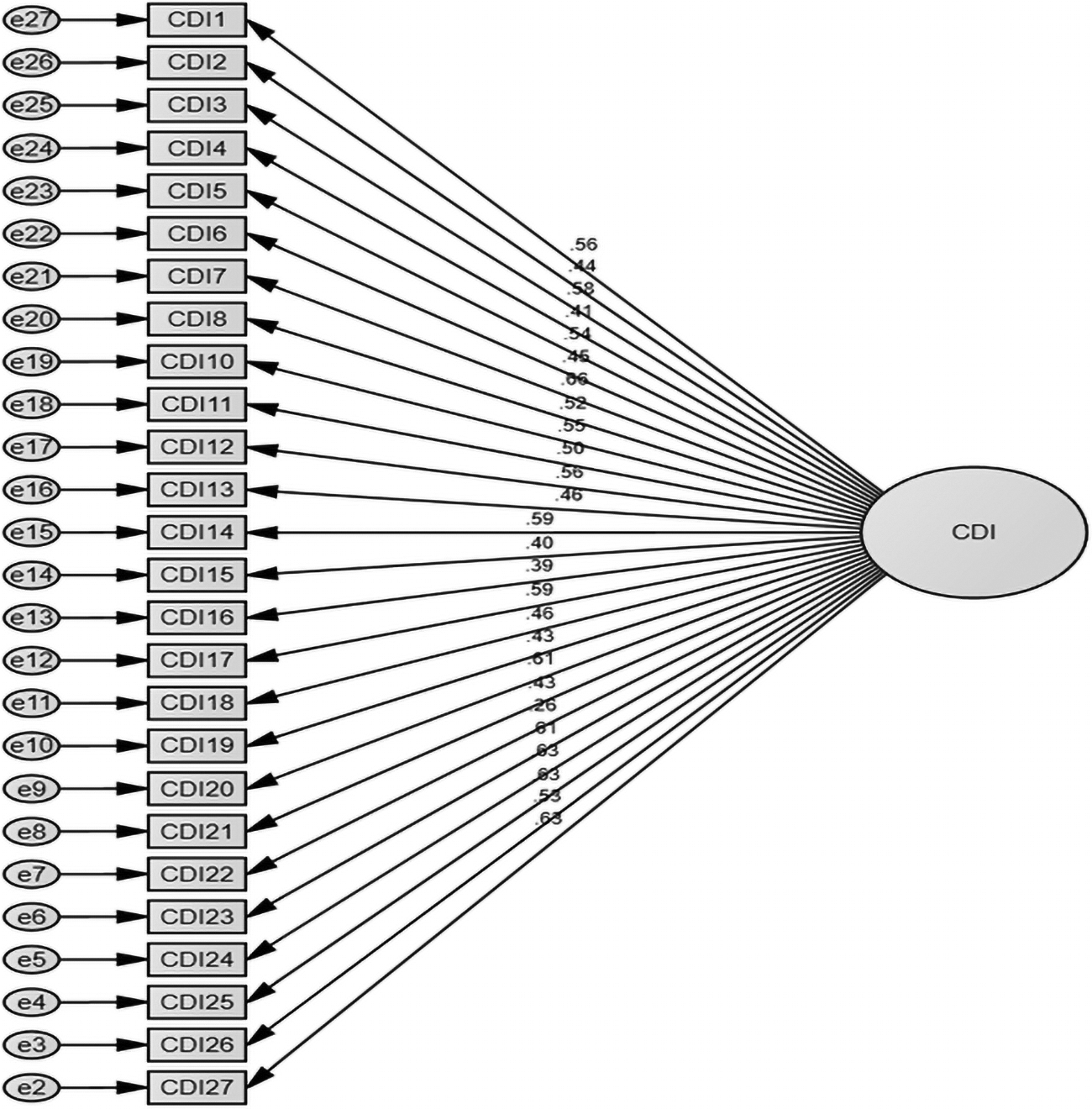
First-order confirmatory factor analysis with standardized coefficients. CDI, Children's Depression Inventory.
Based on the results presented in Table 3, it can be concluded that the model was well fitting for explaining depression. Also, the researcher's hypothesis, that is, CDI has a single-factor structure (26 items), was approved. The results of confirmatory factor analysis indicated that no item had an insignificant loading.
Confirmatory Factor Analysis of Fit Indices
Convergent, divergent, and differential validity
Two validated scales, that is, BDI-II and TISS, were used to investigate the convergent and divergent validity of CDI. The correlation coefficients between the variables are reported in Table 4.
The Correlation Coefficients Between Children's Depression Inventory, Beck's Depression Inventory, and Teenage Inventory of Social Skills
p < 0.01.
BDI-II, Beck's Depression Inventory-Second Edition; CDI, Children's Depression Inventory; TISS, Teenage Inventory of Social Skills.
The findings of the present study are consistent with the results of previous research on the negative correlation of childhood depression with social skills (p < 0.01). Also, the questionnaire scores had a significant positive correlation with BDI (p < 0.01). This confirms the convergent and divergent validity of CDI in adolescents. An independent t-test was also performed to investigate the differential validity of depression variables in girls and boys.
According to the information presented in Table 5, no significant difference was observed between boys and girls (p > 0.05).
Comparison of Depression in Boy and Girl Students
Internal consistency
To investigate the reliability of CDI, Cronbach's alpha method was used. The results related to CDI are reported in Table 6.
The Internal Consistency Reliability of Children's Depression Inventory
CDI, Children's Depression Inventory.
As can be seen in Table 6, the reliability coefficient of the total scale was satisfactory (α > 0.7).
Discussion
This study aimed to investigate the reliability, validity, and factor structure of CDI. Generally, translation and evaluation of the psychometric properties of a questionnaire can promote related research in a country; on the contrary, the increasing amount of research increases the validity of the scale.
Since this scale is the only scale fully compliant with the clinical diagnostic criteria of depression in children, and also can provide more accurate results in the assessment of depression in adolescents compared with BDI (Beck and Steer 1993; Chan 1997), its validation and factor structure can facilitate its application in research and screening, as well as clinical evaluations and mental health surveys in Iran.
Depression is associated with emotional, vegetative, cognitive, and self-image changes, in addition to suicidal thoughts and attempts, which usually lead to impaired performance and reduced quality of life (Kovacs et al. 1997). As mentioned earlier, CDI, which was developed by Kovacs (1992), is an extension of BDI for measuring depression in children and adolescents. In this study, it was found that CDI is valid for assessing depression in students of Tehran schools.
The exploratory factor analysis and confirmatory factor analysis methods were used to investigate the factor structure of CDI. The results of the exploratory factor analysis indicated that there was only one general factor in CDI. The highest factor loading was related to item 7, while the lowest factor loading was related to item 9, which was removed from the final version of the questionnaire. The one-factor model could explain 50.11% of the variance, indicating the optimal selection of items and the suitable theoretical construct. Also, according to the results of the confirmatory factor analysis, the single-factor structure of the scale was confirmed.
An important factor in identifying depression in a child or adolescent is the reliability of both the respondent and the survey tool, as well as appropriate methods for reproducing the scales. Diagnosis of a depressed child or adolescent is a major concern for psychologists, psychiatrists, counselors, social workers, school officials, and mental health organizations. It is also important for practitioners who use depression scales to be as familiar as possible with the application and origins of the scales, besides their key limitations (Reynolds and Johnston 2013).
The present results showed that the reliability coefficient of CDI, based on Cronbach's alpha, was 0.907, which indicates the relatively high internal consistency of items in the questionnaire; therefore, the results can be trusted. Another finding of the present study was that the prevalence of depression was similar in boys and girls. Also, the results of factor analysis showed that CDI is a one-factor model, which explains 50.11% of the variance in the obtained data in the Iranian sample; this result is in line with previous research (Helsel and Matson 1984; Ghareeb and Beshai 1989; Weiss et al. 1991) and with the assumption of Kovacs (1992) regarding the single second-order factor in the original model.
Analysis of divergent validity revealed that CDI scores were negatively correlated with social skills. Consistent with this finding, previous research has shown that CDI is highly correlated with depressive symptoms and is moderately correlated with anxiety symptoms (Roelofs et al. 2010). In a study by Kovacson children's depression, a general factor, with 27 items, was extracted, and the results indicated that CDI is both reliable and valid. Also, the validity coefficient of the scale was 0.87. In the present study, one general factor, with 26 items, was extracted (item 9 was omitted due to poor factor loading).
The present results showed that depression in children was not dependent on gender. In other words, the experience of depressive disorders in boys and girls was almost the same before adolescence (2–6 years). In this regard, factor analysis of the primary items of Kovacs's children and adolescent depression questionnaire was performed in male and female students of third and fourth grades of high school in Ahvaz, Iran. The results of factor analysis showed that there was no significant difference in the level of depression between boys and girls and between Arabic-speaking and Persian-speaking students (Raghabi and Attari 2004).
Conclusion
The present data suggest that the Persian version of CDI has adequate reliability and validity. Therefore, it can be used as a useful tool for early screening of depression in adolescents due to its easy use and specific design for children and adolescents
Clinical Significance
Given the high prevalence of depression among adolescents, the diagnosis of this condition can help select appropriate treatment interventions and improve the adolescents' health. Based on the results of the present study, CDI can be used to diagnose and screen depression in adolescents with excellent sensitivity. Therefore, we can confidently conclude that this tool is effective for diagnosing and screening depressive disorders in Persian-speaking adolescents.
Footnotes
Authors' Contributions
K.Q.B., Z.A.S., and S.H. contributed to the design of the study, conceptualization, and wrote the original draft. K.Q.B., Z.A.S., S.H., and S.A. acquired the data. M.S. and S.Z. devised the method, interpretation of data, and completed statistical analyses. S.A. revised. M.J. supervised on the study, critically reviewed, and approved the final submitted draft of the article.
Acknowledgments
The authors thank all those who helped them in this research, including the General Department of Education of Tehran and the officials of the schools and students who cooperated with them in this project.
Disclosures
K.Q.B. and S.Z. are from Allameh Tabataba'i University (Tehran, Iran); Z.A.S. is from the University of Social Welfare and Rehabilitation Sciences (Tehran, Iran); S.H. and M.J. are from Shahid Beheshti University of Medical Sciences (Tehran, Iran); M.S. is from the Institute for Cognitive Studies (Tehran, Iran); and S.A. is from Payame Noor University (Mazandaran, Iran), all where education and research are the primary functions. K.Q.B., Z.A.S., S.H., M.J., M.S., S.Z., and S.A. have nothing to disclose and has no financial relationships with any pharmaceutical company.