
Abstract
Objectives:
This study aimed to compare the efficacy of methylphenidate and atomoxetine on improving executive functions among children with attention-deficit/hyperactivity disorder (ADHD).
Methods:
This was an open-label, head-to-head, 3-month, randomized clinical trial with two-arm parallel-treatment groups: osmotic-release oral system methylphenidate (OROS-MPH; n = 79) and atomoxetine once daily (n = 78). Three major domains of executive functions were assessed, including response selection/inhibition, flexibility, and planning/working memory. The neuropsychological measures included the Conners' continuous performance test and the Cambridge Neuropsychological Test Automated Battery.
Results:
We found that both treatment groups showed improvement in executive functions (p-value <0.05 for the major indices of each domain). In addition, OROS-MPH was associated with a greater magnitude of improvement in the response selection/inhibition; the slope for detectability improvement in the Conners' continuous performance test was 0.06 for atomoxetine and 0.15 for OROS-MPH (p-value <0.01); the slope in rapid visual information processing was 2.22 for atomoxetine and 3.45 for OROS-MPH (p-value <0.05).
Conclusion:
Both OROS-MPH and atomoxetine improved various domains of executive functions in children with ADHD. There is greater improvement in response selection/inhibition among patients treated with OROS-MPH than those with atomoxetine. This trial was registered with
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder (Polanczyk et al. 2007) with manifestations of behavioral symptoms (Spencer et al. 2007) and deficits in executive functions (Pievsky and McGrath 2017) lasting to adulthood (Lin and Gau 2019). Executive function involves adaptive responses to novel or difficult situations and requires overcoming a habitual or automatic response (Hughes and Graham 2002). Several lines of research demonstrated that executive functions include three major domains as follows: response selection/inhibition, flexibility, and planning/working memory (Happé et al. 2006; Diamond 2013). The executive function deficits are associated with an increased risk for school maladjustment (Gau et al. 2015), social problems (Tseng and Gau 2013), and impaired peer relationships (Chiang and Gau 2014). In longitudinal studies, executive function in childhood could predict academic and social outcomes in adolescence (Miller and Hinshaw 2010).
Neuroimaging studies have shown that executive functions are regulated by distinctive brain areas, including the prefrontal cortex, thalamus, basal ganglia, parietal, and temporal lobes (Collette and Van der Linden 2002). For example, our previous work showed an association between disturbed structural connectivity of the frontostriatal circuitry and executive dysfunction in children with ADHD (Shang et al. 2013). Functional imaging studies demonstrated reduced blood flow and metabolism in the prefrontal cortex, which were corresponding to poor executive functions (Tripp and Wickens 2009). In addition, growing evidence has demonstrated reduced catecholamine input of the prefrontal cortex in patients with ADHD. Optimal levels of norepinephrine acting at postsynaptic alpha-2A-adrenoceptors and dopamine acting at D1 receptors were correlated with the executive functions (Arnsten and Li 2005).
Norepinephrine plays a critical role in memory and attention. For example, dysregulation of the locus coeruleus-norepinephrine system caused deficits in working memory capacity (Unsworth and Robison 2017). In addition, the norepinephrine system is involved in attentional control. The depletion of cortical norepinephrine has shown to lead to attentional deficits (Arnsten and Li 2005).
Dopamine is also important to executive functions. Increasing brain dopamine at an adequate level could improve attention, working memory, and cognitive flexibility in animal and human studies. However, high levels of dopamine might impair working memory and attention. The role of dopamine activity on response inhibition was also controversial (Arnsten and Li 2005). In contrast, the effect of norepinephrine on executive functions is more pervasive, including attention, response inhibition, cognitive flexibility, and working memory (Logue and Gould 2014). Of note, the medications for ADHD are aimed to enhance the dopamine and/or norepinephrine transmission in the prefrontal cortex (Arnsten and Li 2005; Tripp and Wickens 2009).
Methylphenidate and atomoxetine are medications approved by the Food and Drug Administration and widely used in Taiwan (Gau et al. 2006, 2007) and all over the world. The efficacy of these two medications on behavioral symptoms and social functions has been well-established in children and adults with ADHD in western countries (Spencer et al. 2000; Stuhec et al. 2019) and Taiwan (Gau et al. 2006, 2007, 2008). However, their comparative effects on executive functions remain to be studied (Gau and Shang 2010). Moreover, although a head-to-head study examining the effectiveness of these two drugs in modulating neuropsychological functions in adults with ADHD has been performed (Ni et al. 2013, 2016), to the best of our knowledge, there is no report of a head-to-head study with long-term treatment to investigate their comparative effects on the executive functions in children with ADHD (Cortese et al. 2017).
Methylphenidate inhibits the reuptake of dopamine and norepinephrine, thereby enhancing dopamine neurotransmission in the prefrontal cortex, striatum, and a variety of other brain regions (Wilens 2008) and norepinephrine transmission in locus coeruleus, raphe nuclei, thalamus, and thalamic subnuclei (Hannestad et al. 2010). A growing body of evidence has demonstrated that methylphenidate could improve executive functions in patients with ADHD (Coghill et al. 2014). However, several studies failed to show the beneficial effects of methylphenidate on response selection/inhibition and planning/working memory (Rhodes et al. 2006). The results of studies describing the effect of methylphenidate on improving executive functions were inconclusive. Atomoxetine, another commonly used drug for ADHD (Stuhec and Locatelli 2017), is an inhibitor of the presynaptic norepinephrine transporter and carries a very low affinity for the dopamine transporter (Bymaster et al. 2002). Noradrenaline transporter is primarily responsible for the clearance of dopamine in the prefrontal cortex; therefore, atomoxetine increases both extracellular norepinephrine and dopamine in the prefrontal cortex (Arnsten 2009).
However, studies examining the effect of atomoxetine on executive functions are sparse and inconsistent (Faraone et al. 2005; Gau and Shang 2010). Functional imaging studies showed that methylphenidate and atomoxetine had differential effects on brain activities, which were correlated with reductions in ADHD symptoms (Chou et al. 2015; Shang et al. 2016). Atomoxetine decreased activations in the dorsoanterior cingulate cortex and dorsolateral prefrontal cortex, which correlated with improvement in focused attention while methylphenidate increased activations in the inferior frontal gyrus, which related to improvement in response inhibition (Chou et al. 2015).
Since the underlying mechanisms of action between methylphenidate and atomoxetine are different, we investigated whether there are differential effects on executive functions as well. A few studies have compared the effects of these two medications on the executive functions of children with ADHD (Yildiz et al. 2011; Yang et al. 2012; Bédard et al. 2015). Although several studies suggested that methylphenidate might improve executive functions more effectively than atomoxetine (Bedard et al. 2004; Nandam et al. 2011; Yildiz et al. 2011; Kratz et al. 2012), two studies showed no different effect on attention (Kratz et al. 2012; Ni et al. 2016) and one study found that atomoxetine has significantly greater efficacy in improving spatial planning than methylphenidate. These inconsistent results may be due to small sample size or short-term follow-up observation; most studies were followed <10 weeks (Nandam et al. 2011; Kratz et al. 2012; Yang et al. 2012; Bédard et al. 2015). In addition, most studies were conducted in Caucasian populations except for one research in the ethnic Chinese population (Yang et al. 2012). Hence, we directly compared the efficacy of receiving osmotic-release oral system methylphenidate (OROS-MPH) and atomoxetine in improving executive functions in children with ADHD in Taiwan. We hypothesized that OROS-MPH and atomoxetine would be effective in improving executive functions with some difference in the magnitude of improvement, especially regarding sustained attention and response selection/inhibition.
Methods
This study was approved by the Research Ethics Committee of National Taiwan University Hospital, Taiwan (ID: 200812153M;
Study participants
Eligible participants, aged between 7 and 16 years, had a Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV; American Psychiatric Association 1994) diagnosis of ADHD, confirmed using the Chinese version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Epidemiological (K-SADS-E) Version (Gau et al. 2010). In addition, participants needed to be ADHD medication naive and rated as moderately ill or worse using the Clinical Global Impressions-ADHD Severity (CGI-ADHD-S) Scale, with a score of at least 4 or more on a range of 1 (normal, not at all ill) to 7 (extremely ill). The CGI-ADHD-S is a single-item assessment of the global severity of ADHD symptoms about the clinician's total experience with other ADHD patients, and its Chinese version has been widely used in clinical trials in Taiwan (Gau et al. 2007, 2008; Gau and Shang 2010).
We excluded patients who had comorbid conditions, including bipolar disorder, psychosis, any substance abuse, autism spectrum disorder, intellectual disability (Full-scale intelligent quotient <80), or have serious medical conditions, such as cardiovascular disease or a history of seizures. The details of diagnosis and assessments have been reported in our previous work (Shang et al. 2015).
Study design and procedures
Participants with ADHD were assigned in a 1:1 ratio to receive OROS-MPH or atomoxetine, after having been divided according to a computer-generated random sequence. This head-to-head randomized clinical trial was a 24-week open-label study. Participants were assessed seven times: at baseline (visit 1), week 2 (visit 2), week 4 (visit 3), week 8 (visit 4), week 12 (visit 5), week 16 (visit 6), and week 24 (visit 7). At visit 1, participants commenced with OROS-MPH being administered at a single morning dose of 18 mg per day or atomoxetine at a single morning dose of 0.5 mg/kg per day in the first week and 1.2 mg/kg per day thereafter, if the participants can tolerate atomoxetine. Drug dosage was titrated based on treatment response and adverse effects at visits 2–7. The maximal daily dose was 54 mg daily for OROS-MPH or 1.2 mg/kg daily for atomoxetine.
Clinical assessments
Information for basic physical conditions (body weight and height, blood pressure, heart rate) and ADHD symptoms (as assessed by ADHD Rating Scale-IV-Parent version (Pappas 2006) the CGI-ADHD-S and parent-, teacher-, and self-reported Swanson, Nolan, and Pelman-IV [SNAP-IV]) (Gau et al. 2008) were measured at each visit. Adverse effects of medications were clinically assessed from visit 2 through visit 7.
Executive function assessment
Executive functions include three major distinct domains: response selection/inhibition, flexibility, and planning/working memory (Happé et al. 2006; Diamond 2013). In this study, these functions were measured using the Conners' Continuous Performance Tests (CCPTs) for response selection/inhibition and four tasks of Cambridge Neuropsychological Test Automated Battery (CANTAB), including the Rapid Visual Information Processing (RVIP) for response selection/inhibition; Intra-Extra-Dimensional (IED) Set Shifts for flexibility; Stockings of Cambridge (SOC); and the Spatial Working Memory (SWM) for planning/working memory. CANTAB is a computerized test with standard procedures and widely used for measuring a variety of neuropsychological functions (Lin et al. 2013). The validation and reliability in CANTAB tasks involving executive abilities were well established (Gau and Shang 2010).
The dose was properly titrated, and the drug effects were stable in the first 4 weeks. Thus, we tested the executive functions at visit 1 (baseline) and visit 3 (week 4) and explored the long-term effect on visit 5 (week 12). Most assessments were conducted in the morning clinics.
Response selection/inhibition
The CCPT is a sensitive test of sustained attention and response selection/inhibition. The correlations between CCPT measures and ADHD symptoms are well established (Epstein et al. 2003). In the test, we administered a letter that appeared on the computer screen and subsequently changed to another letter. The display time of each letter was 250 ms, and the interstimulus intervals varied from 1 to 4 seconds randomly. The participant had to press the space bar for every letter (signal) except the letter “X” (noise). Three major indices included (1) omission errors: the number of errors involving missed signal letters, indicating sustained attention; (2) commission errors: the number of incorrect responses to noise letters, measuring the ability of response inhibition; and (3) detectability: assessment of the participant's discriminative power between the signal and noise distributions, indicating the overall ability of response selection/inhibition.
The RVIP is similar to the CCPT. Digits (ranging from 2 to 9) appear in a random order (Gau and Huang 2014). The participant had to detect three target sequences (3–5–7, 2–4–6, 4–6–8) and respond within 1800 ms after the appearance of the last number. Three major indices were included: (1) probability of hits: total correct hits divided by the sum of total hits and total misses, indicating sustained attention; (2) probability of false alarms: total incorrect hits divided by the sum of total incorrect hits and total correct rejections, measuring response inhibition; and (3) A′ (detectability): a signal detection measure of sensitivity to the target, indicating overall response selection/inhibition.
Flexibility
The IED test assessed the participant's flexibility of rule acquisition and reversal. The participants needed to pay attention to the specific attribute of compound stimuli (color-filled shapes or white lines) across different examples (intradimensional shift) and then to shift their attention to different attributes of the stimuli (extradimensional shift [EDS]) (Downes et al. 1989). Throughout this task, the participant had to discover rules, initially through trial and error. Once the rule was acquired on six correct responses, the computer would change the rule. The participant needed to disregard the previous rule and acquire a new rule. Four target indices for flexibility were included: (1) completed stages: the number of stages completed; (2) pre-EDS errors: the number of errors made before the EDS stage; (3) EDS errors: errors made in the EDS stage; and (4) adjusted total trials: the adjustment adds 50 for each stage not attempted due to failure at an earlier stage.
Planning/working memory
The SOC is a test to assess the participant's spatial planning and functions. The participants were required to move balls to a goal position as few moves as possible. In the beginning, three suspended vertical stockings and three colored balls were presented on the monitor screen. Participants were required to move the colored balls, in a single move at a time, between the stockings to fulfill a goal position within a specified number of moves in the problem-solving condition, and subsequently, they were required to copy each move by following the identical sequence of moves played back by the computer, based on their employment of problem-solving in the control condition. Two major indices were measured: (1) spatial problem-solved in minimum moves: the number of occasions that were completed in the minimum possible number of moves; and (2) total moves: the number of moves taken more than the specified minimum number, but within the maximum allowed.
The SWM assessed the ability of manipulation of visuospatial information and nonverbal working memory. In the beginning, several boxes were showing on the screen. There was a hidden token in the boxes, and the participant selected boxes and used the method of elimination to find it. Once the token was found, there would never be another token inside the same box. Thus, the participant needed to remember those boxes that had been searched to avoid inefficient searches. The order of searching was determined by the participants themselves. The number of boxes started at two and increased to eight boxes gradually. Two major indices include the following: (1) strategy utilization: the number of search sequences used to start with a novel box in the difficult problems; and (2) total between errors: the number of errors where the participant chose a box in which a token had already been found.
Data analysis
Baseline demographic characteristics, symptom severity, and baseline neuropsychiatric assessments were presented in mean scores and standard deviation for continuous variables and the number and the corresponding percentage for categorical variables. We used the intent-to-treat principle in the statistical analysis. Thus, the last observation carried forward method was applied to missing data or patient dropout. Hierarchical linear mixed-effect models were conducted to address the lack of statistical independence of repeated measurements of the same participants over time. Cohen's d was used to compute the effect size for the comparisons between week 4 and baseline and between weeks 12 and baseline. The effect size of Cohen's d was considered small, medium, or large when the value was 0.2 to 0.5, 0.5 to 0.8, and ≥0.8, respectively. In particular, both intercepts and slope (time) effects in the linear mixed model with time-dependent variables were treated as random effects. This was done to account for variations among subjects in baseline values and slopes for individual trajectories of neuropsychological parameter changes over three assessments, in addition to the main treatment and fixed-time effect of the two treatment groups. To test the difference in the slope of change between two treatment groups, the interaction terms between visits × drugs were tested.
In addition, we extended our analysis to the Pearson correlations of the changes of clinical symptom severity (the CGI-ADHD-S, the inattention subscale, and hyperactivity-impulsive subscale of ADHD Rating Scale-IV-Parent version) with the executive functions (CCPT, CANTAB). The details of drug effects on clinical symptom severity were reported in our work (Shang et al. 2015). SAS version 9.4 was used to conduct statistical data analysis. The alpha value was preselected at the level of p < 0.05.
Results
Of the 174 patients screened, 160 patients were enrolled and randomly assigned to the OROS-MPH (n = 80) or atomoxetine (n = 80) groups. Among them, 79 patients treated with OROS-MPH and 78 patients treated with atomoxetine received CCPT. Given that CANTAB was only applied to patients aged 8 years or more, 56 patients treated with atomoxetine and 50 patients treated with OROS-MPH have received CANTAB (Fig. 1). There were no statistically significant group differences in demographic characteristics, clinical profiles, and baseline cognitive functions (Table 1). During the follow-up period, there were eight patients treated with OROS-MPH, and five patients treated with atomoxetine dropped out at week 12. The baseline characteristics for those dropped are shown in the Supplementary Table S1. The details of reasons for dropout had been reported in our previous study (Shang et al. 2015). In addition, there was no significant difference in drug adherence between the two treatment groups (Shang et al. 2015).
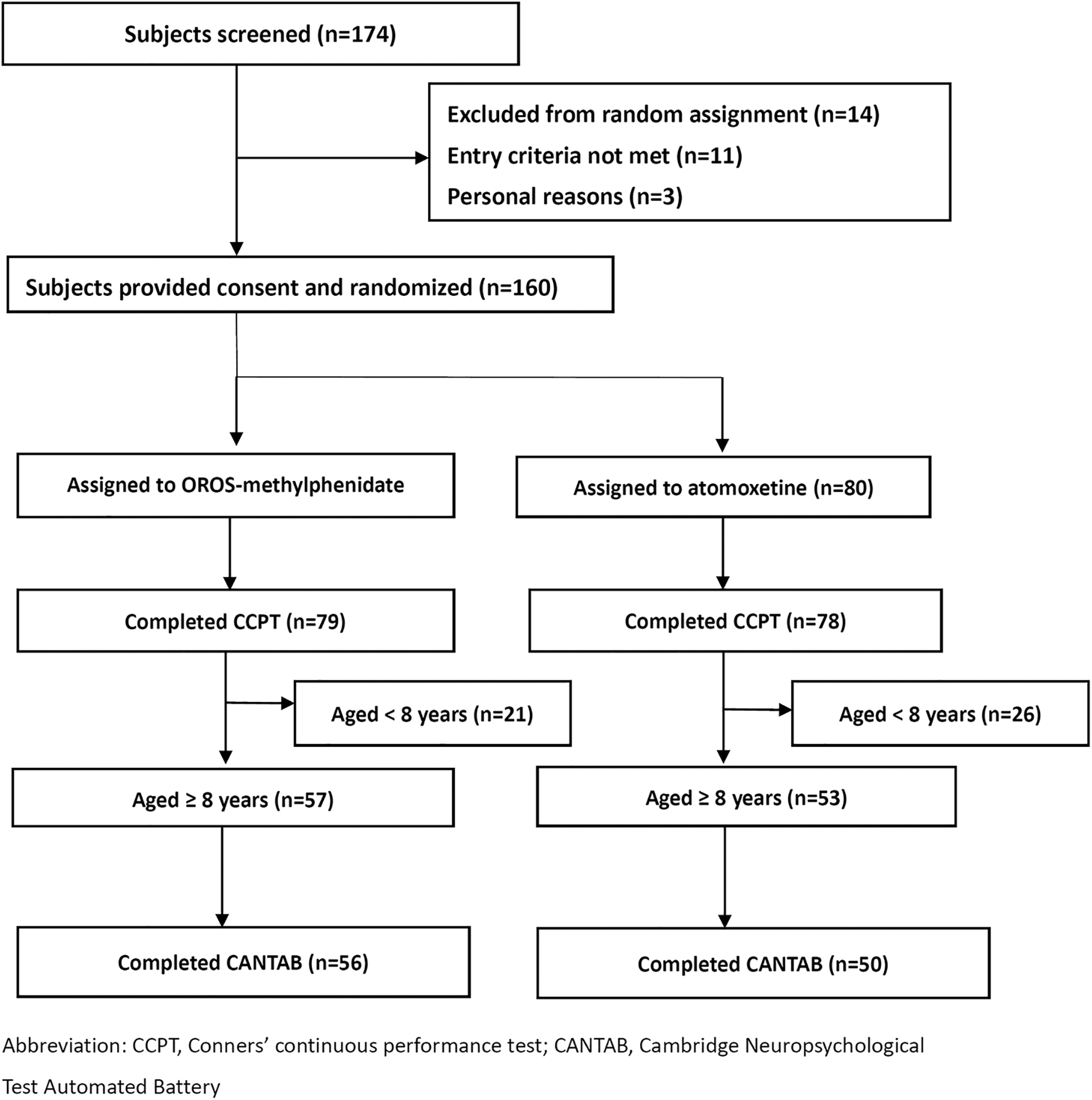
Flow chart of the randomization procedure.
Demographics, Clinical Symptoms, and Executive Functions at Baseline Among Study Patients
There were 56 patients who were administered with atomoxetine and 50 patients with methylphenidate that finished CANTAB; there was no difference in age, gender, clinical, and cognitive profiles between the two groups among those that finished CANTAB.
CANTAB, Cambridge Neuropsychological Test Automated Battery; CGI, Clinical Global Impressions; IQ, intelligent quotient; SD, standard deviation; SNAP-IV, Swanson, Nolan, and Pelman-IV.
Comparison of clinical profiles and executive functions in baseline
There was no statistically significant difference in the performance of baseline executive functions between these two groups (all p-values >0.05) except that patients treated with atomoxetine have a higher number of strategy utilization in SWM than those with OROS-MPH (Table 1). The details of executive functions at week 4 and weeks 12 are shown in the Supplementary Table S2.
Response selection/inhibition
In the CCPT, both atomoxetine and OROS-MPH groups showed decreased commission errors and improved detectability significantly over the study period. Interaction analysis revealed that the magnitude of increasing detectability and reducing commission errors was significantly greater in the OROS-MPH group (Cohen's d = 0.74 and −0.78, respectively) than the atomoxetine group (Cohen's d = 0.32 and −0.47, respectively). Decreasing omission errors were noted only in the OROS-MPH group (Table 2).
Changes of Executive Functions from Baseline to Week 4 and 12 in the Methylphenidate and Atomoxetine Groups
p < 0.05. ** p < 0.01. *** p < 0.001.
SD, standard deviation.
Similar findings were noted in the RVIP. The probability of hits and detectability (A′) improved after both treatments. However, the probability of false alarm did not change obviously. The slope of improving detectability is more prominent in the OROS-MPH group (Cohen's d = 1.41) than the atomoxetine group (Cohen's d = 0.66, Table 2).
Flexibility (IED)
In the IED set shift, EDS errors, pre-EDS errors, and adjusted total trials significantly decreased from baseline to the end points for the two groups. There were no significant group differences in the slope of improving IED set shift performance.
Spatial planning (SOC)/working memory (SWM)
The SOC assessed spatial planning. We found that the total moves of SOC needed to complete the tasks reduced after treatment with both OROS-MPH and atomoxetine across the 12 weeks. The number of problems solved with minimum moves significantly increased early at week 4 in the OROS-MPH group and week 12 for both groups without significant group differences in the slopes (Table 2).
In the SWM, we found that the strategy utilization improved after treatment and total between errors decreased from baseline to week 4 and end point for the two groups, but the slope of improvement was significant only in the atomoxetine group without a statistically relevant group difference in the slope of improvement (Table 2).
Correlations between the changes of clinical symptom severity and executive functions
The correlations between clinical symptom severity and executive function were relatively weak. We found that there were negative associations between the detectability of CPT among patients treated with OROS-MPH but null findings among patients treated with atomoxetine. In addition, we did not find any association between clinical severity and the executive function in CANTAB (Supplementary Table S3).
Discussion
Main findings
In this head-to-head randomized clinical trial in children with ADHD, we found that both medications, OROS-MPH and atomoxetine, improved executive functions, including response selection/inhibition (CCPT and RVIP), flexibility (IED), and spatial planning and working memory (SOC and SWM). In addition, the significantly greater magnitude of improvement over time in the sustained attention and response selection/inhibition was found in the OROS-MPH group than the atomoxetine group. The magnitude and timing of improvement in spatial planning were greater and faster in the OROS-MPH group than that in the atomoxetine group, despite no group difference in the slope of improvement.
Response selection/inhibition
Our findings that both OROS-MPH and atomoxetine have a beneficial effect on improving sustained attention (increasing probability of hit or decreasing omission errors) and response selection/inhibition (reducing commission errors) were in line with previous studies (Bédard et al. 2015). We used two different test batteries to measure sustained attention and response selection/inhibition and found consistent results, which further supported the robustness of our findings.
Of note, OROS-MPH was more effective than atomoxetine, particularly in the tasks measuring sustained attention and response selection/inhibition. These findings were in line with previous studies in the youth (Nandam et al. 2011; Bédard et al. 2015) and adult (Ni et al. 2013) populations. Moreover, another randomized controlled study also showed that methylphenidate improved sustained attention and reduced reaction time and reaction time variability in 102 youths with ADHD (Bédard et al. 2015).
These findings might be attributed to the difference in the mechanisms of action between these two drugs. In one neuroimaging study, atomoxetine decreased activation in the dorsolateral prefrontal cortex, which correlated with improving focused attention (Chou et al. 2015). However, atomoxetine might have little effect on the subcortical dopaminergic system (Bymaster et al. 2002). It should be noted that subcortical striatum activation plays an important role in inhibitory control (Zandbelt and Vink 2010). In contrast, methylphenidate increased activation in the inferior frontal gyrus, which is associated with decreased severity of impulsivity (Chou et al. 2015). In addition to the prefrontal cortex, methylphenidate (Tomasi et al. 2011) was associated with decreased activity of the default mode network, thereby filtering noise stimuli and enhancing attention. Furthermore, methylphenidate could enhance the dopamine level in the ventral striatum, which might be associated with improving attention and inhibitory control. Altogether, these different mechanisms of action of the two medications might partially explain the fact that methylphenidate was more effective than atomoxetine with respect to sustained attention and response selection/inhibition.
Flexibility
We found that both medications have a beneficial effect on the flexibility measured by the IED test. Our findings support one placebo-controlled clinical trial, which showed that methylphenidate improved visual set shifting (Konrad et al. 2004). Another open-label trial showed that atomoxetine improved attentional set shifting in children with ADHD (Gau and Shang 2010). We found that atomoxetine and methylphenidate had comparable effects on these executive functions, which is consistent with several studies (Yang et al. 2012). In one 4- to 6-week randomized controlled trial, both methylphenidate and atomoxetine improved cognitive flexibility measured by Stroop color-word task in children and adolescents with ADHD, with no significant difference between the two medications (Yang et al. 2012). Although the underlying mechanism of action was different between the two medications, they might share a common pathway in the prefrontal cortex area after an adequate lapse in the duration of treatment.
Planning/working memory
The planning and working memory measured by SOC and SWM improved in both medication groups. These results were consistent with previous clinical trials (Konrad et al. 2004; Mehta et al. 2004). The working memory was highly related to the dopaminergic modulation of the frontostriatal circuitry (D'esposito and Postle, 2015). The mechanism of action between methylphenidate and atomoxetine was different, but these two medications could directly or indirectly enhance the dopaminergic pathway (Arnsten and Li 2005), thereby enhancing working memory.
Correlations between the changes of clinical symptom severity and executive functions
We found that the change of the detectability of CPT was weakly correlated with the improvement of clinical symptom severity among patients treated with OROS-methylphenidate. However, such findings were not replicated in the RVIP of CANTAB. In addition, there were null associations of clinical symptom improvement with the change of other executive functions. We thought that the drug effect on patients might be heterogeneous; some patients get more benefits in clinical symptoms but the others improve their executive functions more dominantly. The role of executive function change on the therapeutic effect on clinical severity needs further evaluations.
Strength and limitations
This work describes one of the first head-to-head randomized clinical trials comparing the effects of OROS-MPH and atomoxetine directly in executive functions among children with ADHD. The major strengths of this work included longer duration of treatment, and comprehensive and well-validated neuropsychological tests were used to assess executive functions.
However, there are several limitations to this study. First, we did not include a placebo group; therefore, the improvement of executive functions might be partially attributed to the placebo effect, learning effect, regression to the mean, or age effect. We had analyzed the age effect and found that the slope of age was smaller compared with treatment (Supplementary Table S4). In addition, the difference between OROS-MPH and atomoxetine could not be explained by the placebo or learning effect. Second, methylphenidate-containing drug is a controlled drug in Taiwan, which prevents us from conducting a double-blinded, randomized clinical trial as an investigator-initiated clinical trial. However, the executive functions were measured objectively and were minimally influenced by the patient's subjective feelings. Third, we did not control for multiple comparisons, which might increase the possibility of type 1 errors. If we use Bonferroni method to adjust multiple comparisons (p-value should be <0.01), the treatment effects of both drugs on executive functions and the comparison for the detectability of the CPT were still statistically significant. However, a larger sample size (276 or more patients each arm, which is estimated based on post hoc analysis) might be needed to detect the group difference in the other domains of executive functions if the difference exists. Fourth, study samples were included from only one medical center in Taipei, and we excluded patients with comorbid psychiatric conditions. Thus, the study results might or might not be generalized to patients with complicated comorbid disease and broader ethnic Chinese populations with ADHD. Finally, the executive functions were assessed at baseline, week 4, and week 12 only. The determination of long-term clinical outcomes warrants further evaluation.
Conclusions
Our findings indicated that treatment with OROS-MPH and atomoxetine was associated with improvements in executive functions with respect to response selection/inhibition, spatial working memory, planning, and flexibility for set-shifting. In addition, we found that OROS-MPH was more effective than atomoxetine in improving sustained attention and inhibition control, which was confirmed by the RVIP and CCPT tasks. These differences implied that the underlying mechanisms of methylphenidate and atomoxetine treating ADHD effects might be different. The clinical implications of our findings, that is, whether the differences in improving executive functions would differentially predict further clinical symptom improvement and long-term clinical and cognitive outcomes, warrant further investigation.
Clinical Significance
This clinical trial demonstrated that treatment with OROS-MPH and atomoxetine was associated with improving executive functions; however, the effects were not the same. OROS-MPH was more effective than atomoxetine in improving sustained attention and inhibition control. The difference in underlying mechanisms and improving executive functions might be applied in personalized therapy.
Footnotes
Disclaimer
The Ministry of Science and Technology and National Health Research Institutes had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the article.
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.