
Abstract
Objectives:
To determine the differences in information between prescribing guidelines and drug labeling, as well as to compare the approval of psychotropic medicines for major depression in pediatric patients (“pediatric depression”) across countries.
Methods:
The recommendations of The Maudsley Prescribing Guidelines in Psychiatry (MPGP) for the treatment of pediatric depression (<18 years) were compared against the regulatory-approved drug-labeling documents from the United Kingdom, Australia, New Zealand, Canada, and the United States. The use of medicines outside of their regulatory approval is defined as off-label use, so differences between the drug labeling and MPGP were characterized according to unapproved age, indication, dosage, or route of administration. Information in the drug labeling was also compared across countries.
Results:
MPGP provides recommendations for 6 medicines for the treatment of pediatric depression, for which, 30 drug labeling were retrieved. Three of 30 drug labeling were consistent with MPGP recommendations (fluoxetine in the United Kingdom, fluoxetine and escitalopram in the United States). Differences in information between MPGP and the drug labeling were identified in 26 of 30 drug labeling analyzed, most often due to age (24/26) followed by indication (2/26). No differences pertaining to dosage or route of administration information were identified. The number of approved psychotropic medicines varied across the studied countries and we found cross-country discrepancies in information in the drug labeling.
Conclusion:
Significant differences in information exists between MPGP and the drug labeling for psychotropic medicines for pediatric depression, due to unapproved ages or indications. Additionally, approval information in the drug labeling are not consistent across countries. Further research into reasons for variability and impact on practice may be warranted.
Introduction
Major depression in pediatric patients (“pediatric depression”) is a serious psychiatric illness, which is often underdiagnosed and undertreated (Charles and Fazeli 2017). Psychotropic medicine use in the pediatric population is widespread, with estimates of pooled global prevalence of antidepressant medicine use reported as 6.4% and antipsychotic medicine use as 5.5% (Piovani et al. 2019). Despite limited regulatory approvals, psychotropic medicines are often used in the treatment of pediatric depression, resulting in off-label use (Dorks et al. 2013; Schroder et al. 2017). Off-label use is commonly referred to as the use of a medicine outside the product license with reference to age, indication, dosage, or route of administration (Pandolfini and Bonati 2005).
The labeling of a medicine is authorized by regulatory authorities, and acts as a main source of information for health professionals. There are few clinical trials focused on psychotropic medicine use in pediatric depression (Murthy et al. 2013) and it is acknowledged that insufficient clinical data often result in a lack of pediatric dosing information in the drug labeling (Permala et al. 2010). Off-label use may be associated with an increase in medication errors (Rinke et al. 2010) and potential increased risk of adverse drug reactions (Horen et al. 2002; Jonville-Béra et al. 2005; McLaren et al. 2018). In practice, dosages for pediatric patients are often scaled from adult dosages despite insufficient methods for scaling (Johnson 2008). Further to this, the growth and developmental changes associated with youth may result in responses to psychotropic medicine treatment, which do not mirror the responses from a fully developed adult brain (McLaren et al. 2018).
Prescribing for off-label use is, however, accepted and may be the standard of care in many cases (Meadows and Hollowell 2007). Thus, prescribers are free to prescribe outside the product licensing, although they assume greater professional responsibility and liability (Sugarman et al. 2013). The General Medical Council's Good Practice guidelines for doctors recommend that prescribers should be aware of the requirements involved, including satisfaction with the current evidence, which exists or sufficient experience with the medicine and belief that it will be safe and effective in the intended patients (Sugarman et al. 2013; General Medical Council 2019).
Prescribers may refer to the drug labeling during practice as they are a source of important clinical trial information, as well as safety and dosage information. The drug labeling may, however, differ across countries, according to the requirements of different regulatory authorities. Additionally, the recommendations of prescribing guidelines are expected to differ from information in the drug labeling, as off-label medicine use in pediatric depression is widespread (Dorks et al. 2013; Palmaro et al. 2015; Deng et al. 2018). These differences could thus result in variations in treatment and prescribing in practice.
Little is known about the differences in information between prescribing guideline recommendations and the drug labeling for the treatment of pediatric depression, or the cross-country differences in approval of psychotropic medicines. Thus, the aims of this study were to determine the differences in information between prescribing guidelines and the drug labeling, as well as to compare the approval of psychotropic medicines for pediatric depression across countries.
Methods
The psychotropic medicines included within this study were defined by the Anatomical Therapeutic Chemical (ATC) classification system (WHO Collaborating Center for Drug Statistics Methodology 2019) and comprised either: Psycholeptics (N05) or Psychoanaleptics (N06).
The approval of medicines in a country is outlined by regulatory-approved drug-labeling documents, which are referred to as the “Summary of Product Characteristics” in the United Kingdom, “Product Information” in Australia, “Data Sheet” in New Zealand, “Product Monograph” in Canada, and “Prescribing Information” in the United States. These documents were sourced from online databases (DataPharm Ltd. 2019; Health Canada 2019; Medsafe 2019; Therapeutic Goods Administration 2019; U.S. National Library of Medicine 2019). There are several online databases containing drug labeling. The online databases used for this analysis are often used by health care professionals as they are easily accessible and provide efficient search methods for a large number of medicines and their drug labeling.
Drug labeling was retrieved for each country in July 2019 (Table 1) and saved locally for data extraction and analysis. The Canadian Product Monograph for imipramine oral tablets could not be retrieved despite a “marketed” status on the website (Health Canada 2019).
A Summary of the Reference Information for the Drug Labeling of Psychotropic Medicines for Pediatric Depression
The Canadian Product Monograph for imipramine oral tablets could not be retrieved from the Health Canada website (Health Canada 2019), despite a “marketed” status. Thus, the approval for pediatric depression in Canada could not be determined and no comparison could be made against the U.S. Prescribing Information.
ATC, Anatomical Therapeutic Chemical; COF, conventional oral formulation; DR, delayed-release oral formulation; IMI, intramuscular injection.
The Maudsley Prescribing Guidelines in Psychiatry (MPGP) (Taylor et al. 2018) were consulted for guidance on the use of psychotropic medicines for pediatric depression. MPGP recommends the following psychotropic medicines for pediatric depression: fluoxetine (first line), sertraline or citalopram (second line), escitalopram (third line) and recommends consideration of augmentation of antidepressant medicines with a second-generation antipsychotic medicine or lithium, or to consider mirtazapine (where sedation is required) (fourth line). No immediate second-generation antipsychotic medicines were listed.
The pediatric age group was defined by those <18 years of age. Many synonyms for the indication “depression” were used across the drug labeling for medicines approved for pediatric depression (Box 1).
Box 1. Variety of Terms Used for “Depression” in the Indications Section of the Drug Labeling Approved for Pediatric Depression
The “Indications” section lists the following: “The treatment of depressive states (in adults only), including endogenous, reactive, neurotic, organic … .” Under the “Dosage and Administration” section, the term “adolescent depression” is used, indicating approval for the pediatric population. See the NZ Data Sheet for additional information.
The “Indications” section lists the following: “It has been found to be effective in depressed patients clinically characterized as ‘atypical,’ ‘nonendogenous,’ ‘neurotic,’ or where treatment with other antidepressants has failed … .” See the U.K. Summary of Product Characteristics for additional information.
The “Indications” section lists the following: “… indicated in the treatment of depressed patients clinically characterized as ‘atypical,’ ‘nonendogenous,’ or ‘neurotic’ … .” See the Canadian Product Monograph for additional information.
COF, conventional oral formulation; DR, delayed-release oral formulation; IMI, intramuscular injection.
To address the aims of this study, two sets of medicine comparisons were made: We performed a cross-comparison document analysis of MPGP medicine recommendations for pediatric depression and their respective drug labeling from five conveniently selected high-income countries (the United Kingdom, Australia, New Zealand, Canada, and the United States) (Fig. 1). Medicines recommended by MPGP were searched in each online database and the drug labeling was retrieved for comparisons. MPGP medicine recommendations, which aligned with the drug labeling, were characterized as “on-label,” whereas those which did not were characterized as “off-label” due to age, indication, dosage, or route of administration. Similar to the article by Palmaro et al. (2015), dosage was compared with a 20% tolerance margin. We performed a cross-comparison document analysis of drug labeling from these five countries (the United Kingdom, Australia, New Zealand, Canada, and the United States) (Fig. 2). All psychotropic medicines comprising ATC groups N05 and N06 were searched in each online database and drug labeling was retrieved for the medicines approved for pediatric depression (unless already retrieved from the above search). Comparisons of all the approval information (for pediatric depression) were made across countries.
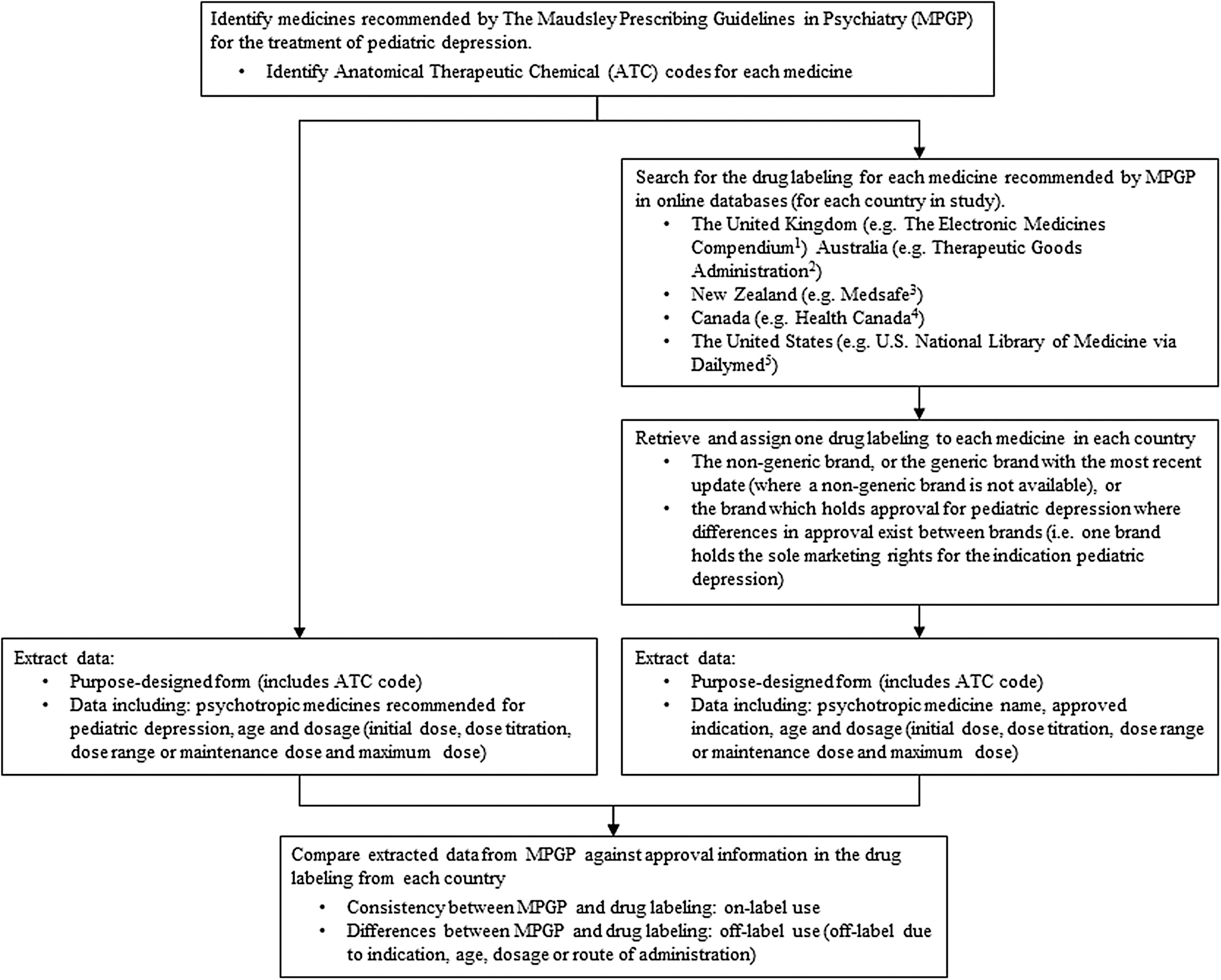
Process of comparing the recommendations of The Maudsley Prescribing Guidelines in Psychiatry against the drug labeling. 1DataPharm Ltd. (2019); 2Therapeutic Goods Administration (2019); 3Medsafe (2019); 4Health Canada (2019); 5U.S. National Library of Medicine (2019).
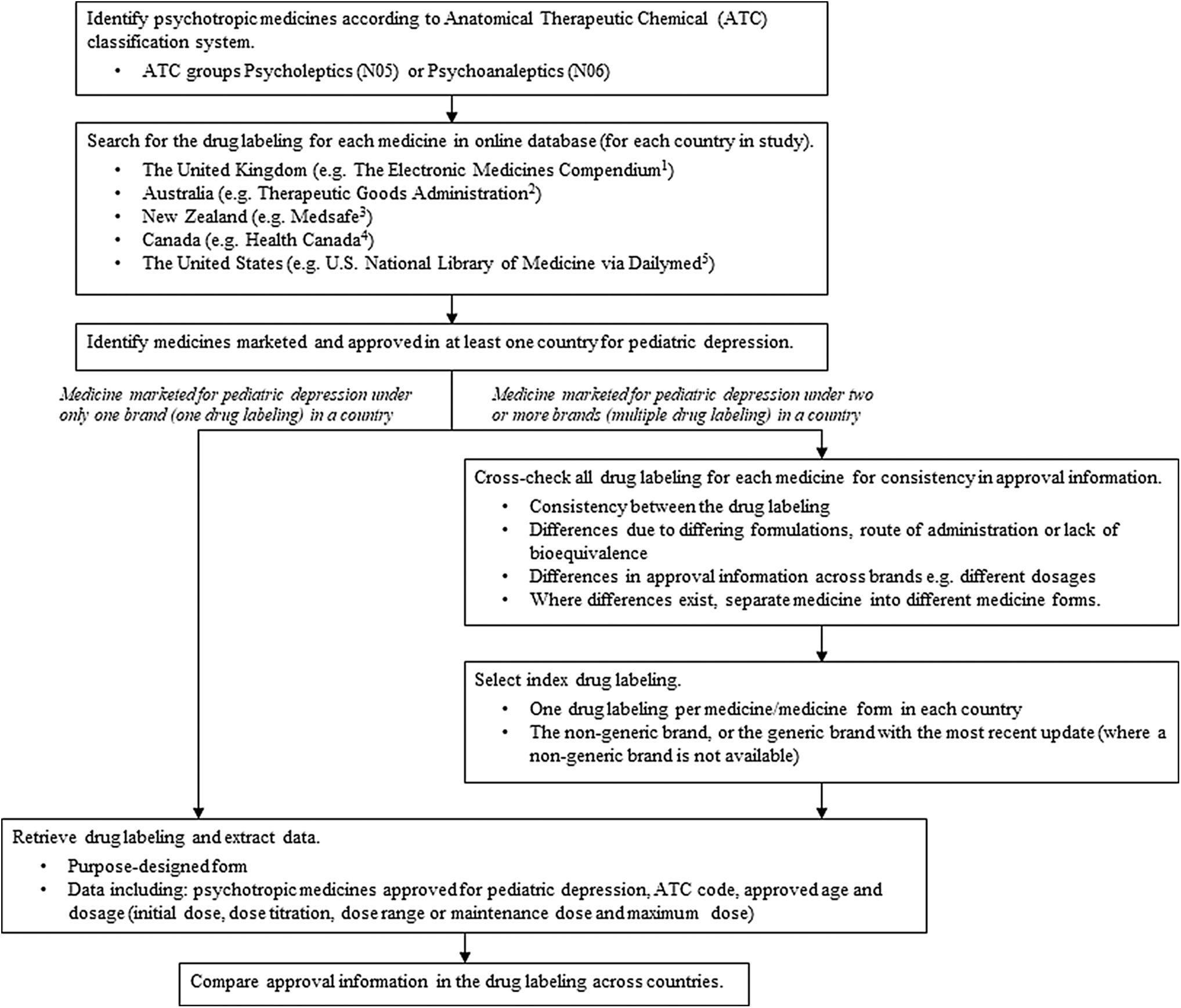
Process of identifying psychotropic medicines and drug labeling for cross-country comparisons of approved information. 1DataPharm Ltd. (2019); 2Therapeutic Goods Administration (2019); 3Medsafe (2019); 4Health Canada (2019); 5U.S. National Library of Medicine (2019).
Where a medicine was marketed or approved in a country under more than one trade name, or more than one formulation, resulting in multiple drug labeling, all documents were cross-checked for consistency. We found consistency across the drug labeling of different brands for the same medicine, except for imipramine and fluoxetine, due to multiple marketed formulations. To be comprehensive, approved medicines with different formulations and routes of administrations, which resulted in different dosage guidelines, were treated as different medicines (i.e., imipramine oral formulation and imipramine intramuscular injection, and fluoxetine conventional oral formulation and fluoxetine delayed-release oral formulation). Thus, only one drug labeling was assigned per medicine per country during data analysis, the nongeneric brand or a generic brand with the most recent update (where a nongeneric brand was not available) (Table 1).
Data extraction and analysis were performed by one author (L.T.), with 10% of the data independently checked by another (A.L.). Where discrepancies existed, a discussion was held until consensus was reached, and adjudicated by a third reviewer (T.F.C.).
Results
Comparison of MPGP against the drug labeling
A total of 30 drug labeling were retrieved for the 6 psychotropic medicines recommended for pediatric depression in MPGP (fluoxetine, sertraline, citalopram, escitalopram, lithium, and mirtazapine). Differences in information between MPGP and the drug labeling were identified in 26/30 drug labeling (off-label use). In most cases, medicines recommended for pediatric depression in MPGP were only approved for adult populations; and 24/30 drug labeling indicated off-label use due to age. Lithium was not approved for depression in any age group in Canada or the United States; thus, 2 of the 30 drug labeling suggested off-label use due to indication. Only fluoxetine (United Kingdom and United States), escitalopram (United States), and lithium (Australia) were approved for pediatric depression (Table 2). Three of the 30 drug labeling indicated on-label use, as fluoxetine (United Kingdom and United States) and escitalopram (United States) drug labeling aligned with the recommendations of MPGP. However, as there were no apparent dosage guidelines for pediatric depression in the lithium drug labeling (Australian Product Information), it is unclear whether the recommendations of MPGP align with the drug labeling (possibly on-label).
Comparison of the Recommendations of Maudsley Prescribing Guidelines in Psychiatry for Pediatric Depression Against the Drug Labeling from Five Countries
On-label: consistency between drug labeling and MPGP.
There are no apparent dosage guidelines for lithium for pediatric depression in the Australian Product Information, so it is unclear whether the recommendations of MPGP align with the Product Information.
Off-label: differences between drug labeling and MPGP with regards to age, indication, dosage, or route of administration.
MPGP, Maudsley Prescribing Guidelines in Psychiatry.
Cross-country comparison of drug labeling
Thirteen medicines from ATC groups N05 and N06 were approved for pediatric depression across the 5 countries (total 22 drug labeling). The number of psychotropic medicines approved for pediatric depression varied across the studied countries and no medicine was consistent in approval across all five countries. The United States had the most medicine approvals (nine), followed by New Zealand (five), the United Kingdom (four), Canada (three), and Australia (one) (Table 3).
Overview of the Approval of Psychotropic Medicines (Comprising Anatomical Therapeutic Chemical Groups N05 and N06) for Pediatric Depression Across Five Countries
The Canadian Product Monograph for imipramine oral tablets could not be retrieved from the Health Canada website (Health Canada 2019), despite a “marketed” status. Thus, the approval for pediatric depression in Canada could not be determined and no comparison could be made against the U.S. Prescribing Information.
ATC, Anatomical Therapeutic Chemical; COF, conventional oral formulation; DR, delayed-release oral formulation; IMI, intramuscular injection.
Approval for imipramine oral tablets for pediatric depression in Canada could not be determined as the Canadian Product Monograph could not be retrieved and no comparison could be made against the U.S. Prescribing Information.
Approved age
Five of the 13 psychotropic medicines were approved for pediatric depression in 2 or more countries (amitriptyline, doxepin, nortriptyline, fluoxetine conventional oral formulation, and phenelzine). The approved age groups in the NZ drug labeling for amitriptyline, doxepin, and nortriptyline (adolescents 13–18 years only under the supervision of a specialist) differed from the other approved countries. In contrast, amitriptyline (Canada and the United States) and doxepin (United Kingdom and United States) were approved in adolescents ≥12 years of age, whereas nortriptyline (United Kingdom, Canada, and the United States) was approved in “adolescents” (with no specified age range). Fluoxetine conventional oral formulation was approved in both the United Kingdom and the United States for children and adolescents ≥8 years of age, and phenelzine was approved in both the United Kingdom and Canada for adolescents ≥16 years of age (Tables 4–7).
Nonselective Monoamine Reuptake Inhibitors: Comparison of the Approval Information in the Drug Labeling for Pediatric Depression Across Five Countries
Not approved for depression in adolescents 13–18 years of age unless under the supervision of a specialist. Contraindicated for depression in patients 12 years of age and under; see New Zealand Data Sheet.
Although general dosages have been included, they are not specifically mapped to the pediatric population and thus it is unclear if they apply to the pediatric OR adult population, OR both.
The Canadian Product Monograph for amitriptyline states that for adolescents, “… Lower dosages are recommended … In those patients who may not tolerate higher doses, 50 mg daily may be satisfactory …”
The U.S. Prescribing Information for amitriptyline states that for adolescents, “… Lower dosages are recommended …10 mg three times a day with 20 mg at bedtime may be satisfactory in adolescents … who do not tolerate higher dosages.”
The Canadian Product Monograph for imipramine oral tablets could not be retrieved from the Health Canada website (Health Canada 2019), despite a “marketed” status. Thus, the approval for pediatric depression in Canada could not be determined and no comparison could be made against the U.S. Prescribing Information.
ATC, Anatomical Therapeutic Chemical; COF, conventional oral formulation; IMI, intramuscular injection.
Selective Serotonin Reuptake Inhibitors: Comparison of the Approval Information in the Drug Labeling for Pediatric Depression Across Five Countries
Although general dosages have been included, they are not specifically mapped to the pediatric population and thus it is unclear if they apply to the pediatric OR adult population, OR both.
ATC, Anatomical Therapeutic Chemical; COF, conventional oral formulation; DR, delayed-release oral formulation.
Monoamine Oxidase Inhibitors: Comparison of the Approval Information in the Drug Labeling for Pediatric Depression Across Five Countries
Although general dosages have been included, they are not specifically mapped to the pediatric population and thus it is unclear if they apply to the pediatric OR adult population, OR both.
ATC, Anatomical Therapeutic Chemical; COF, conventional oral formulation.
Lithium: Comparison of the Approval Information in the Drug Labeling for Pediatric Depression Across Five Countries
ATC, Anatomical Therapeutic Chemical; COF, conventional oral formulation.
Approved dosage
Only 2 of the 22 drug labeling contained information on all aspects of dosage: initial dose and dose titration, dose range or maintenance dose, and maximum dose (clomipramine in New Zealand and escitalopram in the United States). Three of 22 drug labeling did not contain any information on dosage for the pediatric population (dosulepin in New Zealand, phenelzine in the United Kingdom and lithium in Australia). Of all the dosage aspects, the maximum dose was most often not provided, and was absent in 20 of the 22 drug labeling.
For the five psychotropic medicines approved for pediatric depression in two or more countries (amitriptyline, doxepin, nortriptyline, fluoxetine conventional oral formulation, and phenelzine), there were some differences in the drug-labeling dosage information across countries. Differences were noted for amitriptyline, doxepin, nortriptyline, and fluoxetine conventional oral formulation (Tables 4–7). Cross-country dosage comparisons could not be made for phenelzine (between the United Kingdom and Canada) as no dosage guidelines were provided for pediatric depression in the U.K. Summary of Product Characteristics.
Discussion
This study is the first to compare information from the drug labeling of psychotropic medicines for use in pediatric depression against a recognized psychotropic prescribing guideline. Health care professionals looking for guidance on the use of psychotropic medicines for pediatric depression will encounter discrepancies when key resources are searched. A total of 13 psychotropic medicines were approved in one or more of the studied countries, however, only 3 of these medicines were recommended by MPGP (fluoxetine, escitalopram, and lithium). Specifically, the eight tricyclic antidepressant medicines (TCAs), which hold approval for pediatric depression in one or more of the studied countries, are not recommended for use in pediatric depression in MPGP. This recommendation is supported by a Cochrane review, which found that TCAs are not useful in treating major depression in children, and there is marginal evidence to support their use in the treatment of major depression in adolescents (Hazell and Mirzaie 2013).
MPGP recommends the consideration of augmentation of antidepressant medicines with a second-generation antipsychotic medicine (fourth-line pharmacotherapy), although the recommended second-generation antipsychotic medicines are not immediately listed, and no second-generation antipsychotic medicines are approved for pediatric depression in any of the studied countries. There is increasing evidence supporting the benefits of second-generation antipsychotic medicines for treatment-resistant major depression in adults, either as monotherapy or augmentation to antidepressant medicines. In particular, aripiprazole, brexpiprazole, olanzapine (in combination with fluoxetine) and quetiapine (extended-release) are approved in the United States for augmentation of antidepressant medicines in adults and some evidence also supports the benefits of other, unapproved, second-generation antipsychotic medicines (Han et al. 2013; Wang et al. 2016). A lack of studies in the pediatric population warrants the need for clinical trial data evaluating lithium or augmentation of antidepressant medicines with a second-generation antipsychotic medicine for pediatric depression (Han et al. 2013).
Our study found that differences in information between MPGP and the drug labeling was most often due to the recommendation of medicines outside of the approved age (24/26), followed by indication (2/26). Similarly, studies by Schroder et al. (2017) and Deng et al. (2018) comparing pediatric outpatient antidepressant medicine prescriptions against regulatory approvals found unapproved ages or indications to be the most common types of off-label use. It is important to note that both studies were not restricted to use of antidepressant medicines in pediatric depression alone, but rather extended to use in other psychiatric conditions in pediatric patients.
Fluoxetine has been found to be the leading prescribed antidepressant medicine for pediatric depression in the United Kingdom, whereas sertraline was the leading prescribed antidepressant medicine in the United States (Bachmann et al. 2016). Interestingly, fluoxetine is recommended as first-line treatment in pediatric depression by MPGP and is approved in both the United Kingdom and the United States for pediatric depression, whereas sertraline is also recommended by MPGP (second-line pharmacotherapy), but is not approved for use in pediatric depression in any of the studied countries. Other studies have also shown sertraline to be most commonly prescribed (in adolescents) in France, China, and Croatia (Marsanic et al. 2012; Deng et al. 2018; Revet et al. 2018) or second most commonly prescribed (in children and adolescents) in multiple Asian countries (Chee et al. 2016).
Despite a recent systematic review by Ignaszewski and Waslick (2018) supporting the safe use of antidepressant medicines in pediatric depression, concerns associated with clinical trial designs could limit their ability to reflect real-world responses. According to Dubicka and Brent (2017), most suicide-prone individuals treated with antidepressant medicines would not be included in clinical trials, so the real public health impact of antidepressant medicine treatment may be underestimated. Furthermore, when using psychotropic medicines off-label due to age, it is worth noting that the growth and developmental changes associated with youth may result in responses to treatment, which do not mirror the responses from a fully developed adult brain (McLaren et al. 2018). Off-label use of medicines could also expose patients to unknown side effects or safety concerns if their characteristics differ to those of the patients included in clinical trial studies (Wittich et al. 2012; Eguale et al. 2016; McLaren et al. 2018).
Many differences in regulatory approved information were identified in terms of indication, age specifications, and dosage instructions across the five countries. Despite the same available evidence and applications from a single pharmaceutical company, different regulatory processes across countries result in different regulatory decisions and outcomes. For example, Prozac® (fluoxetine) is marketed by Eli Lilly and Company in the United Kingdom, Australia, New Zealand, and Canada, and is manufactured by Eli Lilly and Company in the United States (labeled by Dista Products Company) (Table 1), but is only approved for pediatric depression in the United Kingdom and United States, and some differences in the approved dosage information exist between the two drug labeling. Obtaining new regulatory approvals for medicines may be costly and time consuming for pharmaceutical companies (Wittich et al. 2012) and regulatory processes may differ across countries, which could explain why cross-country differences in approval exist. However, further research is required to explore these reasons.
Consistent with other studies (San Miguel et al. 2005; Beers et al. 2013; Salgado et al. 2013; Arguello et al. 2014; Weersink et al. 2019) we also found deficiencies in many drug labeling, especially in relation to missing or ambiguous approval information. For example, the approval of clomipramine for pediatric depression in New Zealand is ambiguous and the general dosage guidelines provided are not specifically mapped to a particular age group, raising questions about whether these dosages are applicable to pediatric patients. This was also the case for other drug labeling. Additionally, pediatric depression dosage information was often not provided, raising concerns about the completeness of the included information. Such deficiencies in the approval information leave the decision making up to the health care professional and may potentially contribute to variations in dosing and prescribing habits in practice. Our findings identify an opportunity to update and improve the clarity of drug labeling, and this may be useful for pharmaceutical companies who are undergoing the revision of drug labeling, particularly for psychotropic medicines for use in pediatric depression. It is worth noting that some drug labeling provided a clear and complete summary of the approval information necessary for the analysis of this study. An example is the U.S. Prescribing Information for escitalopram.
The findings of this study relating to the international comparisons of drug labeling may facilitate the decisions of regulatory bodies, such as the U.S. Food and Drug Administration, Therapeutic Goods Administration (Australia), the U.K. Medicines and Healthcare Products Regulatory Agency, and others, to aid the global harmonization of these documents. Changes have been implemented in recent years by regulatory agencies across different countries, including Australia and New Zealand, to improve the format of drug labeling and to harmonize with international regulators (New Zealand Medicines and Medical Devices Safety Authority 2017; Therapeutic Goods Administration 2020). Our findings show further areas for consideration during the update of drug labeling. Additionally, the concept of our study is in line with the mission of The International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH), for greater harmonization of regulatory processes, worldwide (The International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use 2020).
This study has some limitations. This study examined the approval of psychotropic medicines from five countries and findings may not be generalizable to other countries. Additionally, the ambiguity and deficiencies in information in the drug labeling may have impacted on the reporting of results. We acknowledge that only one researcher extracted all of the data. To provide robustness, 10% of the data set was randomly and independently checked by a second author. No significant discrepancies between the two authors were noted. Furthermore, it is recognized that only one prescribing guideline was used during this analysis, however, MPGP is internationally recognized and provides relevance and significance to this study from the perspective of all the countries included.
Future studies examining information from other prescribing guidelines and drug labeling extending to other countries could provide a wider understanding of the differences between the two resources and could positively influence progression toward global harmonization of the regulatory approval of medicines. Additionally, a further analysis into other sections of the drug labeling may also add to the findings of this study and help to strengthen the quality of these regulatory documents. It is acknowledged that the drug labeling change over time, necessitating an update to these findings in the future. Alongside the findings of this study and the limited research available regarding the off-label use of psychotropic medicines in pediatric depression, there is a need for further investigation into reasons for variability in information in the drug labeling across countries, and the implications of off-label use in practice.
Conclusions
In summary, there are significant differences in information between the recommendations of MPGP and the approved drug labeling for psychotropic medicines for use in pediatric depression, most often due to unapproved age or indication parameters. Additionally, the cross-country discrepancies in approval information, and deficiencies in information in the drug labeling identified during our study support the need for the update and global harmonization of these documents. Further research into the reasons for variability between drug labeling across countries, as well as the impact of off-label use in practice may be needed.
Clinical Significance
Drug labeling and prescribing guidelines provide guidance on the use of psychotropic medicines from regulatory and clinical practice perspectives, respectively. The off-label use of psychotropic medicines in pediatric depression is widespread, despite limited research, and research into the impact of off-label use in practice is needed. Drug labeling has been shown to lack in important medicine information, and our findings indicate that this extends to psychotropic medicines for use in pediatric depression. Cross-country discrepancies in the drug labeling and ambiguity and deficiencies in the included information necessitate the update and global harmonization of these documents.
Footnotes
Disclosures
No competing financial interests exist.