
Abstract

Stimulant use is less utilized in individuals with attention-deficit/hyperactivity disorder (ADHD) with parents from Africa, Asia, the Middle East, or South America (non-Western origins, NWO) compared with Europe, North America, and Oceania (Western origins, WO) (Ghosh et al. 2014). This discrepancy may be due to cross-cultural differences; however, limited studies have explored this topic. We conducted a meta-analysis to delineate the differences in the prevalence of stimulant use for ADHD between NWO and WO.
A systematic search was conducted following the PRISMA guidelines (Fig. 1) and registered in PROSPERO (CRD42020202481). All studies included in the meta-analysis were selected by searching the PubMed database through February 2021, using the search strings “ADHD” or “attention deficit hyperactivity disorder” and “immigrants” or “country of birth” and “stimulants” or “treatment” or “treatment lag.” Studies included in our analysis were required to meet the following criteria: (1) used original data and published in peer-reviewed journals as a primary, cohort, crossover, or observational study; (2) included only human participants who were <25 years; (3) used stimulant medication only for ADHD; (4) published in English; and (5) reported sufficient data to calculate either odds ratio (OR) or prevalence, confidence interval (CI), and p-value. Randomized pooled prevalence estimates and ORs were performed using the Comprehensive Meta-Analysis software version 3.0, with 95% CIs.
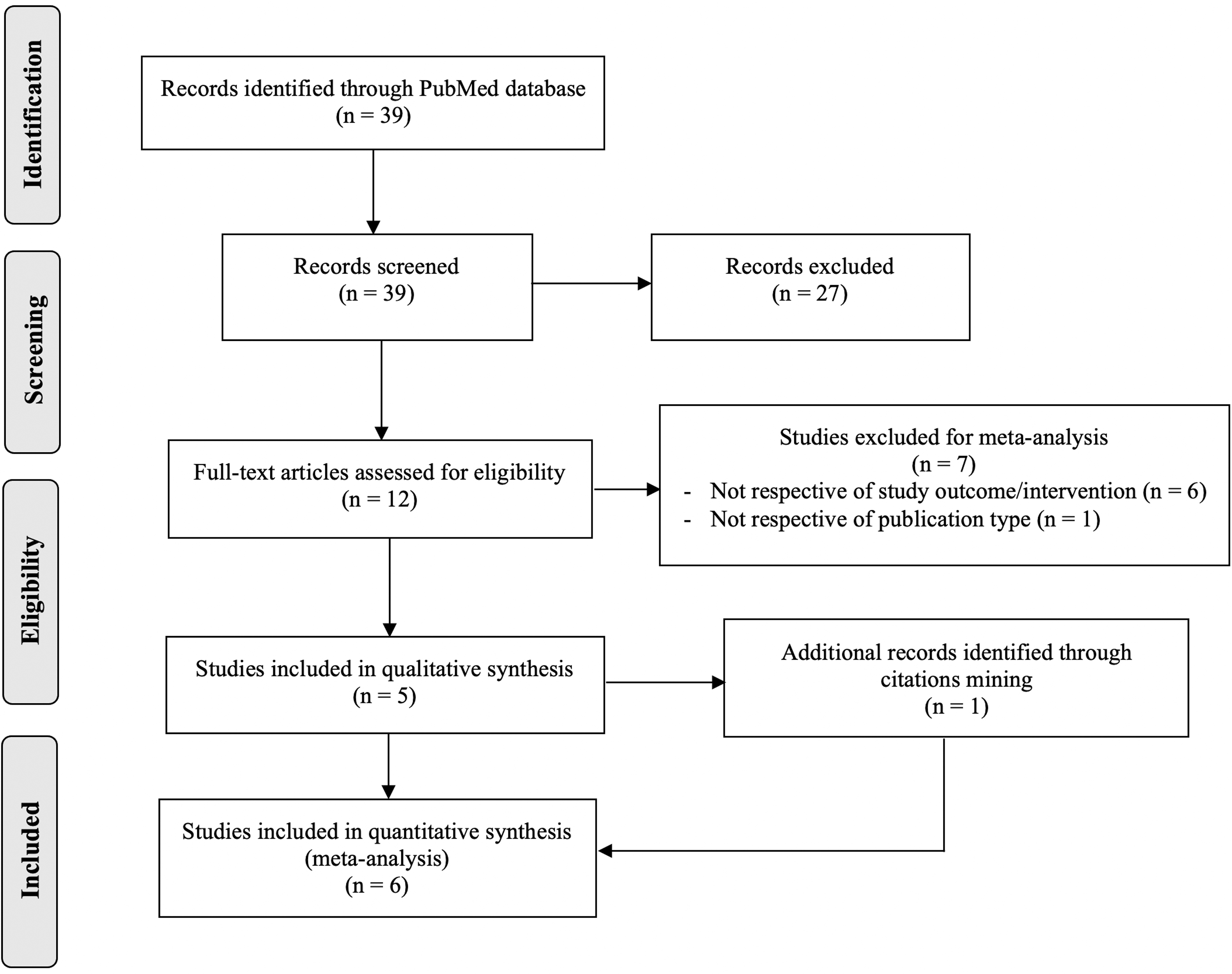
PRISMA flowchart.
In total, 39 articles were identified, and 12 full-text articles were received, of which 6 studies were included (n = 3,034,450 participants: n boys = 1,549,985; n girls = 1,4713,318). Specifically, the number of participants using a stimulant for ADHD was n = 70,516 (n boys = 52,111; n girls = 19,108). Stimulants were classified as amphetamine, dexamphetamine, methamphetamine, and methylphenidate. A few studies defined pemoline, fencamfamin, modafinil, fenozolone, and atomoxetine as stimulants.
The pooled prevalence of stimulant use for ADHD among (1) those of NWO was 10.7% (95% CI: 5.0–21.4; p < 0.05), and among (2) those of WO, it was 86.1% (95% CI: 76.4–92.1; p < 0.05) (Zuvekas and Vitiello 2012; Knopf et al. 2012; Ghosh et al. 2014; Ghosh et al. 2017; Arat et al. 2018; Jablonska et al. 2020) (Fig. 2). Significant heterogeneity was found (I 2 = 99.99). The odds of using stimulants for ADHD decreased by 50% if individuals were of NWO and increased by 82% if individuals were of WO (OR = 0.55, 95% CI: 0.369–0.817, p = 0.003 and OR = 1.82, 95% CI: 1.23–2.71, p = 0.003, respectively) (Zuvekas and Vitiello 2012; Ghosh et al. 2014; Ghosh et al. 2017; Arat et al. 2018).
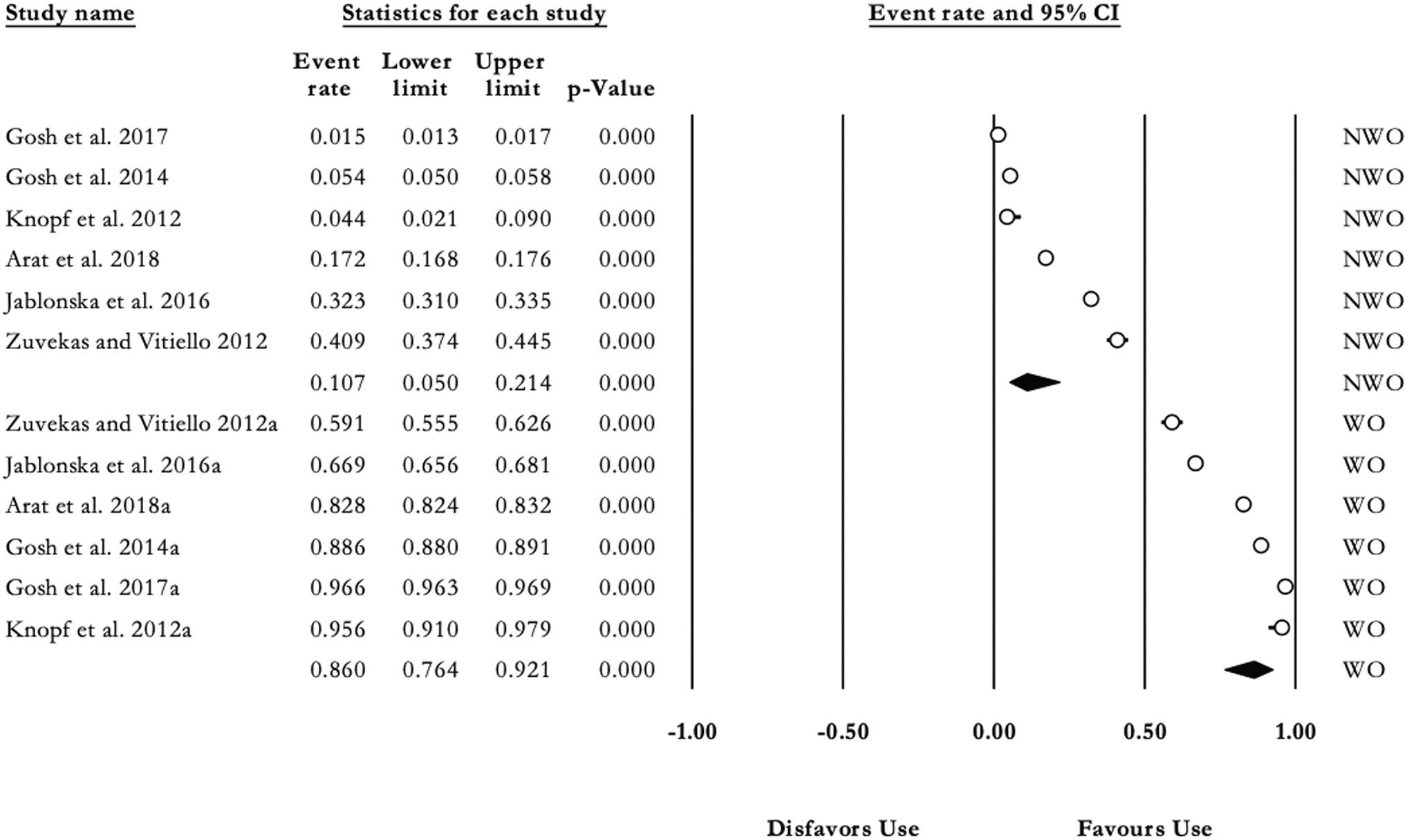
Prevalence of stimulant usage in NWO and WO (n = 70,516). Event rate, prevalence estimate; NWO, non-Western origin; WO, Western origin.
Limitations to this meta-analysis include the substantial amount of heterogeneity of 99%. This considerable heterogeneity indicates a significant variation of outcomes between the included studies, which could have been to several factors such as characteristics of the population, sample size, diagnostic criteria, or the small number of included studies (n = 6). The sources of heterogeneity were not explored due to limited information. Although substantial heterogeneity reduces the reliability of results, our study provides findings that can guide research, clinicians, and raise awareness about low stimulant use among NWO with ADHD. Future researchers investigating this topic are suggested to perform subgroup analysis using moderators such as age, gender, age of diagnosis, and parental level of education/socioeconomic status, to identify the rationale of reduced stimulant use among ADHD individuals of NWO.
Footnotes
Disclosures
The authors of this article, Nikhila Veluri and Rikinkumar Patel, certify that they do not have any affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs in the subject matter or materials discussed in this article during the course of its preparation or submission.