
Abstract
Objective:
Prescription of multiple medications concurrently for children and adolescents has increased in recent years. Examination of this practice has been undervalued relative to its incidence. This article reviews studies investigating effectiveness of medication combinations for youth with attention-deficit/hyperactivity disorder (ADHD).
Methods:
A literature search identified studies that combined two or more prescribed medications for the treatment of ADHD. Included studies focused on youth; had study design of randomized controlled trial (RCT), nonrandomized trial, or case review (n > 10); and included an outcome measure of treatment effectiveness.
Results:
Thirty-nine pertinent studies were identified. All studies combined two medications, with the vast majority including a stimulant (n = 37). The largest group (n = 16) combined stimulant and alpha-agonist, finding greater efficacy than alpha-agonist alone but not stimulant alone in all cases. A few RCTs found benefit from the addition of risperidone or divalproex to stimulant for comorbid aggression. Four studies adding atomoxetine found mixed reports of benefit, including the only small RCT showing no benefit. RCTs with selective serotonin reuptake inhibitors found minimal evidence of benefit for mood or anxiety comorbidities.
Conclusion:
The best studied combination is stimulant and alpha-agonist; addition of alpha-agonist to stimulant seems effective for residual symptoms of ADHD. Stimulant plus risperidone has the most evidence of efficacy for comorbid aggression or disruptive behavior. Limited support exists for the effectiveness of other medication combinations, including no trials studying three or more medications concurrently. Combinations frequently yielded more side effects, leaving monotherapy preferable if a sufficient treatment response can be achieved.
Introduction
Combined pharmacotherapy can be the optimal therapeutic intervention in some youth, including situations with residual symptoms on monotherapy, presence of comorbid conditions, potential synergistic effects from targeting different symptom clusters or mechanisms of action, or prophylaxis for or management of adverse effects (Wilens et al. 1995). The rate of psychotropic polypharmacy (defined as the simultaneous use of two or more psychotropic medications) has increased in recent years among the general pediatric population. Polypharmacy among visits where a psychotropic medication was prescribed increased from 14.3% to 20.2% over a 12-year period ending in 2007 (Comer et al. 2010). Among medication classes, second-generation antipsychotic (SGA) use increased by 22% between 2004 and 2008, with 85% of prescriptions concurrent with other medications (Kreider et al. 2014). Youth diagnosed with attention-deficit/hyperactivity disorder (ADHD) with no other stated comorbid diagnosis experienced a 14.6% increase in concurrent SGA use between 2004 and 2008, and those with comorbid diagnosis similarly showed 8.8% increase, totaling 10% of the subsample in 2008. ADHD and antipsychotic medications are among the most commonly co-prescribed medications, specifically methylphenidate (MPH) and risperidone (28.3% and 20.1%, respectively, of multiclass visits; Comer et al. 2010).
Aggressive behavior frequently coexists with childhood psychiatric disorders including ADHD and can be the target of polypharmacy prescribing (Jensen 2014). Existing guidelines address the topic of polypharmacy in management of ADHD including when comorbidities are present (Pappadopulos et al. 2003; Pliszka et al. 2006). These guidelines provide a clinical framework for pharmacologic treatment approaches but stop short of summarizing evidence regarding efficacy for specific medication combinations.
Empirical evidence is needed to ensure that appropriate prescribing practices are used to achieve the safest and best outcomes (Lohr et al. 2018), and prescribers must carefully weigh the risk benefit for each youth and each medication combination (Woolston 1999). There are several reasons to be cautious. Polypharmacy is associated with a higher incidence of adverse effects, risk of drug interactions, and poorer patient adherence (Kingsbury et al. 2001; Hilt et al. 2014; Bogler et al. 2019). Children have immature and developing organ systems that may increase vulnerability to some long-term side effects (Wilens 2009; Safer 2011). Finally, duration of medication effectiveness studies is often several weeks, and may not detect side effects of combination (COMB) treatment used for longer durations.
Two previous reviews surveyed psychotropic polypharmacy in children and adolescents; both included ADHD although neither focused solely on this diagnosis. In a search ending in 2001, Safer et al. (2003) identified 33 articles, including only six randomized controlled trials (RCTs); authors concluded that the evidence for the effectiveness of polypharmacy in youth was weak. Jureidini et al. (2013) updated this search (and expanded inclusion to supplements) identifying 37 articles that were not included in the previous review. Of 18 RCTs, only 2 showed significant effect size (ES) benefits, both for adding a second psychotropic to a stimulant in the treatment of ADHD.
Investigation of psychotropic combinations has been undervalued relative to the frequency of this practice in the community (Brown et al. 2008; Wilens 2009). Most research in youth focuses on monotherapy (Olfson 2014; Baker et al. 2017), which raises concern because polypharmacy is increasingly the norm in clinical practice (Brown et al. 2008). The objective of this review was to provide an updated, thorough examination of the research evidence of efficacy for combining two or more psychotropic medications for the treatment of youth with ADHD.
Methodology
The literature search was registered in the United Kingdom's National Institute for Health Research PROSPERO system (CRD42018082139). The initial search was designed to identify studies of polypharmacy in youth for all behavioral health indications, with the final step focusing on ADHD for this review.
Search strategy
MEDLINE, MEDLINE EPub Ahead of Print and In-Process & Other Non-Indexed Citations, PsycINFO, EMBASE, and Cochrane Database of Systematic Reviews were all queried over the period from 1987 to 2019. The polypharmacy dataset was augmented by identifying all articles with title or author keywords starting with the terms adjunct- or coadminst- or polypharm-, then adding in all articles with titles with a combination of terms of add- or combin- or concomitant- or concurrent PLUS a term of admin- or manag- or pharmacother- or ther- or treat-. This widely inclusive dataset was then limited to: articles in which at least one prescription psychiatric medication was mentioned in the title or keyword, studies specifically including children or adolescents, English language, and study types that could be of a controlled trial nature (excluding case reports). The search identified 2352 citations, with another 57 identified through review of references or authors' knowledge of relevant citations (in one case unpublished data on clinicaltrials.gov).
There were four inclusionary criteria. First, the research focus had to be a mental health disorder (Diagnostic and Statistical Manual of Mental Disorders [DSM] diagnosis) or a behavioral health indication. Second, the research combined two or more prescribed psychotropic medications, not including supplements. Third, the study population included or focused on children or adolescents (age <18 years). Fourth, the research design needed to: (1) be an RCT, nonrandomized trial, or retrospective chart review (RCR) of 10 or more subjects; (2) have a control group for comparison (pre- and postintervention acceptable for open label or chart review); (3) have an outcome measure related to treatment effectiveness (even if not the primary outcome); and (4) not focus solely side effects. Although safety data are likewise important, authors chose to focus on efficacy owing to the large number of studies to synthesize.
Screening process
To establish consistency in the application of the inclusion criteria, all five authors independently reviewed three randomly selected article sets, and then discussed differences in opinion for articles where there was no perfect agreement. Upon completion of these iterative reviews, we attained a 93% unanimous agreement rate. The articles were randomly divided into five roughly equal sets, with each set reviewed by one of the authors. Information from the article titles and abstracts were used in the screening review.
The screening process eliminated 1746 articles that did not meet inclusionary criteria (reasons shown in Fig. 1). The 262 articles identified for full-text screening were randomly distributed between the five authors. Reviewers used the same set of screening criteria to determine final inclusion or exclusion status. After the full-text review, 87 studies were identified as meeting all inclusionary criteria, with the focus of this review being the subset of 39 articles about treatment of ADHD.
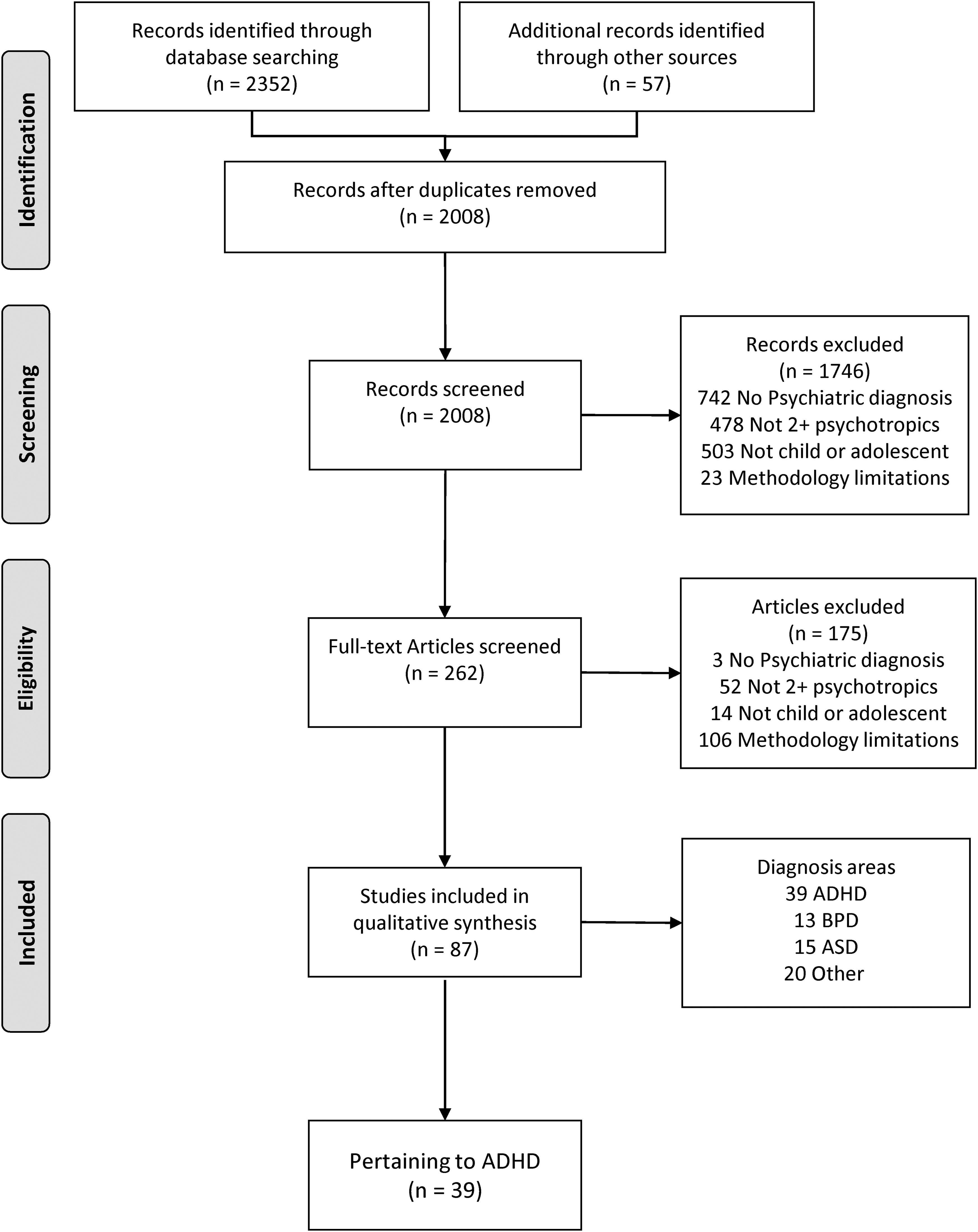
Flow diagram for article selection. From Moher et al. (2009). The PRISMA Group.
Results
The literature examining the use of polypharmacy in youth with ADHD included one meta-analysis, 17 RCTs (many with multiple publications), 10 nonrandomized trials, 3 RCRs, and one cost-effectiveness analysis. No studies systematically reviewed combinations of three or more medications. Nearly all trials (n = 37) included a stimulant as one of the two study medications. The most frequently studied addition to stimulants was alpha-agonist (clonidine [CLON] or guanfacine, n = 16) followed by risperidone and atomoxetine.
Stimulant and alpha-agonist (summarized in Table 1)
Stimulant and Alpha-Agonist (N = 16)
“Bold”—if a priori identified as primary.
Indicates RCT was included in Hirota meta-analysis.
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale-IV; ASQ, Connors Abbreviated Symptom Questionnaire; CD, conduct disorder; C-GAS, Clinician Ratings of Global Functioning; CGI, Clinical Global Impression (Severity/Improvement); CGI-P, Conners Global Index—Parent; COMB, combination treatment; CPRS, Conners Parent Rating Scale Revised; ES, effect size; MPH, methylphenidate; NR, not reported; ODD, oppositional defiant disorder; PGA, Parent Global Assessment; RCT, randomized controlled trial; QALY, quality adjusted life years; SMD, standard mean difference.
Meta-analysis and RCTs
Hirota et al. (2014) completed a meta-analysis of three RCTs combining stimulant and alpha-agonist for treatment of ADHD including 726 youth ages 6–17 (mean 10.4). In the smallest study youth had a comorbid externalizing disorder (Hazell and Stuart 2003). Study design for each RCT was continuation of stable dose of stimulant followed by addition of an alpha-agonist or placebo (PBO) for residual symptoms. No non-medication comparator group was used. The two larger studies showed superior effectiveness of combined treatment for symptoms of ADHD (Kollins et al. 2011; Wilens et al. 2012); the smallest showed no difference (Hazell and Stuart 2003). Standard mean differences of adjunctive alpha-agonist (−0.39) were smaller than alpha-agonist monotherapy (−0.59). COMB treatment was associated with more side effects (number needed to harm = 10), including somnolence, hypotension, and bradycardia. Discontinuation rates were similar to PBO.
The smallest of the three studies in the meta-analysis, Hazell and Stuart (2003) reported on 67 youth (COMB n = 38, stimulant n = 29) ages 6–14 with comorbid oppositional defiant disorder (ODD) or conduct disorder (CD). Youth were continued on stable stimulant dose and randomized to added CLON or PBO. Significantly greater improvements with COMB were found for conduct problems (primary outcome), but not hyperactivity.
Kollins et al. (2011) conducted a relatively large phase 3, double-blind, randomized controlled trial of youth age 6–17 with ADHD (n = 198). Those who had an inadequate response to their stable stimulant regimen were randomized to receive adjunctive CLON-XR (n = 102) or PBO (n = 96). Primary endpoint of ADHD-Rating Scale-IV (ADHD-RS) total score was four points better for COMB than stimulant monotherapy and had significantly greater improvement in both inattentive and hyperactive subscales. The overall ES for COMB versus stimulant monotherapy was 0.34.
In the largest RCT, Wilens et al. (2012) randomized 461 youth with persistent symptoms on a stable stimulant regimen to receive guanfacine-XR (GXR; n = 303) or PBO (n = 153). At study endpoint week 9, ADHD-RS decreased more for those treated with COMB (20.1 with morning dosing; 20.9 with evening dosing), compared with 15.6 for PBO, giving an estimated ES of 0.38 and 0.45, respectively. COMB was associated with mean decrease in pulse and blood pressure; no serious adverse events were deemed related to trial medication.
Secondary analyses of these data found higher response and remission rates for COMB based on a variety of definitions (Cutler et al. 2014); including remission (defined as ADHD-RS score ≤18) more frequently observed in youth on guanfacine (a.m. 61.1%, p.m. 62.2%) than PBO (46.1%). This PBO remission rate is notable, specifically that nearly half of youth continued on stimulant plus PBO achieved remission, considering that the population had been defined by persistent symptoms on stimulant monotherapy. This high response rate led authors to postulate that nonadherence may be confounding results, and increased adherence associated with research study enrollment could have contributed to observed improvement.
Analysis of study data further identified greater improvement in oppositional symptoms as rated on Conners Parent Rating Scale—Revised, with estimated ES of 0.36–0.39 (Findling et al. 2014), and better morning and evening functioning (Wilens et al. 2017). The final publication was a cost-effectiveness analysis, which estimated that the cost of GXR use was $892 per year with corresponding quality-adjusted life-years (QALY) increase of 0.03, leading to the conclusion that adding GXR in youth with suboptimal stimulant response had a cost-effectiveness ratio threshold of $50,000/QALY, summarized as a “good value” (Sikirica et al. 2012).
The three RCTs mentioned previously, all included in the Hirota meta-analysis, represent a similar study design that required residual symptoms despite stimulant treatment. One limitation relates to the naturalistic use of stimulant at enrollment, without systematic dose optimization or measuring the impact of monotherapy before initiation of alpha-agonist. Two RCTs examine this same combination with a substantially different design: youth were randomized to several weeks of alpha-agonist or PBO, followed by addition of stimulant or PBO. These studies did not require residual symptoms on stimulant or any history of suboptimal response to medication, consistent with a test of drug synergism assessing superiority of combination from the start of treatment. Design included comparison of combination to monotherapy with either stimulant or alpha-agonist, and the smaller study included a true placebo control group.
The larger study was an 8-week trial of 207 youth given guanfacine (n = 68),
The smaller (n = 122) study looked at CLON (n = 31), MPH (n = 29), COMB (n = 32) or PBO (n = 30), including youth with prior exposure to either drug stopped before study enrollment (Palumbo et al. 2008). Youth were given CLON or PBO for 4 weeks, followed by MPH or PBO for 4 weeks, then continued for 8 weeks. At 16 weeks, COMB was better than CLON but not MPH alone for teacher-rated ADHD symptoms. The study had high attrition especially in the PBO group. A secondary analysis of quality-of-life measures found all active treatment groups improved over time, whereas comparisons between either monotherapy or COMB treatment were not statistically significant (Cannon et al. 2009).
Three RCTs examined ADHD and a comorbid condition. As reported previously, in a small RCT, Hazell and Stuart (2003) found stimulant and CLON treatment superior for conduct problems (primary outcome). For youth with comorbid tic disorders, MPH and CLON combined led to superior improvement of ADHD symptoms than either alone, with all groups having improved tics compared with PBO (Kurlan et al. 2002). In a pilot study of aggression without a primary outcome measure, Connor et al. (2000) randomized 24 youth to MPH (n = 8), CLON (n = 8), or COMB (n = 8). Authors ran a large number of associations on parent- and teacher-rated symptoms and functioning relating to ADHD, disruptive behavior, and cognitive performance, and found no difference between groups on most measures.
Non-RCT
Two open-label studies had a primary outcome of safety and secondary efficacy measures. The first continued youth (n = 75) with ADHD symptoms on their stable dose of MPH or amphetamine and added guanfacine (Spencer et al. 2009). Primary outcome of the study was to assess safety; mild to moderate adverse effects were common with the addition of guanfacine (77%), particularly somnolence, sedation, and fatigue (56%). Secondary measures observed a 56% reduction in baseline ADHD-RS scores. A longer -term study of guanfacine (n = 206) combined the above data with another open-label study of guanfacine alone (Sallee et al. 2009). Efficacy measures found improvements in ADHD-RS for all subjects, numerically greater for COMB (n = 53), although a direct comparison was not made between groups. Only 60 (23%) total subjects completed the 2-year follow-up, although authors noted low discontinuation owing to either treatment emergent adverse effects (12%) or lack of efficacy (10%).
Stimulant and antipsychotic or mood stabilizer for comorbid disruptive behavior (summarized in Table 2)
Stimulant and Antipsychotic or Mood Stabilizer for Comorbid Disruptive Behavior (N = 15)
“Bold”—if a priori identified as primary.
ABS, Antisocial Behavior Scale; ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale-IV; BYI, Beck Youth Inventory; CASI-4R, Child and Adolescent Symptom Inventory-4R; CAS-P, Children's Aggression Scale-Parent; CAS-T, Children's Aggression Scale-Teacher; CBCL, Child Behavior Checklist; CD, conduct disorder; CGI, Clinical Global Impression (Severity/Improvement); CGI-P, Conners Global Index—Parent; COMB, combination treatment; CPT, Conners Continuous Performance Test; CPRS, Conners Parent Rating Scale Revised; DBD, disruptive behavior disorder; DMDD, disruptive mood dysregulation disorder; ES, effect size; GAF, Global Assessment of Functioning; IQ, intelligent quotient; MOAS, Modified Overt Aggression Scale; MPH, methylphenidate; NCBRF-D, Nisonger Child Behavior Rating Form—Disruptive Behavior; NCBRF-D-TS, Nisonger Child Behavior Rating Form—Disruptive Behavior Total Score; ODD, oppositional defiant disorder; RCT, randomized controlled trial; RMOAS, Revised Modified Overt Aggression Scale; SNAP-IV, Swanson, Nolan, and Pelham-IV Questionnaire; TOSCA, Treatment of Severe Childhood Aggression; WISC, Wechsler Intelligence Scale for Children.
RCTs of stimulant and risperidone or divalproex
Armenteros et al. (2007) assigned youth with ADHD and aggression on stable stimulant regimen to risperidone (mean 1.08 mg/day) or PBO for 4 weeks. Primary outcome was Children's Aggression Scale—Parent and —Teacher total score. Both groups improved >30% by parent (but not teacher) ratings, including 100% for COMB and 77% with PBO; no significant difference was found in mean scores between groups at study endpoint. Rate of adverse events was higher with PBO, although COMB reported more nausea and vomiting. No significant difference in weight was observed.
The Treatment of Severe Childhood Aggression (TOSCA) study of ADHD with comorbid ODD or CD first optimized stimulant for 3 weeks, then randomized youth to receive risperidone (mean 1.65 mg/day) or PBO for 6 weeks (Aman et al. 2014). All families received concurrent parent training. The primary outcome measure, Nisonger Child Behavior Rating Form (Aman et al. 1996)—Disruptive subscale showed a greater decrease for COMB with estimated ES of 0.5. Prolactin elevations, gastrointestinal upset, and initial insomnia occurred more frequently with COMB. Body mass index (BMI) did not change significantly for those receiving risperidone, although more weight gain in the risperidone group was observed.
Subsequent analysis found COMB superior for ADHD symptoms based on teacher but not parent ratings, and for ODD symptoms and peer aggression based on parent but not teacher ratings (Gadow et al. 2014). COMB treatment was associated with reductions in anxiety and psychotic spectrum symptoms (Arnold et al. 2015). Finally, analysis of cognitive measures found initial significant improvement in digit span memory for COMB at before randomization but not at study endpoint, leading authors to conclude that risperidone lacked deleterious effects on attention and short-term memory (Farmer et al. 2017).
In a 12-week blinded extension phase of the TOSCA study, responders were continued on assigned treatment. Results found prior improvement in disruptive behavior slightly diminished over the extension period with no significant difference between groups, and sustained improvement compared with study entry (Findling et al. 2017). A 52-week naturalistic follow-up found no difference in functioning based on three primary outcome measures relating to aggression and behavioral disturbance (Gadow et al. 2016). The number on multiple drugs (51% and 57%) or not prescribed medication (17%) was not significantly different based on initially having been assigned to PBO or risperidone. Youth assigned to stimulant monotherapy lost weight at 52 weeks compared with baseline, and those who received risperidone did not lose or gain weight. Persistent hyperprolactinemia was common.
Jahangard et al. (2017) conducted an 8-week RCT in youth with persistent symptoms of ADHD and ODD after treatment with MPH and family counseling. Youth were randomized to low-dose risperidone (0.5 mg/day) or PBO. Greater symptom improvement was found for COMB for oppositional problems, cognitive problems, inattention, hyperactivity, anxious-shy problems, perfectionisms, social problems, and psychosomatic problems; ES ranged from 0.45 to 0.67. Waist circumference and body weight were significantly higher with COMB. Serum prolactin was elevated with risperidone, with no difference for metabolic measures. Of importance, the MPH dose constituting nonresponse before enrollment was 10–15 mg/day, which likely does not represent dose optimization. Although authors do note clear benefit of small to medium ES, their conclusion recommends these benefits be weighed against costs of weight gain, increased waist circumference, and hyperprolactinemia.
Blader et al. (2009) studied 27 youth with ADHD and either ODD or CD. The first phase optimized long-acting MPH or dextroamphetamine, which led to improved ADHD symptoms and aggression (Retrospective-Modified Overt Aggression Scale [R-MOAS] score ≤18) in 50% of participants. Those with persistent aggression were randomized to divalproex or PBO. COMB treatment led to significantly higher rates of remission of aggressive behavior (R-MOAS score ≤10), and greater improvement in inattentive symptoms. No difference was seen on Conners Global Index—Parent total score. Valproic acid blood levels were not associated with response. Youth treated with divalproex reported more treatment-emergent sadness and initial insomnia. The small sample size resulted in a large confidence interval.
In a subsequent trial, Blader et al. (2020) enrolled 175 youth with ADHD and either ODD or CD, plus significant aggressive behavior. All youth had prior insufficient response to stimulants. Family-based behaviorally oriented psychosocial treatment occurred throughout. The first phase optimized stimulant treatment, resulting in remission of aggression in 63.6%. The 45 youth who remained aggressive were continued on stimulant and randomized to 8 weeks of risperidone (n = 17; mean 1.15 mg/day), divalproex (n = 14), or PBO (n = 9). Both combinations were efficacious for reducing aggression, and difference from PBO was larger for risperidone. Standardized BMI scores increased significantly with risperidone (+2.23 kg); compared with divalproex (+0.65 kg) and PBO (+0.02 kg). Authors noted that COMB did not result in as complete a response of aggression as those who had responded to stimulant monotherapy.
Non-RCTs
A 13-week open-label study added quetiapine for youth with ADHD, disruptive behavior disorder, and persistent aggression despite titration of osmotic release oral system (OROS)-MPH (Kronenberger et al. 2007). Five youth improved with OROS-MPH alone before adding quetiapine. The remaining 24 youth treated with quetiapine up to 600 mg daily had significant improvement of aggression. Nearly half (42%) met “stringent” criteria for clinically significant improvement. Weight decreased in the stimulant monotherapy phase and increased with added quetiapine.
A small (n = 11) open-label study simultaneously started atomoxetine with olanzapine for ADHD and comorbid disruptive behavior (Holzer et al. 2013). Youth had improved scores in ADHD-RS and R-MOAS at endpoint. Average weight gain was 3.9 kg over 10 weeks, with over half having BMI increase of 2–3 points.
A post hoc study by Aman et al. (2004) used data from two RCTs that randomized youth with CD and low intelligent quotient to either risperidone or PBO. For the subset with an ADHD diagnosis, risperidone compared with PBO was associated with improved hyperactivity, irritability, and conduct issues, for both youth taking and not taking stimulants. COMB and stimulant monotherapy were not compared directly. Weight gain was noted with risperidone use (2.17 kg).
A chart review reported on 35 youth with comorbid disruptive behavior who had been treated with stimulant plus either risperidone, carbamazepine, lithium, or other unspecified medications (Bandou et al. 2010). Risperidone showed a tendency toward improved Clinical Global Impressions—Severity (CGI-S) scores with 50% considered responders compared with carbamazepine (20%) and lithium (0%).
Stimulant and atomoxetine (summarized in Table 3)
Stimulant and Atomoxetine (N = 4)
“Bold”—if a priori identified as primary.
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale-IV; CGI, Clinical Global Impression (Severity/Improvement); COMB, combination treatment; CPRS, Conners Parent Rating Scale Revised; MPH, methylphenidate; RCR, retrospective chart review; RCT, randomized controlled trial.
Randomized controlled trial
Carlson et al. (2007) studied 25 youth with ADHD with a history of failed stimulant trial started on atomoxetine. Of those with residual symptoms after 4 weeks, half (N = 9) were randomly assigned to adjuvant OROS-MPH. No difference was found between groups on primary outcome measure, ADHD-RS. Vital sign readings and discontinuation owing to adverse events were similar between groups. Both groups continued to improve following the 4-week atomoxetine monotherapy, suggesting atomoxetine treatment for >4 weeks may be needed for optimal response.
Non-RCT
Wilens et al. (2009) examined the effectiveness of adding MPH for 50 youth who partially responded to atomoxetine during a 7-week, two-phase, open-label study. There was a 40% reduction in ADHD-RS-IV and improvements in executive functioning over the 3 weeks of COMB treatment. Insomnia, headache, appetite loss, and irritability were most commonly reported with COMB.
The first of two chart reviews examined 73 youth on atomoxetine, of whom 39 were concurrently receiving a stimulant typically owing to lack of improvement on monotherapy (Clemow et al. 2015). Most had a comorbid diagnosis. Improvement over time was noted for all treatments, with no difference in CGI-S, inattention, hyperactivity, or impulsivity between atomoxetine and COMB groups. The second chart review examined 54 cases where youth received both atomoxetine and stimulant (Scott et al. 2010). Study outcome measure was author's retrospective assessment of reason for discontinuation, without any standardized scales of efficacy. The rate of discontinuation for atomoxetine was 77%, with discontinuation reason being “success” of treatment occurring more often with concomitant stimulant and atomoxetine use than with atomoxetine alone. Conclusions were limited owing to ambiguity of outcome measure and the reason for discontinuation being “indeterminable” in 34% of charts.
ADHD medication with selective serotonin reuptake inhibitors or second generation antipsychotics for comorbid anxiety and mood disorder (summarized in Table 4)
Attention-Deficit/Hyperactivity Disorder Medication with Selective Serotonin Reuptake Inhibitor or Second Generation Antipsychotic for Comorbid Anxiety or Mood Disorder (N = 6)
“Bold”—if a priori identified as primary.
ABC, Aberrant Behavior Checklist; ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale-IV; CDI, Children's Depression Inventory; CDRS, Children's Depression Rating Scale-Revised; C-GAS, clinician ratings of global functioning; CGI, Clinical Global Impression (Severity/Improvement); CGI-P, Conners Global Index—Parent; CGI-T, Conners Global Index—Teacher; COMB, combination treatment; CPRS, Conners Parent Rating Scale Revised; DMDD, disruptive mood dysregulation disorder; GAS, (Children's) Global Assessment of Severity; MASC, Multidimensional Anxiety Scale for Children; MPH, methylphenidate; PARS, Pediatric Anxiety Rating Scale; PBO, placebo; RCT, randomized controlled trial; RMOAS, Revised Modified Overt Aggression Scale; SNAP-IV, Swanson, Nolan, and Pelham-IV Questionnaire.
Randomized controlled trial
Abikoff et al. (2005) treated youth with comorbid anxiety first by optimizing MPH. This resulted in improvements in ADHD symptoms in 81% of the 30 treatment-naive children. The 25 youth who remained anxious were randomized to 8 weeks of fluvoxamine (n = 15) or PBO (n = 10). No differences were found in anxiety, ADHD, or Clinical Global Impression—Improvement (CGI-I) between COMB and stimulant groups. Medications in both arms were well tolerated.
In 173 youth with comorbid depression or anxiety, Kratochvil et al. (2005) randomized youth to fluoxetine (n = 127) or PBO (n = 46) for 3 weeks, followed by atomoxetine for all youth for 5 weeks. The primary outcome was safety and tolerability, and COMB had higher rates of decreased appetite. Secondary outcomes for depression, anxiety, and ADHD symptoms improved for all groups, with no difference between groups for anxiety or ADHD symptoms. Greater improvements in depression rating were seen for COMB on one of the two depression scales.
In data available at
A recent similar study that did not formally meet our inclusion criteria (enrollment diagnosis related to mood dysregulation, not ADHD) combined MPH with citalopram to target irritability. Towbin et al. (2020) studied 53 youth meeting criteria for severe mood dysregulation (before Diagnostic and Statistical Manual of Mental Disorders, 5th edition [DSM-5]; American Psychiatric Association 2013, which defined DMDD). Subject comorbidities (90% of enrolled youth had ADHD; 80% had ODD) suggest this population substantially overlaps with those meeting this study inclusion criteria. Youth were treated open label with MPH and then randomized to citalopram or PBO for 8 weeks.
The initial primary outcome measure, the Aberrant Behavior Checklist—Irritability scale, used to measure irritability with autism research (McCracken et al. 2002; Marcus et al. 2009), was found to be inappropriate for the study population. The primary outcome measure became the CGI-I rated for irritability score of 1 or 2, and significantly more youth receiving combined treatment (35%) than PBO (6%) met response criteria. No difference was noted in clinician ratings of global functioning between groups. There was no effect on measures of depression or anxiety. The study did not include any standardized measure of ADHD symptoms.
Non-RCT
An open-label study included 24 youth with ADHD and DMDD, with simultaneous titration of MPH and aripiprazole over 6 weeks (Pan et al. 2018). Primary outcome measure was an author-generated three-item Swanson, Nolan, and Pelham-IV Questionnaire (SNAP-IV) subscale for “irritability,” which decreased by 3.5 points over the 6 weeks (d = 1.26). Improvement was observed in all SNAP-IV subscale scores, most Child Behavior Checklist subscale scores, and Beck Youth Inventory-II subscale scores (anxiety, depression, and angry). Two youth discontinued because of vomiting, lethargy, and dysphoric mood, six reported extrapyramidal symptoms not severe enough for discontinuation, and average weight gain was 2.67 kg.
In an open-label study of 32 youth with ADHD and high incidence of mood comorbidity, youth with persistent ADHD symptoms on MPH were given fluoxetine (Gammon and Brown 1993). Authors noted significant benefits in a wide array of measures of hyperactivity, irritability, oppositionality, anxiety, and mood.
Discussion
The first observation of this review is the relatively limited evidence base (39 studies and 17 RCTs) to support a practice that occurred in 20% of outpatient visits in 2007, and is likely higher today. No studies examined the use of three or more medications in a controlled manner. The heterogeneity of data and lack of consistency among outcome measures makes synthesis of this information challenging, although we believe a few generalizations can be made about polypharmacy in the treatment of ADHD. When positive effect is found from COMB treatment, the incremental benefit of the added medication is typically of lower magnitude than is observed with stimulants or other first-line medications, including alpha-agonists. Side effects can be greater with COMB treatment, and the duration of monitoring in the studies reviewed here does not allow the full elucidation of long-term side effects.
Regarding specific medication combinations, data from RCTs find combination stimulant and alpha-agonist consistently superior to alpha-agonist alone, although not superior to stimulant alone in all cases. Specifically, treatment with combination stimulant and alpha-agonist without history of incomplete response to stimulant did not result in superior management of ADHD symptoms compared with stimulant alone. For stimulant partial responders, addition of alpha-agonist appeared effective in reducing residual symptoms of ADHD after stimulant optimization, with the one meta-analysis noting an ES of ∼0.4. This combination was associated with somnolence, sedation, bradycardia, and hypotension.
Overall, data support COMB treatment for residual symptoms or only partial response to stimulants, but not at treatment outset for anticipated synergistic effects from different mechanisms of action. Minimal data address the effectiveness of added alpha-agonists for comorbid disruptive behavior. The short-acting nature of stimulant effects and time-limited effects of even extended-release stimulant formulations may limit complete response to stimulant monotherapy. This may contribute to improved treatment response with augmentation, although this theory was not directly addressed by any of the above studies.
Randomized-controlled data find combination stimulant and divalproex or risperidone leads to incremental benefit beyond stimulant monotherapy for comorbid aggression and disruptive behavior, with greatest empirical support for risperidone. Outcome measures varied; primary outcomes most frequently focused on level of conduct issues or aggression, and some included measures of ADHD symptoms. Clinicians should note that all studies used low-dose risperidone (mean dose <2 mg/day for all studies, which has been termed “ultra-low dose” in schizophrenia research; Li et al. 2009). Despite low doses and often short study duration, significant prolactin elevation and weight gain were seen in risperidone trials.
The single small RCT with atomoxetine found robust response to atomoxetine without evidence of improvement with added MPH, with specific suggestion that optimizing dose and allowing adequate duration for response is favorable to adding medications. Observational studies were mixed and had significant methodological limitations. Studies that reported side effects noted some increased rates of vital sign abnormalities, although small sample sizes limit conclusions.
Finally, RCT data combining SSRI with ADHD medication for management of comorbid anxiety, depression, and DMDD supports safety but not efficacy of these combinations. Comorbidity between ADHD and targets of SSRIs such as anxiety and depression may lead to co-prescribing, and the relative comfort child psychiatric providers have with each of these medication classes independently may increase perceived safety and/or efficacy of the combination, despite limited evidence.
The limited studies on this combination constitute a large gap between evidence base and clinical practice, as these medications are commonly co-prescribed in clinical practice (Díaz-Caneja et al. 2014). The reason for this discrepancy is unclear, although the same has been noted for studies on adult polypharmacy (Schatzberg and DeBattista 2015) and attributed to lack of motivation by both the pharmaceutical industry and National Institute of Mental Health to study what are currently off-label medication uses. Authors hypothesize that cost of high-quality controlled studies without clear financial benefit limits pharmaceutical company investment in this research.
This review has several limitations. Authors did not assess risk of bias in any systematic way. Of the 17 RCTs, seven reported funding from the pharmaceutical industry, and in several grant-funded projects author disclosures revealed ties to industry. Six of the 10 nonrandomized trials were funded by industry (2 did not report funding); and 1 of the 3 RCRs was industry funded. Clinicians should be aware of the risk of bias owing to financial ties to pharmaceutics industry, although these studies currently represent the only available data in the field. Another limitation is that the initial goal of the review was to identify studies of polypharmacy for all child and adolescent psychiatric disorders, and only in subsequent steps focused on ADHD, which could have led to missing pertinent studies.
Study methods including screening of abstracts may have failed to identify all articles containing pertinent data. Inclusion was limited to studies reporting some measure of efficacy of combinations; those reporting only safety or side effect data were excluded, and this should not be considered a comprehensive review of data regarding adverse effects of polypharmacy. Finally, the authors identified the need for synthesis of the evidence base for polypharmacy owing to their collective identification of polypharmacy being an area of concern in the psychiatric care of child and adolescents, which may bias interpretation and reporting given the descriptive nature of this analysis.
Conclusion
The data reviewed here support pharmacologic recommendations of existing guidelines (Pappadopulos et al. 2003; Pliszka et al. 2006) including a stepwise approach to treating ADHD with comorbid disruptive behavior and aggression, starting with stimulant optimization and behavioral treatments. ESs of stimulants are large, even when addressing symptoms that fall outside the typical diagnostic symptomatology, as seen for aggression in the studies by Blader et al. (2009, 2020).
This review supports the idea that beginning with COMB treatment misses those children who would adequately respond to stimulant monotherapy, creating unnecessary exposure to polypharmacy and associated risks. In current guidelines, addition of antipsychotic medication is recommended only when aggression is severe and/or persistent (Pliszka et al. 2006). In our review, low-dose risperidone augmentation for residual comorbid disruptive and aggressive behavior showed a consistent although less robust effect than stimulant monotherapy, and two RCTs demonstrated some effectiveness of divalproex augmentation.
Clinical significance of these statistically significant differences remains unclear, and the physician must determine if the magnitude of anticipated impact of added medication justifies the risk. For example, if the two-point reduction seen in antisocial behavior in the TOSCA trial would prevent out-of-home placement or facilitate a less restrictive placement in school, then higher risk medication could be tolerable.
Close monitoring of response is imperative, as it remains unknown if the relatively smaller impact of added medication is owing to these medications having a less robust effect, or represents some youth responding well and some not at all. Youth who do not respond to monotherapy can be quite ill and display extreme symptoms that impact their functioning and relationships; this may represent a more severe form of ADHD or disruptive behavior disorder, or an inherently different underlying pathophysiology associated with diminished treatment responsiveness (Blader et al. 2020). Starting a second medication particularly for aggressive or disruptive behavior should involve vigilant observation of the actual clinical effects and side effects, including the use of standardized measures or assessment scales to monitor target symptoms or behaviors. This is especially important in the case of risperidone and other SGAs, which have significant risk of weight gain, metabolic disturbance, hyperprolactinemia, and extrapyramidal side effects.
Clinicians should develop sequential plans such as a timeframe for trial discontinuation after improvement or alternative strategies should negative effects be observed. Authors synthesizing data from the TOSCA studies provide specific guidance that risperidone should be discontinued if ineffective, if observed risks outweigh benefits, and even when effective, after 6 months of improved aggression (Barterian et al. 2017). Ideally, evidence-based psychosocial interventions are simultaneously implemented that would facilitate stabilization and discontinuation of higher risk medications. Together, these steps would prevent polypharmacy being indefinite without a clear observation of benefit or defined endpoint.
Given the current prevalence of polypharmacy, additional high-quality randomized studies are needed to better understand which combinations are effective for which clinical presentations, for how long and at what long-term risks. Information is also lacking about the long-term safety of individual medications, safety of drug combinations, frequency of drug–drug interactions, and safety and effectiveness of combining with commonly used vitamins and supplements. Clinicians are faced daily with clinical use of medication combinations with insufficient information to guide these decisions. Investment is urgently needed to prioritize studying safety and effectiveness of medications combinations.
Footnotes
Clinical Significance
ADHD is a common presenting issue in child and adolescent psychiatric practice. Polypharmacy is increasingly common in treating ADHD. This review summarizes and synthesis existing studies examining the efficacy of two or more medications prescribed simultaneously for treatment of ADHD and comorbid conditions.
Statistical Consultant
No consultant was utilized for this review.
Disclosures
M.B. and J.C.H. report no biomedical financial interests or potential conflicts of interest. C.B. reports the following: Medical Director of the National Training and Technical Assistance Network for Children's Behavioral Health funded by SAMHSA; Clinical Consultant for the National Quality Improvement Center on Tailored Services, Placement Stability, and Permanency for LGBTQ Children and Youth in Foster Care funded by the Children's Bureau, ACF of HHS; volunteer Board member of the Association of Children's Residential Centers and the National Association for the Advancement of Adolescent Health. C.B. has been an expert witness for Children's Rights, Disability Rights of Vermont and The National Center for Youth Law. He reports no Pharma conflicts of interest. R.H. reports consult work for Optum, book royalties from American Psychiatric Association Publishing, and research funding from the National Institute of Health and Human Resources and Services Administration. G.A.C. reports research funding from the National Institute of Mental Health and Patient-Centered Outcomes Research Institute; G.A.C.'s husband is on the Data Safety Monitoring Boards of Lundbeck and Pfizer.