
Abstract
Objectives:
To describe the study design and clinical characteristics of patients in the Sertraline Pediatric RegIstry for The Evaluation of Safety (SPRITES).
Methods:
SPRITES is an open-label postmarketing study of development and safety outcomes in patients aged 6 to 16 years treated with sertraline (with or without psychotherapy) compared with psychotherapy alone for up to 3 years in the United States. Baseline data included demographics and psychiatric history. Primary outcomes included measures of cognitive and emotional development (Trails B, Behavior Rating Inventory of Executive Function [BRIEF]), physical development (height and weight), and pubertal status (Tanner Stage). Data were also collected on present/lifetime risk of suicide-related events using the Columbia-Suicide Severity Rating Scale.
Results:
SPRITES enrolled 941 patients between the ages of 6 and 16 years. Patients' baseline mean age was 11.9 years (2.9), 57.2% were female, and 84.8% were white. Most patients (78.4%) had an anxiety disorder, and 15.6% were diagnosed with obsessive-compulsive disorder. The mean age at onset of first mental illness was 7.9 years. A higher percentage of sertraline-treated patients compared with patients who received no pharmacological treatment received prior psychotherapy (59.0% vs. 34.4%, p < 0.001), psychotropic medications for a psychiatric disorder (14.1% vs. 3.3%, p < 0.001), and other non-sertraline selective serotonin reuptake inhibitors (8.6% vs. 1.2%, p < 0.001). Most patients were moderately ill on the Clinical Global Impressions-Severity scale, and a higher (p < 0.001) percentage of sertraline-treated patients had a moderate-to-severe mental illness score compared with the no pharmacological treatment group (73.0% vs. 57.8%, respectively). Although patients at high and imminent risk of a suicidal event were excluded at study entry, the sertraline-treated patients reported higher levels of lifetime suicidal behavior compared with patients treated with no pharmacological treatment (5.8% vs. 2.5%, p = 0.039).
Conclusions:
Baseline data from this nonrandomized observational study suggest that patients prescribed sertraline are reflective of a more mentally ill study population compared with patients receiving psychotherapy.
ClinicalTrials.gov identifier: NCT01302080.
Introduction
Sertraline is a selective serotonin reuptake inhibitor (SSRI) that has demonstrated efficacy in the treatment of children and adolescents with moderate-to-severe obsessive-compulsive disorder (OCD) (March 1998). Although only approved for the treatment of OCD in pediatric patients (Zoloft 2021), sertraline is used off-label to treat various psychiatric conditions in child and adolescent clinical practice. Approximately 4.8% of all prescriptions for 12- to 19-year olds are for antidepressants, ranking third after psychostimulants (6.1%) and bronchodilators (5.4%) (Gu 2010). Expanded use of antidepressants for adolescents was corroborated in another national survey of trends in 12-month prevalence of major depressive episodes and treatment between 2005 and 2014 showing a significant increase in medicated youth age 12 to 17 years old (Mojtabai et al. 2016). Furthermore, SSRIs comprise a significant proportion of antidepressants prescribed for pediatric depression treatment, with more than 70% of child and adolescent (aged 0–19 years) users taking an SSRI (Zito et al. 2002; Bachmann et al. 2016). These data were corroborated in a recent study of a large Medicaid population of children and adolescents younger than 20 years whereby SSRI use represented 78% of total antidepressant users (Zito et al. 2020).
In contrast to short-term effectiveness, the long-term impact of sertraline use on physical, cognitive, and emotional development has not been systematically explored in the context of benefits and tolerability of sertraline in children and adolescents. One study conducted by Günther et al. (2005) investigated the effect of a 6-week course of sertraline on verbal memory and attention in 28 children and adolescents diagnosed with various anxiety disorders, including social phobia and generalized and separation anxiety disorders, compared with 28 healthy controls. No significant difference was reported between sertraline and control groups regarding attentional performance (p > 0.05). However, patients treated with sertraline had a higher response speed in a divided attention paradigm, compared with controls (p = 0.02), whereas performance of the interference part of a verbal memory task decreased (p = 0.05). Methodological limitations of this study include use of healthy controls instead of controls with similar psychiatric diagnoses, short duration of treatment, and limited power due to small sample size.
In a second study of 267 risperidone-treated 5- to 17-year-old boys previously enrolled in studies aimed at examining skeletal effects of risperidone, SSRI use was associated with reduced longitudinal growth, particularly in those undergoing puberty (Calarge et al. 2018). Methodological limitations of this study include not primary evidence (i.e., reanalysis of data collected from four studies and subsequent limitations inherent in pooling data), confounding by indication, confounding due to concurrent psychostimulant use, and potential interaction due to concurrent risperidone use. Whether adult height or other metabolic or psychological outcomes were affected was not studied. Nevertheless, given the dearth of published literature and multiple methodological weaknesses with the available evidence, this study was designed to obtain safety information for patients with long-term sertraline use. This study was conducted to fulfill a regulatory commitment to the Medicine Evaluations Board in the Netherlands.
Sertraline Pediatric RegIstry for The Evaluation of Safety (SPRITES), a long-term multicenter, open-label, prospective observational study, was designed to compare sertraline with psychotherapy with respect to development and safety outcomes, including the primary outcomes of cognitive, emotional, and physical development, and pubertal maturation. Psychotherapy was chosen as the comparator group since psychosocial interventions, including psychotherapy and behavioral therapies such as cognitive behavioral therapy (CBT), are often utilized as the first-line treatment for anxiety disorders in children, including mild-to-moderate OCD (Walkup et al. 2008). We chose an observational study design to enable enrollment of children and adolescents who are prescribed sertraline in real-world clinical settings. The study is near completion, and the main analyses, although described herein, are not yet publicly available. The purpose of this article was to describe the design, methods, and rationale of the SPRITES study and to present the clinical characteristics of the baseline sample.
Methods
Study design
An observational study design was chosen with minimal modification of normal medical care, other than ascertainment of postbaseline study assessments of cognition, emotional, and physical development, and pubertal maturation. Following initiation of sertraline treatment within 45 days of study enrollment, patients received sertraline (with or without psychotherapy) or psychotherapy alone (referred to as “no pharmacological treatment” for the purpose of this analysis) in an unblinded manner. Patients in the sertraline group were eligible if s/he were being treated for any mental disorder that would be appropriately treated with an SSRI. Types of psychotherapy in this study included CBT, supportive therapy, family therapy, group therapy, and play therapy. Patients were prospectively followed as clinically appropriate, and outcomes were assessed. No laboratory testing was required by the protocol. As this is an observational study, treating physicians were permitted to change the treatment of individual patients at any time based on their clinical judgment. Consequently, patients could switch from one treatment modality to another during the study.
Study sites
Approximately 900 children and adolescents were to be enrolled in the study from 50 U.S. centers from academic, community, and private clinic settings, including those from the Child and Adolescent Psychiatry Trials Network (CAPTN). CAPTN began in 2003 as a National Institute of Mental Health (NIMH)-funded practical clinical trials network in pediatric psychiatry (Shapiro et al. 2009). Even after NIMH funding ended, the network was intended to be operational with support from the Duke Clinical Research Institute (DCRI) for the duration of SPRITES. Due to lower than expected patient enrollment, site participation was broadened to include non-CAPTN sites.
Study enrollment
Physicians were provided the approved labeling for sertraline and asked to use this information, coupled with their clinical judgment, to determine whether the patients were eligible for inclusion in the study. Study entry criteria allowed enrollment of patients who were eligible for treatment with sertraline based on their physician's clinical judgment with some exclusions (Table 1). Use of psychostimulants known to be associated with a growth delay was originally excluded; however, this criterion was later amended to exclude any patient taking stimulants at baseline. The decision to exclude concurrent psychostimulants was based on the potential confounding effect of psychostimulant use in children on growth, a known and widely published drug effect. For each patient who met study entry criteria, participating physicians followed the steps outlined in Figure 1.
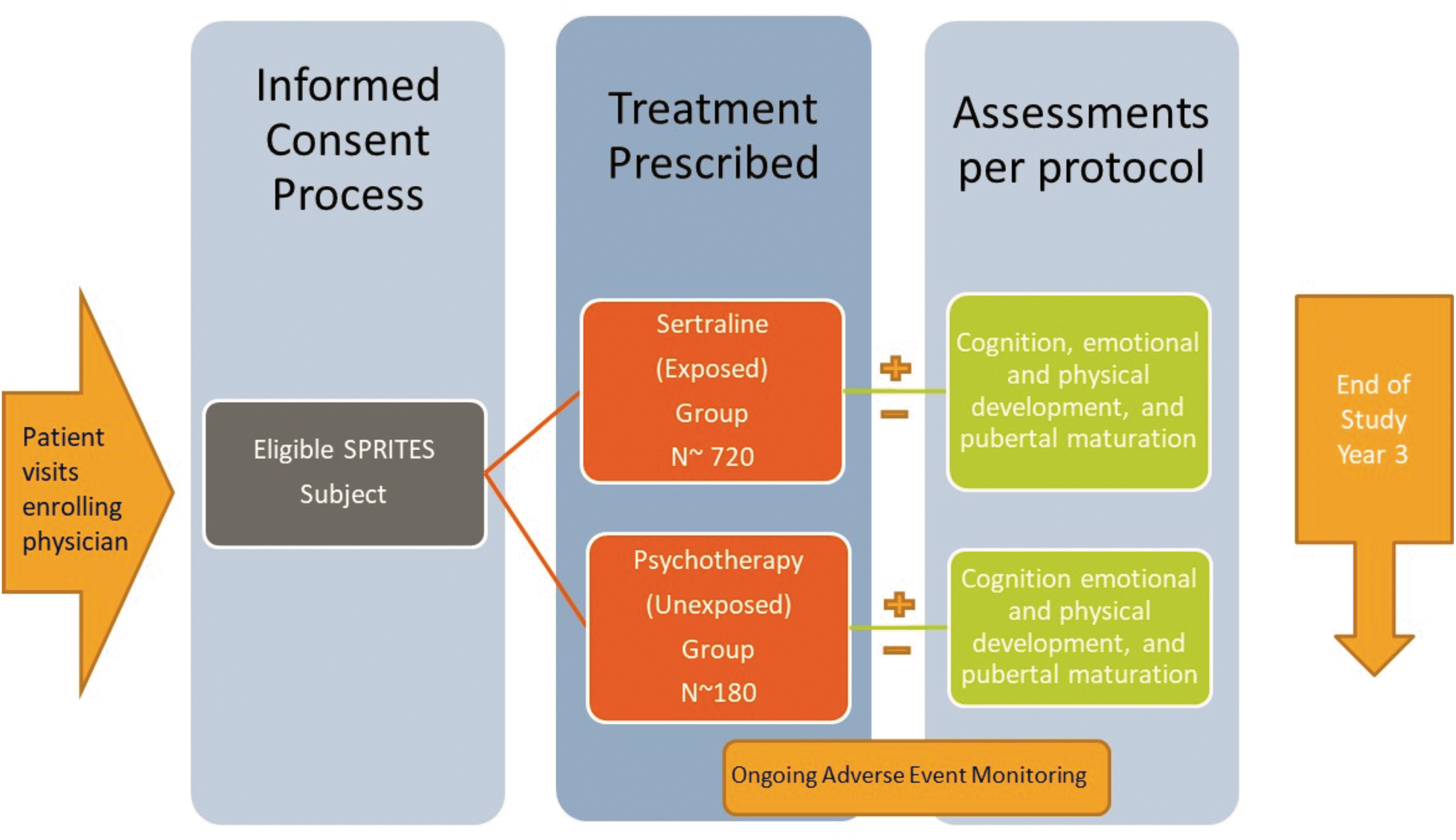
SPRITES study schematic. SPRITES, Sertraline Pediatric RegIstry for The Evaluation of Safety.
Inclusion and Exclusion Criteria
BRIEF, Behavior Rating Inventory of Executive Function; NOS, not otherwise specified; SPRITES, Sertraline Pediatric RegIstry for The Evaluation of Safety; SSRI, selective serotonin reuptake inhibitor.
After a physician determined that a patient was eligible for inclusion in the study and willing to participate, the patient signed a written and dated assent form with corresponding parental consent, acknowledging his or her understanding of the risk and benefits of participating in the study. Patients who reached the age of majority (i.e., 18 years) were reconsented and signed a written informed consent. The baseline electronic case report form collected information on demographics, psychiatric diagnoses, psychiatric history, family psychiatric history, previous treatment with psychotropic medications, Clinical Global Impressions-Severity (CGI-S, a measure of severity of the underlying psychiatric diagnosis), suicidal events captured on the Columbia-Suicide Severity Rating Scale (C-SSRS), and primary outcome assessments. Study enrollment occurred between April 2012 and July 2017.
Baseline study treatment
At baseline (or within 45 days prior), patients were prescribed sertraline, with or without psychotherapy, or psychotherapy only (i.e., no pharmacotherapy). Patients were classified into a baseline treatment exposure category based on treatment exposure information collected at the baseline visit and at the Month 3 visit. Treatment exposure information for the Month 3 visit was collected for each month between the baseline and Month 3 visits. Only the first of these months that had exposure information available was used for the Month 3 visit information used to determine treatment exposure at baseline. The baseline treatment exposure categories are as follows: Sertraline: the patient was exposed to sertraline (with or without psychotherapy or other antidepressant treatment) at baseline. Other Antidepressants: the patient was exposed to only non-sertraline antidepressant treatment (with or without psychotherapy) during the first month between the baseline and Month 3 visits that had antidepressant exposure information available. No Pharmacological Therapy: the patient received psychotherapy only or no treatment at all at baseline. Patients were classified into this exposure category if they did not meet the criteria to be classified into either the Sertraline or Other Antidepressants categories.
Study follow-up
To align with the real-world nature of the study, each patient was to be followed for 3 years, regardless of how long s/he continued or switched treatment based on their physician's clinical judgment. Follow-up information on the primary outcome measures, secondary outcome measures, possible adverse events (AEs), and serious AEs (SAEs) were collected at regular intervals by the treating physician or other designated member of the medical care team. Structured data collection occurred at 3, 6, 12, 18, 24, 30, and 36 months following the baseline visit. Clinicians were encouraged to schedule follow-up visits so that the routine visit data and study assessments for those patients were gathered during or near the key postbaseline assessment points, as clinically indicated. If a patient was unable to be contacted, three attempts were made to follow-up with the patient. A patient was deemed lost to follow-up if: (1) s/he moved with no prospect of continuing in the study, that is, with no local participating center to which the patient could transfer or (2) there was no contact for a period of 6 months despite three attempts to re-contact the patient/parent/guardian.
Study outcomes
At each study visit, measurements were collected on the primary outcome measures as summarized in Table 2.
Summary of Primary and Secondary Outcome Measures in Sertraline Pediatric RegIstry for The Evaluation of Safety
BRIEF, Behavior Rating Inventory of Executive Function.
Clinicians also monitored patients closely for any AEs or indications of suicidal feelings, behavior changes, or other signs of clinical deterioration. At each study visit, AEs were assessed using the 43-item Pediatric Adverse Events Rating Scale (PAERS), which is an empirically derived and validated AE monitoring tool. The PAERS monitoring tool provides coverage for common important AEs due to all major classes of central nervous system-active medications (Wehmeier et al. 2008). SAEs were collected and reported to the Pfizer Safety Database, and suicidal events were ascertained using the C-SSRS (Posner et al. 2007; Posner 2011).
The study was approved by the Copernicus Institutional Review Board, Western Institutional Review Board, and 24 local Institutional review boards as well as the Duke University Health System Institute Review Board. The Duke University Health System Institute Review Board covers the DCRIs coordinating center activities.
Statistical analysis of baseline data
The analysis of baseline data, as presented in this article, include summaries of patient enrollment, baseline characteristics, baseline primary outcome data, and baseline safety data. Patient follow-up is still ongoing, therefore the main analyses, although described herein, will not be completed until the last patient completes the study and the study database is locked.
Patient enrollment and study completion were summarized by the treatment that was planned for the patient at baseline, whereas all other baseline summaries were analyzed by the actual treatment received at baseline. Comparisons of the baseline characteristics between the three study groups, Sertraline, Other Antidepressants, No Pharmacological Therapy, were completed to evaluate whether differences exist in these baseline characteristics by the actual treatment that a patient received at baseline.
Descriptive summaries of baseline measurements were produced and stratified by the actual treatment received at baseline. Baseline measures include results from: Trails B assessment, Behavior Rating Inventory of Executive Function (BRIEF) Metacognition Index, BRIEF Behavioral Regulation Index, Tanner Stage, height, and weight. Body mass index (BMI) was analyzed as an outcome measure to provide height-adjusted weight data. All primary outcome measures, with the exception of Tanner Staging, were standardized. BRIEF, height, and weight outcome measures were sex and age standardized via a Z-score or T-score, and Trails B and BMI was standardized by age only. All primary outcome measures, as well as BMI, were also summarized using nonstandardized results. Missing data were left as missing and were not imputed, except for missing C-SSRS suicidal ideation (SI) information at baseline, which was imputed using the SI over the lifetime of the patient. In addition, when the patient did not provide information about sertraline or other antidepressant exposure, he/she was categorized as being exposed to No Pharmacological Therapy.
Descriptive baseline safety summaries were provided for: (1) C-SSRS assessments, (2) PAERS assessments, (3) SAEs, and (4) deaths by the actual baseline therapy exposure. All summaries of safety data were among patients in the safety population who are patients that meet at least one of the following criteria:
Have PAERS or SAE information available during follow-up.
Have treatment information available during follow-up.
Have a postbaseline C-SSRS assessment.
C-SSRS results at baseline contain information on SI and suicidal behavior (SB). The information collected for SI for the baseline visit includes SI across the lifetime of the patient as well as SI within the last 6 months before the baseline visit. The information for SB for the baseline visit includes only the SB across the lifetime of the patient. Descriptive summaries of SI data at baseline included both the information collected corresponding to the entire lifetime of the patient as well as within the last 6 months. A summary of SB data across the lifetime of the patient was completed.
Main analysis of final data
Descriptive summaries of the primary and secondary outcome measures will be produced for each visit and will be stratified by the treatment exposure since the previous visit. For each follow-up visit, the change in a patient's value from their baseline value will be calculated for both standardized and nonstandardized results. Pubertal development will be assessed and summarized utilizing shift tables that will display the summary of individual patient changes in Tanner Stage at each year following the baseline visit.
Change from baseline in Trails B, BRIEF Metacognition Index, BRIEF Behavioral Regulation Index, height, weight, BMI, and Tanner Stage will be analyzed using a marginal structural model (MSM) framework, a repeated-measures model that accounts for potential treatment switching and dropout using inverse probability weighting (Robins et al. 2000). An MSM analysis is a weighted repeated-measures approach using treatment as a time-varying covariate. Weights produce a pseudo-population with a balance in both time-invariant and time-varying covariates supporting causal treatment comparisons using standard repeated-measures models. Adjustments for data missing at random or missing completely at random can be incorporated directly into the proposed models. The MSM analyses will address the relationship between sertraline exposure and the outcomes and will be run multiple times using different definitions for the sertraline exposure as follows:
Cumulative exposure as a continuous variable
Cumulative exposure as a categorical variable
Recent exposure as a continuous variable
Recent exposure as a categorical variable
Sertraline-exposed (“Always Exposed”) versus unexposed (“Never Exposed”)
Cumulative sertraline exposure is defined at a particular visit as the total amount of sertraline (in mg) taken by the patient between the baseline visit and the visit divided by the number of days between the baseline visit and the visit. For a given visit, recent sertraline exposure is defined as the total amount of sertraline (in mg) taken by the patient since the previous visit divided by the number of days between the previous visit and the current visit.
Patients corresponding to the “Always” group will be those patients who are on sertraline at baseline and are still on sertraline for at least their 3-month visit. The visits included for “Always” patients will be those visits where the patient has not yet stopped taking sertraline since their baseline visit. Patients corresponding to the “Never” group will be those patients who are not on sertraline at baseline and are still not on sertraline for at least their 3-month visit. The visits included for “Never” patients will be those visits where the patient has not yet started taking sertraline since their baseline visit.
Postbaseline C-SSRS data will be summarized descriptively among patients in the safety population. Postbaseline C-SSRS data will be summarized based on if there was SI or SB at any time during the follow-up as well as if there was SI or SB at a particular visit during the follow-up. New onset or worsening SI or SB data will also be summarized separately in patients who did and did not switch treatment after baseline. In patients who switched treatment after baseline, these data will be summarized by whether a new onset or worsening of SI or SB occurred before, at or after the visit where a patient first switched treatment after baseline.
The C-SSRS outcome of a new or worsening SI or SB will be the only safety information that will be analyzed using the MSM analysis framework. If a patient's baseline SI data are missing, then the SI across the lifetime of the patient, if it is available, will be used for the baseline SI data. This MSM approach will only focus on the comparison of sertraline-exposed (“Always Exposed”) to unexposed (“Never Exposed”) patients.
Results
SPRITES enrolled 941 patients between the ages of 6 and 16 years.
Demographics
The breakdown of baseline demographics and primary psychiatric disorders are given in Table 3. Baseline comparisons are possible between the Sertraline and No Pharmacological Therapy groups; however, the small number of patients in the Other Antidepressants group at baseline precludes meaningful comparisons to this group (use of other antidepressants at baseline was a study exclusion criterion, and the number of patients in the Other Antidepressants group at baseline [n = 2] was consequently low).
Baseline Demographics and Psychiatric Diagnoses (All Patients)
All patients = all patients enrolled in SPRITES. The three therapy exposure categories were based on the actual treatment received at baseline. Diagnosis categories were not mutually exclusive; investigators could have reported more than one primary diagnosis.
Max, maximum; Min, minimum; NOS, not otherwise specified; OCD, obsessive-compulsive disorder; Q, quartile; SD, standard deviation; SPRITES, Sertraline Pediatric RegIstry for The Evaluation of Safety.
The mean baseline age was 11.9 years (standard deviation of 2.9), 57.2% were female, and 84.8% were white. Overall, the majority of patients in the Sertraline and No Pharmacological Therapy groups had an anxiety disorder (80.0% and 74.2%, respectively). A higher percentage of patients in the Sertraline group than the No Pharmacological Therapy group had a mood disorder (52.1% vs. 32.4%, p < 0.001), and a lower percentage of patients in the Sertraline group than the No Pharmacological Therapy group had an OCD disorder (13.7% vs. 21.3%, p = 0.006).
Psychiatric history, medication use at baseline, and severity of mental illness
The mean baseline age at the onset of first mental illness was 7.9 years, and the most frequently reported family history of mental illness was depressive and anxiety disorders, 63.2% and 60.5%, respectively (Table 4).
Baseline Psychiatric History (All Patients)
All patients = all patients enrolled in SPRITES. Assignment to the three therapy exposure categories was based on the actual treatment received at baseline.
All applicable history of family illness categories can be chosen. The denominator for the history of family illness categories besides “None” and “Unknown” is the number of patients that are indicated as having a history of family illness.
ADHD, attention-deficit/hyperactivity disorder; CD, conduct disorder; Max, maximum; Min, minimum; OCD, obsessive-compulsive disorder; ODD, oppositional defiant disorder; PDD, pervasive developmental disorder; PTSD, posttraumatic stress disorder; Q, quartile; SD, standard deviation; SPRITES, Sertraline Pediatric RegIstry for The Evaluation of Safety.
A summary of past treatment for primary psychiatric disorders and CGI-S, a global rating of illness severity, is presented in Table 5. When compared with the No Pharmacological Therapy group, a higher percentage of sertraline-treated patients received prior psychotherapy (59.0% vs. 34.4%, p < 0.001), psychotropic medications for a psychiatric disorder (14.1% vs. 3.3%, p < 0.001), and non-sertraline SSRIs (8.6% vs. 1.2%, p < 0.001). Psychiatric medications used by ≥5% of patients in any treatment group included psychostimulants and alpha-2 agonists. The percentage of patients who used psychostimulants was similar for the Sertraline and No Pharmacological Therapy groups (18.7% and 16.4%, p = 0.441), whereas the percentage of patients who used alpha-2 agonists was higher in the Sertraline group than in the No Pharmacological Therapy group (7.5% vs. 1.6%, p < 0.001).
Treatment for Primary Psychiatric Disorders and Clinical Global Impressions-Severity Before Baseline (All Patients)
All patients = all patients enrolled in SPRITES. Assignment to the three therapy exposure categories was based on the actual treatment received at baseline.
AE, adverse event; CGI-S, Clinical Global Impressions-Severity; Max, maximum; Min, minimum; NERI, norepinephrine reuptake inhibitor; Q, quartile; SD, standard deviation; SNRI, serotonin norepinephrine reuptake inhibitor; SPRITES, Sertraline Pediatric RegIstry for The Evaluation of Safety; SSRI, selective serotonin reuptake inhibitor.
For the clinician-rated CGI-S scale, most patients were moderately ill, and a higher percentage of sertraline-treated patients had a moderate-to-severe mental illness score (73.0% vs. 57.8%, p < 0.001).
SI and SB
A total of 205 patients (29.5%) in the Sertraline group and 60 patients (24.6%) in the No Pharmacological Therapy group reported any history of SB and/or SI during their lifetime (Table 6), as reported at baseline. The numerical difference in percentages was due to the higher proportion of sertraline-treated patients who reported SB (5.8% vs. 2.5%, p = 0.039). Note that in the current study, the investigators had already excluded those patients at high and imminent risk of a suicidal event at study entry. Thus, within 6 months before baseline, a numerically higher proportion of patients in the Sertraline group reported SI compared with the No Pharmacological Therapy group (21.3% and 17.5%, p = 0.257). Screening and baseline C-SSRS data reflect that a greater proportion of patients in the Sertraline group than in the No Pharmacological Therapy group reported the most severe ideation types including active SI with some intent to act without a specific plan and active SI with specific plan and intent (i.e., the rates are generally three to five times higher in the Sertraline group than in the No Pharmacological Therapy group at both lifetime and in the last 6 months before baseline).
Columbia-Suicide Severity Rating Scale at Screening and Baseline (All Patients)
All patients = all patients enrolled in SPRITES. The treatment categories are based on the actual treatment received at baseline.
SI, suicidal ideation; SB, suicidal behavior; SPRITES, Sertraline Pediatric RegIstry for The Evaluation of Safety.
Discussion
To the best of our knowledge, SPRITES is the first and largest prospective observational study conducted among children to examine the long-term safety of sertraline or any SSRI. It promises to yield clinically relevant information on the safety of a widely used SSRI and should also provide a valuable perspective on routine medical care of children with depressive and anxiety disorders. Previous data demonstrated effectiveness and safety of sertraline with short-term use. Thus, the goal of this study was to determine whether long-term use of sertraline when taken to treat children with various psychiatric disorders under routine clinical care affects growth and development.
Baseline comparisons between the Sertraline and No Pharmacological Therapy groups are possible; however, the use of other antidepressants at baseline was a study exclusion criterion, and the small number of patients in the Other Antidepressants group (n = 2) at baseline precludes meaningful comparisons to this group.
At baseline, the mean age of patients in the Sertraline group was greater than that of patients in the No Pharmacological Therapy group. The mean ages at baseline of patients in the Sertraline and No Pharmacological Therapy groups were ∼12.2 and 11.1 years, respectively. At baseline, the majority of patients in the Sertraline group were female (58.3%), white (84.5%), and not Hispanic or Latino (89.5%). The majority of patients in the No Pharmacological Therapy group at baseline were female (53.7%), white (85.7%), and not Hispanic or Latino (90.6%).
Baseline psychiatric history was similar among the Sertraline and No Pharmacological Therapy groups, except for a higher rate of a family history of depressive disorder in the Sertraline group than the No Pharmacological Therapy group (64.6% vs. 59.0%, respectively) and a lower rate of a family history of OCD (13.3% in the Sertraline group vs. 20.2% in the No Pharmacological Therapy group). The majority of patients in both the Sertraline and the No Pharmacological Therapy groups had an anxiety disorder (80.0% and 74.2%, respectively). A higher percentage of patients in the Sertraline group than the No Pharmacological Therapy group had a mood disorder (52.1% vs. 32.4%, respectively). A lower percentage of patients in the Sertraline group than the No Pharmacological Therapy group had an OCD disorder (13.7% vs. 21.3%, respectively). The treatment history of the groups suggests that patients in the Sertraline group generally had more severe underlying psychiatric illness than their counterparts in the No Pharmacological Therapy group at baseline; this observation is in line with customary clinical practice and treatment guidelines.
SI, SB, and self-injurious behavior without suicidal intent or of unknown intent were more common in the Sertraline group than the No Pharmacological Therapy group at baseline.
SPRITES has a number of design features of note. First, simple study procedures permit approximation of real-world clinical practice and allow for observation periods that are much longer than in typical clinical trials. Also, outcomes may be less completely recorded since we rely on reports from psychiatrists or other treatment team members for these outcomes instead of the child's primary pediatrician.
Second, as an observational study, SPRITES is susceptible to confounding resulting from imbalances in the distribution of baseline factors between the treatment groups since treatment is not randomly allocated. This can only be achieved through baseline randomization of study treatment, which would greatly minimize selection bias, a major limitation of observational studies. In other words, patients who receive different drugs may be inherently at different risk of the outcomes of interest. Randomization of exposure provides increased credibility to the study's comparative results. In clinical practice, patients treated with sertraline may be systematically different from those treated with psychotherapy and other antidepressants due to the prescribers' channeling of the drug to patients with varying severity of underlying mental illness. This possibility exists given failed attempts at psychotherapy, or conversely, prescribing physicians concerned about SI- and SB-related events may selectively avoid sertraline. Given these likely selection phenomena, randomization would be the best approach affording the certainty of a fair comparison between groups. Similarly, channeling bias could explain the inclusion of more patients diagnosed with OCD at baseline since psychosocial interventions are often utilized as the first-line treatment for anxiety disorders in children, including mild-to-moderate OCD.
Furthermore, given the observed imbalance in several baseline characteristics, it will be critical to control for key baseline characteristics. In the absence of randomization, we attempted to control for these selection phenomena as well as stable and time-varying confounders, treatment discontinuation, and switches, by utilizing an MSM approach (Robins et al. 2000). These key baseline characteristics include the baseline severity of psychiatric illness as well as the lifetime prevalence of SI, SB, and self-injurious behavior.
Third, its large sample size enables generalization and applicability of the study results to the population of children with these psychiatric disorders. Furthermore, long-term studies are often plagued with high patient attrition rates; therefore, this study attempted to recruit a sizable number of patients to offset this study limitation.
Conclusions
Examining the baseline data now available for SPRITES, one can see that patients prescribed sertraline are reflective of a more mentally ill population when compared with persons treated with psychotherapy only, as evidenced by:
Summary of baseline CGI-S data.
Higher percentage of sertraline-treated patients received prior psychotherapy, psychotropic medications for a psychiatric disorder, and treatment with a non-sertraline SSRIs.
Higher levels of lifetime and baseline SI/SB in the sertraline-treated group compared with patients receiving No Pharmacological Therapy.
For a nonrandomized study, these baseline results are not surprising, especially since children and adolescents treated in routine clinical practice with an SSRI have typically undergone multiple treatment modalities before pharmacological therapy. Also, physicians enrolled patients with mental health disorders that they deemed eligible to receive treatment with sertraline (according to their clinical judgment) even though sertraline is only approved for treatment of OCD in children aged 6 to 17 years. As a result, this study also demonstrates the extent of off-label use in children with mental health illness. Since the purpose of SPRITES is to follow pediatric patients in real-world clinical practice, these baseline results provide reassurance that the study population is generally reflective of children treated with sertraline outside the confines of a study.
Clinical Significance
Although only approved for the treatment of OCD in pediatric patients, sertraline, an SSRI, is used off-label to treat various psychiatric conditions in child and adolescent clinical practice. Furthermore, SSRIs comprise a significant proportion of antidepressants prescribed for pediatric depression treatment. In contrast to short-term effectiveness, the long-term impact of sertraline use on physical, cognitive, and emotional development has not been systematically explored in the context of benefits and tolerability of sertraline in children and adolescents. Nevertheless, given the dearth of the published literature and multiple methodological weaknesses with the available evidence, this study was designed to obtain safety information for patients with long-term sertraline use.
Footnotes
Authors' Contributions
F.K. participated in the design of the study. S.B., F.K., S.R., P.C., J.O., W.B., S.C., and Y.L. were involved with scientific/logistical/operational decisions, assisted with drafting of the study statistical analysis plan, interpreted the data, and helped draft the article. All authors read and approved the final article.
Acknowledgments
We thank all the investigators and coordinators who took part in this study; the 941 participants in SPRITES; the Pfizer Medical, Worldwide Safety and Regulatory: Nicolle Gatto, Cynthia DeLuise, Tanya Russell, Omar Ahmed, Sarah Dubrava, Lisa Falato, and Lisa Ludwig. Joann Munting is an employee of Execupharm, who was a paid contractor to Pfizer in the management of this study. John March, Mary Creed, Kristy Vaughan, Sara Taylor, Jennifer Murphy, and Eliza Sgherza are employees of Duke Clinical Research Institute (DCRI), which received financial support in the management of this study.
Disclosures
W.B., F.K., P.C., and S.R. are full-time employees and stock shareholders of Pfizer. At the time of study conduct, J.O. was a full-time employee and shock shareholder of Pfizer. S.C., S.B., and Y.L. are employees of Duke University/Duke Clinical Research Institute.