
Abstract
Objectives:
Serotonin toxicity is a state of central nervous system (CNS) excitation classically featuring altered mental status, neuromuscular excitation, and autonomic instability. While retrospective studies and reviews have characterized serotonin toxicity in adults, there have been no systematic reviews of serotonin toxicity in pediatric populations. The goal of this review was to use published case reports to describe serotonin toxicity in pediatric patients and to consider the impact of age on clinical presentation.
Methods:
A search for case reports of serotonin toxicity in patients younger than 18 years was conducted. Cases were systematically screened for inclusion using serotonin toxicity diagnostic tools, and a meta-analysis of case characteristics was conducted.
Results:
Sixty-six cases of serotonin toxicity in pediatric patients were reviewed. Only 56.1% met diagnostic criteria for serotonin toxicity on all three of the most commonly used diagnostic tools. Antidepressants were found to be the most common trigger of toxicity, implicated in 78.8% of cases. While onset of toxicity was rapid following overdose, toxicity was more likely to be delayed in the setting of medication titration (71.8% vs. 0%, p < 0.0001). Signs of neuromuscular excitation were prevalent, occurring in 92.4% of cases with 81.8% showing the full triad of neuromuscular symptoms, altered mental status, and autonomic instability. The only age-related differences occurred in relation to activation symptoms (more likely to be reported in children than in adolescents) and seizures (less likely to be reported in children than in adolescents or toddlers). Treatment was primarily supportive in nature, although 25.8% of patients received cyproheptadine. In all but one reviewed case, the patient survived.
Conclusions:
The presentation of serotonin toxicity in the pediatric population is similar to that seen in adults. Treatment is supportive with most patients achieving full recovery. Further exploration of the age-related differences in serotonin activity within the CNS is needed.
Introduction
Serotonin toxicity, also known as serotonin syndrome, is classically characterized by the triad of mental status changes, neuromuscular excitation, and autonomic instability. While most commonly associated with antidepressants, serotonin toxicity can occur in the setting of any substance or pathophysiological process that produces increased serotonergic activity in the central nervous system (CNS) (Sternbach 1991). Much of our understanding of this toxidrome is derived from adult cases; however, serotonin toxicity can occur at any age.
The vasomotor effects of hyperserotonemia were first described in the 1950s in the context of carcinoid tumors and other physiological hyperserotonergic states (Waldenstrom 1958). A case report published in 1959 described an “unusual neurological syndrome associated with hyperserotonemia” characterized by mood lability, autonomic instability, flushing, tremors, ataxia, disturbed speech, and lower extremity hypertonia (Southren et al. 1959). The term “serotonin syndrome” was later coined to describe this cluster of symptoms, and case reports of serotonin syndrome secondary to antidepressant use appeared in the literature in 1982 (Hwang 1979; Insel et al. 1982). Over a decade would pass before the first published report of serotonin syndrome in a pediatric patient (Kaminski et al. 1994). By then, the toxidrome had been well described. In a review, Sternbach (1991) aggregated the first 38 published cases of serotonin syndrome in adults to formulate a diagnostic algorithm now known as the Sternbach Criteria (SC). Revised diagnostic criteria were proposed by Radomski et al. (2000) after review of an additional 28 cases published between 1991 and 1995. No pediatric cases were included in either review.
Dunkley et al. (2003) took a different approach to characterizing serotonin syndrome. Rather than reviewing published case reports, they performed a chart review of all presentations to a toxicology service for serotonin poisoning. To narrow their observations to serotonin effects, they only analyzed patients with selective serotonin reuptake inhibitor (SSRI)-alone overdoses, a total of 73 cases. Analysis of symptoms led the authors to conclude that serotonin toxicity has a heterogeneous presentation and that the term “syndrome” was a misnomer (Dunkley et al. 2003). The authors used their findings to develop a new set of diagnostic decision rules entitled the Hunter Serotonin Toxicity Criteria. The Hunter Criteria (HC) focused on the presence of clonus and/or hyperreflexia, which the authors identified as discriminating neuromuscular features of serotonin toxicity. Unfortunately, Dunkley et al. (2003) did not provide information on the ages of the included patients, although they did report that age had a statistically significant association with the diagnosis of serotonin toxicity (p = 0.004). The direction of this association was not specified.
In the 17 years since the HC were published, consideration of how toxicity presents across age groups has remained relatively unstudied. Pediatric providers diagnosing or treating serotonin toxicity in children and adolescents have had to rely on knowledge derived predominantly from adult patients. As of yet, no systematic review of serotonin toxicity in the pediatric population has been published. Several retrospective cohort and database studies have included pediatric patients, but analyses have combined children and adults together (Graudins et al. 2002; Whyte et al. 2003; Isbister et al. 2004; Van Gorp et al. 2009; Abadie et al. 2015; Cooper et al. 2017; Moss and Hendrickson 2019). There is potential danger in assuming that findings in adult patients can be generalized to pediatrics. First, younger age is associated with increased sensitivity to serotonin, as demonstrated by the age-dependent risk for activation symptoms (Safer and Zito 2006). Age also impacts neuronal maturation and reflex activity. Hyperreflexia and clonus, hallmark symptoms of serotonin toxicity per the HC, can be normal findings in very young children (Haslam 2013). While landmark articles on serotonin syndrome have largely omitted or glossed over the pediatric population, there is knowledge to be gained from the literature review. The vast majority of publications on the topic of serotonin toxicity in children are in the form of case reports or case studies, and the aggregation of these cases can provide a source of valuable information.
The aggregation of case reports as a source of evidence is not without controversy. Case reports and case series are often dismissed as biased. They emphasize the rare and atypical, cannot be used to draw epidemiological conclusions, and cannot infer causation (Nissen et al. 2014; Frieden 2017). For these reasons, the publication of case reports has received pushback, whereas randomized controlled trials (RCTs) have been held up as the gold standard of evidence-based medicine. Yet, while RCTs are vital for comparing treatment outcomes, the approach has limitations. RCTs often lack external validity, are expensive and time-consuming, provide limited ability to consider the individual, and are often constrained by ethical or logistic issues. RCTs are generally not large enough or long enough in duration to capture rare but serious adverse treatment outcomes such as serotonin toxicity (Frieden 2017). Therefore, while RCTs serve an important role in advancing evidence-based medicine, they cannot be the sole source of medical knowledge.
Case reports differ from RCTs and large observational studies in their ability to provide detailed and contextualized information about an event or illness. They are rich with minutia typically omitted from large studies and thus can capture disease presentation, diagnosis, treatment course, and response to interventions (Jackson et al. 2014). They are inexpensive and often serve as the first line of evidence for a new diagnosis, treatment modality, or adverse outcome (Nakamura et al. 2014). Case reports have played a sentinel role in identifying and defining new syndromes across specialties, serotonin syndrome being an illustrative example (Nakamura et al. 2014; Nissen et al. 2014). Therefore, while case reports may be imperfect, the knowledge that they contain should not be discarded. The aggregation of cases can enhance our knowledge in areas of medicine that are not easily studied through other means. This is particularly true when the goal is to develop a better understanding of clinical features, treatment, and outcomes in an effort improve diagnosis and treatment rather than to determine treatment superiority (Frieden 2017). Preliminary studies comparing the meta-analysis of case reports to clinical trials have found agreement in outcomes despite concern for potential biases (Sampayo-Cordero et al. 2018, 2019).
The aggregation and meta-analyses of case reports have played an important role in the characterization and diagnostic approach to serotonin toxicity over the past three decades (Sternbach 1991; Radomski et al. 2000; Werneke et al. 2016). Adding pediatric cases to this foundational understanding will help expand this knowledge base. The primary goal of this study was to describe the precipitants, clinical manifestations, management, and outcomes of serotonin toxicity in the pediatric population based on published case reports. The secondary aim was to conduct a preliminary examination of age-related differences in the hallmark symptoms of serotonin toxicity (mental status changes, neuromuscular changes, and autonomic instability) with the hypothesis that increased serotonin sensitivity and neuronal immaturity may have an impact on the risk for behavioral disinhibition and hyperreflexia.
Methods
Design
We conducted a systematic review and meta-analysis of cases of serotonin toxicity in children and adolescents described in the literature following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Moher et al. 2009).
Eligibility
Case reports were eligible for inclusion if the following criteria were met: (1) age of the patient was younger than 18 years, (2) there was documented exposure to a serotonergic substance, and (3) the patient met the criteria for serotonin toxicity based on satisfying at least one of three validated diagnostic tools: SC, Radomski Criteria (RC), and/or HC (Supplementary Appendix SA). When determining whether a patient met the criteria for the SC or RC, the criterion that no neuroleptic had been recently started or adjusted (as stipulated in both diagnostic tools) was waived as long as the patient also had at least one sign of neuromuscular excitation (hyperreflexia, clonus, or myoclonus) to help distinguish from neuroleptic malignant syndrome (NMS) (which is more likely to have severe rigidity producing bradykinesia and hyporeflexia) (Tormoehlen and Rusyniak 2018). The criterion that cases satisfy a diagnostic tool was applied in an effort to minimize diagnostic and/or confirmation biases.
Search strategy
We performed a search using the terms “serotonin toxicity” and “serotonin syndrome” in the databases PubMed, Embase, and PsycInfo. We applied the following filters: children and adolescents (0–18 years) and English language. The most recent search was conducted on August 29, 2020. We also examined the references of reviewed articles to identify any case reports that may have been missed in the database searches.
Study selection
Search results were initially screened by the lead author to identify those articles or abstracts containing descriptions of pediatric cases. All identified cases were reviewed separately by two authors (the lead author and one additional author) to determine eligibility and gather data. Any disagreements between authors were resolved by group consensus.
Data collection
Data collected from case reports included patient age, gender, presenting symptoms, premorbid diagnoses, drug exposures, nature of exposure (i.e., as prescribed, overdose, accidental ingestion, or in utero exposure), time to symptom onset (defined as time from drug exposure or most recent dose change until emergence of first symptoms or presentation to the emergency department), treatment setting, treatment modalities, outcomes, and time to symptom resolution (defined as time from symptom onset until complete resolution of symptoms or discharge from the hospital if the former was not specified). For the purpose of the study, the terminology used in case reports to describe symptoms was assumed to be accurate unless there was clear evidence of discrepancy between the term and the description of the symptom. An example of such discrepancy occurred in one case series where authors used the descriptive phrase “sustained myoclonus with bilateral Achilles reflexes,” and group consensus was reached to code this as clonus rather than myoclonus based on the context (Rushton and Charlton 2014). The decision was also made to equate nystagmus to ocular clonus since ocular clonus is often defined as “nondirectional nystagmus,” and differentiating these symptoms is challenging in the clinical setting (Isbister et al. 2007).
When collecting data on complications of serotonin toxicity, we used the following cutoffs: we defined leukocytosis as white blood cell count >10,000/μL; acute renal injury as creatinine >1.0 mg/dL; elevated liver enzymes as aspartate aminotransferase and/or alanine aminotransferase >50 U/L; and rhabdomyolysis as creatine kinase (CK) >1000 U/L.
Analysis
Descriptive analyses in the form of counts, percentages, means, medians, and interquartile ranges (IQR) were performed on the data collected from included case reports. Significance was set at p < 0.05. Fisher's exact test was used to compare the likelihood of a case meeting the inclusion criteria if published in abstract form compared with full-length article. Patients included in case reports were grouped according to age: infants and toddlers (0–3 years), children (4–12 years), and adolescents (13–17 years). Pearson's χ 2 or Fisher's exact tests were used to compare categorical variables across age groups in 3 × 2 contingency tables. If a χ 2 or exact test was found to be significant across age groups, then 2 × 2 analysis between each age group was conducted separately, again using Pearson's χ 2 or Fisher's exact test, as appropriate. Cohen's kappa was calculated to evaluate agreement between diagnostic tools.
Results
General characteristics of cases
The search terms identified a total of 309 articles and abstracts. After initial screening, 120 articles and abstracts containing a total of 134 cases were identified for further review (Fig. 1). These cases underwent review by two authors, after which 66 cases met the inclusion criteria and were included in analysis. Cases reported in abstract form were significantly less likely to meet the inclusion criteria compared with those published in full articles (29.2% vs. 53.6%, p = 0.042). A full list of reviewed articles and abstracts can be found in Supplementary Appendix SB.
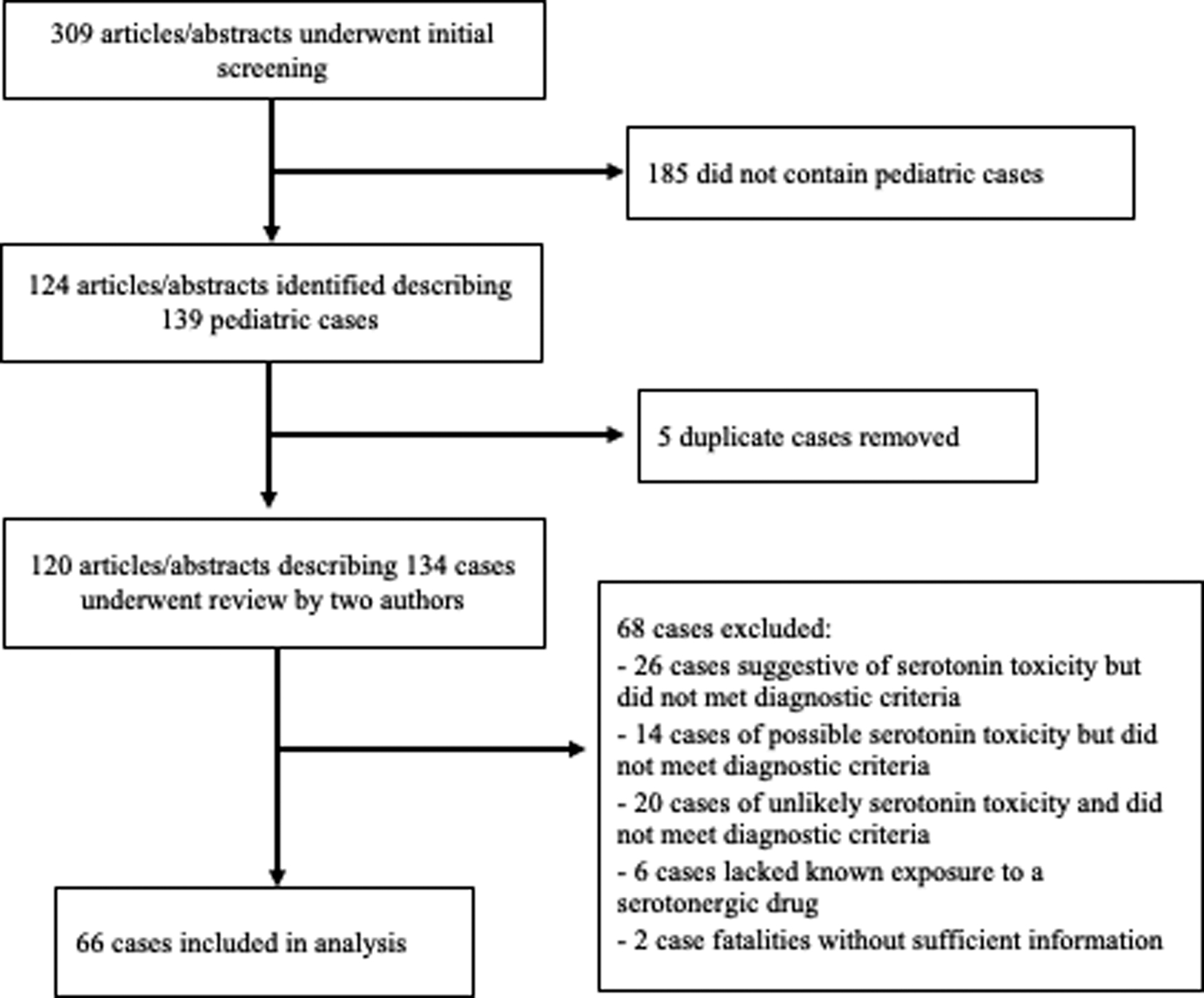
Flow diagram of case screening and selection process. The term “abstract” refers to published abstracts presented at professional conferences. In all instances where cases were published in article format, the full article was obtained for review.
Seven (10.6%) of the included cases were reported in abstract form while the remaining were full journal articles. The earliest case was published in 1994 and the most recent in 2020 (median = 2013). Ten cases were published between 1991 and 2000, 18 between 2001 and 2010, and 38 between 2011 and 2020. Case reports originated from 12 different countries, although the majority (66.2%) were from the United States. Patient characteristics are reported in Table 1. Age range was 0–17 years (median 12; IQR 5–15).
Case Demographics and Mode of Serotonergic Drug Exposure
Bold indicates statistical significance as defined by p < .05.
Calculated using the Freeman–Halton extension of Fisher's exact test.
Diagnostic tools
Of the 66 cases that met the criteria on at least one diagnostic tool, 37 cases (56.1%) met the criteria on all three tools, whereas 13 (19.7%) met the criteria for two, and 16 (24.2%) met the criteria for only one. Overall, 57 patients met the SC, 49 met the RC, and 47 met the HC. Diagnostic agreement between the SC and RC was moderate (81.8%, Cohen's κ = 0.44 [95% confidence interval, CI: 0.18–0.69]), while there was only slight agreement between the RC and HC (66.7%, Cohen's κ = 0.16 [95% CI: −0.09 to 0.41]), and no agreement beyond chance between the SC and HC (63.6%, Cohen's κ = −0.05 [95% CI: −0.26 to 0.15]).
Drug exposure
Thirty-nine drugs with serotonergic properties were identified as potential contributors to toxicity in the reported cases (Table 2). Forty cases (60.6%) involved exposure to a single serotonergic drug, 17 (25.8%) involved two serotonergic drugs, and 9 (13.6%) involved three or more. Antidepressants were involved in 78.8% (n = 52) of cases and accounted for 80% of cases where only one serotonergic drug was ingested. Other classes of drugs implicated in single exposure toxicity included cough suppressants (dextromethorphan, n = 2), opioids (tramadol, n = 1), antiemetics (ondansetron, n = 1), mood stabilizers (lamotrigine, n = 1), stimulants (lisdexamfetamine [n = 1], sibutramine [n = 1]), and drugs of abuse (3,4-methylendioxymethamphetamine [MDMA], n = 1).
Serotonergic Drugs Associated with Serotonin Toxicity in Reviewed Cases
Associated with serotonin toxicity in the setting of single-drug exposure taken at prescribed doses.
Associated with serotonin toxicity in the setting of single-drug exposure via overdose/abuse/accidental ingestion.
ADHD, attention-deficit/hyperactivity disorder; MAO, monoamine oxidase; MAOI, MAO inhibitor; MDMA, 3,4-methylendioxymethamphetamine; SNRI, selective norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
Twenty-two patients (33.3%) experienced toxicity while taking medications as prescribed while the remainder either involved in utero exposure (n = 4, 6.1%), accidental ingestion (n = 15, 22.7%), or intentional overdose/abuse/misuse (n = 25, 37.9%). Mode of exposure differed significantly between age groups (p < 0.0001, Table 1). Infants/toddlers more frequently experienced accidental exposure than children (p < 0.0001) and adolescents (p < 0.0001); children were more frequently reported to develop symptoms when taking medication as prescribed than infants/toddlers (p = 0.0002) and adolescents (p = 0.025); and adolescents were more likely to be exposed via overdose or abuse than infants/toddlers (p < 0.0001) and children (p < 0.0001).
In the cases where toxicity occurred while medications were being taken as prescribed, 5 cases (23.7%) developed toxicity from a single serotonergic agent, 11 (50%) from a combination of two agents, and 6 (27.3%) from three or more. Drug combinations can be found in Table 3. Among those with accidental or intentional overdose, 35 (79.5%) involved a single serotonergic agent, 6 (13.6%) involved two agents, and 3 (6.8%) involved three or more agents.
Medication Combinations Associated with Serotonin Toxicity at Prescribed Doses
SSRI, selective serotonin reuptake inhibitor.
Fifteen patients (22.7%) had co-ingestion of at least two different drugs with overlapping toxidromes: serotonergic + neuroleptic (n = 7), serotonergic + anticholinergic (n = 5), and serotonergic + neuroleptic + anticholinergic (n = 3).
Clinical presentation
Time to onset
Symptoms occurred within 24 hours of overdose, medication initiation, or dose change in 44 cases (66.7%), after 24 hours in 15 (22.7%), and was unspecified in 7 (10.6%). Earliest documented onset of symptoms was 30 minutes after ingestion and longest was “months” after most recent medication change. Among those with time to onset reported, 15 (71.4%) of those who developed toxicity under treatment conditions showed symptoms more than 24 hours after the most recent medication change, while all those with overdose or accidental exposure developed symptoms in under 24 hours (p < 0.0001).
Symptoms
Fifty-four cases (81.8%) described the full triad of altered mental status, neuromuscular changes, and autonomic instability, while 5 (7.6%) had only mental status and neuromuscular changes, 5 (7.6%) had only neuromuscular and autonomic symptoms, and 2 (3%) reported only neuromuscular symptoms. Signs of neuromuscular excitation (hyperreflexia, clonus, and/or myoclonus) were reported in 60 cases (90.9%). See Table 4 for frequency of reported symptoms.
Clinical Presentation of Pediatric Patients with Serotonin Toxicity
Bold indicates statistical significance as defined by p < .05.
Hallucinations, incoherent/slurred speech, anxiety, mania/disinhibition, and catatonia symptoms were not reported in any infants or toddlers. These symptom categories were considered nonapplicable in this age group due to developmental factors.
p = 0.022.
p = 0.003.
CK, creatine kinase; GI, gastrointestinal; N/A, not applicable; WBC, white blood cell.
Laboratory findings
Leukocytosis was reported in 15 cases (22.7%). Elevated liver enzymes, metabolic acidosis, and elevated creatinine each occurred in five cases (7.6%). Elevated CK (>200 U/L) was reported in 24 cases (36.4%) with moderate (1000–10,000 U/L) elevation in 9 (13.6%) and severe (>10,000 U/L) elevation in 4 (6.1%). Hyperammonemia was reported in one patient with ornithine transcarbamylase deficiency.
Complications
Rhabdomyolysis occurred in 13 patients (19.7%). Disseminated intravascular coagulation occurred in one patient. Syndrome of inappropriate antidiuretic hormone secretion occurred in two patients (a neonate with co-occurring jaundice and a 12-year-old boy found to have a suprasellar germinoma).
Impact of age on clinical presentation
Symptoms were reported with similar frequency across age groups with two exceptions: activation symptoms (hypomania/disinhibition) and seizures. Specifically, children (4–12 years old) were more likely than adolescents to have activation symptoms (19% vs. 0%, p = 0.022) and were also less likely than both infants (0% vs. 28.6%, p = 0.019) and adolescents (0% vs. 35.5%, p = 0.002) to experience seizures. Children were more likely to have elevated CK than infants (57.1% vs. 21.4%, p = 0.046) but did not meet significance when compared with adolescents (57.1% vs. 29%, p = 0.051). There was a trend toward significance in age-related differences in respiratory distress (71.4% vs. 42.9% vs. 32.3%, p = 0.05), although the difference was only significant when comparing infants with adolescents (71.4% vs. 32.3%, p = 0.023).
Treatment
Setting
Sixty-one patients (92.4%) were managed in the hospital setting with 42 cases (63.6%) specifying admission to the pediatric intensive care unit. Five patients (7.6%) were managed as outpatients.
Interventions
Three patients (4.5%) were treated by discontinuation of serotonergic medications only (all managed in the outpatient setting). Hospital-based interventions included decontamination with activated charcoal, discontinuing medications, administration of intravenous fluids, and use of cooling measures. Intubation was reported in 25 cases (37.9%). Hemodialysis was used in one case. The most common medications administered were benzodiazepines (n = 40, 60.6%), cyproheptadine (n = 17, 25.8%), dexmedetomidine (n = 8, 12.1%), and antiepileptics (n = 4, 6.1%).
Cyproheptadine was administered using different regimens across the 13 cases where dosing information was provided. In three cases, a single dose of cyproheptadine was given (ranging from 1 to 4 mg). In two of these cases, one involving a 3-year-old and the other a 16-year-old, further doses were not given due to rapid clinical improvement (both involved 4 mg doses). In the third case, in which a 1 mg dose was administered to a 13-month-old, additional doses were not given due to lack of clinical response. Four cases described administration of an initial loading dose (4–12 mg), followed by scheduled or as needed doses of a lower strength (ranging 2–8 mg). Six cases used consistent scheduled doses of cyproheptadine (1–8 mg given every 6–8 h) without loading first. Only one case provided weight-based dosing: cyproheptadine 0.25 mg/kg/day divided every 6 hours given to a 23-month-old with clinical improvement over 24 hours.
Outcomes
Survival
The patient recovered in 98.5% (n = 65) of included cases. In all these cases, the patient experienced full recovery except for one adolescent who developed bilateral hippocampal anoxic brain injury with impaired short-term memory after intentional overdose of vilazodone and bupropion. The only reported fatality involved the patient with T-cell acute lymphoblastic leukemia and ornithine transcarbamylase deficiency, who developed severe hyperammonemia after being prescribed fluoxetine during induction chemotherapy.
Time to recovery
The average time to recovery was 4.3 days (range: 1 hour to 17 days; standard deviation 3.9 days). Two outlier cases were removed from analysis of recovery time due to the nonspecific nature of ongoing symptoms reported: a neonate with microcephaly who had hypertonia lasting 6 weeks, and an 8-year-old boy with intellectual disability and attention-deficit/hyperactivity disorder who had lingering behavior problems for 36 weeks. Longer than average recovery times were often reported in patients who experienced treatment complications such as ventilator-associated pneumonia.
Discussion
This aggregation of pediatric case reports expands our understanding of serotonin toxicity across younger age groups. As with adults, serotonin toxicity in children and adolescents is heterogeneous in presentation. Neuromuscular symptoms were present in all included patients from infancy through adolescence. These symptoms were accompanied by high, but not universal, rates of mental status changes and autonomic instability. Some form of neuromuscular excitation (clonus, hyperreflexia, and/or myoclonus) was reported in 90.9% of cases. This is higher than expected based on studies of adults or mixed age groups. Moss and Hendrickson (2019) in their recent review of 1010 cases of serotonin toxicity (70% adults) found that 60% had hyperreflexia/clonus/myoclonus. This could be consistent with our hypothesis that hyperreflexia is more prominent at younger ages, but the risk for selection bias in case reports prevents direct comparison between the studies. Within the reviewed pediatric cases, there was a trend toward more reported hyperreflexia in infants and toddlers compared with children and adolescents, but the difference did not reach statistical significance. The reviewed cases supported our hypothesis that younger age is associated with increased risk for activation symptoms (hypomania/disinhibition), although in general these symptoms were not commonly reported. This may reflect reporting practices rather than true incidence as many authors used the term “altered mental status” without detailing specific mental status findings.
Our findings suggest that respiratory distress may be especially characteristic of infants experiencing serotonin toxicity. This is consistent with a retrospective chart review that found antidepressant-exposed neonates were 2.5 times more likely to experience tachypnea than a nonexposed cohort (Boucher et al. 2008). The association between neonatal respiratory distress and antidepressant exposure is postulated to result from serotonin's control over ventilatory pathways (Taylor et al. 2005). The immaturity of the neonatal nervous system may exacerbate serotonin's effects on the respiratory system.
Seizures occurred in one-third of toddlers and adolescents, but in none of the cases in the 4- to 12-year-old age group. The absence of seizures in the child group can be explained as a matter of dose, as seizures occurred exclusively in the setting of overdose or accidental ingestion. Overdoses occurred most frequently in adolescent patients while accidental ingestions occurred most frequently in infants/toddlers.
This study has several important limitations. Case reports are at high risk for both selection bias (selection of rare or unusual cases) and publication bias (preference for cases with positive findings). Selection bias is of particular concern in this review and can impact generalizability of case report findings. Mild cases or those considered “classic” presentations are less likely to be published, resulting in potentially skewed findings. The aggregation of cases can help reduce the impact of selection bias by mitigating the impact of outliers, although a larger number of cases would accomplish this more effectively. The study was further limited in its reliance on the accuracy and thoroughness of the case reports reviewed. Some symptoms may have been omitted due to word count limitations or author style. Furthermore, since our inclusion criteria required that cases meet diagnostic criteria that have not been validated in pediatric populations, it is possible that atypical presentations were unintentionally excluded. With these considerations in mind, frequencies and statistical significance in this study should be interpreted with caution. These findings reflect frequencies across case reports, rather than in the general population. We intentionally kept our statistical analyses simple with the cognizance that attempting to draw too many conclusions from a potentially skewed population would have been inappropriate. Yet despite these anticipated limitations, we feel that this study contributes important descriptive knowledge of serotonin toxicity in children and adolescents.
The incidence of serotonin toxicity in children and adolescents remains unknown. Toxicity is too rare to be picked up in RTCs of antidepressant medications (Locher et al. 2017). A recent study looking at adverse drug reactions in children and adolescents exposed to antidepressants in France between 1985 and 2016 found only 12 cases of serotonin syndrome reported (Barthez et al. 2020). In cohort studies looking at antidepressant overdoses across age groups, the prevalence of serotonin syndrome ranges from 0% to 15%, suggesting that the majority of serotonergic overdoses do not result in significant toxicity (Graudins et al. 2002; Isbister et al. 2004; van Gorp et al. 2009; Cooper et al. 2017). While overall rates are low, there is some evidence that children are more suspectable to serotonin toxicity than adults. A study analyzing SSRI and selective norepinephrine reuptake inhibitor overdoses over a 23-year period (age range 13–86 years) found that the risk for serotonin toxicity decreased for every 10-year increase in age (odds ratio 0.84; 95% CI: 0.63–0.95) (Cooper et al. 2018). Younger age as a risk factor for serotonergic toxicity is poorly understood. Serotonin is thought to play a key role in neurogenesis and plasticity, and animal studies show age-dependent differences in serotonin (5-HT) receptor sensitivity (Shayit et al. 2003). There may be particular windows of increased serotonin sensitivity correlating with developmental stages, but this concept requires further exploration (Olivier et al. 2011).
The mechanism of serotonin toxicity is postulated based on the known functions of serotonin in the nervous system. In the periphery, serotonin is involved in gastrointestinal motility, platelet adhesion, vasoconstriction, and uterine contraction. In the CNS, serotonin is involved in modulation of homeostatic functions (sleep, appetite, breathing, and thermoregulation), nausea, mood, memory, cognition, and behavior (Culbertson et al. 2018). Serotonin also regulates muscular activity through modulation of motoneuron and interneuron excitability in the spinal cord (Sławińska et al. 2014; Ghosh and Pearse 2015). Excessive CNS serotonin activity results in disrupted homeostasis, cognitive changes, and neuromuscular excitation, while overactivity of serotonin in the periphery causes gastrointestinal symptoms and hypertension (due to vasoconstriction). Yet serotonin toxicity does not occur in a predictable manner. There are some cases where toxicity has occurred within 30 minutes of a single dose of an SSRI and other cases where massive overdoses resulted in minimal adverse outcomes (Graudins et al. 2002; Phan et al. 2008). There may be factors intrinsic to individuals such as differences in 5-HT receptor function or monoamine oxidase-A (MAO-A) genotypes, which impart heightened risk for toxicity (Hilli et al. 2009). Synergistic effects of interacting drugs can also increase risk for toxicity, especially when the drugs have differing mechanisms (as with the combination of an MAO inhibitor and a tricyclic antidepressant) (Chan et al. 1998).
Serotonin toxicity can be triggered by any substance or pathophysiological process that increases serotonin activity in the brain. This can occur through direct agonism at 5-HT receptors, increased serotonin synthesis and/or release, decreased serotonin reuptake, or decreased serotonin breakdown (Tormoehlen and Rusyniak 2018). Because antidepressant medications primarily act via these mechanisms, they are commonly implicated in serotonin toxicity. This held true in the current study with antidepressant exposure in 78.8% of the reviewed cases. While drug combinations are thought to impart the greatest risk, antidepressants can cause toxicity on their own and occasionally at relatively low doses. Sertraline, an SSRI, is the most commonly prescribed antidepressant in children and adolescents, which most likely accounts for the high frequency at which it was implicated in toxicity (Lopez-Leon et al. 2018). After SSRIs, the next most frequently implicated antidepressants were vilazodone and bupropion. Bupropion is not traditionally considered a trigger for serotonin toxicity because its mechanism is primarily through norepinephrine and dopamine reuptake inhibition. Even so, a recent study of bupropion overdoses found that 5.9% of patients with single-agent bupropion overdose experienced symptoms of serotonin toxicity (Murray et al. 2020).
A variety of non-antidepressant drugs with serotonergic activity are also capable of triggering serotonin toxicity. The medications reported in the pediatric case reports were similar to those identified in adult studies. The role of psychostimulants is notable in the pediatric population given the prevalent use of these medications in children and adolescents. Drugs of abuse, particularly MDMA and synthetic stimulants, are also associated with serotonin toxicity, as are cannabis and ketamine to a lesser degree (Smischney et al. 2018; Baltz and Le 2020). The mechanisms by which each of these agents increases serotonin activity are beyond the scope of this review, but it should be noted that the mechanisms are highly variable both between and within drug classes. As such, drug combinations can create pharmacodynamic synergism, increasing risk for toxicity. Drug combinations can also lead to toxicity through effects on pharmacokinetics. For example, macrolide antibiotics are thought to trigger toxicity in some patients taking SSRIs due to interference in metabolism or displacement from proteins leading to increased serum drug concentrations (Lee and Lee 1999; Jaber et al. 2006; Misselbrook and Shekhar 2011).
Symptoms of serotonin toxicity are expected to occur when serotonin levels in the synapse are at their peak, which happens within a few hours of medication ingestion (Tormoehlen and Rusyniak 2018). This rapid onset has been found in many cases but is not a universal rule (Sternbach 1991). We found that at least 22.7% of reviewed cases reported onset of symptoms more than 24 hours after a medication initiation or change. Similarly, Werneke et al. (2016) found that symptoms occurred more than 24 hours after the most recent medication change in about 60% of adult cases when medications were being gradually titrated. This would suggest that providers should maintain a level of suspicion for serotonin toxicity throughout treatment course.
The heterogeneous presentation of serotonin toxicity can make diagnosis challenging in many cases, especially when patients were exposed to medications or drugs with effects on multiple neurotransmitters. The differential diagnosis for the triad of mental status changes, neuromuscular excitation, and autonomic instability is broad, especially if there is no obvious temporal link to a serotonergic medication exposure. The differential includes other toxidromes such as NMS and anticholinergic syndrome; withdrawal syndromes such those seen in benzodiazepine, alcohol, or opioid withdrawal; malignant hyperthermia or catatonia; infectious or anti-N-methyl-D-aspartate receptor encephalitis; carcinoid syndrome; and thyrotoxicosis (Tormoehlen and Rusyniak 2018; Francescangeli et al. 2019). Designing better strategies to differentiate and diagnose serotonin toxicity has been a goal since the syndrome was first described in the 1950s. The SC provides the greatest diagnostic flexibility but has been criticized for being overly weighted toward changes in mental status and therefore insufficiently specific (Dunkley et al. 2003). The HC, however, were designed to focus on the most discriminating aspects of serotonin toxicity, but the narrow focus on clonus and hyperreflexia risks missing atypical or severe cases (Werneke et al. 2016). About a quarter of reviewed cases met the criteria of only one diagnostic tool, and there was no agreement between the SC and HC beyond chance. These findings replicate those reported in a meta-analysis of adult cases (Werneke et al. 2016). The lack of agreement between the SC and HC indicates that one set of criteria often picked up the cases that the other criteria missed. The cases in this review demonstrate that the HC may help with detection of milder cases in children and adolescents where neuromuscular symptoms predominate.
The diagnosis of serotonin toxicity in the neonatal population is complicated by the overlapping symptoms of neonatal abstinence syndrome (Convertino et al. 2016). While there has been debate as to whether symptoms in a neonate reflect toxicity versus withdrawal, at least one study demonstrated correlation between the presence of the drug in the infant's serum and scores on a serotonin toxicity scale (Laine et al. 2003). This finding supports the postulation that symptoms are in fact due to toxicity from maternal exposure, although withdrawal should remain on the differential.
Treatment of serotonin toxicity occurred in the hospital setting in the majority of the cases reviewed. Discontinuation of serotonergic medications is key to recovery because symptoms typically improve as serotonin is cleared from the neuronal synapse (Tormoehlen and Rusyniak 2018). Past studies have demonstrated that management of serotonin toxicity is primarily supportive with a focus on hydration, respiratory support, and cooling as indicated. Benzodiazepines can be used to target agitation and neuromuscular symptoms, with the goal of preventing muscle breakdown and mitigating autonomic effects (Radomski et al. 2000). Only about a quarter (26.2%) of patients in the reported cases were given cyproheptadine, a serotonin antagonist.
The role of cyproheptadine in the treatment of serotonin toxicity is controversial. Cyproheptadine is a nonspecific antagonist at 5-HT1A and 5-HT2A receptors and so has been of interest in the treatment of serotonin toxicity since the 1970s (Stewart et al. 1979; Graudins et al. 1998). Findings in individual case reports have been mixed, and there are several reasons why cyproheptadine might not be indicated in the treatment of serotonin toxicity. First, symptoms observed in individual cases of serotonin toxicity may not be solely serotonin mediated (e.g., tachycardia and hypertension in venlafaxine overdose likely involve norepinephrine activity). Second, the symptoms of serotonin toxicity often rapidly resolve without intervention, and cyproheptadine introduces risk for adverse side effects of its own. Nguyen et al. (2019) conducted a retrospective review of cyproheptadine use in the setting of serotonin toxicity in California over an 11-year span and found no significant differences in outcomes or hospitalization rates between those who received cyproheptadine and those who did not. Similar to the findings of this meta-analysis, they reported that cyproheptadine was used in 23.1% of serotonin toxicity cases in their sample.
While death is a possible outcome of serotonin toxicity, it is uncommon (Moss and Hendrickson 2019). Almost all patients in the reviewed cases experienced a full recovery. Signs of improvement were often identified within 24 hours of initial presentation, sometimes within hours. The only pediatric case reviewed that reported fatality in the setting of serotonin toxicity described a patient with an enzyme deficiency leading to hyperammonemia (Lally et al. 2016). There are additional reported fatalities linked to serotonin toxicity in the literature, but these cases were excluded from analysis due to lack of sufficient information to confirm the diagnosis. The fatality rate of serotonin toxicity cannot be determined from case reports alone, but it is reassuring that most reported cases recovered without significant complications.
Conclusions
Serotonin toxicity in children and adolescents is an uncommon but serious complication of serotonergic medication use. Overall, the presentation of serotonin toxicity in the pediatric population is similar to that in adults. Neuromuscular excitation, considered a hallmark of serotonin toxicity across age groups, is reported at particularly high rates in pediatric cases. Mental status changes and autonomic instability are also common, but not pervasive. Toxicity is triggered most frequently by antidepressant medications, but other serotonergic drugs have been implicated either in isolation or in combination. Pediatric providers should be mindful of the risk with psychostimulants, particularly in combination with other serotonergic medications. Treatment is primarily supportive, although cyproheptadine can be considered as an augmenting strategy. Most cases recover fully over the course of a few days.
Large-scale epidemiology studies are needed to understand the incidence of serotonin syndrome across all age groups. Cohort and database studies are helpful starting points for studying incidence and clinical presentation, and studies of this variety focused on the pediatric population are needed. Existing data suggest that younger age may impart greater risk for toxicity. For this reason, it is essential for pediatricians and child psychiatrists to consider serotonin toxicity in patients prescribed serotonergic medications. The more gradual onset of symptoms that is seen in the setting of medication titration and maintenance highlights the need for tools and guidance to assist in early recognition. Better understanding of why some patients develop toxicity while others do not would aid in the safe prescribing of psychotropic medications to children.
Footnotes
Clinical Significance
Toxicity caused by serotonergic medications has been documented since the 1980s, but few studies have focused on clinical presentation and course in the pediatric population. While triggers and clinical symptoms seem to share many core features with adult patients, there may be subtle differences in pediatric manifestations related to increased serotonin sensitivity in the CNS and neuronal immaturity. While serotonin toxicity is uncommon, clinician awareness and monitoring are essential for detecting early signs such as hyperreflexia and clonus. Careful consideration of drug-drug interactions is particularly important when combining medications that may have primary or secondary serotonergic effects.
Disclosures
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA
Supplementary Appendix SB
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.