
Abstract
Objectives:
Antipsychotic prescribing in children and adolescents increased sharply beginning in the 1990s, but recent reports among Medicaid enrollees suggest declining trends. However, few studies have included both commercially and publicly insured patients or focused on trends in new antipsychotic medications in children without documented psychotic disorders or other indicated conditions. The objective of the study was to report trends in new antipsychotic prescribing for pediatric patients (age 3–17 years) in a large children's health care system.
Methods:
Data were abstracted from electronic medical records (January 1, 2013 to December 31, 2017). New antipsychotic medication orders were defined as antipsychotic orders for patients without an order in the 180 days prior. Patients were excluded if the order was initiated in an emergency department or inpatient setting; they were diagnosed with psychotic disorder, mania, autism spectrum disorder, or intellectual disability; or the order was for prochlorperazine. The crude rate of new antipsychotic prescribing is reported quarterly with Poisson 95% confidence intervals in the total sample and by demographic subgroups (child vs. adolescent, female vs. male, public vs. private insurance, and white vs. nonwhite).
Results:
Antipsychotic orders decreased from 54.9 prescriptions per 10,000 person months in the first quarter of 2013 to 34.1 per 10,000 person months in the last quarter of 2017. Rates of antipsychotic prescribing were significantly higher for adolescents compared with children, patients who were commercially insured compared with Medicaid insured, and at most time points for white compared with non-white patients. However, prescribing rates did not differ significantly based on gender.
Conclusions:
Antipsychotic prescribing declined for both commercially and Medicaid-insured children in a pediatric hospital-based system, although white and commercially insured patients were more likely to be prescribed antipsychotics. More attention may be needed for reducing potentially avoidable prescribing of antipsychotics in previously understudied subgroups, such as commercially insured patients.
Clinical Trial Registration Number: NCT03448575.
Introduction
The use of antipsychotic drugs prescribed for children and adolescents increased dramatically starting in 1990 (Cooper et al. 2006; Olfson et al. 2012, 2015), raising concerns among parents, clinicians, advocates, and policymakers because of their high cost, unknown effects on the developing brain, and adverse side effects (Daviss et al. 2016; Galling et al. 2016; Cohen et al. 2017; Minjon et al. 2019). Moreover, prescriptions were frequently prescribed for disruptive behaviors, rather than for documented psychotic disorders or other approved indications, further exacerbating concerns (Cooper et al. 2006; Olfson et al. 2012, 2015; Correll and Blader 2015). Antipsychotic medication use is associated with significant increases in weight and can cause metabolic disorders (Bobo et al. 2012; Nicol et al. 2018). The low rates of weight and metabolic monitoring for pediatric patients prescribed antipsychotics underscored the lack of adequate oversight in use of antipsychotic medications with potential for long-term health consequences, when other, safer, treatment options existed for many patients (De Hert and Detraux 2018; Nicol et al. 2018).
As a result of the growing concern regarding use of antipsychotics in children, a variety of local, state and federal governmental policies and health care pharmaceutical control practices were put into place over the past two decades (Constantine et al. 2012; Barclay et al. 2017; Melvin et al. 2017; Zito et al. 2018). Some evidence suggests that these efforts, which have gained momentum since 2010, may have been associated with modest declines in antipsychotic prescribing (Stein et al. 2014; Crystal et al. 2016; Akincigil et al. 2020; Mackie et al. 2021). However, most studies in the United States have relied on Medicaid claims data, with little to no research on commercially insured children or of all-payer prescribing data on children and adolescents, such as in hospital-based health care settings (Saldana et al. 2014; Spence et al. 2020). Moreover, most studies have examined trends in overall prevalence of antipsychotic prescribing (Edelsohn et al. 2017; Kalverdijk et al. 2017), rather than prescribing among youth who do not have psychotic disorders or other indicated conditions (Olfson et al. 2012), for whom safer alternatives to antipsychotics may be available (e.g., first-line psychosocial care or other medications). Finally, studies to date have largely examined filled prescriptions based on claims data, which may be affected by patient-level factors and may differ from trends based on antipsychotic orders by clinicians (i.e., when prescriptions go unfilled). Thus, the current literature leaves an incomplete picture of the use of antipsychotics in U.S. children and changes over time.
The present study addresses the limitations of prior studies. We report on the trends observed between 2013 and 2017 in antipsychotic prescribing for patients at a large hospital-based pediatric health care system, Nationwide Children's Hospital (NCH). We make use of data on antipsychotic medication orders from electronic medical records (EMRs), which included children and adolescents prescribed antipsychotics, regardless of insurance type or whether patients/families filled prescriptions. NCH was part of a large multisite pragmatic trial, the “Safer Use of Antipsychotics in Youth” (SUAY) study (
Methods
Data collection and setting
NCH is located in Columbus, Ohio with more than 1.5 million outpatient visits and more than 19,000 inpatient admissions per year. NCH provides a full range of preventive and specialty care services at inpatient and outpatient care sites, including inpatient and outpatient behavioral health services. The present study used data recorded in the EMR from January 1, 2013 to December 31, 2017 for all patients who had at least one encounter in two specialty mental health departments—Behavioral Health or Developmental Pediatrics. We report trends through December 2017 to report the baseline trends in antipsychotic prescribing before the SUAY study began. Data from the EMR provided information on patient demographic characteristics (age, gender, race, insurance coverage), diagnoses, and medications ordered, (e.g., whether a first- or second-generation antipsychotic medication was ordered).
The patient population for this study (denominator for rates) included individuals ≥3 and <18 years of age at the time of their encounter (January 1, 2013–December 31, 2017) in the departments of Behavioral Health or Developmental Pediatrics. We excluded individuals with an ICD9/10 diagnosis for a psychotic disorder, mania, autism spectrum disorder, or intellectual disability. The index event for the numerator was a “new” order for an antipsychotic medication, meaning that the patient did not have a previous antipsychotic medication order in the prior 180 days. Patients were excluded from the numerator if the index antipsychotic was ordered in an inpatient, emergency department, or urgent care setting. We also excluded prochlorperazine (Comazol®), which is almost exclusively used to treat nausea. The analyses reported in the present study were reviewed and approved by the Institutional Review Boards at both Kaiser Permanente Washington and Nationwide Children's Hospital. The study was granted a waiver of informed consent.
Measures
Antipsychotic medications
An initial list of first- and second-generation antipsychotic medication names was developed based on the generic drug name and national drug code (NDC) for all antipsychotic medications available on the Mental Health Research Network Github page (MentalHealthResearchNetwork 2020). This list includes all drug names for the selected NDC codes listed in First Data Bank or RxNormAntipsychotic medication orders in the EMR, which were identified based on the generic drug names and medication class groupers. While clinicians enter orders by medication name, these names are converted to unique identification numbers (depending on the particular EMR) and then crosswalked to NDC codes for prescription dispensings at the pharmacy.
Analyses
We report the crude rates of initiation of antipsychotics among pediatric patients meeting eligibility criteria for encounters each quarter within NCH care sites between January 1, 2013 and December 31, 2017. We calculated rates monthly but report the average monthly rates over each quarter due to small numbers of new antipsychotic orders during some months. Smoothing the rates facilitates focusing on the broader trends over time. We also report the Poisson 95% confidence intervals for proportions using the exact method. We report trends separately based on age group (3–11 years, 12–17 years), gender, race (white vs. nonwhite), and insurance status (Commercial vs. Medicaid). For subgroup trends, the numerators and denominators followed the same method outlined above but were limited to only those in the specific demographic group each quarter.
Results
The average eligible patient population size per calendar quarter was 8758 and the average number of antipsychotic medication orders was 41.5 per 10,000 person months. There was an overall declining trend over time in rate of index antipsychotic prescriptions for eligible patients, with a rate of 54.9 prescriptions per 10,000 person months in the first quarter of 2013 and 34.1 per 10,000 person months in the last quarter of 2017 (Fig. 1). Although the rates of antipsychotic prescribing declined for all groups, they were significantly higher at nearly all time points for adolescents compared with children, patients who were commercially insured compared with Medicaid insured, and at most time points for white compared with non-white children and adolescents compared with children (Fig. 2). However, there were no significant differences in rates of antipsychotic prescribing based on gender.

Overall trend over time in rate of antipsychotic medication ordering.
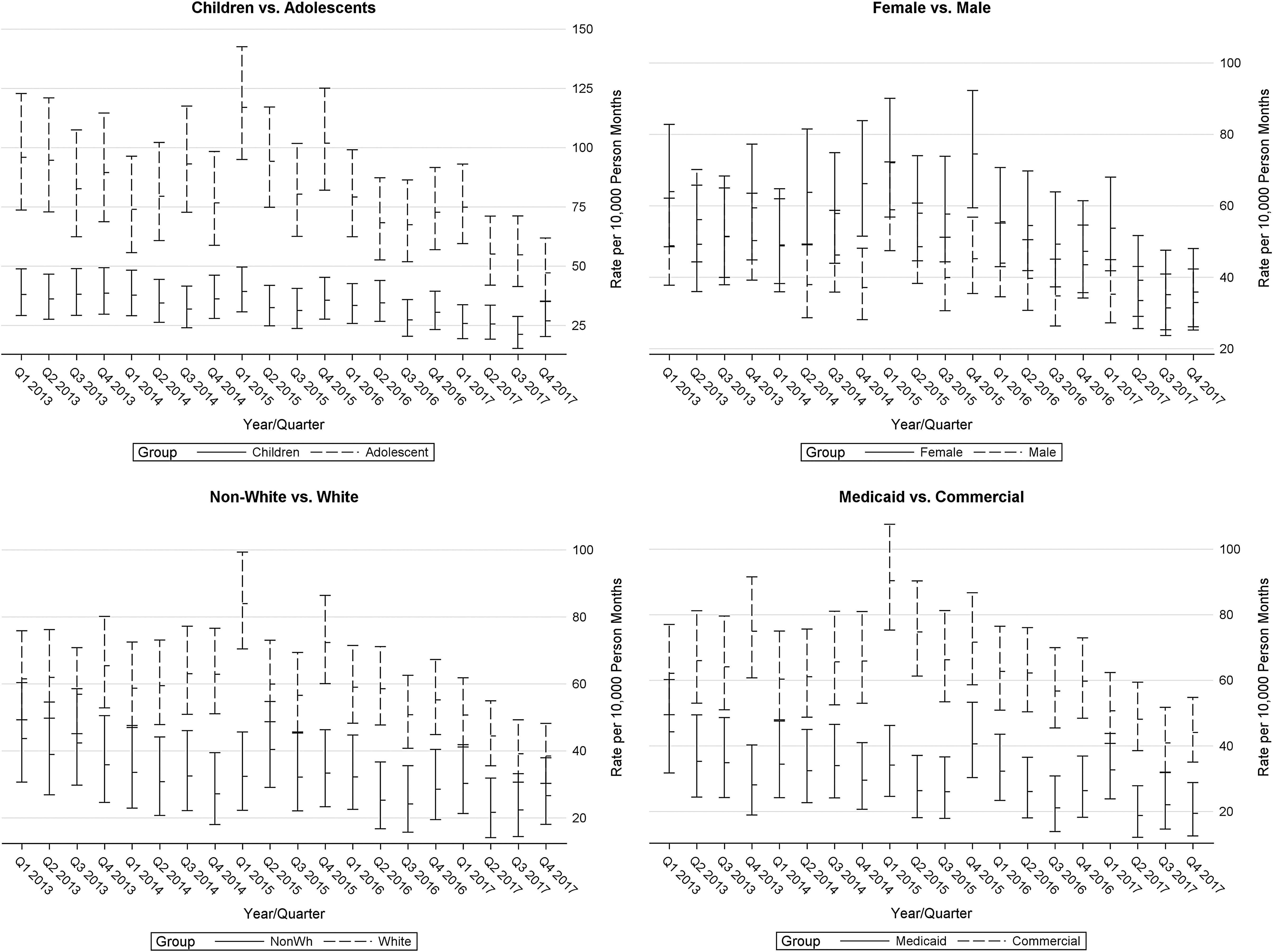
Differences in rates of antipsychotic medication ordering by patient characteristics.
Discussion
This study is the first to report on changes over time in initiation of antipsychotic prescribing in a large hospital-based pediatric health care system and among children and adolescents who did not have documented psychotic disorders, mania associated with bipolar disorder, autism spectrum disorder, or intellectual disability. With concern over potential overuse of antipsychotics in children, it is important to look separately at pediatric patients for whom safer alternatives may be available (e.g., antidepressants, stimulants for disruptive behaviors, or first-line psychosocial therapy). In addition, this is one of few studies to include pediatric patients with multiple types of insurance in the same sample, both those commercially and publicly insured. We found a marked decrease over time in the rates of new antipsychotic prescribing across all subgroups of patients. However, overall prescribing was consistently higher among both commercially insured patients (relative to Medicaid) and White patients (relative to non-White).
The setting and data source of the present study differ from many prior studies, but results appear to confirm recent declining trends in antipsychotic use among children and adolescents (Edelsohn et al. 2017). Although prior studies that relied on prescription fills data identified declining trends, a limitation of these studies was that they could not rule out the possibility that observed trends were the result of changes in patient/family attitudes toward antipsychotic medications, rather than changes in providers' prescribing of antipsychotics. For example, it could indicate that strategies used thus far to target antipsychotic prescribing, many of which are costly and burdensome for prescribers, are not worth the investment. However, the fact that the present study confirmed prior observed trends using data that more immediately captured medication orders offers further evidence that strategies targeting prescribing behaviors are having the intended effects. This has important implications for how we proceed regarding quality improvement of medications for behavioral health conditions as well as other medications that may be of concern, such as opioid analgesics.
There were also some notable differences between the findings of the present study and those of previous studies. We observed lower rates of antipsychotic prescribing for Medicaid relative to commercially insured patients, which differs from most prior research that highlighted the urgent need to reduce antipsychotic prescribing in Medicaid patients, particularly those children in state foster care systems (Leckman-Westin et al. 2018). Lower prescribing rates among Medicaid patients could reflect the greater progress in reducing antipsychotic prescribing through focused Medicaid initiatives, such as prior authorization programs or peer review programs (Akincigil et al. 2020; Mackie et al. 2021). In Ohio, a state-wide behavioral health quality improvement initiative through Ohio's Medicaid program, “Ohio Minds Matter (OMM),” was credited with reducing antipsychotic prescribing for children and adolescents from 2013 through 2015 (Thackeray et al. 2018). However, Medicaid initiatives aimed at reducing antipsychotic prescribing have not been shown to have spillover effects for reducing antipsychotic prescribing among commercially insured patients (Spence et al. 2020; Mackie et al. 2021). This is the first study to compare pediatric prescribing practices based on insurance status within the same large health care system. Moreover, with the present study's use of prescribing data we can rule out the possibility that the observed differences based on insurance result from a lower likelihood of filling prescriptions among caregivers of children enrolled in Medicaid relative to those whose children are enrolled in commercial insurance (Finkelstein et al. 2000; Wang et al. 2006).
Contrary to prior studies, we did not observe a markedly higher rate of antipsychotic prescribing for male compared with female patients or for minority compared with white patients, as has been found in multiple prior studies (Patel et al. 2002, 2005; Lohr et al. 2015; Goddard et al. 2016; Edelsohn et al. 2017; Fontanella et al. 2018; Substance Abuse and Mental Health Services Administration 2019). One important distinction between our study and prior studies is that we excluded patients with a prior medication order for antipsychotics in the previous 180 days or who had specific diagnoses. Thus, it is possible that when comparing the prevalence of antipsychotics use for a broader group of patients, including both incident and prevalent use and youth with other diagnoses, higher rates of use for males and non-white patients would be observed. The differences in prescribing by age, gender, and race in our analysis could be related to parent/guardian preferences for starting new medications versus alternative treatments. Further research is needed to explore the factors parents and guardians consider at the time of treatment initiation.
There are potential limitations to the present study. First, because the data source was limited to the EMR, we do not have information from pharmacy claims regarding whether a prescription was filled and cannot report rates of prescription filling or compare them to prescribing rates. Still, the focus on provider behavior through use of data on antipsychotic prescribing in the EMR is also an advantage of this study. Second, the study is limited to specialty departments within a pediatric hospital-based health care system. Therefore, we do not know whether our findings would generalize to other health systems in other locations. Nevertheless, this is a setting that has been seldom included in the study of antipsychotic medication trends and offers a unique view.
Conclusions
Prescribing of antipsychotics in children and adolescents is decreasing overall in a hospital-based pediatric health care system, but differences in rates are observed between children and adolescents, white versus non-white patients, and Medicaid versus commercially insured patients, but not by gender. These overall trends likely reflect the combined progress of policies, legislation, guidelines, and increased knowledge of risks associated with antipsychotics in children.
Clinical Significance
This study is the first to report trends in antipsychotic medication orders among patients who do not have a documented psychotic disorder, mania, autism spectrum disorder, or intellectual disability. The reported declining trends in prescribing suggest that efforts to reduce prescribing, particularly for pediatric patients for whom there are preferred first-line treatment alternatives, are having an impact on care delivery. However, other findings suggest these gains may be limited to patients in specific subgroups. In particular, a higher rate of new antipsychotic prescribing was observed among patients with commercial insurance, which suggests initiatives to reduce potentially avoidable antipsychotic prescribing, similar to those implemented in state Medicaid programs, may be successful among the commercially insured.
Footnotes
Disclosures
The sponsor (NIMH) provided guidance on the study design but was not involved in data collection, analysis, and interpretation of results, or writing of the report. All authors contributed to the design of the analysis and participated in drafting of the article. There have been no prior presentations of the study findings in any form (poster or abstract).