
Abstract
Objective:
Studies interrogating therapeutics which alter the excitation-inhibition balance in the treatment of autism spectrum disorder (ASD) have reported mixed results on social and behavioral outcomes.
Methods:
The aim of this randomized, double-blind placebo-controlled pilot trial was to evaluate neurocognitive effects of memantine over a 24-week trial. Twenty-three children ages 6–12 years old with ASD were randomized to memantine or placebo. Primary outcomes included measures of apraxia and expressive language with evaluations at midpoint (week 12) and endpoint (week 24). Secondary outcomes included memory and adaptive behavior measures. Exploratory outcomes included changes in overall cognitive functioning and behavior (e.g., Aberrant Behavior Checklist).
Results:
Results suggest that memantine was well-tolerated. Dropout rates were high across groups with only 14 participants completing the 6-month trial. Memantine was not associated with improvements in apraxia and expressive language. Treatment with memantine was associated with improvements in verbal recognition memory as measured by the Narrative Memory-Recognition (NEPSY-II) (F = 5.05, p = .03). In addition, exploratory analyses of changes in Intelligence quotient (IQ) suggest improvements on verbal IQ (d = 1.8).
Conclusions:
Results suggest future studies of memantine in ASD may benefit from shifting treatment targets from social and behavioral outcomes to exploration of effects of memantine on cognition, potentially as an adjunct to learning and educational interventions.
Introduction
Theories related to the pathophysiology of autism spectrum disorder (ASD) commonly point to a genetic etiology leading to a cascade of effects on early brain development, neurotransmission, and neural function. Disrupted balance between excitatory and inhibitory (E:I) neurotransmission during early development has been proposed as one mechanism in the early pathogenesis of ASD. Disrupted E:I transmission is hypothesized to interfere with neural development and function at the synaptic and circuit level (Purcell et al. 2001; Uzunova et al. 2014; Mechler et al. 2017). Gamma-aminobutyric (GABA) and glutamate are critical neurotransmitters in the maintenance of homeostatic control during E:I transmission and are thought to play a particularly important role in these early neural processes.
Studies also point to altered GABA and glutamate levels in individuals with ASD (Lee et al. 2017). For example, early clinical studies reported elevated plasma glutamate levels in individuals with ASD relative to healthy controls (Rolf et al. 1993; Moreno-Fuenmayor et al. 1996; Aldred et al. 2003; Shinohe et al. 2006). Alterations in glutamatergic receptor function in either direction have also been reported in ASD (Lee et al. 2015). Reduced signaling in GABA pathways is also reported in preclinical, electrophysiological, and clinical studies (Chao et al. 2010; Nelson et al. 2015; Green and Garg 2018). In addition, several genes implicated in the pathophysiology of ASD, including neuroligin and neurexin genes, as well as FMR1, the gene associated with fragile X syndrome (FXS), play important roles in synaptic transmission and E:I balance.
Taken together, these data have fueled experimental therapeutic programs interrogating GABA and glutamate modulating compounds in the treatment of ASD, FXS, and related conditions. Open-label and pilot trials of GABA-B agonists, N-methyl-D-aspartic acid (NMDA) inhibitors, and the medication acamprosate, which affects both NMDA and GABA-A neuroreceptors, suggest improvements in caregiver reports of social and behavioral domains (Erickson et al. 2011, 2013, 2014; Bruining et al. 2015; Lee et al. 2015; Lemonnier et al. 2017).
Evidence of memantine's ability to reduce activation of glutamatergic neurotransmission and slow neurocognitive decline in individuals with Alzheimer's disease led to an interest in memantine as a treatment of relevance to ASD. Memantine and its analogue amantadine target the N-methyl-
Until recently, only a handful of memantine studies were reported in individuals with ASD, including retrospective and case series as well as pediatric and adult open-label trials (Owley et al. 2006; Chez et al. 2007; Erickson et al. 2007; Joshi et al. 2016). Dosing ranged from 4 to 20 mg across published trials. Results from an early 8-week pediatric open-label study reported improvements in memory measured by the Children Memory's Scale (CMS) and reduced problem behavior measured by the Aberrant Behavior Checklist (ABC) hyperactivity and lethargy scales (Owley et al. 2006). A recent 12-week open-label trial in 20 adults with ASD found improved self-ratings of ADHD, a replication of results from previous adult ADHD memantine studies (Joshi et al. 2016; Biederman et al. 2017). Findings also suggested improvements on self-report of social impairment on the Social Responsiveness Scale (SRS) and detection of affect in faces on the Diagnostic Assessment of Nonverbal Accuracy-2 (DANVA-2) (Joshi et al. 2016). Safety profiles in open-label studies appear to be favorable overall with some reports of hyperactivity in children (5 of 14 participants) and tachycardia in adults (2 of 20 participants) (Owley et al. 2006; Joshi et al. 2016).
Recently, (Aman et al. 2017) reported on the first randomized-controlled trial (RCT) of memantine in 107 children with ASD, ages 6–12 years, and cognitive abilities in the mildly impaired to normal range. The study evaluated a daily, extended-release (ER) dose of memantine or placebo in a 12-week RCT targeting core symptoms of ASD, including a 48-week open-label extension. Safety findings were similar to open-label studies suggesting mild-to-moderate treatment-emergent adverse events (AEs). Irritability and aggression were the most commonly reported AEs in the memantine group (irritability: 6.7% memantine, 3.3% placebo; aggression: 6.7% memantine, 4.9% placebo). There were no group differences in measures of core ASD symptoms (SRS, primary endpoint), pragmatic communication skills (Children's Communication Checklist [CCC], secondary endpoint), or clinician rating scales of core ASD symptoms (proprietary study-specific measure, secondary endpoint). Both groups had improved clinician ratings of core ASD symptoms in the open-label extension. Overall, results support a relatively safe clinical profile in memantine ER with limited findings of improvements in social communication or behavioral domains.
Another report from the same investigative group reported on a series of trials of memantine ER in ASD: (1) a 50-week open-label, lead-in trial to identify responders; (2) a 12-week randomized, double-blind, placebo-controlled RCT; and (3) <48-week open-label extension to the double-blind RCT that was discontinued early (Hardan et al. 2019). Together, the studies enrolled 906 verbal children with ASD across 118 sites worldwide. Core symptoms were measured by caregiver reports on the SRS and CCC-2; behavioral problems were measured by the ABC. Safety and tolerability data were similar to reports in Aman et al. (2017). In the open-label lead-in, ∼75% demonstrated improvements in the SRS total raw score, defined by improvements of 10 points or greater at the endpoint. However, the 12-week double-blind RCT did not indicate a separation between memantine and placebo on the SRS or other efficacy variables. Several common challenges in the conduct of pediatric clinical trials were identified in this series of studies, including a strong placebo response in the double-blind RCT. A possible nocebo effect, that is, a negative expectancy effect following the open-label, lead-in arm, may have also influenced outcomes in this trial.
Collectively, the broad efficacy of memantine on core and associated behavioral symptoms of ASD appears uncertain. The accumulating data suggest that memantine has a relatively safe profile in pediatric populations, but limited efficacy in behavioral domains. Recent studies also highlight several gaps in the evaluation of novel therapeutics in developmental conditions where translational studies suggest cognitive enhancement as putative targets rather than core symptom improvement in ASD and other developmental disorders. This study seeks to contribute to the understanding of the impact of glutamatergic compounds such as memantine through interrogation of mechanism-specific, neurocognitive effects observed in translational work. To date, the putative cognitive enhancement effects of memantine have been evaluated only in open-label studies and case reports in ASD and related neuropsychiatric disorders. Toward this effort, we report on a 24-week randomized, double-blind, placebo-controlled trial focused on memory, language, and motor outcomes in children with ASD. The study follows several safety and efficacy protocol elements outlined in Aman et al. (2017) and Hardan et al. (2019) to facilitate comparison.
Experimental Procedures
Participants
Study participants were recruited from outpatient clinics at two U.S. sites as well as the community in the form of self-referrals responding to fliers and other advertisements. Study subjects were verbal (as defined by meeting the criteria for Autism Diagnostic Observation Schedule [ADOS] module 2 or 3) outpatients ages 6 to 12 years with a primary DSM-IV diagnosis of pervasive developmental disorder (PDD) (i.e., autistic disorder, Asperger's disorder, or PDD-NOS) or ASD as defined by DSM-5. Participants were required to have difficulty with motor skills as per caregiver report during the psychiatric intake interview. In addition, subjects were stable on all nonpharmacologic treatments for 3 months before randomization and stable on up to two concomitant psychotropic medications 30 days before randomization. All participants had a Clinical Global Impressions-Severity (CGI-S) score of 4 (i.e., moderately ill) or greater. Subjects also had to have an ABC—Irritability subscale score of less than 17.
Participants born before 35 weeks of gestation were excluded due to confounding nonspecific effects of prematurity. In addition, patients who were on
Participants were characterized using standard diagnostic assessments for ASD: autism diagnostic observation schedule-generic (ADOS-G) (Lord et al. 1999) and the Autism Diagnostic Interview—Revised (ADI-R, Lord et al. 1994) or Autism Diagnostic Interview Screener (ADI-S).
Design
This study was designed originally as a Phase II, large, multisite, randomized, double-blind, placebo-controlled trial to evaluate memantine's tolerability and primary efficacy on neurocognitive outcomes, including motor planning, speech, and memory in individuals with ASD (n = 144). The original study design and plans were modified following a hold placed by the FDA to collect more toxicity data in the target age groups. Subsequent budgeting and recruitment challenges resulted in the narrowing of the original trial objectives to include a signal finding study conducted at the Rush University Medical Center and the Icahn School of Medicine at Mount Sinai in the United States. Participants (n = 23), ages 6–12, were randomized at a 1:1 ratio to treatment with memantine or placebo by the study pharmacist at the Icahn School of Medicine at Mount Sinai (original coordinating site). Treatment duration was established at 24 weeks based on trial designs of neurocognitive outcomes of memantine in neurodegenerative disorders. All participants and investigators were blind to group assignment until the blind was broken by the study statistician at the end of the study.
Treatment groups
Memantine and placebo were initiated at 3 mg and the dose was titrated up by 3 mg a week to a maximum of dose of 6, 9, or 12 mg depending on weight and tolerability with dose adjustments conducted between biweekly study visits as needed. Maximum daily doses per weight classes are as follows: 20–40 kg (6 mg), 40–60 kg (9 mg), and >60 kg (12 mg) and were informed by FDA submissions from Forest Pharmaceuticals for trials of memantine ER (Aman et al. 2017; Hardan et al. 2019). In the Forest Pharmaceuticals trial, the maximum dose for the highest weight category was 3 mg higher than this evaluation of neurocognitive outcomes. The protocol indicated that study subjects unable to tolerate 6 mg of memantine or placebo would be discontinued from treatment. Study subjects were seen biweekly for the first 12 weeks and then every 4 weeks from week 12 to 24 and evaluated for both tolerability and efficacy. Phone calls were made to assess safety at week 1 and 3 in between clinic in-person visits.
Regulatory approval
The protocol was approved by the FDA (IND #111576) and the institutional review board at each site. Informed consent and assent procedures were conducted before any study procedures were performed.
Safety measures
Safety measures included the Safety Monitoring Uniform Report Form (SMURF; Greenhill et al. 2004) conducted at each in-person visit and phone call to facilitate the assessment of AEs. Routine blood hematology, blood chemistry, liver function, and urinalysis were assessed at baseline, week 12, and week 24. As part of the safety battery, the following was assessed at each in-person visit: height, weight, blood pressure, pulse, and body mass index.
Outcome measures
The FDA-approved protocol for the original multisite trial outlined primary, secondary, and exploratory neurocognitive and functional outcomes. Dual primary outcomes in apraxia and expressive output, and dual secondary outcomes in memory and adaptive behavior domains were collected at baseline, week 12, and week 24. Measures of intelligence, maladaptive behavior, motor proficiency, social impairment, oromotor apraxia, and sensory behaviors also were collected as exploratory outcomes. Outcome measures are described in detail below.
Primary: Apraxia and expressive speech/language
Apraxia subtests from the Narrative Memory-Recognition (NEPSY-II) included Imitating Hand Posture (IHP), Manual Motor Sequences (MMS), and Oromotor Sequences (OS) (A Developmental NEuroPSYchological Assessment; Pearson; Korkmanet al. 2007). Measures of expressive output included the NEPSY-II Repetition of Nonsense Words (RNW) subtest and the Expressive Vocabulary Test, Second Edition (EVT-2; Williams 2007).
Secondary: Memory and adaptive behavior
Secondary outcome measures included the NEPSY-II Memory for Design and Narrative Memory subtests, the Stanford-Binet-5 Nonverbal Working Memory subtest (Roid 2003), and the Vineland Adaptive Behavior Scale-2 (Vineland-II) to assess adaptive functioning (Sparrow et al. 2005).
Exploratory
Several exploratory measures were included in the trial: the ABC, Bruininks Oseretsky Test of Motor Proficiency-2, Short Form (BOT-2), Behavior Rating Inventory of Executive Function-Parent Questionnaire (BRIEF; Gioia et al. 2000), the Sensory Profile (SP; Dunn 1999), the Apraxia Profile (Hickman 1997), the SRS (Constantino 2005) and Wechsler Intelligence Scale for Children-IV (WISC-IV; Wechsler 2003) at baseline and the Wechsler Abbreviated Scale of Intelligence(WASI-II) (Wechsler 2011) at week 24. The ABC and BRIEF are reported here to provide metrics of impact on behavioral and EF domains and Intelligence quotient (IQ) measures are included to provide preliminary data on the overall neurocognitive effects.
Data analyses
Analyses were conducted per protocol on the intent-to-treat (ITT) population. Hot deck imputation methods were used on measures with less than 30% missing data across participants. Mixed-model analysis with repeated measures at three intervals (baseline, week 12, week 24) was conducted in SPSS 22 starting with omnibus analyses of primary and secondary outcome domains of apraxia, expressive speech, memory, and adaptive behavior using a multivariate analysis of variance (MANOVA) to adjust for multiple tests of hypotheses. These analyses were followed by individual mixed-effects tests on all measures to better interpret significant multivariate results (see the Outcome Measures section). Raw scores on measures were used in the analysis except for the IQ, Vineland Adaptive Behavior Scales-II, and the BRIEF analyses. The magnitude of the effect was calculated with Cohen's d based on change scores from baseline to week 24 for variables included in the ITT analysis. ITT analyses and imputing for missing data were not conducted on IQ scales as this variable was only collected at two intervals. Descriptive analysis of changes in IQ scores was conducted on 14 of 15 completers with post-treatment IQ data using odds ratios defined by changes in standardized scores of greater than 10 points.
Results
Randomization and baseline characterization
Forty-one participants enrolled in the trial and 23 were randomized to one of the two groups after meeting the eligibility criteria. Fifteen participants completed week 24; eight participants withdrew (Fig. 1). Reasons for withdrawal included time constraints (2), lack of efficacy (2), no contact upon follow-up (1), and adverse reactions, described below (3). The sample was largely male with IQ and adaptive behavior scores in the low average range (Table 1). Self-identified ethnicity indicated a diverse sample including 65% Caucasian (including Hispanic) and 35% black, Asian, and other minority groups. There were no differences between treatment arms at baseline on age, sex, ethnicity, intellectual ability, or efficacy variables (Table 1).
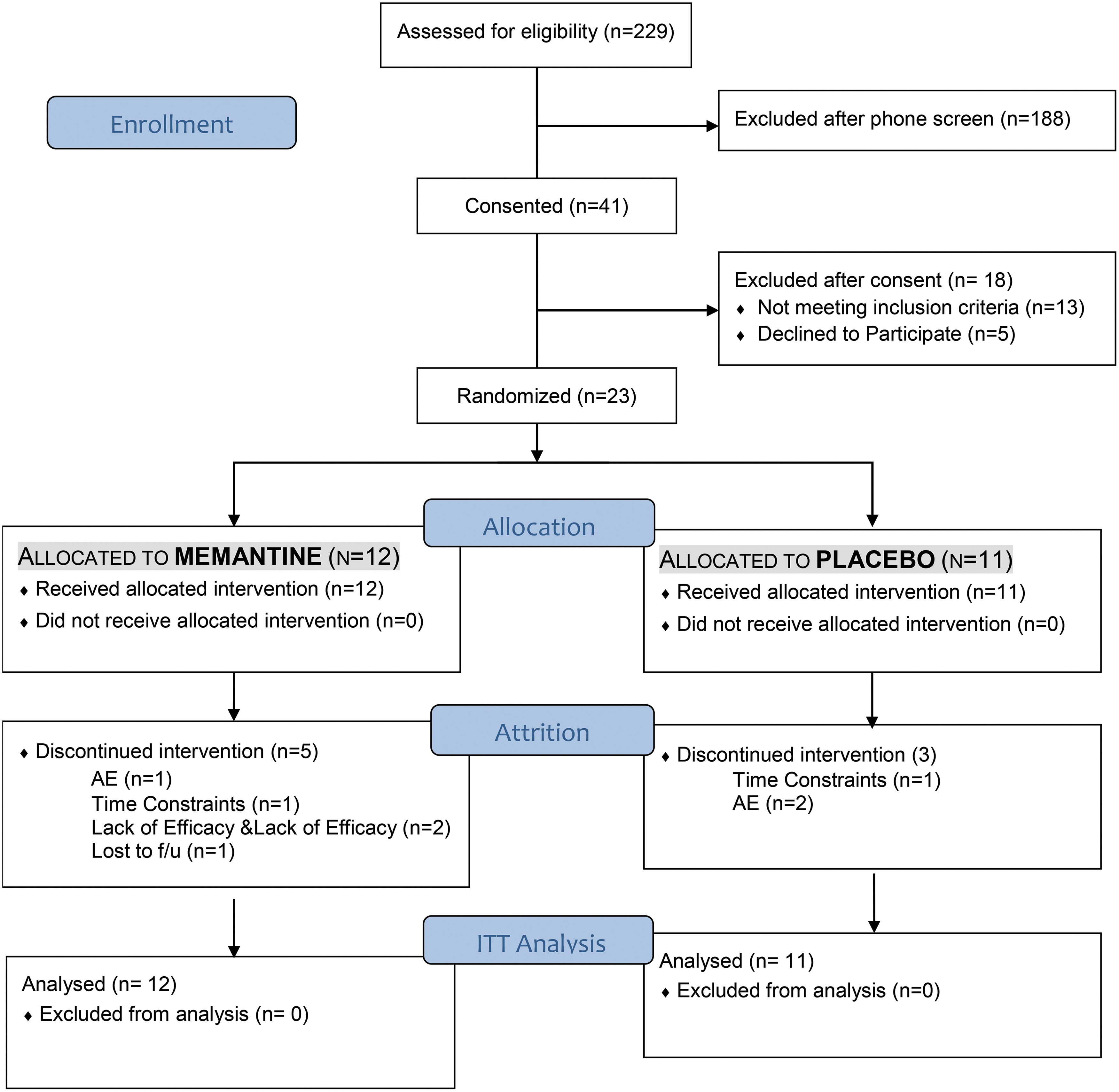
Consolidated Standards of Reporting Trials (CONSORT) diagram.
Participant Characteristics
Missing data in analysis: memantine n = 9; placebo n = 11.
ABC, Aberrant Behavior Checklist; ADOS-G, Autism Diagnostic Observation Schedule-Generic; CGI-Severity, Clinical Global Impressions-Severity; IQ, Intelligence quotient; SD, standard deviation.
Safety and tolerability
Table 2 reports AEs from the SMURF. No serious adverse events were reported in the memantine or placebo treatment arms. All treatment-emergent AEs were mild to moderate with 75% of reported AEs in the mild range, categorized as unrelated, unlikely related, or possibly related to treatment. Gastrointestinal and mood/psychiatric symptoms were the most commonly reported AEs on the SMURF with participants in the memantine condition reporting greater frequency of symptoms in both categories (although not statistically significant in this small sample). Mood/psychiatric symptoms included increased irritability in both groups, angry mood in the placebo group, and depressed mood, compulsive hand washing, and self-injurious behavior in the memantine group only. Two participants in the placebo condition withdrew as a result of treatment-limiting AEs, including diarrhea and emotional lability. One participant in the memantine condition withdrew as a result of a treatment limiting AE, specifically activation (e.g., overly energetic).
Adverse Events Reported on the Safety Monitoring Uniform Report Form
Efficacy measures
Primary outcome measures
There were no significant effects of treatment on apraxia subtests of the NEPSY-II or expressive output as measured by the EVT-2 and RNW (NEPSY-II) (Table 3).
Results of Mixed-Effects Analysis on Primary and Secondary Outcome Measures (Intent-to-Treat Analysis)
IHP, imitating hand posture; MMS, manual motor sequences; NEPSY-II, Narrative Memory-Recognition; OS, Oromotor Sequences; SD, standard deviation.
Secondary outcome measures
There was a nominally statistically significant effect of treatment on the NEPSY-II Narrative Memory-Recognition subtest indicating improvement in verbal recognition memory (Fig. 2). Strong effect sizes were found on this delayed verbal memory measure as well as the immediate verbal memory measure (i.e., NEPSY-II Free & Cued Recall) (Fig. 3). No treatment effects were found on NEPSY-II visual memory scales or the Vineland-II ABC scale.
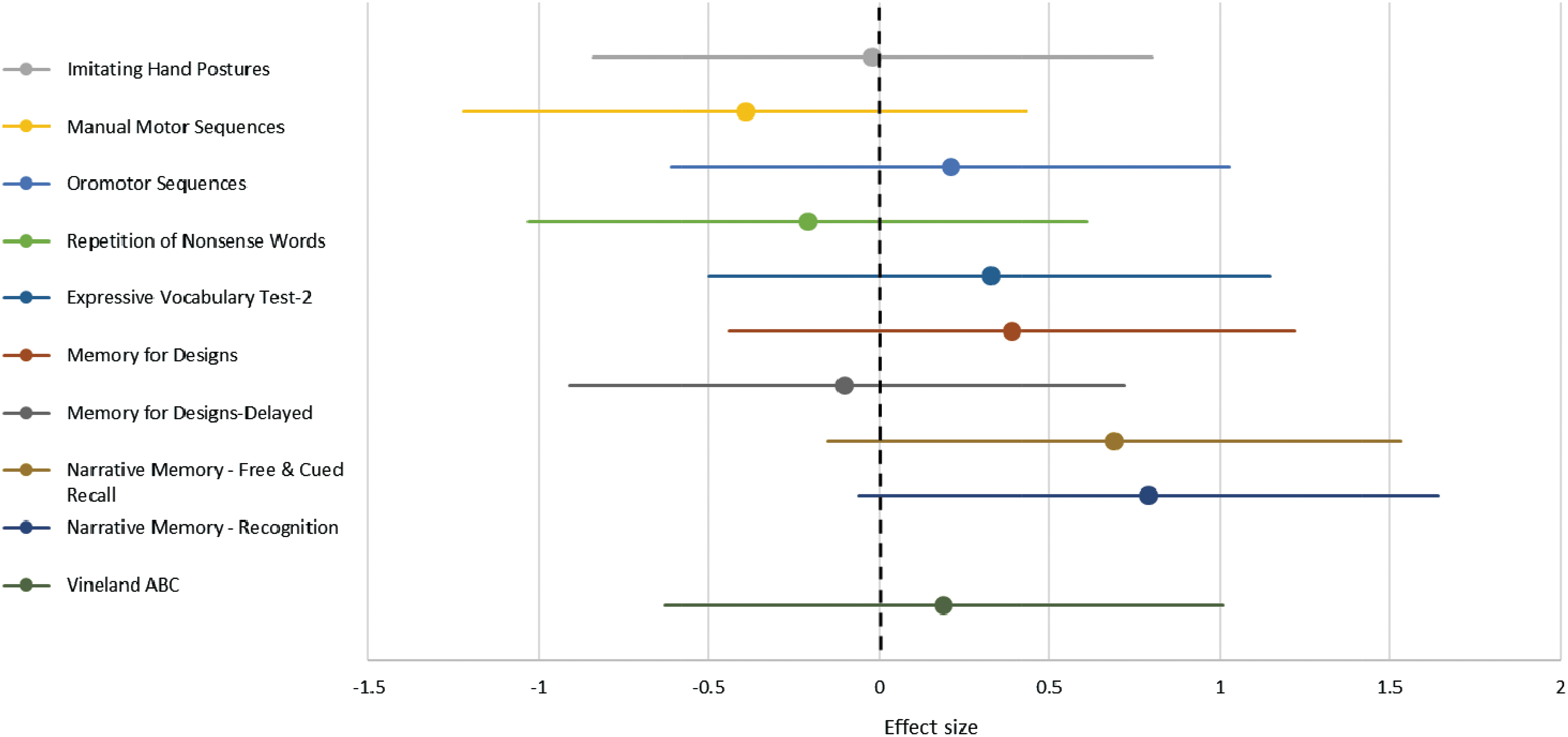
Effect sizes for primary and secondary outcome measures (95% confidence interval).
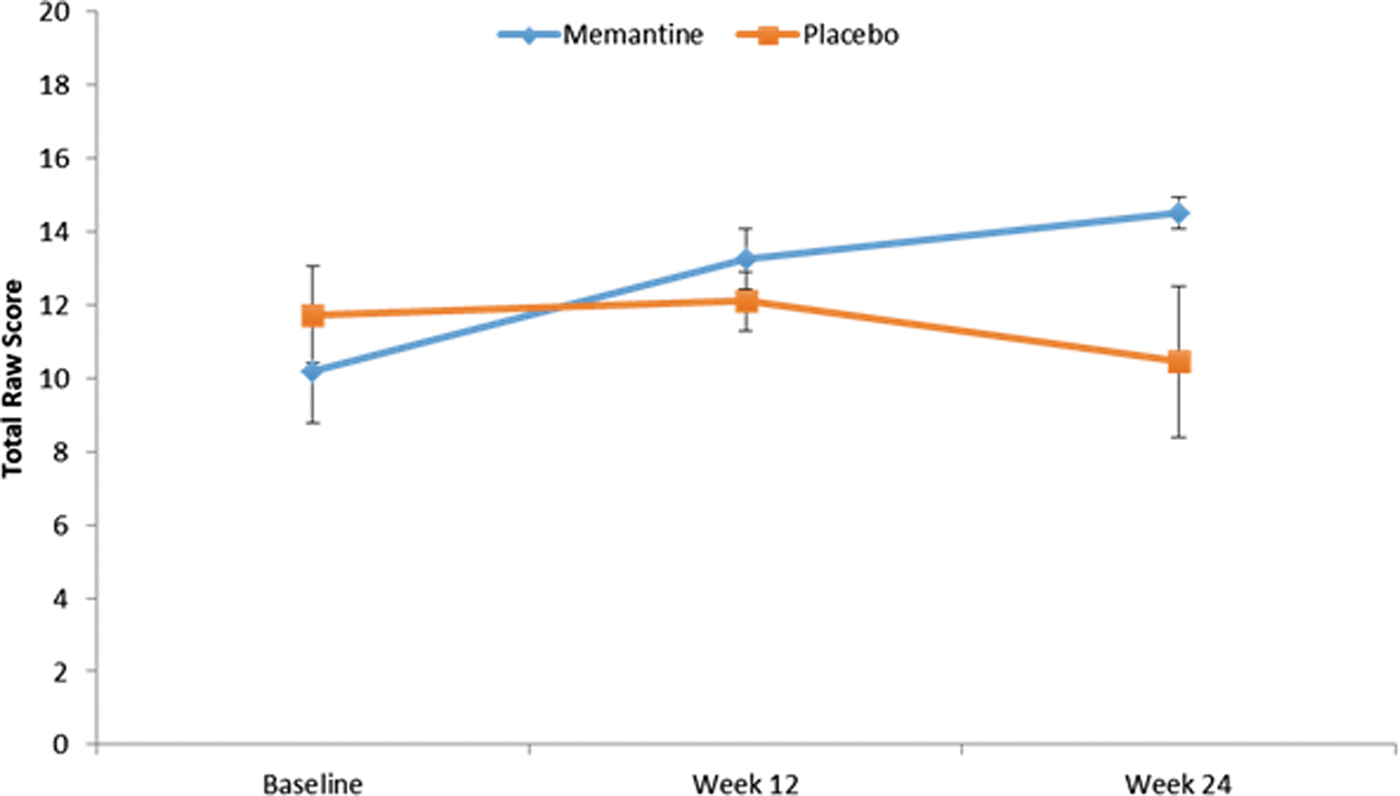
Improvements in secondary outcome: Narrative Memory Recognition Total Score (NEPSY-II).
Exploratory outcome measures
No significant treatment effects were found on ITT analyses on motor and apraxia scores on the BOT-II or Apraxia Profile-II. Behavioral and psychiatric symptoms as measured by the ABC, BRIEF-II, and Sensory Profile-II also did not show improvements or group differences. As indicated, ITT analyses were not possible on exploratory IQ outcomes as these were only collected at two time points to limit test–retest effects on IQ tests. Descriptive analyses were conducted on completers with IQ data at week 24 (n = 14) and are presented in Figure 4. Results indicated baseline differences between conditions, with memantine completers having higher verbal and visual/spatial IQ domain scores. Descriptive analyses indicated that 5/7 participants in the memantine condition gained 10 points or greater from baseline to endpoint on verbal IQ (VIQ) (odd ratio [OR]: 2.5), compared with 0/7 in the placebo condition (OR: 1.9). Group differences in visual/spatial IQ were not evident from descriptive data.
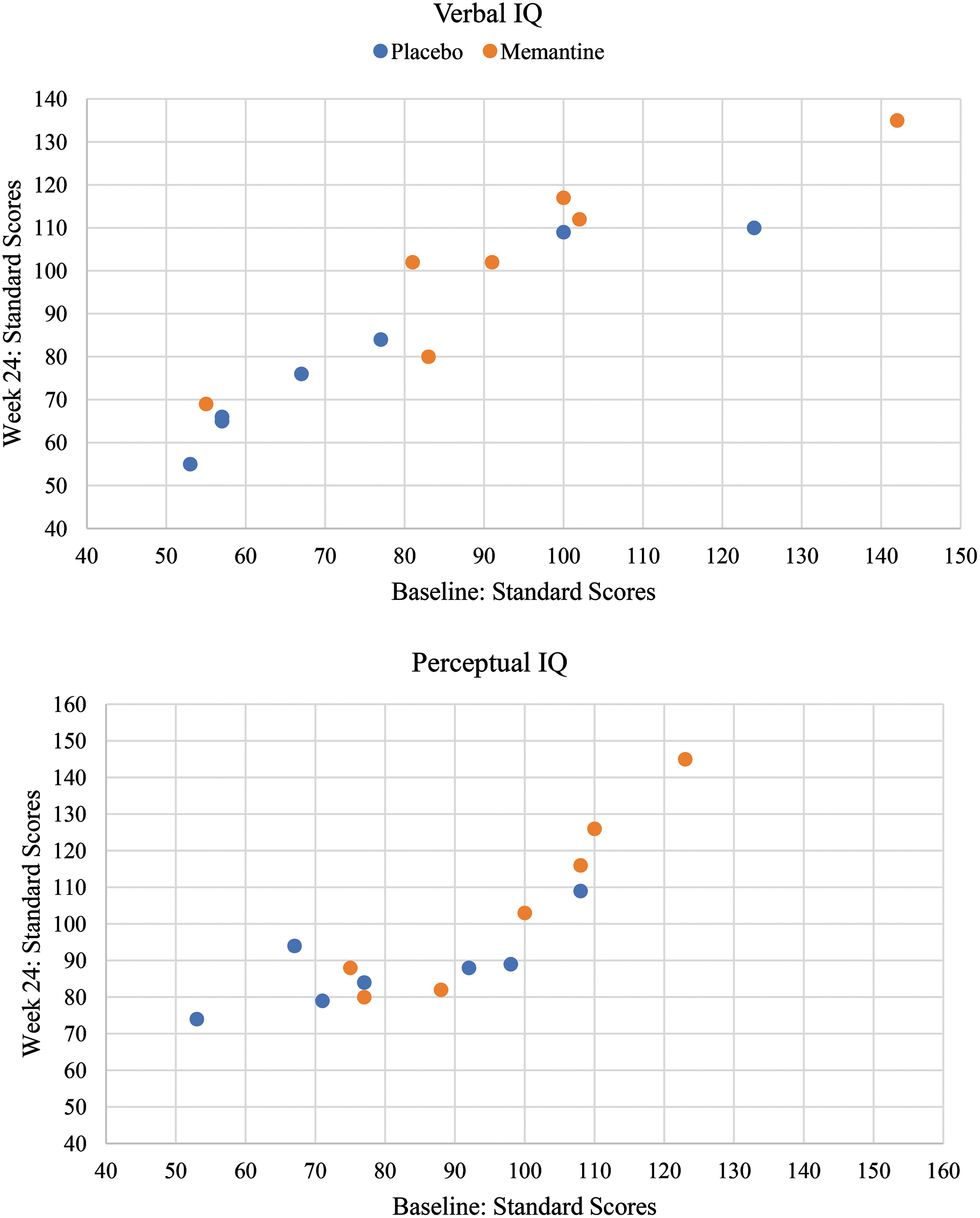
Completer analysis: changes in IQ scores after 6 months. IQ, Intelligence quotient.
Discussion
This is the first randomized placebo-controlled trial evaluating neurocognitive effects of memantine in children with ASD. Results indicate that 24 weeks of memantine treatment was associated with improvements in verbal recognition memory. Results from exploratory analyses show VIQ gains of 10 points or more in 5 of 7 memantine completers at week 24. No participants in the placebo group demonstrated comparable gains in VIQ scores at study completion.
Findings of cognitive growth are noteworthy considering prior open-label findings on the Children's Memory Scale (Owley et al. 2006) in children and spatial working memory (Joshi et al., 2016) in adults with ASD. However, these findings are qualified by the pilot nature of these data, including the lack of improvements on functional outcomes such as the Vineland-II. Furthermore, available data support memantine's neuroprotective role on cognitive decline in neurodegenerative disorders. While one pilot study of adult fragile X premutation carriers found that 12 months of treatment with memantine resulted in improvements on comparable cued verbal memory measure (Yang et al. 2014), the mechanisms by which memantine may improve memory are not well understood. Also, it is notable that both memory impairments in ASD and the potential mechanisms by which memantine may improve memory in ASD are largely unknown. As such, future efforts to understand the role of memantine in autism on attention, consolidation, and/or retrieval processes would be valuable in developing memantine as a cognitive enhancer in neurodevelopmental conditions.
To date, three open-label memantine studies reported reductions in problem behaviors and ASD symptoms (Joshi et al. 2016; Nikvarz et al. 2016; Owley et al. 2016). Nikvarz et al. (2016) suggest that a reduction in ABC and Childhood Autism Rating Scale (CARS) scores was similar with memantine compared with risperidone. Our results do not provide evidence for the therapeutic effects of memantine on behavioral and social outcomes, consistent with recent double-blind, placebo-controlled RCTs (Aman et al. 2017). In addition to testing within a more rigorous design, recent RCTs of memantine included longer treatment intervals (6 months) and a restricted age range (6–12 years). Altogether, results of recent memantine trials suggest that memantine's putative effects lie closer to translational models, which implicate neurocognitive enhancement rather than reduction in the behavioral symptoms of ASD or related neurodevelopmental disorders.
Effects of memantine on verbal memory and VIQ scores in this pilot study suggest verbal abilities as possible treatment targets of this and other glutamatergic medications in ASD. These findings are in the context of several recent studies suggesting a role for memantine monotherapy as well as memantine augmentation in neuropsychiatric conditions (Lu et al. 2018). Targets vary from core symptoms to signals on neurocognitive outcomes in schizophrenia (Zheng et al. 2018) and ADHD (Biederman et al. 2017). Taken together, available results support continued exploration of neurocognitive outcomes when interrogating this class of therapeutic agents in individuals with ASD and related neurodevelopmental conditions. Future studies require the utilization of novel measurement strategies for studies of memantine in younger and minimally verbal populations who would likely stand to benefit most from medications with presumed effects on verbal learning. Also, novel and personalized trial designs will be needed to understand durability, maintenance, and response to treatment.
Interpretation of present findings is cautioned by several design limitations. As indicated, the planned ITT analyses were developed for a multisite clinical trial that was later reduced in scope. The resulting small sample size limited statistical power, and thus, all results should be considered exploratory until replication. Future studies will require corrections for multiple comparisons and covariate analyses to understand potential participant variables influencing completion. For example, a descriptive review of completers indicates a potential influence of IQ on completion rates. Despite no group differences on IQ measures at baseline, the subset of completers in the memantine group had a higher mean IQ than the completers in the placebo arm (Fig. 4). The study had poor retention with ∼35% of the sample completing the 6-month trial. Subsequent research with adequate power will be vital to corroborate verbal memory as a putative neurocognitive treatment target, memantine effects on VIQ, as well as participant variables influencing completion.
Although not statistically significant, descriptive data suggest marginally higher levels of early terminations and behavioral and mood problems in memantine versus placebo groups (Fig. 1 and Table 2). These nonsignificant but potentially elevated rates were also found in Aman et al. (2017) and are notable considering the exclusion criteria in both RCTs for high irritability and problem behaviors, retention rates, and open-label results, suggesting increased activation during memantine treatment (Owley et al. 2006). Further evaluation of tolerability and cost/benefit analysis in clinical care is suggested by available data.
While placebo response and well-known measurement challenges likely influenced results, psychometric issues related to measuring skill growth require additional consideration in this trial. Measurement challenges particular to neurocognitive trial designs include the following: (1) variability of test–retest intervals across measures, (2) limited data on sensitivity to treatment gains, (3) availability of alternate forms, and (4) scarcity of cognitive assessments designed for use in minimally verbal populations. Addressing these measurement challenges will be important to advancing treatment studies of memantine and related compounds. Preliminary findings of associations between improvements in facial and affect recognition and core ASD symptoms in the open-label, adult memantine trial (Joshi et al. 2016) indicate a need to also evaluate associations between neurocognitive, biological, and functional outcomes.
Conclusions
Our findings lend support for the emerging paradigm shift in ASD pharmacotherapies from symptom-focused trials to translational, mechanistic trials targeting the fundamental alteration of developmental learning and cognitive impairments. Specifically, our results suggest that memantine may aid cognition but does not impact behavioral or social impairments in ASD. Berry-Kravis et al. (2017) describe the need to explore innovative designs and measurement strategies in translational neurodevelopmental trials. Studies interrogating cognitive outcomes will require longer treatment intervals and measurement tools designed to detect gains rather than symptom reduction. These promising cognitive pharmacotherapies may also require evaluation within evidence-based behavioral and educational sciences to identify optimal models of care. Recently, several proof-of-concept studies have emerged to evaluate the potentiating effects of novel pharmacotherapies with behavioral treatments, including in memantine (Karahmadi et al. 2018). Other optimization models such as potentiating, synergistic, or potentially antagonist agents to reduce side effects may also be possible and would be of interest for future investigations of cognitive enhancement pharmacotherapies in neurodevelopmental disorders.
Clinical Significance
This pilot study provides an overview of the clinical potential of pharmacotherapies targeting the E/I imbalance in school-aged children with ASD. Results suggest verbal memory as a putative target for memantine's therapeutic effects and a need for further studies of neurocognitive targets and outcomes in pediatric autism trials.
Footnotes
Authors' Contributions
E.A. designed the study, wrote the protocol, and provided regulatory oversight for the trial. L.V.S. designed the neurocognitive outcomes in the protocol, was a site PI, conducted and oversaw training for neurocognitive evaluations, and wrote the first draft of the article. L.V.S., L.F., and E.O. led data cleaning and statistical analysis. S.Y. and M.P. led clinical recruitment at a site and contributed to literature reviews and article preparation and submission. S.L. was a lead clinician at a site, overseeing the safety protocols and training. D.G. was a site-PI. D.G., D.H., and A.K. participated in clinical recruitment, safety, and clinical evaluations at a site. D.G. and A.K. oversaw the lead data management team for network.
Contributors
Sara Soffes, Sofia Silveri Sytniak, Jane Lee, Jessica Kiarashi, and Yousef Bader.
Disclosures
Study medication was provided through an in-kind contribution from Forest Pharmaceuticals. E.A. received consultation fees from Roche and Quadrant, research funding from Roche, in kind supports from AMO Pharma, royalties from APPI and Springer, and editorial honorarium from Wiley. L.V.S. received consultation fees from Roche, royalties from Hogrefe Publications, and holds equity/ownership interest in Argus Cognitive, Inc. A.K. receives research support from AMO Pharma and consults to Ovid Therapeutics, Acadia, and sema4. All other authors declare that they have no conflicts of interest.