
Abstract
Objectives:
To describe the development of a protocol and practical tool for the safe delivery of telemental health (TMH) services to the home. The COVID-19 pandemic forced providers to rapidly transition their outpatient practices to home-based TMH (HB-TMH) without existing protocols or tools to guide them. This experience underscored the need for a standardized privacy and safety tool as HB-TMH is expected to continue as a resource during future crises as well as to become a component of the routine mental health care landscape.
Methods:
The authors represent a subset of the Child and Adolescent Psychiatry Telemental Health Consortium. They met weekly through videoconferencing to review published safety standards of care, existing TMH guidelines for clinic-based and home-based services, and their own institutional protocols. They agreed on three domains foundational to the delivery of HB-TMH: environmental safety, clinical safety, and disposition planning. Through multiple iterations, they agreed upon a final Privacy and Safety Protocol for HB-TMH. The protocol was then operationalized into the Privacy and Safety Assessment Tool (PSA Tool) based on two keystone medical safety constructs: the World Health Organization (WHO) Surgical Safety Checklist/Time-Out and the Checklist Manifesto.
Results:
The PSA Tool comprised four modules: (1) Screening for Safety for HB-TMH; (2) Assessment for Safety During the HB-TMH Initial Visit; (3) End of the Initial Visit and Disposition Planning; and (4) the TMH Time-Out and Reassessment during subsequent visits. A sample workflow guides implementation.
Conclusions:
The Privacy and Safety Protocol and PSA Tool aim to prepare providers for the private and safe delivery of HB-TMH. Its modular format can be adapted to each site's resources. Going forward, the PSA Tool should help to facilitate the integration of HB-TMH into the routine mental health care landscape.
Introduction
The COVID-19 pandemic led to a transformation in health care service delivery and clinical practice across the world. Shelter-in-place restrictions required both providers and patients to stay at home, whenever possible. Many child and adolescent mental health programs rapidly transitioned to the use of telemedicine to deliver services directly to patients' homes. In this article, we adhere to the Center for Medicare and Medicaid Services (CMS) description of telemedicine as remote service delivery that includes both audio and video components in a two-way interactive communication (Center for Medicare and Medicaid Services 2020). When telemedicine is used to deliver mental health care services, the term telemental health (TMH) is generally used (Yellowlees et al. 2010), a convention we follow here.
The increased use of home-based TMH (HB-TMH), in which patients are treated virtually in their homes, necessitated the development of safe approaches to the delivery of mental health services to this nonclinic-based site of service. Most providers were naive to TMH in general and to HB-TMH in particular with no available standardized protocols to guide them in safely providing services to patients in their homes. Luxton et al. (2010, 2012) work with adults has suggested safety precautions to address potential crises that may occur during sessions. Schoenfelder Gonzalez et al. (2019) and Doan et al. (2020) have specifically addressed safety concerns for children and adolescents such as needing to modify usual consent procedures and ensuring the availability of an adult in case safety is compromised. Sharma et al. (2020) have further noted their use of a two-part protocol to assess and minimize risks during HB-TMH. Safety also relates to providers' experience. TMH-naive providers experience stress in transitioning themselves and their patients to HB-TMH (Morgantini et al. 2020; Rosic et al. 2020). Despite these important concerns and suggestions, a specific protocol and tool for delivering TMH services to youth privately and safely in their homes have not yet been available for general distribution.
The objectives of this article are twofold: to describe the development of a protocol for the private and safe delivery of HB-TMH and to present a tool for implementation of the protocol. Although many factors contribute to a successful TMH program, such as developing a virtual therapeutic alliance, ethical practice, professionalism, and cultural humility (Nelson et al. 2013; Gloff et al. 2015; Shore et al. 2018), these topics have been systematically summarized in formal guidelines for telepsychiatric care (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017). Here, the authors focus on the development of a practical tool for assessing privacy and safety as these issues have not been adequately addressed and should contribute to quality improvement for HB-TMH.
Methods
Authors
The authors comprise a subset of the Child and Adolescent Psychiatry Telemental Health Consortium that consists of select faculty from a nonrandom sample of child and adolescent psychiatry programs at major North American (United States and Canada) academic centers that convened to describe their efforts in successfully transitioning to HB-TMH during the COVID-19 pandemic (Folk et al. 2021). Pre-COVID-19, the sites had highly variable experience in TMH. None had major experience with HB-TMH (Folk et al. 2021). Each program transitioned to HB-TMH without existing protocols or tools to guide them. To address safety, some of the programs included existing rating scales, such as screenings for suicide and self-harm, into HB-TMH encounters. Others adapted their crisis clinic protocols to the home environment. One program developed a targeted safety tool (Sharma et al. 2020), and two programs developed comprehensive protocols (Stuart and Colleagues; Doan and Colleagues, unpublished protocols).
Procedures for the development of Privacy and Safety Protocol
The authors met weekly for 1 hour over 10 weeks through videoconferencing to develop a privacy and safety protocol. They shared their individual sites' protocols, discussed their experiences in using these protocols, noted deficiencies in each site's approach, and reviewed the literature on TMH generally and HB-TMH specifically. They agreed upon the relevant material to include from each site, modified by their experiences, and extracted relevant material from published articles. The authors then merged these materials into a preliminary document describing salient aspects needed to establish privacy and safety in HB-TMH. Between weekly meetings, individual authors provided feedback on each other's contributions. Through several rounds of shared iterative group processes, they honed this document into the Privacy and Safety Protocol. Then, they operationalized the Privacy and Safety Protocol into a practical Privacy and Safety Assessment Tool (PSA Tool) by translating core protocol concepts into concrete action items that were organized in a flexible modular format and presented in checklists for implementation by different programs according to their needs, expertise, and resources, as well as for efficient use by providers in clinical practice. Finally, the Privacy and Safety Protocol and PSA Tool were reviewed by representatives from five of the eight consortium sites who made constructive suggestions.
Construction of the PSA Tool
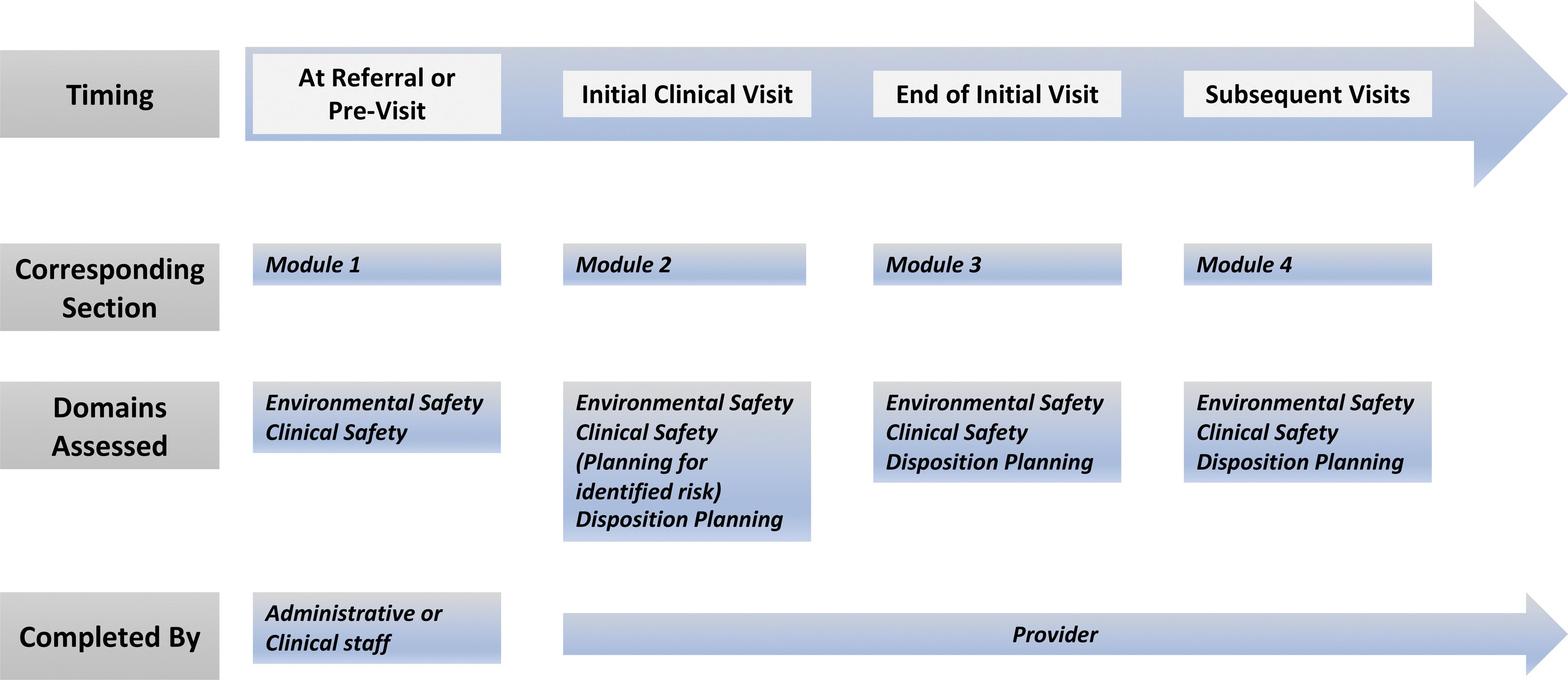
The authors conceptualized safety across three domains discerned from their clinical experience and published TMH standards of care (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017; Rosic et al. 2020): (1) environmental safety; (2) clinical safety; and (3) safety-driven disposition planning. These three domains and their components, parsed by timing of consideration, are summarized in Table 1.
Domains and Relevant Components of the Home-Based-Telemental Health Privacy and Safety Protocol and Documentation Tool
HB-TMH, home-based telemental health.
To translate these domains into a practical tool, the authors adopted concepts from two sources. First is the World Health Organization (WHO) Surgical Safety Checklist/Time-Out (WHO 2009; American College of Surgeons 2017) that engages the clinical team to review a planned clinical procedure with the goal of minimizing errors and identifying individuals' responsibilities. In the variation used here, the “TMH Time-Out,” the provider teams up with the family to authenticate the patient's identity, confirm location of service, identify the responsible adult caregiver or other trusted adult, ensure privacy and safety, and clarify the intended intervention. Second, and related, is the Checklist Manifesto that advocates the use of checklists in routine and unexpected circumstances to ensure adherence to safety steps as outlined by various professional disciplines, including medical practice (Gawande 2011). The checklist approach also offers efficiency for providers and facilitates integration of the PSA Tool into the electronic medical record (EMR).
To ensure that the PSA Tool is relevant across sites, regulatory agencies, providers' needs, and patient populations, the authors also considered the following issues:
Compliance with regulations: ○ Consistent with state/provincial and federal regulations related to age-of-consent and confidentiality. ○ Consistent with professional organizational guidelines. ○ Adaptable to institutional standards.
Ease of implementation:
○ Accessible and compatible with digital health, for example, online completion and/or uploadable to the EMR.
○ Sufficiently brief to be administered efficiently and consistently without excessive burden to providers or patients.
○ Sufficiently clear to be easily interpreted and documented.
Broad applicability across populations:
○ Relevant across geographic boundaries served by the program.
○ Culturally responsive and relevant to and easily understandable by all patients.
○ Applicable to patients' and caregivers' varied levels of digital literacy.
Adaptability to variations in:
○ Demographics (e.g., patient age, socioeconomic status).
○ Clinical conditions (e.g., intellectual disability; caregiver ability to assist in the patient's care).
○ Setting (e.g., treatment centers, schools, and correctional facilities).
○ Modality (e.g., group services).
○ Language and interpreter services.
○ Supervision needs.
○ Technical issues (e.g., screen size, connectivity).
A challenge in developing the PSA Tool was identifying the unique considerations for ensuring safety and response during HB-TMH using established clinical standards for assessment and planning. Certain clinical standards of care are readily applied, such as screening for firearms in the home and educating on their safe storage. This issue must be addressed before any clinical session as part of determining patient appropriateness for HB-TMH, and rechecked as indicated at subsequent clinical sessions as circumstances may change. The PSA Tool adheres to established guidelines for clinical assessments (American Academy of Child and Adolescent Psychiatry 2021a) and safety plans (Stanley and Brown 2012) to ensure consistency with the standards established for in-person care. The PSA Tool does not prescribe specific instruments, but recognizes the need for measurement-based care to determine and document the patient's safety and response to treatment (Fortney et al. 2017; The Joint Commission 2021).
The final PSA Tool, based on the three foundational domains and their components in Table 1, includes three formats:
○ Open text entry (e.g., address, contact persons, individual-specific clinical factors, and contingency plans).
○ Clickable checklists for prior risks and current risks/status during data gathering.
○ Checklist prompts for an action (e.g., completed a contingency plan, reviewed risk assessment at the end of the session).
Results
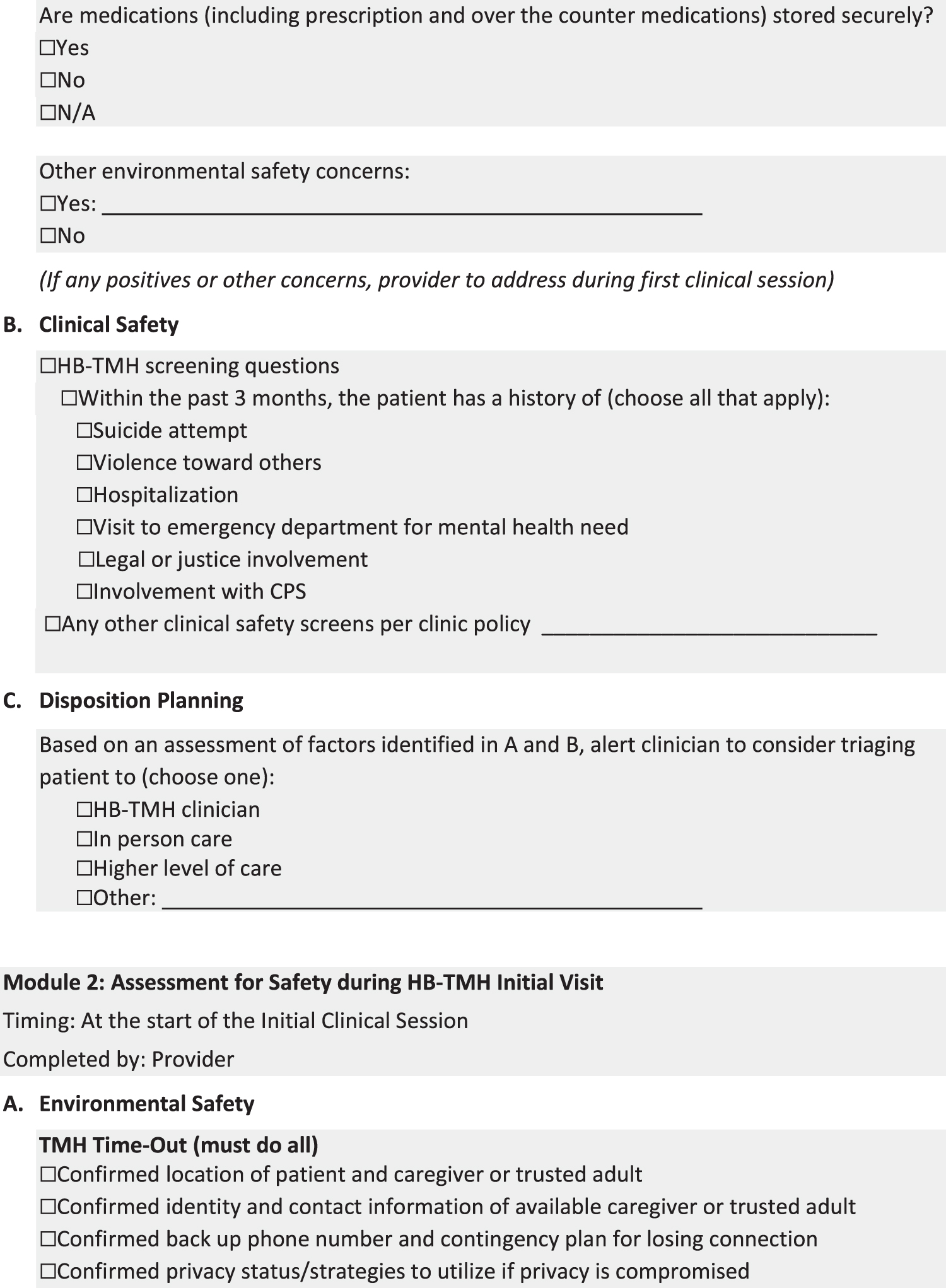
The final PSA Tool is shown in Figure 1 and briefly described here.

Home-based telemental health privacy and safety assessment tool. TMH, telemental health.
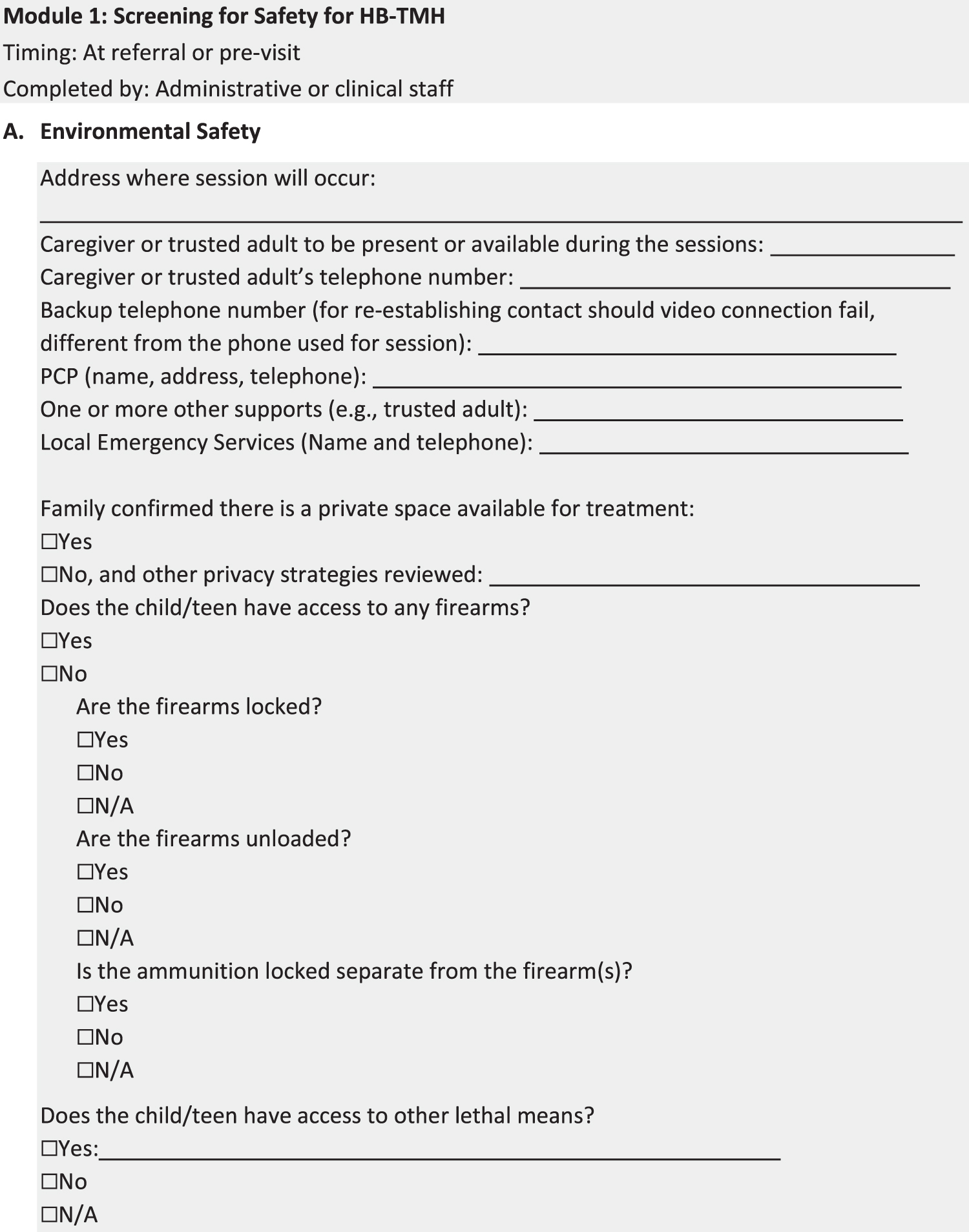


Module 1A, Environmental Safety, consists of concrete questions related to the home and lethal means restriction. The first section uses an open text format to document information specific to the youth and family, such as the address at time of service and relevant contacts. The second portion uses a clickable checklist format with dichotomized responses for ease of administration regarding the environment. Module 1B, Clinical Safety, continues the checklist format. It asks sensitive questions regarding suicidality, violence, psychiatric hospitalizations, or use of emergency rooms, and involvement with juvenile justice or Child Protective Services. Module 1C, Disposition Planning, requires a final disposition by administration support staff, or consultation with clinical staff, regarding appropriateness for HB-TMH and any potential alternative modalities and level of care. The patient may be screened as inappropriate for HB-TMH at this point dependent upon the specific program's guidelines for services. For example, a program that routinely serves homeless youth or families living in abusive situations may have more structured resources to address a potential compromise of safety in session, compared with a training program that serves outpatient populations in medical clinics.
The crucial point is that Module 1 authenticates the patient, determines the patient's appropriateness for HB-TMH, assesses safety of the patient's setting, and lists resources to contact in case of any crises during the subsequent clinical session. The provider will need all of this information before establishing a therapeutic alliance and safely initiating treatment. This approach is consistent with the eligibility screening and registration steps that in-person clinics utilize to match appropriate patents with available services and then to schedule in-person treatment services.
Potential challenges to Module 1 include the need for training of support staff in asking and responding to sensitive questions (Module 1B). As an alternative, some sites utilize a nontreating clinical staff (e.g., nurse, social worker, therapist, psychologist) to collect all of the information in Module 1. This approach may be more clinically sound, but more expensive and limiting when clinical staff resources are scarce. Another potential challenge may be the additional burden on administrative staff to complete this screening and disposition process, which could also incur additional cost to the clinic. Another challenge may be integrating these items into an existing EMR typically used in private practice rather than into hospital-based or large organization-based EMRs.
Potential challenges to Module 2 may include the provider needing to react to new information. Examples include the following: no adult available for the visit; patient located in a nonprivate or unsafe environment; and patient located out of state (Kramer and Luxton 2016). Providers may discount the need for Module 2A, thinking that it has already been done. Finally, providers may perceive the time required to complete Module 2 as detracting from their time available for clinical intervention.
Challenges to Module 3 include the stress to the provider of determining appropriateness. Providers could be burdened by identifying in-person services if the patient is determined not appropriate for HB-TMH. Psychiatrists who are new to TMH may also find burdensome coordinating extra steps such as obtaining rating scales and locating community crisis resources for support in between HB-TMH sessions. Use of patient portals to exchange information can be helpful, but takes additional time to set up and educate families on their use.
The main challenge to Module 4 is checklist fatigue. Providers may omit this step, not appreciating the fluidity of HB-TMH, as patients may change their location or their available caregiver and that caregiver may change location. Also, providers may experience “change blindness” (Rensink 2005). HB-TMH imposes additional expectations on the provider. In addition to the interaction with the patient, providers must attend to alterations in the patient's environment, a site that is not familiar to them. They must also coordinate the technology used during the session, such as checking the medical record, typing the note, or dealing with visual or auditory delays. They may not readily appreciate changes in the patient's affect or ideation that occur in the moment. These additional expectations are fatiguing, leading to “change blindness” regarding the patient's response to interventions.
Workflow
Successful implementation of the PSA Tool depends on workflow. A suggestion is shown in Figure 2. The PSA Tool is designed to be flexible to each program's expertise and resources. The workflow is, therefore, modifiable. Suggested potential variations in implementation of the workflow may include the following:
Workflow for privacy and safety planning tool.
○ Various staff participate in use of the PSA Tool, allowing different sites to utilize the PSA Tool as best fits their expertise, needs, and resources.
○ Identification of staff who would administer sections of the tool:
o Provider may complete the entire form. The upside is consolidating the process to one person and the provider's expertise in discerning the potential need for branch steps. A downside would mean the provider contacts the youth and family before officially assuming care. Providers may incur some liability risk, if they determine that the patient is not appropriate for HB-TMH, but the patient assumes that the provider had established care. Also, screening may not be the optimal approach for the use of valuable, scarce, and expensive clinical staff.
o A division of labor in which administrative support or nontreating clinical staff may collect demographics and contact information, confirm availability of private space or mitigation strategies to maintain privacy, outline expectations of visit, obtain consents, and screen for clinical risk factors. The provider would then review these aspects when conducting the initial clinical interventions session in Module 2. The benefits would include protecting the time of clinical staff for treatment-related activities, flexibility by having various staff share screening activities, and less expense for the clinic. A downside may be having to train support staff to ask sensitive questions related to lethal means restriction or involvement with social services agencies.
o Patient and/or family completes selected sections of the PSA Tool online (e.g., Module 1, location of the youth at time of service, telephone numbers, the caregiver or other trusted adults available at the site of service, and lethal means in the home). A support staff or nontreating clinical staff would then review the information and send it to the provider. Alternatively, the provider could directly review the family's responses. This approach would likely be appropriate to a limited patient population, such as those with sufficient language and digital literacy. If conducted previsit, a concern may be that awaiting a youth's or family's response could delay treatment. If an online method is used, a support staff or nontreating clinician could follow-up via telephone with families who have not completed the PSA Tool online 24 hours before the appointment.
○ Identification of timing in administering the PSA Tool.
o Support or nontreating clinical staff complete all the environmental safety components before any intervention session.
o Provider reviews the environmental safety components before and at the end of the initial intervention session.
o Provider completes clinical safety components at the start of the initial intervention session.
○ Deciding a process for entering results of the completed tool into the EMR.
Discussion
The gradually increasing implementation of HB-TMH in the private and public sectors over the past decade attests to its advantages to and growing acceptance by patients, providers, and health care organizations. Its widespread implementation in the home during the COVID-19 pandemic suggests that HB-TMH will remain a resource during future crises as well as become part of the evolving routine mental health care landscape. A major challenge to this integration is safety. To our knowledge, the development of our Privacy and Safety Protocol and PSA Tool is the first attempt to address safety with a practical instrument.
The PSA Tool adheres to the standards for traditional in-person care (AACAP 2021a) and for clinic-based TMH (American Academy of Child and Adolescent Psychiatry Committee on Telepsychiatry and Committee on Quality Issues 2017) with modifications for delivery to patients' homes. Module 1 most specifically addresses this modification by identifying private space for sessions and documenting community resources in case of a breach of safety. For example, usual clinic staff are not available to assist with safety concerns, such as a patient walking out of the visit, or starting to engage in self-harm. If a parent is not going to be on-site during the session, the provider needs ready access to the caregiver's contact information at the time of service and that of another trusted adult in case the caregiver is not reachable. Potentially, such issues may necessitate a modified consent form. Other items in Module 1 are consistent with an in-person evaluation but are assessed before contact with the provider to determine patient appropriateness for HB-TMH. Modules 2, 3, and 4 entail continuous safety assessment at different points of contact, as safety assessment transitions to the provider. The checklist format is intended to make this process routine, efficient, and not burdensome to the provider. The PSA workflow allows the integration of rating scales to document safety as well as to document progress of treatment. While the PSA Tool does not reference a patient portal, sites may utilize such portals for ease of collecting results of rating scales or other clinical information.
The COVID-19 pandemic necessitated a rapid transition to HB-TMH by providers who had no previous training in TMH, and in the absence of standards for safe delivery to patients' homes (Pinals et al. 2020). There is now a workforce of experienced HB-TMH providers that can help organizations to take the next steps in modifying and implementing the PSA Tool across patient populations, disorders, and acuity (Rienits et al. 2015). These efforts will concomitantly require resource allocation by these organizations for continuous quality assurance in HB-TMH (Halpren-Ruder et al. 2019). For example, “smart” templates may be adapted for HB-TMH services to prompt providers on session standards and documentation that optimize consistency across HB-TMH providers as well as consistency with in-person services. Online care groups may provide remediation conversations to bolster the digital communication infrastructure to improve the technology for HB-TMH. Audits for quality improvement will likely be part of the growing integration into the mental health care landscape if reimbursement is to continue, and increase. Finally, academic programs will need resources to prepare their trainees for their future practices that will likely include HB-TMH and use of the PSA Tool.
Future directions include obtaining empirical evidence on use of the PSA Tool. Ideally, investigators would test the effectiveness of the PSA Tool in identifying, managing, and reducing risk. However, violence and suicidal activity are relatively rare outcomes. Thus, such testing may not be realistic. Rather, descriptive data regarding providers' and patients' input on the feasibility and satisfaction in using the PSA Tool and whether it interferes with the provision of clinical care would yield useful information. Similarly, caregiver, patient, and provider adherence to the initial agreements of providing HB-TMH may comprise a testable hypothesis. Inter-rater reliability on use of the PSA Tool would certainly be testable. On a more practical level, future work may also test whether an online version of Module 1, which patients complete before contact with staff, produces completion of Module 1's items comparable with item completion in the current form. An abbreviated version may also reduce providers' burden and could be tested. Finally, a toolkit specific to HB-TMH, similar to the general telepsychiatry toolkit (AACAP 2020b), will assist providers in integrating HB-TMH into their practices.
Crises create opportunities and often bring lasting societal change. The pandemic highlighted the need to advance TMH practice to home delivery. Continued innovation in HB-TMH will allow psychiatry to mobilize more rapidly during the next crisis (Gates 2018) and to advance mental health service delivery, generally, to a more patient-centered approach. Our Privacy and Safety Protocol and PSA Tool aim to help move these goals forward.
Conclusion
The new Privacy and Safety Protocol and PSA Tool aim to optimize the safe implementation of HB-TMH during future crises as well as during the integration of HB-TMH into the routine mental health care landscape. They are based on three domains foundational to the safety of TMH service delivery. The PSA Tool is structured on the WHO Surgical Safety Checklist/Time-Out and the Checklist Manifesto that have been successfully integrated into other areas of medicine and industry. The modular format allows the PSA Tool to be utilized across age, mental health specialties, disciplines, and resources.
Limitations
The Privacy and Safety Protocol and PSA Tool were developed by a limited group of experienced TMH providers who were not representative of TMH providers generally. In particular, the authors did not include representatives from the private sector who did not have organizational guidance and support as they transitioned to HB-TMH. The process of developing the Protocol and PSA Tool did not follow a formal Delphi or Nominal Group Technique (Jones 1995; ASQE 2021) to ensure that all authors had comparable input to the decision-making in conceptualizing the Privacy and Safety Protocol or constructing the PSA Tool. Review of the final Privacy and Safety Protocol and the PSA Tool was undertaken by only five of the eight Consortium sites.
Clinical Significance
The transition to HB-TMH during the COVID-19 pandemic demonstrated the need for a structured tool to guide the assessment of privacy and safety for the delivery of mental health services through videoconferencing to patients in their homes. The current article describes the Privacy and Safety Assessment Tool (PSA Tool) for children and adolescents. It is based on the World Health Organization Surgical Safety Checklist/Time-Out and the Checklist Manifesto. The modular format can be modified to fit a site's needs and resources. The PSA Tool aims to standardize the assessment of privacy and safety to facilitate quality improvement, while minimizing burden to providers, in delivering TMH services to patients in their homes.
Footnotes
Disclosures
No competing financial interests exist.