
Abstract
Objectives:
The study investigates the risk of obesity for young children prescribed an atypical antipsychotic (AAP) for 6 months or more. AAPs are associated with risk of obesity. They are used in children for a variety of psychiatric conditions and are often prescribed off-label. Long-term risk of obesity in this age group is unknown as most studies are short-term investigations and generally combine younger children with adolescents and adults.
Methods:
A retrospective cohort of children, 10 years old or younger, prescribed either an AAP or selective serotonin reuptake inhibitor (SSRI) for 6 months or more were followed for up to 9.5 years. The primary endpoint was the body–mass index (BMI) reaching the 95th percentile.
Results:
One thousand six hundred fifty-five patients met inclusion criteria. One thousand one hundred eighteen patients were prescribed an AAP and 537 were prescribed an SSRI: 1152 (74.5%) patients were male and mean (standard deviation) age was 7.9 [1.90] years at study entry. Median follow-up was 3.58 years for the AAP cohort and 3.28 years for the SSRI cohort (p = 0.02). After adjusting for baseline demographic variables, BMI, and other concomitantly prescribed medications, children prescribed AAPs for 6 months or longer were twice as likely to become obese compared with children prescribed SSRIs (adjusted hazard ratio [HR] 2.06 [95% confidence interval; CI 1.60–2.66], p < 0.0001). Further stratification by AAP revealed that the obesity risk for patients prescribed aripiprazole was 34% greater than for those prescribed risperidone (adjusted HR 1.34 [95% CI 1.01–1.78], p = 0.0033).
Conclusions:
The risk of obesity for young children prescribed an AAP for 6 months or more is approximately double that of children prescribed an SSRI. The risk of obesity is greater with aripiprazole than risperidone in the first year. Prescribers should consider the risk of obesity when prescribing AAPs and consider alternative treatment modalities in this vulnerable patient population.
Introduction
Second-generation or atypical antipsychotics (AAPs) have been approved for use in children and adolescents by the FDA for the treatment of psychosis, bipolar disorder, Tourette's syndrome, and irritability (aggressive and self-injurious behavior) in the context of autism spectrum disorder (Lee 2018). However, these and other AAPs are often used off-label to treat a variety of psychiatric conditions (Rettew et al. 2015) for which the risks and benefits may not be fully known (Correll and Blader 2015). Edelsohn et al. (2017) found that from 2008 to 2013, among Medicaid-eligible children aged 6–12 years, the most frequent diagnoses in patients treated with an AAP were attention-deficit/hyperactivity disorder (ADHD) (34.6%), disruptive behavior disorders (16.08%), and autism spectrum disorder (18.04%); similar percentages were found in a study by Olfson et al. (2015) reviewing AAP prescriptions from retail pharmacies during the period 2006–2010.
Studies of AAPs in children and adolescents have shown metabolic side effects, including weight gain (Correll et al. 2009; De Hert et al. 2011; Fraguas et al. 2011; Maayan and Correll 2011; Amor 2012; Seida et al. 2012), dyslipidemia (Correll et al. 2009; Seida 2011), impaired glucose tolerance, and increased risk of diabetes mellitus type 2 (Andrade et al. 2011; Galling et al. 2016). Longer duration on AAPs has been associated with increased risk for these side effects (Galling et al. 2016; Baeza et al. 2017). A recent study (Ray et al. 2019) found a small increased risk of premature death when antipsychotics were prescribed off-label to children and adolescents, frequently from cardiovascular or metabolic causes.
Despite these known risks, AAPs are often prescribed to children and adolescents for long durations (McIntyre and Jarell 2008). Only a few studies we are aware of have followed children and adolescents who are on AAPs for more than 2 years (Calarge et al. 2009; Cianchetti and Ledda 2011; Noguera et al. 2013). Additionally, no reports that we are aware of have examined risks separately for young prepubescent children as previous studies have generally grouped young children with adolescents and/or young adults. Young children may be more vulnerable to adverse metabolic side effects from AAPs than older children (Safer 2004; Kowatch et al. 2015; Nicol et al. 2018) and the risk–benefit ratio for AAPs may be less favorable than for adults (Stafford et al. 2015), although this is limited by the small number of studies in this age group.
Among the AAPs, the risk for metabolic side effects varies. For example, in the Second-Generation Antipsychotic Treatment Indications, Effectiveness and Tolerability in Youth trial (Correll et al. 2009), a 12-week nonrandomized study of AAPs in youth aged 4–19 years, weight gain and dyslipidemia were significantly higher for youth prescribed olanzapine and quetiapine compared to youth prescribed risperidone and aripiprazole, in that order. This is similar to what is found in adults (Pillinger et al. 2020), with olanzapine and clozapine on average showing the greatest increases in body–mass index (BMI), glucose, and LDL cholesterol, while aripiprazole, brexpiprazole, cariprazine, lurasidone, and ziprasidone showed the least increases, and other AAPs, including risperidone and quetiapine, have moderate effects on these measures.
Most of the studies in youth that examined the efficacy and/or side effects of AAPs have compared them with one another or with placebo. However, the use of a comparison group in active treatment with a psychotropic medication may reduce the potential inherent obesity risk of the psychiatric illness itself (Puder and Munsch 2010). Children with psychiatric illness have a higher risk for obesity than the general population due, in part, to not only the use of psychotropic medications but also to other factors such as social isolation, poor dietary habits, sedentary lifestyle, socioeconomic status, parental obesity and parental monitoring of the child's eating habits, impulsivity, and emotional dysregulation (Puder and Munsch 2010). One study (Andrade et al. 2011) that also compared patients on AAPs with patients on antidepressants found a higher relative risk for the development of type 2 diabetes mellitus or abnormal glucose laboratory results in the AAP group compared with the antidepressant group, and both groups had higher relative risk than placebo.
The objective of this study was to assess the risk of obesity among children (aged 10 years and under) prescribed AAPs for 6 months or longer compared with children prescribed selective serotonin reuptake inhibitors (SSRIs) for 6 months or longer. We hypothesized that the risk of obesity would be significantly greater in the AAP cohort. As a secondary objective, we also compared obesity risk among children prescribed different AAPs.
Methods
Study design, setting, and population
We conducted a retrospective cohort study at Kaiser Permanente Southern California, a large integrated health system in Southern California, serving ∼4.6 million members. The Kaiser Permanente electronic health record, referred to as Health Connect, contained all relevant pharmacy, demographic, and clinical data for this study and was used to identify the cohort (Xiang et al. 2015). The study population included patients 10 years old or younger who were newly prescribed and dispensed an AAP or SSRI between January 2008 and December 2015. The Generic Product Indicator (GPI) drug classification system was used to identify patients using the medications of interest for the study. The AAP medication cohort included patients orally prescribed risperidone (including paliperidone and iloperidone, which are classified under the same GPI), aripiprazole, ziprasidone, olanzapine, quetiapine, clozapine, asenapine, or lurasidone. The SSRI cohort included patients orally prescribed fluoxetine, fluvoxamine, sertraline, paroxetine, citalopram, or escitalopram.
Patients who were adherent to their AAP or SSRI for 6 months or more were included. To be classified as adherent, patients had to fill two or more prescriptions (30–100-day supplies) of the same AAP or SSRI medication within a 6-month period. Dose changes were not tracked. If patients were prescribed both an AAP and SSRI for more than 6 months, they were included in the cohort for the first prescribed medication class only. If an AAP and SSRI were initially prescribed on the same date, or two AAPs were prescribed on the same date, the patient was excluded. If patients switched from one medication to another in the same medication class within the first 6 months, they would be included only if on the second medication for 6 months or more (e.g., if on risperidone for 3 months and then aripiprazole for 9 months, the data were collected only for the period of time on aripiprazole). Only patients with a standard drug benefit were included so that it could be determined that the medication was filled at the pharmacy, and patients could not have a gap in medication coverage of over 90 days.
The cohort was also limited to patients with 6 months or more of continuous coverage in the health plan (with up to a 45-day gap in coverage) before their first medication was dispensed. Patients who had less than 6 months of continuous membership were excluded as these patients may have previous prescriptions of the medications of interest that were not recorded in our databases. Patients who were obese at baseline were also excluded.
Height and weight are measured routinely at office visits and emergency room or hospital admissions; these data are converted into age–sex-specific BMI percentiles using the 2000 Centers for Disease Control and Prevention normative growth charts (Kuczmarski et al. 2002): underweight is defined as BMI less than the 5th percentile; normal or healthy weight range is 5th percentile to less than 85th percentile; overweight range is 85th percentile to less than 95th percentile; and obesity range is 95th percentile or greater. Baseline BMI was measured using participant's BMI percentile at the time the first psychotropic prescription was dispensed or within the 90 days prior. All patients were followed until the time of the event (BMI reached the 95th percentile), death, end of membership, or the end of the study in September 2017, whichever occurred first. Participants had to have at least one BMI percentile measurement during the follow-up period to be included in the study. Figure 1 outlines the study design and inclusion and exclusion criteria.
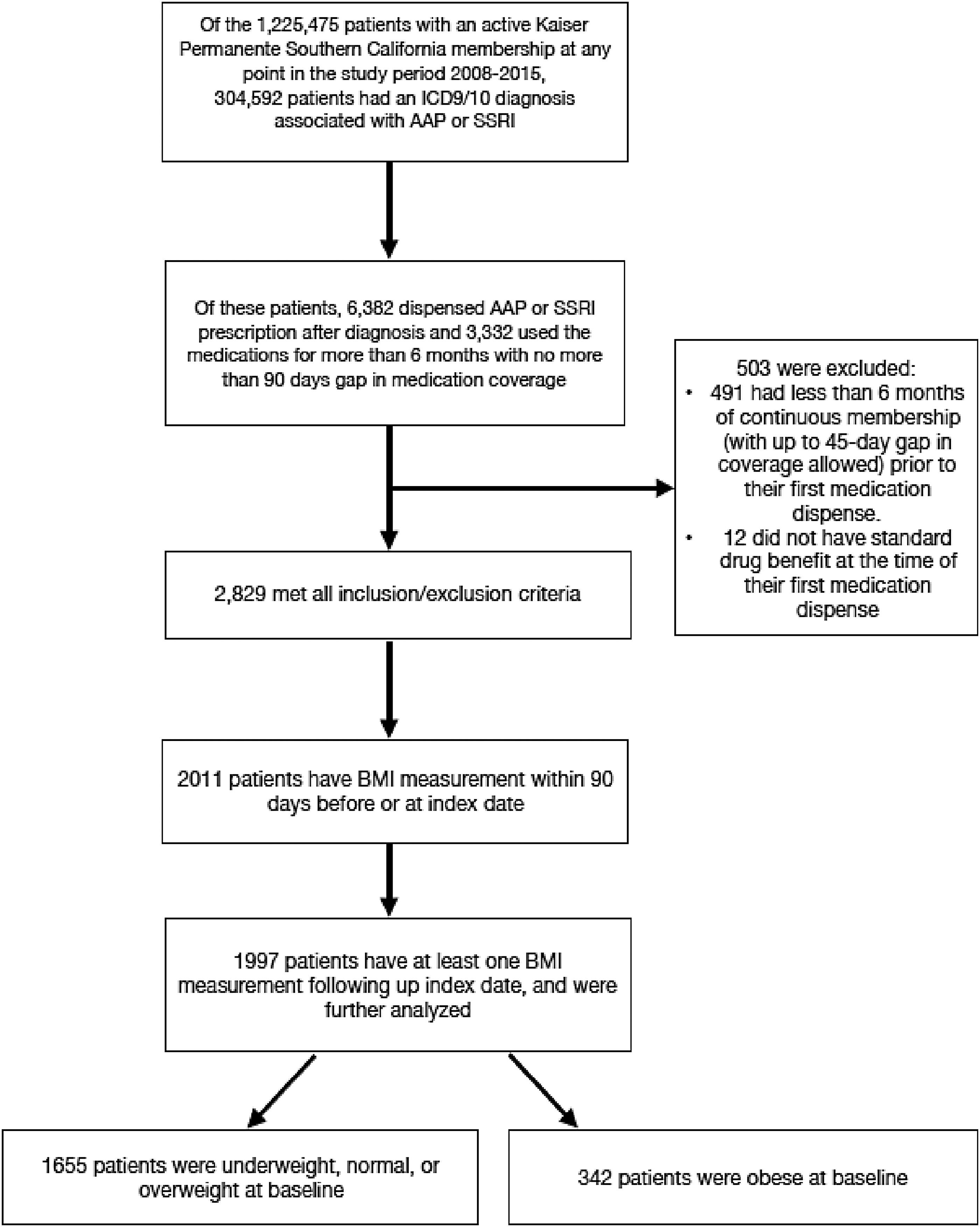
Flow diagram for inclusion and exclusion criteria.
The primary outcome was transition to obesity during the follow-up period (defined as BMI percentile reaching the 95th percentile). The follow-up period started when patients had adhered to their medication for at least 6 months. At the time of the event, patients could have already discontinued the medication.
We compared the risk of transitioning to obesity for patients on AAPs versus SSRIs as well as among the different AAPs.
Data were also collected from medical and pharmacy records to measure initial and final dates of each prescription of psychotropic medication that was dispensed to determine the total length of time (in years) on medication, age at first medication dispense date, sex, race/ethnicity, and geocoded median household income. The Charlson comorbidity index, an approach to classify and statistically account for patients with comorbid diseases that increase their risk of death (Charlson et al. 1987), was calculated based on patients' disease status from the KP Health Connect database and measured at baseline.
Use of other medications known to affect BMI was also tracked, including psychostimulants, norepinephrine reuptake inhibitors, norepinephrine–dopamine reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, tricyclic antidepressants, other antidepressant classes, buspirone, benzodiazepines, lithium, anticonvulsants, beta blockers, benztropine/trihexyphenidyl, and glucose-controlling agents. We assumed concomitant use of these medications if the medication was prescribed at least once during the study period.
Demographic and clinical characteristics were described for the sample overall and separately for patients prescribed AAPs and SSRIs. Means and standard deviations (SDs) and medians and interquartile ranges were calculated for continuous variables, and percentages were calculated for categorical variables. We tested for differences in the AAP and SSRI group characteristics using the Wilcoxon–Mann–Whitney test for continuous variables and chi-square test for categorical variables. Kaplan–Meier curves were generated to compare risks for obesity in children prescribed AAP versus SSRI and for children using specific AAPs given that not all patients remained in the cohort until the end of the data collection period. After collection of data, it was discovered that risperidone and aripiprazole accounted for 95% of all AAPs prescribed in this population, so we shifted focus to comparing only these two AAPs.
A Cox proportional hazards regression model was used to determine hazard ratios (HRs) and 95% confidence intervals (CIs) for obesity in the AAP group compared with the SSRI group. Both crude and adjusted models were estimated. Covariates included in the adjusted model were age at medication start, sex, race/ethnicity, geocoded median household income, Charlson's comorbidity index, and concomitant use of other medications associated with potential BMI change.
All analyses were performed using SAS Enterprise Guide 5.1 (SAS Institute, Cary, NC, USA) and R.
The study protocol was approved by the Institutional Review Board of Kaiser Permanente Southern California.
Results
Figure 1 describes the inclusion/exclusion criteria leading to the final sample. Within the time period, January 2008 to December 2015, there were 6382 patients, 10 years old or younger, who were prescribed an AAP or SSRI. Of those, 3332 patients met initial inclusion criteria and were prescribed the medication for more than 6 months with no more than a 90-day gap in medication coverage for that time period. Four hundred ninety-one patients were excluded for having less than 6 months of continuous insurance coverage before the first medication was dispensed and 12 patients did not have a standard drug benefit at the first medication dispense date. Of the remaining 2829 patients, only 2011 patients had a BMI measurement within 90 days before or at date of first prescription and 1997 patients had at least one BMI measurement following that. Additionally, 342 patients were excluded as they were already obese at baseline, leaving the final sample size of 1655 patients.
The baseline characteristics of the 1655 patients are as follows (Table 1): 1152 (74.5%) patients were male and the mean (SD) age was 7.9 (1.90) years at study entry; 1118 patients were in the AAP group and 537 were in the SSRI group. Among the AAPs, risperidone was prescribed most frequently (81.3%, n = 909), compared with aripiprazole (13.4%, n = 150), quetiapine (3.9%, n = 44), olanzapine (1.2%, n = 13), and ziprasidone (0.2%, n = 2). The SSRI group could not be broken down further as they were all classified under the same GPI code in our dataset.
Baseline Characteristics of the Study Population
AAP, atypical antipsychotic; BMI, body–mass index; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor.
The mean age at first medication dispense date was statistically significantly lower for the AAP group compared with the SSRI group (7.5 years vs. 8.8 years, p < 0.001). Males comprised a significantly higher percentage of those prescribed AAPs compared with SSRIs (74.5% vs. 59.4%, p < 0.001). Racial and ethnic differences were also found to be statistically significant. Among patients on AAPs, 49.6% were White non-Hispanic, while 11% were Black non-Hispanic. By contrast, among patients on SSRIs, 58.1% were White non-Hispanic, while 3.7% were Black non-Hispanic (p < 0.001). The proportion of patients whose addresses were geocoded to neighborhoods with a median household income of $50,000 or below was significantly higher for patients using AAPs compared with SSRIs (29.8% vs. 23.95%, p = 0.002), while the proportion of children whose addresses were geocoded to neighborhoods with a median household income of $100,000 or above was significantly higher for those prescribed SSRIs compared with AAPs (21.9% vs. 14.4%, p = 0.002). The Charlson comorbidity index did not differ at baseline for children using AAPs versus SSRIs (p = 0.67).
The majority of patients were normal weight at baseline (76.9%). The percentage of patients who were overweight at baseline was 16.3% in the AAP group and 17.1% in the SSRI group. There were no statistically significant differences in weight status for the AAP versus SSRI group at baseline (p = 0.89).
The median follow-up duration was significantly different for the two groups: 3.58 years for the AAP cohort and 3.28 years for the SSRI cohort (p = 0.02).
Within 2 years, the probability of becoming obese for the AAP cohort was 23.5% [95% CI 20.9–26] compared with 11.7% for the SSRI cohort [95% CI 8.8–14.4]. Children prescribed AAPs had a significantly higher risk of obesity compared with those prescribed SSRIs (p < 0.0001) (Fig. 2).

Kaplan–Meier curve showing time in years to obesity (BMI reaching the 95th percentile) for the group on AAP or SSRI. p-Value is from the log-rank test. Survival probability refers to patients who remained nonobese. Within 2 years, the probability of becoming obese for the AAP cohort was 23.5% [95% CI 20.9–26] compared with 11.7% for the SSRI cohort [95% CI 8.8–14.4]. Children prescribed AAPs had a significantly higher risk of obesity compared with those prescribed SSRIs (p < 0.0001). AAP, atypical antipsychotic; BMI, body–mass index; CI, confidence interval; SSRI, selective serotonin reuptake inhibitor.
After adjusting for age, sex, race/ethnicity, geocoded median household income, Charlson's comorbidity index, and exposure to other medications known to affect BMI and baseline BMI category, children prescribed AAPs for 6 months or longer were twice as likely to become obese compared with children prescribed SSRIs (adjusted HR 2.06 [95% CI 1.60–2.66], p < 0.001) (Table 3).
Baseline Characteristics of the Children Prescribed Aripiprazole or Risperidone
BMI, body–mass index; SD, standard deviation.
Results from the Cox Proportional Hazards Model
Adjusted risk of obesity with an AAP prescribed for 6 months or more is more than double that with an SSRI prescribed for 6 months or more. Adjusted risk of obesity with aripiprazole prescribed for 6 months or more is 34% higher than with risperidone prescribed for 6 months or more.
Adjusted for age, BMI at baseline, Charlson's comorbidity index, sex, race/ethnicity, median household income, and concomitant medication use.
AAP, atypical antipsychotic; BMI, body–mass index; CI, confidence interval; SSRI, selective serotonin reuptake inhibitor.
Further examination of baseline demographic variables revealed that males were significantly more likely to become obese than females (HR 1.48 [95% CI 1.17–1.86], p < 0.01) in the sample population. There were no significant differences based on neighborhood household income, Charlson's comorbidity index, or ethnicity (except possibly a trend toward significance for those identifying their ethnicity as “Other”) (HR 1.51 [95% CI 0.99–2.28], p = 0.05).
Concomitant medication significantly affected weight gain and was controlled for in the Cox proportional hazards model. Serotonin–norepinephrine reuptake inhibitors, tricyclic antidepressants, other antidepressants, buspirone, benzodiazepines, lithium, anticonvulsants, beta blockers, benztropine/trihexyphenidyl, and glucose-controlling agents were grouped due to low frequency of use and, overall, significantly decreased obesity risk by 43% ([95% CI 29–54], p < 0.01). Comparatively, atomoxetine and bupropion provided a 57% risk reduction in becoming obese ([95% CI 38–70], p < 0.01), and psychostimulants provided the greatest risk reduction in becoming obese, by 65% ([95% CI 57–71], p < 0.01).
Table 2 describes the baseline characteristics of patients prescribed aripiprazole (n = 150) or risperidone (n = 909). Patients prescribed aripiprazole were 72% male, 8.1 years old [95% CI 7.1–9.5], and had a higher proportion of overweight BMI (27.3%) compared with patients prescribed risperidone who were 75.8% male (p = 0.318), 7.3 years old ([95% CI 5.9–8.9 years], p < 0.001), and had a lower proportion of overweight BMI (14.5%, p < 0.001). After adjusting for age, sex, race/ethnicity, geocoded median household income, Charlson's comorbidity index, and exposure to other medications known to affect BMI and baseline BMI category, there was a 34.6% higher risk for obesity among children prescribed aripiprazole compared with risperidone (p = 0.0033) (Table 3). Within one year, the proportion of patients who were obese among the aripiprazole group was 26.9% [95% CI 20.3–35] compared with 15% for risperidone [95% CI 12.8–17.6] (Fig. 3).
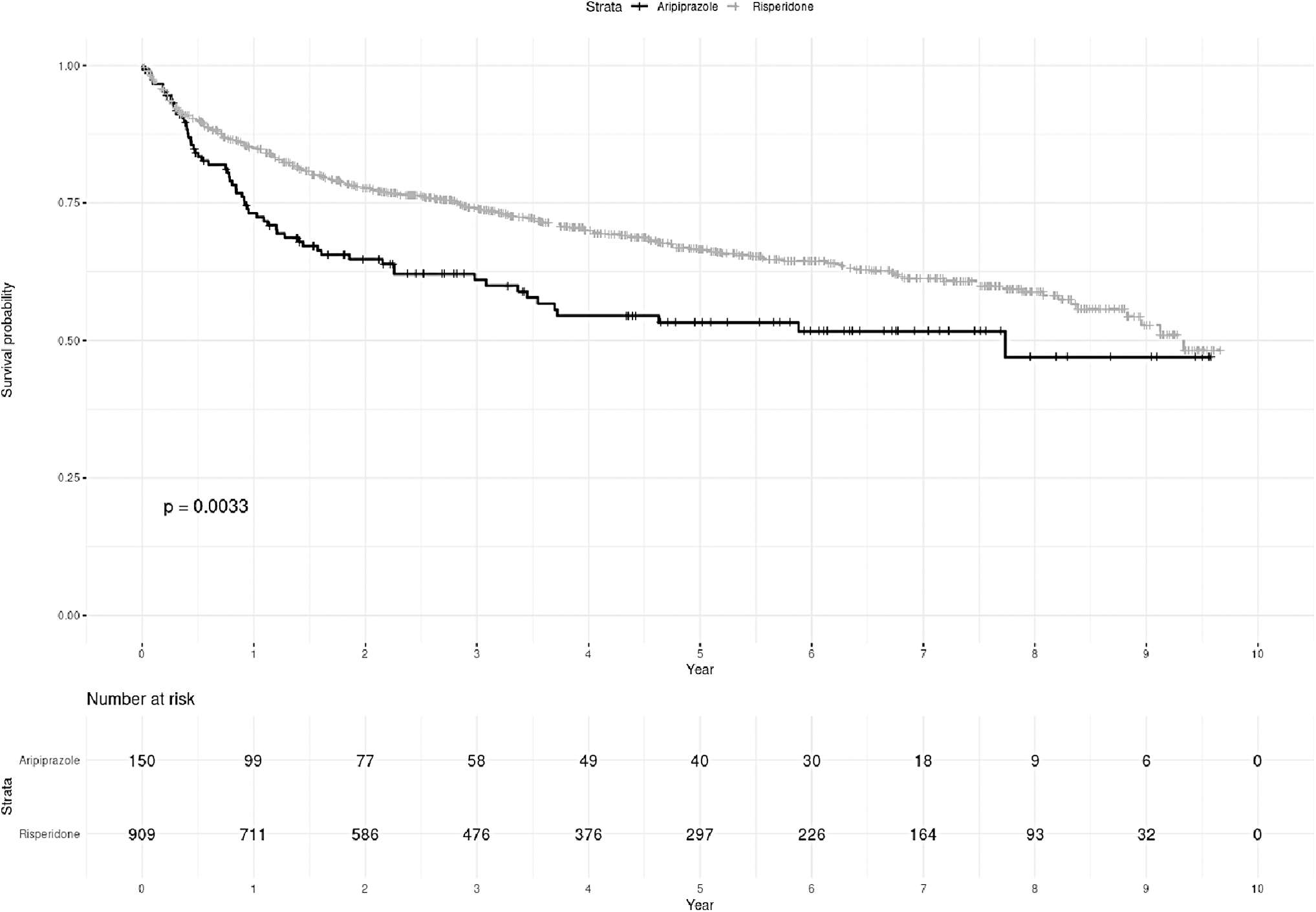
Kaplan–Meier curve showing time in years to obesity (BMI reaching the 95th percentile) for the group on aripiprazole or risperidone. p-Value is from the log-rank test. After adjustment for potential confounders, there was a 34.6% higher risk for obesity among children prescribed aripiprazole compared with risperidone (p = 0.0033). BMI, body–mass index.
Discussion
We hypothesized that long-term treatment with AAPs in young children would be associated with increased risk for obesity compared with treatment with SSRI antidepressants. We found that patients taking AAPs were twice as likely to become obese compared with patients taking SSRIs. This is consistent with other long-term studies of AAPs. Calarge et al. (2009) showed significant weight gain (BMI Z-score +1.6) for already overweight or obese patients on risperidone for up to 2 years in 99 patients with baseline age 10–17 years, although normal weight patients had much lower weight gain (BMI Z-score +0.1). Cianchetti and Ledda (2011) noted excessive weight gain with olanzapine (60.0% of the sample), risperidone (35.5%), and clozapine (28.6%), although not with aripiprazole, with a follow-up time of 3 or more years in 47 patients with baseline age 7–17 years. Noguera et al. (2013), in a study of treatment for the first psychotic episode in 110 children aged 9–17 years at baseline, demonstrated BMI Z-score increases for quetiapine 0.7, risperidone 0.7, and olanzapine 1.6 at the 2-year follow-up, higher than at the 6- and 12-month follow-ups, which (similar to our study) shows that increases in BMI continue over time; however, differences between the groups were statistically insignificant.
We also found that the risk of becoming obese for patients prescribed aripiprazole was statistically significantly higher than for patients prescribed risperidone, even after adjusting for differences in baseline BMI. This was an unexpected finding. In a meta-analysis of 28 randomized controlled trials of antipsychotics by Krause et al. (2018) on about 3000 child and adolescent patients treated for schizophrenia, aripiprazole presented a lower risk of weight gain than risperidone, although the difference was not statistically significant. These findings are similar to another meta-analysis (Pagsberg et al. 2017) that included 12 randomized controlled trials of about 2000 child and adolescent patients with schizophrenia-spectrum disorders. However, these included relatively short-term trials of 12 or fewer weeks.
Our finding is consistent with Pozzi et al. (2019) who followed 166 patients treated with risperidone or aripiprazole for a disruptive behavior disorder with or without autism spectrum disorder and/or intellectual disability for up to 2 years and compared children (≤13 years old) with adolescents (>13 years old). This study showed a higher BMI Z-score at 6 months for aripiprazole in children (+0.396) compared with adolescents (+0.234) than for risperidone in children (+0.096) compared with adolescents (−0.072); however, in this study, the children on risperidone were 2 years younger, on average, than those on aripiprazole and had higher baseline BMIs, and many of the patients had prior trials of AAPs.
We found possible socioeconomic disparities in prescription rates for AAPs and SSRIs, consistent with previous studies. Matone et al. (2012), in a cross-sectional study of all Medicaid-enrolled children, found an increase in AAP use from 2002 to 2007, particularly for patients with ADHD (an off-label use). Kreider et al. (2014) examined Medicaid-enrolled children (2004–2008) and found a high rate of concurrent use of AAPs with other psychotropic medication, particularly for low-income and foster children with ADHD or intellectual disabilities in ambulatory settings. Our study also shows possible racial disparity in prescription rates. However, there was no statistically significant difference in the rate of obesity by socioeconomic or racial category. Additionally, our data are not stratified by diagnosis or prior nonmedication treatments (e.g., psychotherapy), so this difference in prescription rate may not indicate true disparity. Further research should be done to examine the magnitude of these possible disparities.
Reyes et al. (2006) found that weight gain increased over the initial 12 weeks of treatment with risperidone (weight Z-score 0.3) and stabilized through 6 months, compared with those who switched to placebo after week 12 and showed reversal of all weight gain following risperidone discontinuation over a 6-month follow-up, and a study by Calarge et al. (2014) found that following several years of treatment, risperidone discontinuation is associated with a reversal of excessive weight gain over 1.5 years of follow-up. However, a study by Upadhyay et al. (2019) found that among children and adolescents with bipolar disorder prescribed AAPs for 3–24 months, while there was weight loss after medication discontinuation, the weight did not return to baseline within 1 year. Our study includes a notably longer length of follow-up time of up to 9.5 years, but was not designed to find patients who may have become obese and then had a reversal of weight gain to nonobese status. Further study should be done to look at the probability of becoming nonobese after discontinuation of medication.
To our knowledge, ours is the largest cohort of young children on AAPs. It includes a socioeconomically, racially, and ethnically diverse population treated in a large group practice setting, representing patients who have been treated for a variety of conditions, and includes clinical and pharmacy data, including confirmation that the medication was received by the patient.
There are limitations in our study. This was a nonrandomized, retrospective cohort design, with expected baseline differences between the cohorts. While there is some overlap of diagnoses, SSRIs and AAPs are not used to treat the same conditions, severity of patients treated may also differ, and the psychiatric diagnoses may themselves be associated with weight gain (Puder and Munsch 2010). There may similarly be a difference in diagnosis or severity of diagnosis at baseline or in physician's assessment of the propensity for weight gain (e.g., family history of obesity), which may explain a physician's decision to use one AAP over another.
Our finding that patients who were prescribed aripiprazole had a higher risk of obesity compared with risperidone was unexpected. Our methods included patients on aripiprazole for 6 months or more and who may previously have been on another AAP, such as risperidone, for less than 6 months, so it is possible that some of the obesity risk began before starting aripiprazole. We do not have data on any prior shorter-term medication trials (those less than 6 months). However, the aripiprazole group still showed additional risk of obesity over time after correction for baseline BMI category, after 6 months or more on aripiprazole alone.
BMI data were not measured in a standardized manner; for example, the amount of clothing worn at measurement may differ depending on the setting (e.g., clinic vs. emergency department). Nevertheless, measurement errors are equally likely to occur in either cohort, which reduces their potential impact on the findings.
The study design included children aged 10 years or younger to study only the prepubescent population, which may be different in their risk of obesity compared with adolescents and adults. However, there was no confirmatory measure of prepubescence (such as Tanner stage data), which may limit the specificity of the findings of this study.
Despite the known side effects of AAPs, as described previously, and that AAPs have become one of the costliest drug classes within the Medicaid program (Young et al. 2016), they are generally considered a quicker treatment alternative to traditional behavioral therapies, which are difficult to disseminate by providers in highly burdened facilities, may take many weeks to implement, depend on trained professionals for effective delivery, and require extensive family involvement before results are seen (Fossum et al. 2008; Comer et al. 2013).
Physicians and caregivers should consider the risk of obesity and associated long-term sequelae when prescribing AAPs and consider alternative evidence-based psychotropic and psychotherapeutic interventions in this young and vulnerable patient population. When an AAP is a part of the long-term treatment plan, efforts should be made to use AAPs with lower weight gain potential, include nutritional counseling, encourage exercise, or consider the addition of adjunctive pharmacological treatment to reduce weight gain such as metformin (Maayan and Correll 2010).
Conclusions
This study examined the long-term risk of obesity in a large group of young children who were prescribed AAPs or SSRIs for 6 months or more. For children not obese at baseline, those prescribed an AAP have approximately double the risk of obesity compared with those prescribed an SSRI. Children prescribed aripiprazole had a 34% greater risk of obesity than those prescribed risperidone.
Clinical Significance
This study is the first to examine the obesity risk for children 10 years or younger prescribed antipsychotics or SSRIs for 6 months or more in a large community sample. This further informs prescribers of the continuing risk over time for those patients who require long-term treatment.
Footnotes
Acknowledgments
The authors extend their thanks to Davida Becker, PhD, and Gino Mortillaro, MD, for reviewing and editing the manuscript and for their support in getting it submitted. It could not have been done without them.
Disclosure
No competing financial interests exist.